Raosaheb Patil Danve College of Pharmacy, Badnapur, Jalna
Plasmodium, which infects red blood cells. New antimalarial drug is a fixed dose combination of two antimalarial active ingredients arterolane maleate and piperaquine phosphate. Arterolane undergoes reductive cleavage in the food vacuole by ferrous iron to generate free radicals which inhibit PfATP6, a sarcoplasmic endoplasmic reticulum calcium ATPa Malaria is an infectious disease caused by a parasite, se encoded by P. Falciparum. Piperaquine produces inhibition of the heme-digestion pathway in the parasite food vacuole. Both the drugs are well absorbed orally with Peak plasma concentrations between 3-5 hours post dose for arterolane and 4-6 hours post dose for piperaquine and both are highly plasma protein bound with extensive volume of distribution. The major metabolic pathway is the oxidation of the adamantane moiety for arterolane. Overall contribution of CYP3A4 to Arterolane metabolism is 30%. CYP3A4 is the primary isozyme responsible for the metabolism of both arterolane as well as piperaquine. Observed metabolites from liver microsomes are monooxygenation and dioxygenation products for piperaquine. Arterolane is rapidly eliminated from blood plasma. Hence, the combination provides rapid clearance of parasitemia and most malaria-related symptoms, coupled with prevention of recrudescence.
Malaria is an infectious disease caused by a parasite, Plasmodium, which infects red blood cells. Malaria has infected humans since the beginning of mankind. The name "mal aria" (meaning "bad air" in Italian) was first used in 1740 by H. Walpole. The term was shortened to "malaria" in the 20th century. C. Laveran in 1880 was the first to identify the parasites in human blood. The five species that cause malaria are
SIGN AND SYMPTOMS :
The symptoms characteristic of malaria include-
Sometimes symptoms may occur later in those individuals who have taken antimalarial medications. Initial propagation are similar to flu-like symptoms, septicemia, gastroenteritis and viral diseases. They also may include headache, fever, shivering, joint pain, vomiting, - jaundice, hemoglobin urea, retinal damage, convulsions and hemolytic anemia,The main classic symptom is cyclical occurrence of sudden coldness followed by shivering and then fever and sweating, which is known as paroxysm.
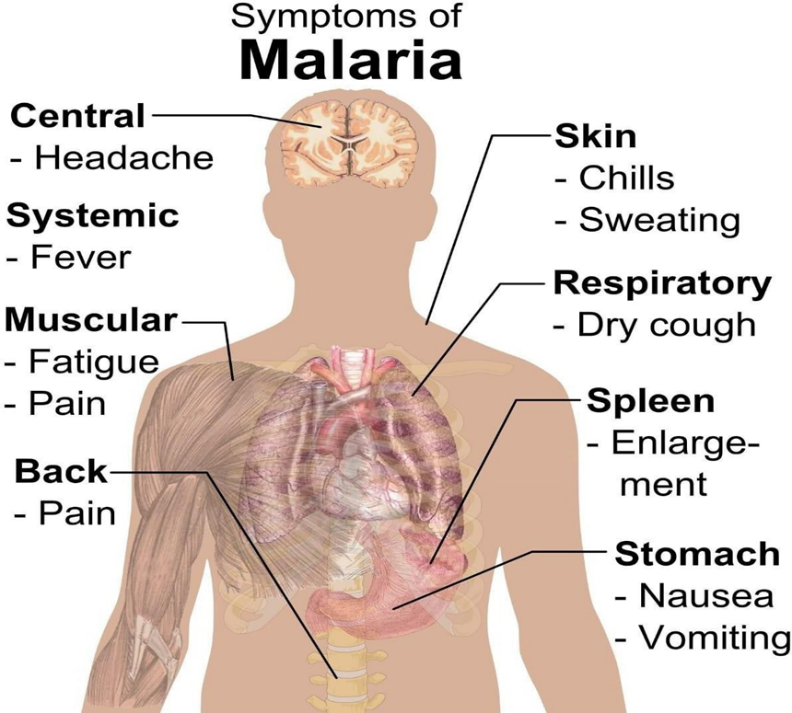
Fig 1. Symptoms of malaria
Complications:-
The main complication is the development of respiratory distress, due to respiratory compensation of metabolic acidosis, Concomitant pneumonia, noncardiogenic pulmonary oedema and severe anaemia. Acute respiratory distress syndrome occurs in 5–25% of adults and up to 29% of pregnant women.7 Infection of HIV with malaria increases the chances of death.8 Due to infection with P. falciparum Cerebral malaria may occur. Which is associated with retinal whitening (a useful clinical sign in distinguishing malaria from other causes of fever.)9 Splenomegaly, liver enlargement, hypoglycemia, severe headache, and hemoglobin urea with renal failure may occur.4 Malaria may cause stillbirths, infant mortality and low birth weight during the pregnancy, 10 particularly in P. falciparum & P. vivax infection.11
Causes of malaria:-
Malaria is caused by P. falciparum, P. malariae, P. ovale, P. vivax in humans 12,13 P. falciparum is the most common species identified (~75%) followed by P. vivax (~20%).3 Although P. falciparum traditionally accounts for the majority of deaths,14 Recent evidence suggests that P. vivax malaria is associated with potentially life-threatening conditions about as often as with a diagnosis of P. falciparum infection.15 P. vivax proportionally is more common outside of Africa.16 P. knowlesi is a zoonotic species that causes malaria in macaques13, these are mostly of limited public health importance.
Life cycle of the malaria parasite:-
The life cycle of the malaria parasite (Plasmodium) is complicated and involves two hosts, humans and Anopheles mosquitoes. The disease is transmitted to humans when an infected Anopheles mosquito bites a person and injects the malaria parasites (sporozoites) into the blood. Sporozoites travel through the bloodstream to the liver, mature, and eventually infect the human red blood cells. While in red blood cells, the parasites again develop until a mosquito takes a blood meal from an infected human and ingests human red blood cells containing the parasites. Then the parasites reach the Anopheles mosquito's stomach and eventually invade the mosquito salivary glands. When an Anopheles mosquito bites a human, these sporozoites complete and repeat the complex Plasmodium life cycle. P. ovale and P. vivax can further complicate the cycle by producing dormant stages (h ypnozoites) that may not develop for weeks to years.
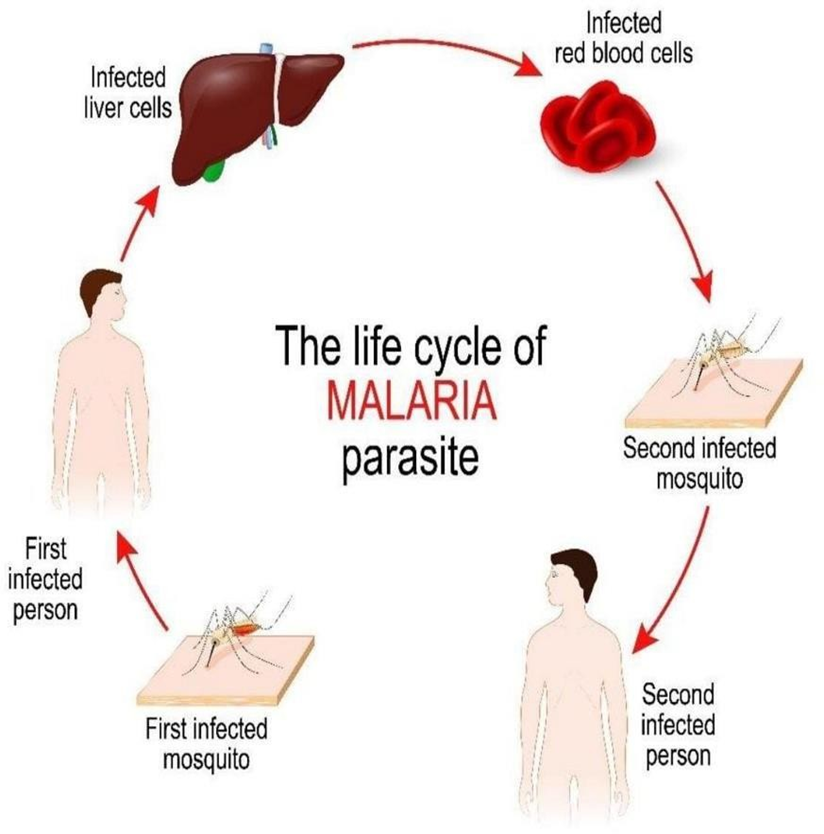
Fig 2. Life cycle of malaria parasite
Diagnosis of malaria:-
Diagnosis of malaria in non-endemic areas requires a high degree of suspicion, which might be elicited by any of the following: recent travel history, enlarged spleen, fever, low number of platelets in the blood, and higher-than-normal levels of bilirubin in the blood combined with a normal level of white blood cells.
Microscopy :-
Malaria is usually confirmed by the microscopic examination or microscopy of blood films or by antigen based rapid diagnostic tests (RDT).20,21 About 165 million blood films were microscopically examined for malaria in 2010.
Fig 3. Microscopy of malarial parasite
Classification of malaria :-
World Health Organization (WHO) classified Malaria into two types:-
The severe malaria is declared when any of the following criteria are present, otherwise it is considered as uncomplicated malaria.
Classification of malaria :-
10000 per µL in high-intensity World Health Organization (WHO) classified Malaria into two types:
The severe malaria is declared when any of the following criteria are present, otherwise it is considered as uncomplicated malaria.24
Methods of malaria prevention :-
There are various methods used to prevent malaria which are such as:
At present there is no vaccine available for malaria. Malaria occurs in an area where the combination of high human population density, high anopheles mosquito population density and high rates of transmission from humans to mosquitoes and from mosquitoes to humans available. If any of these is lowered sufficiently, the parasite will eventually disappear from that area. However, unless the parasite is eliminated from the whole world, it could become re-established if conditions revert to a combination that favours the parasite's reproduction. Furthermore, the cost per person of eliminating anopheles mosquitoes rises with decreasing population density, making it economically possible in some areas.26
Prevention of malaria may be more cost-effective than treatment of the disease in the long run, but the initial costs required are out of reach of many of the world's poorest people. China government announced a strategy to pursue malaria elimination which required small proportion of investment of public expenditure on health. Whereas a similar program in Tanzania would cost an estimated one-fifth of the public health budget.27
Vector control :
Vector control methods used to decrease malaria by reducing the levels of transmission by mosquitoes. For individual protection, the most effective vector control methods are
Insecticide-treated mosquito nets (ITNs) :
Mosquito nets help keep mosquitoes away from people and reduce infection rates and transmission of malaria. Nets are not a perfect barrier and are often treated with an insecticide designed to kill the mosquito before it has time to find a way past the net. Insecticide-treated nets are estimated to be twice as effective as untreated nets and offer greater than 70% protection compared with no net.32Between 2000 and 2008, the use of ITNs saved the lives of an estimated 250,000 infants in SubSaharan Africa.33 About 13% of households in SubSaharan countries own ITNs.34In 2000, 1.7 million (1.8%) African children living in stable malaria endemic conditions were protected by an ITN.
That number increased to 20.3 million (18.5%) African children using ITNs in 2007, leaving 89.6 million children unprotected.35An increased percentage of African households (31%) are estimated to own at least one ITN in 2008. Most nets are impregnated with pyrethroids, a class of insecticides with low toxicity. A recommended practice for usage is to hang a large "bed net" above the center of a bed to drape over it completely with the edges tucked in. Pyrethroid-treated nets and long-lasting insecticide-treated nets offer the best protection, and are most effective when used from dusk to dawn.36
Indoor residual spraying (IRS) :
Indoor residual spraying is the spraying of insecticides on the walls inside a home. After feeding, many mosquito rest on a nearby surface while digesting the bloodmeal, so if the walls of houses have been coated with insecticides, the resting mosquitoes can be killed before they can bite another person and transfer the malaria parasite.37 As of 2006, the World Health Organization recommends 12 insecticides in IRS operations, including DDT and the pyrethroids cyfluthrin and deltamethrin.38 This public health use of small amounts of DDT is permitted under the Stockholm Convention, which prohibits its agricultural use.39One problem with all forms of IRS is insecticide resistance. Mosquitoes affected by IRS tend to rest and live indoors, and due to the irritation caused by spraying, their descendants tend to rest and live outdoors, meaning that they are less affected by the IRS.
Medication of Malaria :
Each antimalarial drug is considered by chemical structure and mechanism of action.
Quinine and related agents :
Quinine is an alkaloid obtained from cinchona acts as a blood schizonticidal and weak gametocide against Plasmodium vivax and Plasmodium malariae. Quinine is accumulated in the food vacuoles of Plasmodium species, especially Plasmodium falciparum and inhibit the hemozoin biocrystallization, thus facilitating an aggregation of cytotoxic heme. Quinine is very effective and widely used in the treatment of acute cases of severe P. falciparum but it is less effective and more toxic than chloroquine. Mostly useful in areas where high level of resistance to chloroquine, mefloquine, and sulfa drug combinations with pyrimethamine. The World Health Organization recommendation for quinine by oral, intravenous or intramuscular routes, is 20 mg/kg first times and 10 mg/kg 8 hr for 5days where as in quinine sensitivity quinine may combined with doxycycline, tetracycline or clindamycin. Use of quinine is characterised by a frequently experienced syndrome called cinchonism. Tinnitus, rashes, vertigo, nausea, vomiting and abdominal pain are the most common symptoms. Quinine can cause hypoglycemia through its action of stimulating insulin secretion. This effect can be exaggerated in pregnancy and therefore additional care in administering and monitoring the dosage is essential. Repeated or over- dosage can result in renal failure and death through depression of the respiratory system. 05
Quinine related agents:
Quinimax and quinidine are the two most commonly used alkaloids. Quinimax is a combination of four alkaloids (quinine, quinidine, cinchoine and cinchonidine). Due to a synergistic action between the four cinchona derivatives this combination has been shown more effective than quinine. Quinidine is a distereoisomer of quinine with similar anti-malarial properties and recommended only for the treatment of severe cases of malaria. Warburg's Tincture was a febrifuge developed by Dr Carl Warburg in 1834, which included quinine as a key ingredient. Warburg's Tincture was highly regarded by many eminent medical professionals who considered it as being superior to quinine (e.g. Surgeon-General W. C. Maclean, Professor of Military Medicine at British Army Medical School, Netley). Warburg's Tincture appeared in Martindale: The complete drug reference from 1883 until about 1920. The formula was published in The Lancet 1875.49
Chloroquine :
Chloroquine was least expensive, best tested ,safest and the most widely used anti-malarial. It was the original prototype from which most methods of treatment are derived. The emergence of drug-resistant parasitic strains is rapidly decreasing its effectiveness. Now Chloroquine is suggested to used in combination with other antimalarial drugs to extend its effective usage. Popular drugs based on chloroquine phosphate (also called nivaquine) are Chloroquine FNA, Resochin and Dawaquin. Chloroquine is a 4- aminoquinolone compound which is believed to reach high concentrations in the vacuoles of the parasite and raises the internal pH. It controls the conversion of toxic heme to hemozoin by inhibiting the biocrystallization of hemozoin, thus poisoning the parasite through excess levels of toxicity. Children and adults should receive 25 mg of chloroquine per kg given over 3 days, recommended by the WHO, involves giving an initial dose of 10 mg/kg followed 6–8 hours later by 5 mg/kg, then 5 mg/kg on the following 2 days.
Amodiaquine :
Amodiaquine is a 4-aminoquinolone anti-malarial drug similar in structure and mechanism of action to chloroquine. Amodiaquine has tended to be administered in areas of chloroquine resistance while some patients prefer its tendency to cause less itching than chloroquine. Amodiaquine is now available in a combined formulation with artesunate (ASAQ) and is among the artemisinin-combination therapies recommended by the World Health Organisation. The drug should be given in doses between 25 mg/ kg and 35 mg/kg over 3 days in a similar method to that used in chloroquine administration
Pyrimethamine :
Pyrimethamine is used in the treatment of uncomplicated malaria, particularly in cases of chloroquine resistant P. falciparum strains when combined with sulfadoxine. It acts by inhibiting dihydrofolate reductase in the parasite thus preventing the biosynthesis of purines and pyrimidines, thereby halting the processes of DNA replication, cell division and reproduction. It acts primarily on the schizonts during the erythrocytic phase, and nowadays is only used in concert with a sulfonamide.
Proguanil :
Proguanil (chloroguanide) is a biguanide ,a synthetic pyrimidine derivative. It has many mechanisms of action but primarily is mediated through conversion to the active metabolite cycloguanil. This inhibits the malarial dihydrofolate reductase enzyme. It has a weak blood schizonticidal activity and is not recommended for therapy of acute infection. However it is useful in prophylaxis when combined with atovaquone or chloroquine (in areas where there is no chloroquine resistance). 3 mg/kg is the advised dosage per day, (hence approximate adult dosage is 200 mg). There are very few side effects to proguanil, with slight hair loss and mouth ulcers being occasionally reported following prophylactic use.
Sulfonamides:
Sulfadoxine and sulfamethoxypyridazine are specific inhibitors of the enzyme dihydropteroate synthetase in the tetrahydrofolate synthesis pathway of malaria parasites. Sulfonamides act on the schizont stages of the erythrocytic cycle. When sulfonamides are co-administration with the antifolate pyrimethamine, most commonly as fixed-dose sulfadoxine- pyrimethamine (Fansidar), produces synergistic effects sufficient to cure sensitive strains of malaria.
Mefloquine :
Mefloquine is a very potent blood schizonticide act by forming toxic heme complexes that damage parasitic food vacuoles. It is now used solely for the prevention of resistant strains of P. falciparum despite being effective against P. vivax, P. ovale and P. marlariae. Mefloquine is effective in prophylaxis and for acute therapy. It is now strictly used for resistant strains and is usually combined with Artesunate. Mefloquine is recommended as a dose of 15–25 mg/ kg, depending on the prevalence of mefloquine resistance. The increased dosage is associated with a much greater level of intolerance, most noticeably in young children; with the drug inducing vomiting and oesophagitis. It was not recommended for use during the first trimester, although considered safe during the second and third trimester.
NEED OF STUDY:-
Malaria remains one of the most serious public health challenges worldwide, especially in tropical and subtropical regions such as Africa, Southeast Asia, and parts of South America.
Children under five, pregnant women, and immunocompromised individuals are most vulnerable to malaria-related deaths.
The major challenge in malaria treatment is resistance to conventional drugs such as chloroquine, sulfadoxine– pyrimethamine, and partially to artemisinin.
The evolution of multidrug-resistant Plasmodium falciparum necessitates the discovery of new chemical entities and combination therapies
A detailed study of antimalarial drugs helps in understanding mechanisms of action, pharmacokinetics, and pharmacodynamics.
For pharmacy students, studying antimalarial drugs provides scientific understanding of drug development, resistance mechanisms, and clinical applications.
A detailed study of antimalarial drugs helps in understanding mechanisms of action, pharmacokinetics, and pharmacodynamics.
For pharmacy students, studying antimalarial drugs provides scientific understanding of drug development, resistance mechanisms, and clinical applications.
A detailed study of antimalarial drugs helps in understanding mechanisms of action, pharmacokinetics, and pharmacodynamics.
For pharmacy students, studying antimalarial drugs provides scientific understanding of drug development, resistance mechanisms, and clinical applications.
AIM:- A Review Report on Anti-Malarial Drugs .
OBJECTIVE :-
1. Understanding Malaria Etiology and Life Cycle:-
To study the causative agents of malaria (Plasmodium species) and the role of Anopheles mosquitoes in transmission.
2. Understanding Malaria Etiology and Life Cycle:-
3. Mechanism of Action:-
To study the biochemical and pharmacological mechanisms by which antimalarial drugs act on parasites.
4. Pharmacokinetics and Pharmacodynamics:-
To examine absorption, distribution, metabolism, and excretion (ADME) of key antimalarial drugs.
5. Drug Resistance Study:-
To study the emergence of drug resistance in Plasmodium falciparum and other species.
6. Recent Advances in Antimalarial Therapy:-
CONCLUSION:-
The combination of Arterolane and Piperaquine act as blood schizonticides with rapid clearance of parasitemia and most malaria-related symptoms, coupled with prevention of recrudescence. The combination provides high clinical efficacy as assessed by PCR corrected ACPR(Adequate Clinical and Parasitological Response), fever clearance time and parasite clearance time. Arterolane maleate and piperaquine phosphate was as well tolerated as artemether and lumefantrine, and had a similar safety profile. Arterolane maleate and Piperaquine phosphate is a synthetic drug and hence easier to manufacture with better predictability and reliability of supplies.
SUMMARY:-
Malaria is one of the most widespread infectious diseases, especially in tropical and subtropical regions. It is mainly caused by Plasmodium falciparum and Plasmodium vivax, transmitted by the female Anopheles mosquito. Antimalarial drugs play a key role in the prevention, control and treatment of malaria. Over the years, several antimalarial agents such as chloroquine, artemisinin derivatives, quinine, primaquine and combination therapies have been developed to reduce morbidity and mortality.
However, increasing drug resistance has become a major global challenge. Chloroquine-resistant P. falciparum has spread in many countries, leading to the development of Artemisinin-based Combination Therapies (ACTs), which are currently the most effective treatment. Continuous monitoring of drug efficacy, development of new molecules, and vaccine research are essential to overcome emerging resistance.
The review highlights the mechanisms of action of different antimalarial drugs, their therapeutic uses, side effects, resistance patterns and recent advancements. New research focuses on next-generation antimalarials, transmission-blocking agents and long-acting injectable formulations. Strengthening surveillance programs and improving clinical management can significantly contribute to malaria eradication efforts.
FUTURE SCOPE :-
REFERENCES


D. R. Gite, Raviraj Rathod, Shaikh Shahebaj, Krishna Pawar, Review on Antimalarial Drug, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 3720-3730. https://doi.org/10.5281/zenodo.18063278
 10.5281/zenodo.18063278
10.5281/zenodo.18063278
