Department of pharmacology, CMR college of pharmacy, Medchal, Kandlakoya, Hyderabad 501401.
Thalidomide, originally introduced in the late 1950s as a sedative and treatment for morning sickness in pregnant women, became infamous for causing severe birth defects. Though banned in many countries, it re-emerged in later decades for specific indications such as multiple myeloma and leprosy-associated complications. This review provides a comprehensive overview of its history, pharmacology, adverse effects, regulatory actions, and current therapeutic repositioning. The article highlights lessons learned and the evolution of drug safety protocols shaped by the thalidomide tragedy. Thalidomide is an infamous pharmaceutical agent once marketed as a safe sedative and antiemetic, particularly for pregnant women. Its widespread use in the late 1950s and early 1960s led to a global tragedy when it was found to cause severe congenital malformations, most notably limb deformities (phocomelia), in thousands of newborns. The thalidomide disaster triggered sweeping reforms in drug development, testing, and regulatory oversight, with long-standing impacts on patient safety and pharmaceutical policy worldwide. Despite its notorious history, thalidomide has found renewed medical applications in the treatment of conditions such as multiple myeloma and leprosy, but with strict precautions to avoid fetal exposure. This review summarizes the history, mechanisms of harm, regulatory changes, and current clinical status of thalidomide, highlighting its lasting legacy on medicine and drug safety.
Thalidomide represents one of the darkest chapters in pharmaceutical history. Marketed initially as a safe sedative for pregnant women, its teratogenic effects were devastating. By the early 1960s, over 10,000 children worldwide were born with severe malformations due to prenatal exposure to thalidomide [1]. Despite its ban, the drug has seen a resurgence in controlled medical settings. This review explores the dual life of thalidomide from tragedy to therapeutic potential.
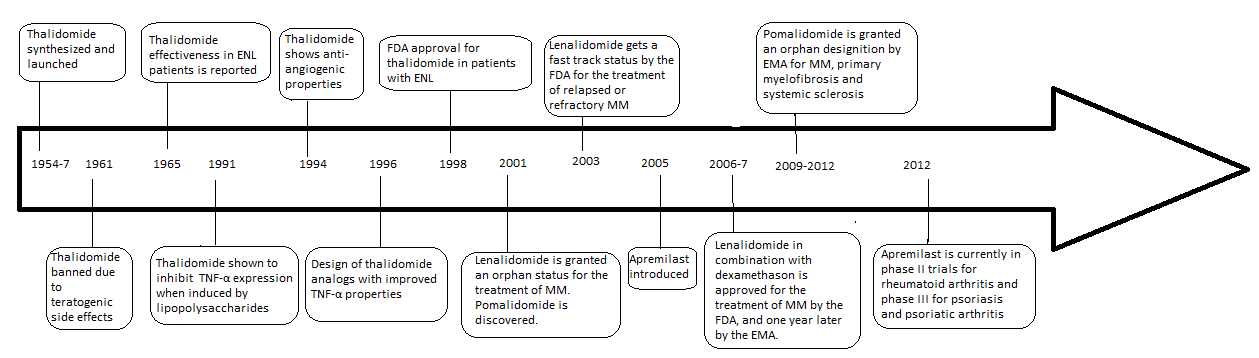
2.History and Development
The Scandal and Ban
Consequences and Regulatory Reforms
Mechanisms of Harm
Ongoing Medical Role and Precautions
Lasting Legacy
Thalidomide’s story underscores the critical need for safety, transparency, and rigorous testing in drug development. It set the benchmark for modern pharmaceutical regulation, patient advocacy, and vigilance in clinical practice. The ongoing availability of thalidomide under closely regulated conditions reflects both its therapeutic potential and the lessons learned from its tragic past.
3.Mechanism of Action
Thalidomide exhibits multiple pharmacological actions:
|
Reason for Ban |
Description |
|
Severe Birth Defects (Teratogenicity) |
Thalidomide caused catastrophic congenital malformations, especially limb deformities, when taken during pregnancy. More than 10,000 children were affected worldwide, primarily with shortened or absent limbs (phocomelia), eye, ear, and heart defects. |
|
Lack of Adequate Safety Testing |
At the time, thalidomide was approved based on animal toxicity but not for teratogenic (birth-defect-causing) effects. Drug safety regulations did not require fetal development studies. |
|
Peripheral Neuropathy in Adults |
Adults taking thalidomide developed nerve damage (peripheral neuritis), manifesting as numbness and tingling in the hands and feet. This initially raised concerns about its general safety. |
|
Over-the-Counter Availability |
Thalidomide was widely and easily accessible in many countries without prescription, increasing the scale of fetal exposure and harm before dangers were recognized. |
|
Delayed Recognition and Withdrawal |
Many early adverse effects were denied or overlooked by the manufacturer and some authorities, leading to delayed drug withdrawal and prolonged public exposure. |
|
Inadequate Drug Regulation |
At the time, drug legislation was insufficient to prevent or respond rapidly to new drug risks. The thalidomide crisis directly prompted reforms in drug testing, approval, and monitoring worldwide. |
4.Teratogenic Effects and Adverse Outcomes
Thalidomide-induced embryopathy results from its interference in limb bud development during early pregnancy [8]. Major anomalies included:
Animal studies revealed species-specific sensitivity, with rabbits and primates showing comparable effects to humans [9]
5.Global Impact and Regulatory Response
The thalidomide tragedy prompted major reforms in drug regulation:
6. Repositioning of Thalidomide
Despite its past, thalidomide has found new roles:
6.1 Leprosy
Approved by the FDA in 1998 for erythema nodosum leprosum (ENL) due to its immunomodulatory effects [13].
6.2 Multiple Myeloma
Used in combination therapies for relapsed or refractory cases [14].
6.3 Other Conditions
The conditions like HIV- related ulcers, Crohn’s disease, graft- versus- host disease are investigated [15].
7. Pharmacokinetics and Metabolism
8. Risk Management Programs
Due to its teratogenicity, programs like S.T.E.P.S. (System for Thalidomide Education and Prescribing Safety) were created to ensure patient safety through pregnancy testing, informed consent, and restricted distribution [17].
9. Thalidomide Analogs
Second-generation analogs developed to reduce toxicity:
10. Ethical and Legal Considerations
Thousands of victims sought compensation. While some countries offered settlements, many cases remain unresolved. The tragedy highlighted ethical concerns in clinical trials and pharmaceutical marketing [20].
11. Lessons Learned
Thalidomide catalyzed significant changes in:
Its story underscores the importance of rigorous preclinical testing, especially in vulnerable populations like pregnant women [21].
12. CONCLUSION
The thalidomide tragedy is a landmark event in pharmaceutical history, symbolizing the catastrophic consequences of inadequate drug testing and insufficient regulatory oversight. Marketed as a safe sedative and antiemetic for pregnant women, thalidomide led to the birth of thousands of children with severe deformities, including limb malformations, blindness, deafness, and internal organ defects. This event prompted a global reevaluation of drug safety protocols, resulting in stricter preclinical testing requirements, more rigorous clinical trial regulations, and the establishment of modern pharmacovigilance systems. The legacy of thalidomide remains a cautionary tale that underscores the ethical responsibility of pharmaceutical companies and regulatory bodies to protect vulnerable populations, particularly during pregnancy. In recent years, thalidomide has been cautiously reintroduced for specific therapeutic purposes, including the treatment of erythema nodosum leprosum and multiple myeloma. This controlled use is supported by comprehensive risk management programs that include mandatory pregnancy testing, informed consent, and restricted distribution. The drug's reemergence, alongside the development of less toxic analogs like lenalidomide and pomalidomide, highlights its therapeutic potential when used responsibly. Nevertheless, the historical impact of thalidomide continues to influence drug development and approval processes worldwide, serving as a persistent reminder of the importance of rigorous safety evaluations, ethical clinical practices, and the prioritization of patient welfare in all aspects of medical research and practice.
REFERENCES


Gunukula Alekhya*, Dr. P. Kishore Kumar, Thalidomide Pharmacological Actions of a Banned Drug, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 10, 2125-2131 https://doi.org/10.5281/zenodo.17395186
 10.5281/zenodo.17395186
10.5281/zenodo.17395186
