Malla Reddy College of Pharmacy, Affiliated to Osmania University, Hyderabad, Telangana.
Asthma-one of the most common chronic, non-communicable diseases in children and adults-is characterized by variable respiratory symptoms and variable airflow limitation. Asthma is a consequence of complex gene-environment interaction, with heterogeneity in clinical presentation and the type and intensity of airway inflammation and re-modelling. The goal of asthma treatment is to achieve good asthma control-i.e., to minimize symptom burden and risk of exacerbations. Anti-inflammatory and bronchodilator treatments are the mainstay of asthma therapy and are used in a stepwise approach. Pharmacological treatment is based on a cycle of assessment and re-evaluation of symptom control, risk factors, comorbidities, side-effects, and patient satisfaction by means of shared decisions. Asthma is classed as severe when requiring high-intensity treatment to keep it under control, or if it remains uncontrolled despite treatment. New biological therapies for treatment of severe asthma, together with developments in biomarkers, present opportunities for phenotype-specific interventions and realization of more personalized treatment.
Asthma is a chronic inflammatory, non-communicable disease that obstructs the airways in the lungs. The key element in the pathophysiology of asthma is inflammation. Asthma is a worldwide health issue that impacts over 300 million people across all age categories, ethnicities, and nations.2 Inflammation, bronchoconstriction, mucus buildup, and structural alterations in the airways are the main causes of airway obstruction.3 Environmental and nutritional modifications to prevent exposure to harmful inhaled antigens are the mainstay therapy for horse asthma. The injection of corticosteroids, bronchodilators, or both is advised when these modifications are not feasible or adequate to alleviate airway obstruction, or when prompt relief is needed.4 Adult-onset asthma, exercise-induced bronchoconstriction (EIB), occupational asthma, asthma-COPD overlap, pediatric asthma, allergic asthma, and non-allergic asthma are among the several forms ofasthma.5Allergens cause the most common type, allergic asthma, but stressful events, virus infections,and severe weather can cause non-allergic asthma. When a person's first asthma symptoms appear solely as an adult, this is referred to as adult-onset asthma.6 This study's main goal was to assess the two medications bronchodilation duration and potency in SA. Its secondary goal was to compare the incidence of side effects. It was hypothesized that while HBB is more effective than salbutamol at treating bronchospasm, it has more negative side effects, particularly tachycardia.
Bronchodilator’s Possible Impact on Asthma Comorbidities:
1. Cardiovascular disorders in bronchodilators and asthma:
Systemic corticosteroids of inhaled bronchodilators are low, or occasionally too low, to be identified by conventional bioanalytical techniques when given at the appropriate dosages.7 It should be mentioned, nonetheless, that plasma levels do not indicate effectiveness, and that β2- agonists and muscarinic antagonists can both reach myocardial receptors, such as muscarinic M2 receptors and β-adrenoreceptors, respectively.
2. Angina and coronary disease:
Hypoxemia and necrosis of the coronary arteries are the causes of angina pectoris. The lack of oxygen in the bloodstream, known as hypoxemia, can be broughton by variations in ventilation, perfusion, or respiratory rate. Hypoxemia can also result from cardiovascular reasons, such as shunts. Shunts, hypoventilation, and imbalances in the ventilation/perfusion rates are the most frequent causes of hypoxemia. One preventable cause of asthma-related death is profound hypoxemia.8
3.Cardiac arrhythmia: In young individuals with asthma, ipratropium bromide had no discernible impact on heart rate or cardiac vagal tone.9. A nested casecontrol research, however, revealed that although the absolute risk was modest, using inhaled ipratropium was linked to a higher incidence of arrhythmia in adolescents and young adults with asthma when compared to nonusers.10 Even at therapeutic levels of theophylline in the serum, the drug can induce tachycardia and severe arrhythmias.11 One arrhythmia linked to this medication is multifocal atrial tachycardia,which may be a sign of abrupt cardiac death. Nevertheless, there is evidence that doxofylline may be a viable substitute for theophylline in the treatment of asthmatic patients, with a better efficacy/safety profile.12
4. Obesity: The pathophysiology of lung disease in this population is significantly impacted by the various alterations that obesity causes in normal lung physiology and immunological function. Lung mechanics are significantly changed by obesity. Due to the loading effects of visceral adipose tissue on the diaphragm and adipose tissue on the chest wall, obese people have a smaller resting lung capacity than thin asthmatics.13.
5. Diabetes Mellitus: Diabetes mellitus (DM) is a chronic illness marked by the inability to transport glucose inside the cells. Insulin resistance, insufficient insulin secretion by the β cells of the pancreatic islets, and hyperglucagonemia all contribute to hyperglycemia in type 2 diabetes mellitus (T2DM). Once believed to be a condition that only affected the elderly, type 2 diabetes is now more common in younger people as well.14
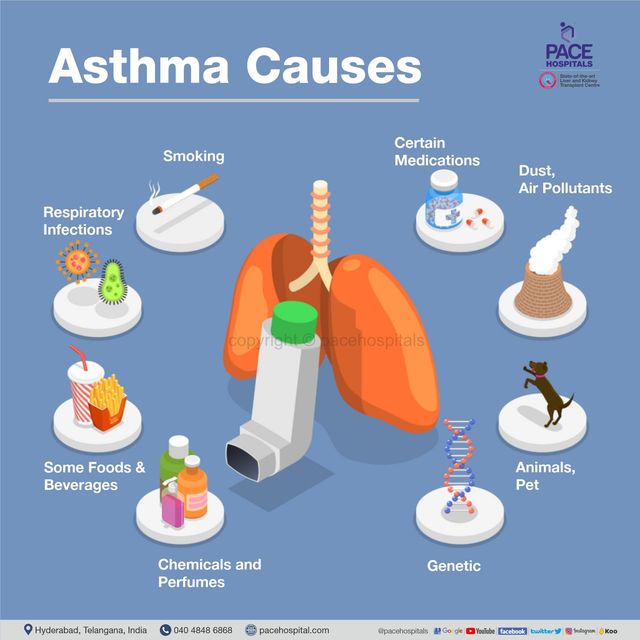
Causes Or Common Threat Factors:
The lungs development and degeneration are caused by common danger factors. Rotundity, smoking, poor physical effort, and adulterants are among the conditions that might cause psoriasis. Malnutrition, infection, exposure to allergens, metabolic pattern, and connective tissue-illnesses, sadness, and medication use. 1. Smoking: Research on smoking has revealed that psoriasis patients smoke more actively and passively than the general population. Research has demonstrated a substantial correlation between smoking and the incidence and severity of psoriatic lesions. In addition, smoking is thought to be the primary cause of chronic obstructive pulmonary disease. Idiopathic pulmonary fibrosis and asthma are two more lung conditions linked to smoking. As a result, smoking might contribute to the higher incidence of lung illness among psoriasis patients.
2.Obesity: Being overweight and not exercising. Physical inactivity and obesity have been found to be risk factors for the development and severity of psoriasis, and it has been shown that psoriasis patients are more likely to be obese. One of the main risk factors for respiratory conditions such sleep apnea, pulmonary hypertension, and asthma is obesity.Additionally, it has been linked to chronic obstructive pulmonary disease.Therefore, the increased incidence of pulmonary illness in psoriasis may be explained by fat.
3.Pollutant: It has been suggested that cadmium, an element present in batteries and dental fillings used in the television and aviation industries, is linked to the onset of psoriasis.cadmium levels in the blood were greater in psoriasis patients.in addition, men with chronic obstructive lung disease, including those who never smoke, are linked to elevated blood levels of cadmium .cadmium (and other air contaminants) can therefore have an equal impact on a person's development of lung disease and psoriasis.
4.Infection: Psoriasis and lung diseases can both be significantly influenced by infections. The development of asthma is linked to the altered lower respiratory tract microbiome, which also interacts with the mucosal innate immune system and may raise the risk of psoriasis. Furthermore, it is well recognized that psoriasis and lung conditions such asthma, chronic obstructive pulmonary disease, and pulmonary arterial hypertension are predisposed to HIV infection. Lung disease and psoriasis can develop or worsen as a result of HIV infection.
5.Allergy: It has been demonstrated that psoriasis patients are somewhat more sensitive to contact allergens, including molds, birch, mugwort, thyme, and rye pollen, as well as dust mites and home dust.There was a correlation between PASI and the severity of the hypersensitive reaction.Additionally, the incidence, severity, and management of asthma are significantly influenced by allergy sensitivity.According to recent research, allergies to mold, cockroaches, animal danger, or house dust mites can increase the risk of developing asthma.
6.Depression: Depressive psoriasis is a chronic inflammatory skin condition that impacts family life, leisure time, and sexuality in addition to limiting social and professional chances. These limitations could lead to stress, which has been linked to psoriasis.[23] However, among patients with interstitial lung disease, depression is a prevalent and long-lasting comorbidity. developing asthma.
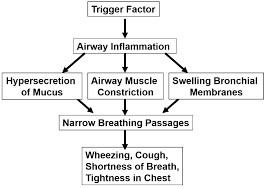
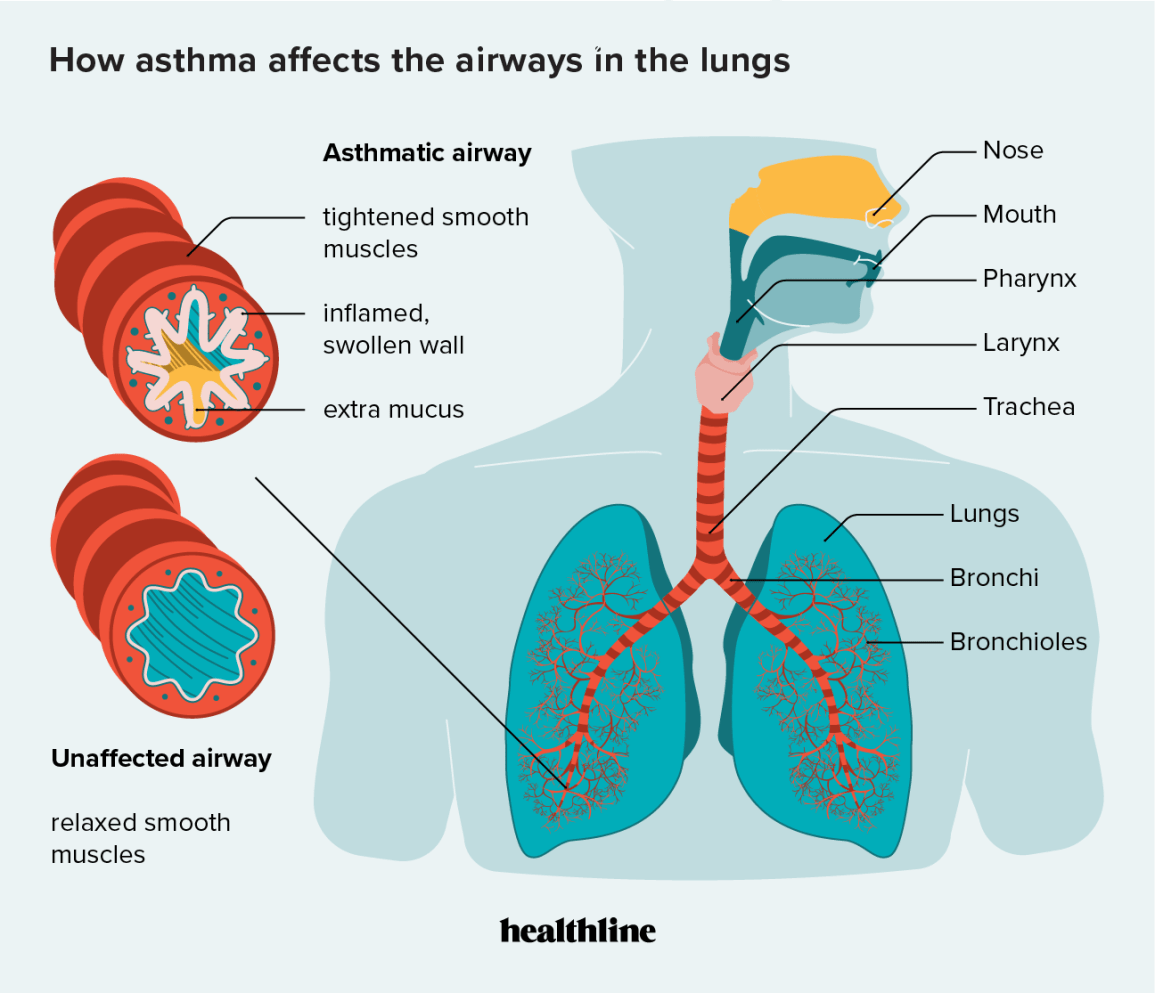
Pathophysiology:
Similar to other atopic disorders, asthma is linked to T helper cell type2 (Th2) immunological responses. Chronic airway inflammation results from a series of immunemediated processes caused by a variety of allergic (such as dust mites, cockroach residue, furred animals, molds, and pollens) and allergic (such as infections, tobacco smoking, cold air, and exercise) stimuli.Certain cytokines, including as interleukin (IL)-4, IL-5, IL-9, and IL13, are released by elevated Th2 cells in the airways and encourage eosinophilic inflammation and mast cell production of immunoglobulin E (IgE). Histamine and cysteinyl leukotrienes are two examples of inflammatory mediators that are released when IgE is produced.The hallmark symptoms of asthma are caused by bronchospasm (contraction of the smooth muscle in the airways), edema (swelling), and increased mucous secretion (mucous hypersecretion) .An further inflammatory response (late-phase asthmatic response) is triggered by the mediators and cytokines generated during the early phase of an immune response to an instigating allergen, which results in increased airway inflammation and bronchial hyperreactivity .There may be a hereditary predisposition to asthma, according to the evidence. Several chromosomal areas have been linked to asthma susceptibility, including those involving the synthesis of inflammatory mediators, the expression of airway hyperresponsiveness, and the creation of IgE antibodies. However, further research is needed to identify the precise genes linked to asthma as well as the gene-environment interactions that could result in the disease's manifestation. Pathophysiology Early postmortem investigations 58 provide a large portion of the present data that links asthma to inflammatory etiology. These studies show that individuals who die from acute asthma have severely inflamed airways, mucus plugging, and edematous airways packed with lymphocytes and eosinophils. It was originally believed that airway hyperresponsiveness caused asthma, therefore this inflammation had to be an end-stage occurrence in deadly asthma. Inflammation has also been detected by newer technologies that enable inspection of people with asthma, such as fiberoptic bronchoscopy and bronchoalveolar lavage (BAL). Although the results are comparable in children, lymphocytes—rather than eosinophils, which are more prevalent in adults—are the most prevalent inflammatory cells.9Patients with asthma have red, swollen airways upon bronchoscopy, and their BAL has higher levels of inflammatory mediators.
Types Of Asthma:
Allergic Asthma:
Allergens such as dust mites, pollen, and pets can cause allergic asthma. Atopic asthma is another name for it. Allergies affect about four out of five asthmatics. You could undergo a blood test or skin prick test to see whether you are allergic to any common allergens if you have been diagnosed with asthma. This will assist you in identifying the things that cause your asthma. Many people who have asthma have non-allergic triggers as well, such as cigarette smoke and cold temperatures.
Non-Allergic Asthma:
Asthma that isn't brought on by an allergen, such as dust mites or pollen, is referred to as non-allergic asthma or non-atopic asthma. Compared to allergic asthma, it is less prevalent. Non-allergic asthma affects about 1 in 5 asthmatics. Asthma that is not allergic frequently appears later in life. You may have non-allergic asthma if allergens such as dust mites, pollen, or dogs do not appear to trigger your asthma. The following can cause non-allergic asthma: colds, flu, chest infections, stress, recreational substances, cigarette smoke, and air pollution, dampness and mold.
Occupational Asthma:
Asthma that necessitates high dosages to manage symptoms is referred to as difficult asthma. Difficult asthma affects about 1 in 5 persons with asthma. It is sometimes referred to as difficult-to-treat or difficult-to-control asthma. For the majority of patients, asthma symptoms can be reduced with proper management. This implies: Using an asthma action plan and taking your preventer or MDI inhaler as directed each day will help you know what to do in the event that you experience asthma symptoms. You should also have an asthma review at least once a year.
Seasonal Asthma:
Some people only have symptoms of asthma during specific seasons, such hay fever season or cold weather. This is sometimes called "seasonal" asthma. It's crucial to stick to your asthma action plan and use your preventer inhaler as directed, even if your symptoms only appear during specific seasons of the year. Your doctor or nurse can recommend an AIR treatment plan if you only require assistance with managing your asthma during specific seasons of the year.
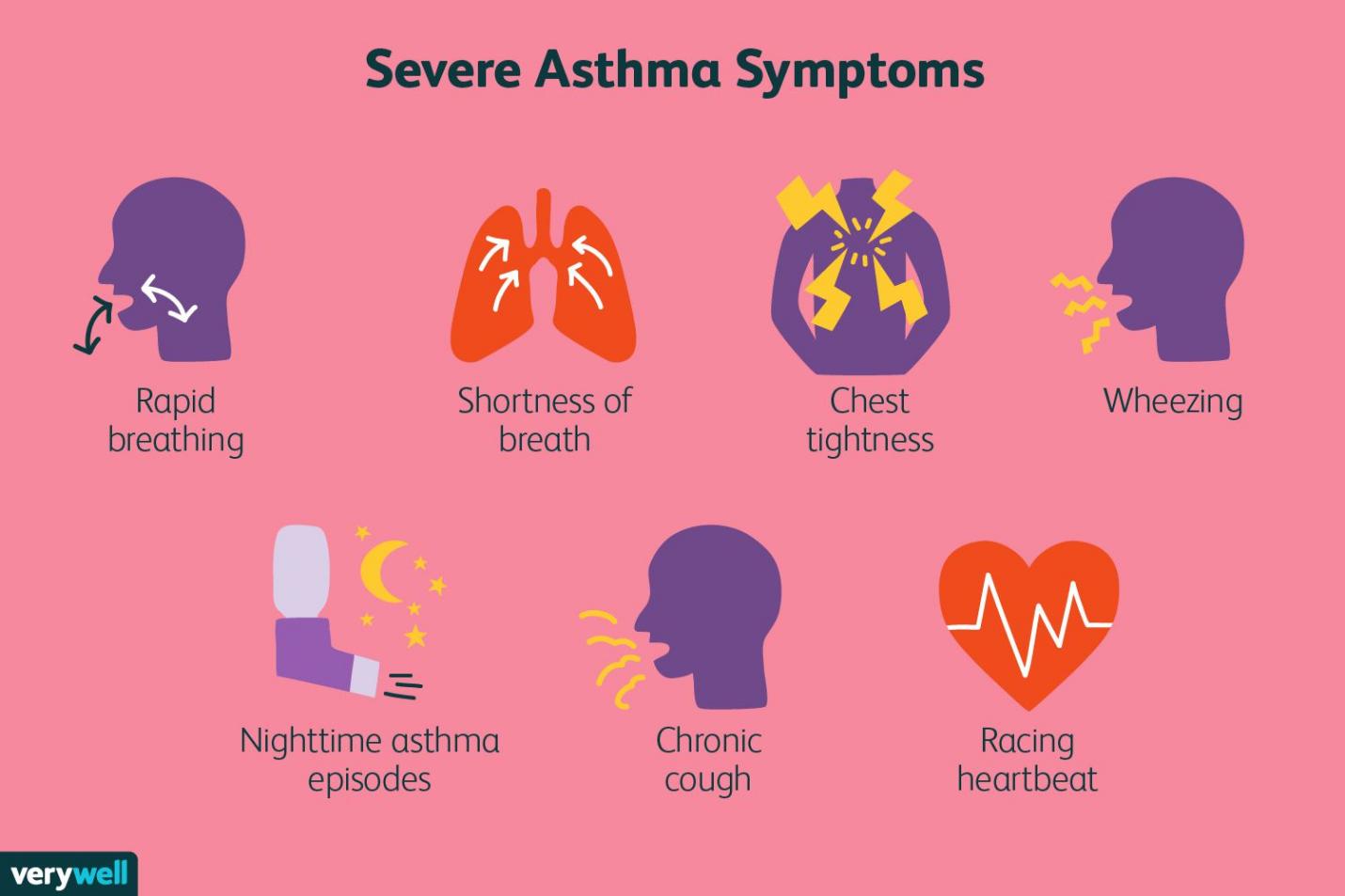
Severe Asthma:
Aim And Objectives
Aim: To Evaluate and compare the efficacy, safety, and therapeutic outcomes of difference classes of bronchodilators in management of asthma.
Objectives:
•To classify the different types of bronchodilators used in asthma management (eg:beta 2 agonists, anti-Cholinergics etc).
•To compare the short acting and long-acting bronchodilators in terms of onset of action, duration and frequency of use.
•To investigate the role of bronchodilators in adult, and generic asthma patients.
Plan of Study:
1.Title Selection
↓
2. Literature Review
↓
3. Define Aim & Objectives
↓
4. Study Design & Methodology
- Observational Cohort
- Sample Size: 60
- Study Duration: 3 Months
↓
5. Patient Selection
- Apply Inclusion/Exclusion Criteria
↓
6. Data Collection
- Clinical data on bronchodilator usage, symptoms, outcomes
↓
7. Data Analysis
- Use Excel & GraphPad Prism
- Apply Descriptive Statistics
↓
8. Result Interpretation
- Compare drug usage, severity, effectiveness
↓
9. Discussion
- Compare findings with existing studies
↓
10. Conclusion & Recommendations
↓
11. References & Report Writing
Literature Review
Research And Methodology
The study was conducted at Malla Reddy Health City Hyderabad Patients who had visited hospital during a period of 3 months.
Study Design: Observational cohort study
Sample Size: During study period of 3 months total 80 cases were collected and studied.
Study Period: The study was carried out for a period of 3 months.
Study Criteria:
Inclusion Criteria:
1.Individuals with a confirmed clinical diagnosis of asthma
2. Patients aged 4 to 80 years
3.Patients with stable asthma
4. Patients with mild to moderate persistent asthma.
Exclusion Criteria:
1.Patients with a diagnosis of COPD, other chronic lung diseases.
2.Patients who have used oral or injectable corticosteroids within the last 4 weeks.
3.Pregnancy and lactation are contraindications due to potential risk to the fetus or infant.
4.Patients with mental illness or cognitive disabilities.
Collection Of Data:
•All asthma patients admitted to the respiratory ward and satisfying the inclusion criteria were selected.
•The data was collected using a pre-structured data collection form designed specifically for this comparative study of bronchodilator therapies.
Statistical Analysis:
•The collected data was entered into Microsoft Excel and analyzed using GraphPad Prism.
•Descriptive statistics such as mean, standard deviation, and percentage were used to summarize demographic data and clinical outcomes.
Table-1: Age And Gender Distribution
|
Age & gender distribution |
4-10 Years |
11-20 Years |
21-30 Years |
31-40 Years |
41-80 Years |
Total |
|
Male |
6 |
5 |
6 |
7 |
22 |
45 |
|
Female |
5 |
5 |
8 |
7 |
10 |
35 |
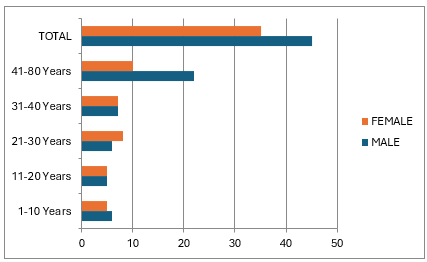
The age-wise distribution indicates that the highest proportion of participants belonged to the 41-80 years age group in both genders. The data shows a higher number of male participants compared to females across most age groups males (45) females (35).
Table-2: Bronchodilators Used by Asthma Patients
|
Bronchodilators |
No of patients |
|
|
|
Male |
Female |
|
Salbutamol |
17 |
13 |
|
Ipratropium |
12 |
5 |
|
Budesonide |
12 |
8 |
|
Formeterol |
2 |
3 |
|
Montelukast |
10 |
6 |
|
Levosalbutamol |
11 |
5 |
|
Albuterol |
12 |
6 |
|
Tiotropium |
15 |
5 |
|
Salmeterol |
11 |
8 |
|
Levocetirizine |
4 |
1 |
|
Methyl Anthine |
4 |
3 |
|
Ambroxolol |
1 |
2 |
|
Fluticasone |
3 |
1 |
|
Budesonide + Formoterol |
8 |
5 |
|
Salmetrol + Fluticasone |
2 |
4 |
|
Etofylline + Theophylline |
1 |
0 |
|
Budesonide + Salmetrol |
2 |
3 |
A study on asthma patients showed that Salbutamol was the most commonly used bronchodilator (17 males, 13 females). Other commonly used drugs includes Tiotropium, Ipratropium, Budesonide, and Albuterol, with slightly higher usage in males. Combination therapies such as Budesonide + Formoterol and Salmeterol + Fluticasone were also prescribed. Overall, most bronchodilators were more commonly used.
Table-3: Grady Of Severity of Asthma Exacerbation Based on Clinical Data
|
Clinical Management |
Male |
Female |
|
Cough |
4 |
10 |
|
Shortness of breath |
12 |
5 |
|
Cold |
4 |
2 |
|
Wheezing |
12 |
8 |
|
Dyspnea |
2 |
1 |
|
Chest tightness |
10 |
6 |
|
Vomiting |
2 |
2 |
|
Total |
46 |
34 |
In male asthma patients, shortness of breath and wheezing were most common (12), followed by chest tightness (10). In females, cough was most common (10), wheezing (8) and chest tightness (6). Overall, 46 males and 34 females had asthma-related symptoms.
Table- 4: Common Symptoms and Complaints During Bronchial Asthma
|
Complaints And Symptoms |
Male |
Female |
|
Cough |
13 |
8 |
|
Shortness Of Breath |
5 |
7 |
|
Chest Tightness |
4 |
6 |
|
Wheezing |
3 |
4 |
|
Persistent Dry Cough |
5 |
6 |
|
Trouble In Sleeping |
3 |
3 |
|
Mucusproduction |
8 |
5 |
The most common symptom in males was cough, followed by mucus production and shortness of breath. In females, cough and shortness of breath were most common, along with other symptoms experienced such as cough, wheezing, chest tightness, trouble in sleeping.
Table-5: Comparison of Repeated Use of Nebulizers Between Groups
|
No Of People |
Male |
Female |
|
Inhaled Corticosteroids |
4 |
2 |
|
Salbutamol |
8 |
6 |
|
Ipratropium Bromide |
6 |
7 |
|
Budesonide |
9 |
5 |
|
Formoterol |
5 |
6 |
|
Ambroxol |
3 |
4 |
|
Formoterol + Budesonide |
2 |
4 |
|
Salmeterol |
3 |
4 |
|
Prednisolone |
1 |
1 |
|
Total |
41 |
39 |
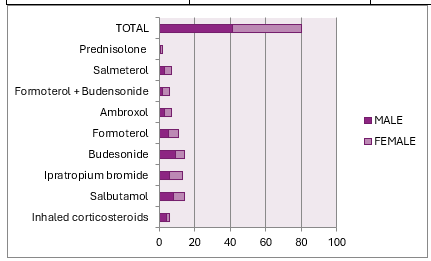
The repeated use of nebulizers was slightly higher in males (41) compared to females (39). Budesonide and Salbutamol were the most commonly used drugs in both groups. Ipratropium bromide and Formoterol were also frequently used.
DISCUSSION
The highest number of asthma patients were observed in the 41–80 years age group, with a male predominance (45 males vs 35 females) across all age categories. This indicates a greater burden of asthma in older populations, possibly due to accumulated environmental exposure, smoking history, or undiagnosed chronic airway diseases overlapping with asthma in older males. Females had a slightly higher count in the 21–30 age group, which may reflect hormonal influences or better healthcare-seeking behavior in this demographic details. The most frequently used bronchodilator was Salbutamol (17 males, 13 females), reinforcing its role as the first-line reliever in asthma management. Other commonly used medications included Tiotropium, Albuterol, Levosalbutamol, Montelukast, and Ipratropium. Combination therapies such as Budesonide + Formoterol and Salmeterol + Fluticasone were also prescribed, particularly in moderate to severe cases.Males showed higher usage of Ipratropium and Tiotropium, suggesting that anticholinergic agents are more commonly used in older males or those with severe symptoms. Combination inhalers were used across both genders, reflecting adherence to stepwise therapy as recommended by asthma management guidelines (e.g., GINA). Symptoms like shortness of breath and wheezing were highly prevalent in males, whereas cough was more commonly reported in females. This reflects possible gender-based differences in symptom perception or response to airway inflammation. Wheezing was a dominant feature in both genders, reaffirming its role as a primary indicator of bronchospasm. Chest tightness and dyspnea were also common, supporting the presence of moderate to severe exacerbation in many patients. Across genders, cough remained the most frequent symptom, followed by shortness of breath and mucus production. These findings are in line with clinical presentations of asthma and support the need for personalized treatment based on symptom type and intensity. Persistent dry cough and trouble sleeping were noted in both groups, indicating poorly controlled asthma or nocturnal symptoms, often requiring long-acting control therapy. Mucus production was slightly higher in males, which might indicate an overlap with chronic bronchitis or increased airway inflammation. Repeated nebulization was reported in both males and females (41 and 39, respectively), with Budesonide, Salbutamol, and Ipratropium bromide being the most used medications. This pattern reflects the need for frequent symptom control, especially during exacerbations. Combination nebulizers such as Formoterol + Budesonide were used more often in females, possibly reflecting more aggressive step-up therapy. Frequent nebulization points to either poor baseline control or increased trigger exposure and underlines the importance of regular monitoring and preventive therapy.
CONCLUSION
This study highlights the critical role bronchodilators play in the effective management of asthma across varying patient demographics and severities. Among the bronchodilators evaluated, Salbutamol emerged as the most frequently used agent due to its rapid onset and effectiveness in acute symptom relief. However, Tiotropium, Ipratropium, and combination therapies such as Budesonide + Formoterol demonstrated better control in moderate to severe cases, especially when used consistently with inhaled corticosteroids. Short-acting bronchodilators (SABAs) are ideal for quick symptom relief, while long-acting agents (LABAs and long-acting anticholinergics) provided sustained control when used appropriately. The combination therapies yielded superior therapeutic outcomes by improving lung function, reducing symptom frequency, and minimizing the need for rescue medications. The comparative analysis also underscored the importance of patient-specific factors, including age, gender, comorbidities, and inhaler technique, in choosing the most effective bronchodilator therapy. Proper education regarding inhaler use and adherence to treatment protocols is essential for optimal outcomes. Overall, while all bronchodilators serve a valuable role in asthma therapy, their efficacy and safety profiles vary. Hence, a personalized, stepwise treatment approach tailored to individual patient needs and response remains the cornerstone of asthma management.
REFERENCES

Dr. Parveen Shaik*, Arkari Rishitha, Ayeesha Nazneen, Badagouni Somnath, Baru Bhanu Vara Prasad, Basangari Sindhu, Comparative Study of Bronchodilators in the Management of Asthma, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 3648-3663. https://doi.org/10.5281/zenodo.16478830
 10.5281/zenodo.16478830
10.5281/zenodo.16478830
