College of Pharmaceutical Sciences, RIMT University, Mandi Govindgarh, Punjab, India
Hepatitis B virus (HBV) infection continues to be a major global health concern. Over 250 million people worldwide suffer from chronic hepatitis B (CHB), which can cause serious liver illnesses such as cirrhosis and hepatocellular carcinoma. Hepatitis B treatment has come a long way, with the main goals now being to stop the virus from replicating and to stop the illness from getting worse. The present hepatitis B treatment approaches are reviewed in this review article, with particular emphasis on the use of nucleoside analogues (NAs), such as entecavir and tenofovir, which are effective in suppressing the virus and enhancing long-term results. Novel therapeutic techniques, such as the use of pegylated interferon, immunomodulatory medicines, and therapeutic vaccinations, have been made possible by recent developments. Furthermore, developments in molecular biology have prompted the creation of next-generation antivirals, including RNA interference-based treatments, capsid assembly modulators, and entrance inhibitors, which target different phases of the HBV life cycle. New information regarding combination therapy's potential to establish a functional cure—defined as a persistent loss of HBsAg, the antigen associated with hepatitis B—is also covered. These novel therapies have the potential to change the way hepatitis B is managed, aiming to increase functional cure rates and eventually enhance patient outcomes. In an effort to find more effective and long-lasting treatments for hepatitis B, this study covers all of the available treatment options and looks at recent scientific developments.
The hepatitis B virus (HBV) is a global public health concern that affects approximately 300 million people with chronic HBV infection. Hepatocellular carcinoma (HCC) and liver cirrhosis are lifelong risks for these patients. Nucleos(t)ide analogues (NAs) and pegylated interferon alpha (Peg-IFN-) are the two groups of therapeutic drugs that are currently approved for the treatment of chronic HBV infection. These treatments can block or prevent this undesired progression. But each has its limitations. On the one hand, the oral, second-generation reverse transcriptase inhibitors that are analogues of nucleos(t)ides include entecavir, tenofovir disoproxil fumarate (TDF), and the newly licenced tenofovir alafenamide (TAF). Effectively suppressing HBV DNA levels, they have been shown to reverse liver fibrosis and even cirrhosis, prevent the disease from progressing to cirrhosis, and lower but not completely remove the risk of HCC [1]. It can spread by sexual contact, contact with infected blood or other bodily fluids (such as semen, vaginal secretions, or blood), and transmission from infected mothers to their foetuses [2]. Both symptomatic and asymptomatic infections can occur during the acute period. Either an acute infection resolves on its own or develops into a chronic infection. Chronic HBV infection is the main cause of hepatocellular carcinoma (HCC) and one of the main causes of hepatic cirrhosis. The World Health Organisation (WHO) reports that 887,000 individuals died from HBV-related causes in 2015, and over 250 million people are chronically infected [3]. The Western Pacific, African, and Southeast Asian countries have the highest rates of epidemic prevalence [4]. Baruch Samuel Blumberg discovered the hepatitis B surface antigen (HBsAg), formerly known as the "Australia antigen" (AusAg), in the serum of native Australians in 1965 [5]. Later research linked this antigen to viral hepatitis [6]. A "functional cure," which is defined as persistently undetectable levels of HBsAg and HBV DNA in serum, with or without sero conversion to hepatitis B surface antibodies (anti-HBs) following treatment completion, is the aim of the current therapeutic development. A better clinical state and a markedly lower risk of infection resurgence have been linked to this reduction. Serum HBV DNA, hepatitis B core antigen (HBcAg) and its antibody anti-HBc, hepatitis B e antigen (HBeAg), and anti-HBe antibody are additional significant HBV indicators [7-9]. In fact, HCC ranks third in terms of cancer mortality, and CHB infections are the primary cause of HCC globally. For the treatment of CHB, two primary groups of antiviral medications are currently licenced. Approximately 25% of patients may experience viral suppression when subcutaneously administered pegylated interferon-alpha (PegIFN-a) for 48 weeks; nevertheless, there are negative effects to this treatment. When taking medications with high antiviral potency and resistance barrier, such as entecavir or tenofovir, the administration of nucleoside analogues (NUC) results in a higher viral suppression in most patients [10,11]. Because cheaper medications have a lower barrier to resistance and have led to the selection of resistant strains, antiviral drug resistance is still a problem in many highly endemic nations. Healthcare management in these countries is also hampered by the need for long-term NUC administration. Because of the relatively good safety profile of NUC, long-term therapy is possible, preventing both the recurrence of liver injury and viral replication. Interferon (IFN) or NUC-based antiviral medication has been linked to a lower risk of HCC, but not its elimination, according to a number of cohort studies. It is still unclear which patient demographic benefits the most from these treatments due to the cohort variability in these studies regarding the length of the infection, the severity of the disease, and the length of treatment [12]. The primary clinical characteristic of a positive result is the decrease in serum small envelope antigen (HBsAg), which permits therapeutic cessation and is linked to a lower chance of developing HCC, particularly in cases where it manifests early in life. Unfortunately, only 10% of patients receiving current treatments achieve HBsAg clearance based on long-term patient follow-up [10,11]. The development of novel antiviral therapies that accomplish functional cure of the infection, rather than only viral suppression, is imperative to support the management of this lethal virus. This could help lower the cost of antiviral therapies over a limited period of time, improve drug accessibility for residents of highly endemic locations, and influence the development of HCC. HBV is a DNA virus that is not cytotoxic and is a member of the Hepadnaviridae family [13]. A covalently closed circular DNA (cccDNA) found in the nucleus of infected hepatocytes is essential for viral persistence. Viral mini-chromosomes are formed when cccDNA binds to his- tones. It also serves as the template for all viral RNA transcriptions, including those of the pre- genomic RNA (pgRNA) [14]. Nucleocapsids are employed for reverse transcription and packing of pgRNA, which is then used for various production or recycling to the nucleus for cccDNA maintenance. In order to regulate viral replication, host immune responses play a major role in the pathobiology of the infection. HBV has developed defences against innate and adaptive immune reactions so that it can cause long-lasting infections [15]. This could hinder immune evasion and have consequences for the creation of a more effective treatment. The scientific community has summarised the following definitions for an "HBV cure" based on current un- derstanding [16].
HBV Replication Cycle
1. Virion Structure and Genome
Dane and associates identified HBV particles, commonly referred to as Dane particles (Figure 1A), for the first time in 1970 [17]. They have a 42 nm diameter and a spherical form. They are made up of an exterior envelope that surrounds the viral nucleocapsid and is a host-derived lipid bilayer that contains three distinct sized HBV surface antigens (HBsAg or HBs): large (L- HBs), medium (M-HBs), and small (S-HBs). The icosahedral nucleocapsid, measuring 27 nm in diameter, contains the viral DNA polymerase (P), the viral DNA genome, and the HBV core protein (HBcAg) [18,19]. The virus also secretes a variety of faulty particles, such as subviral lipid particles bearing the viral surface antigens and enclosed nucleocapsids that are either empty or contain defective immature genomes (Figure 1B). Subviral particles serve a crucial function in inhibiting antibody responses to the virus and are secreted at levels thousands of times greater than those of the infectious virions [20].
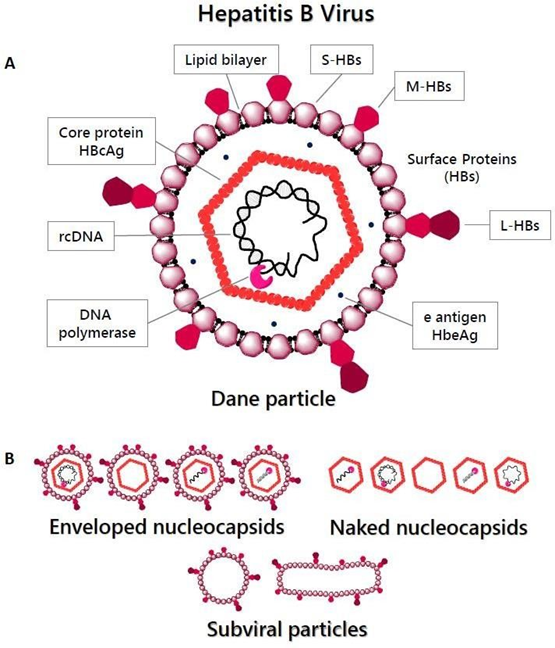
Figure 1. Hepatitis B Virus particles. (A) HBV virion that is infectious (Dane particle). The HBV relaxed circular DNA (rcDNA), the viral DNA polymerase (P), and the core protein (HBcAg) are found within the nucleocapsid, which is surrounded by a lipid envelope that car- ries three different types of surface proteins: small (S-HBs), medium (M-HBs), and large (L- HBs). (B) HBV particles that are not infectious; subviral particles; nucleocapsids that are exposed; and encapsulated nucleocapsids that contain immature or faulty DNA/RNA.
The 3.2 kb circular, partially double-stranded DNA known as relaxed circular DNA, or rcDNA, makes up the HBV genome. While the positive (+) DNA strand is imperfect and has a variable-size 3′ end and a fixed 5′ end, the negative-sense, non-coding DNA strand is com- plete and complementary to the mRNA transcripts. These are translated into seven useful pro- teins after being transcribed into five different-length RNA transcripts. ORF-C yields HBcAg, ORF preC + C yields HBeAg, ORF P yields DNA polymerase, and ORF X yields HBV X protein (HBx). The L-HBs, M-HBs, and S-HBs envelope proteins (pre-S1 + pre-S2 + S, pre-S2 + S, or S, respectively) are encoded by ORF S due to its many in-frame start codons [21–23]. Because of the HBV genome's compact structure, almost two thirds of its nucleo- tides encode several functional elements [24,25]. The P and S genes have the greatest gene overlap of any known animal virus, spanning over 1000 nucleotides.
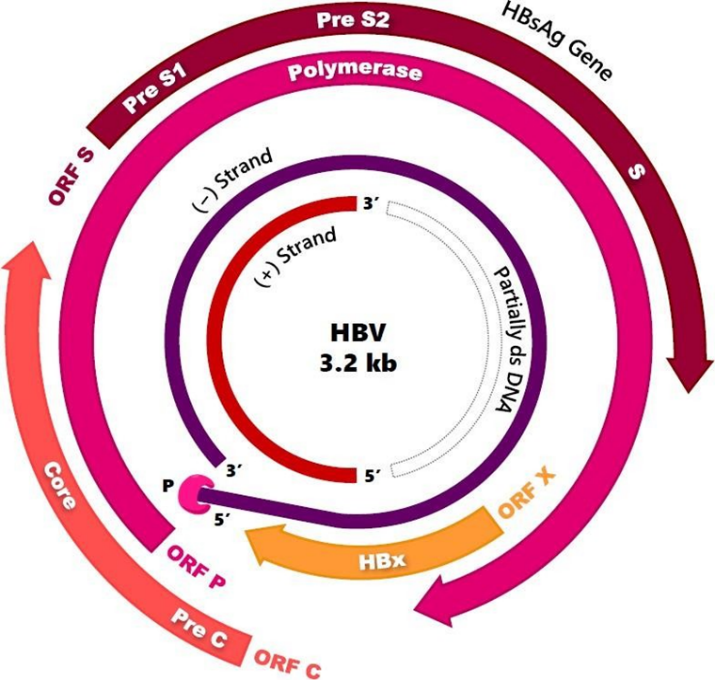
Figure 2. DNA of the hepatitis B virus. Relaxed circular DNA (rcDNA) that is partially double-stranded and has four overlapping open reading frames (ORFs).
2. Viral Entry
Heparan sulphate proteoglycans (HSPGs) are cell-surface receptors that the HBV virion attaches to through non-specific and low-affinity interactions. Following this, the pre-S1 domain of L-HBsAg is recognised and attached by the Na (+)-taurocholate co-transporting polypeptide (NTCP), which acts as a high affinity receptor for this purpose. Hepatitis D virus (HDV) entrance receptor NTCP is a liver-specific peptide that facilitates bile salt uptake into hepatocytes [26,27]. The viral endocytosis is caused by interactions between HBV and NTCP (Figure 3). Recent research indicates that the HBV entrance is facilitated by a complex that forms between NTCP and the epidermal growth factor receptor (EGFR) [28]. Owing to its intricate structure, NTCP is prone to oligomerization, which appears to have an impact on the internalisation of the virus within the cell. The nuclear pore complexes facilitate the entry of the nucleocapsid into the cytoplasm, uncoating, and subsequent transport of the rcDNA to the nucleus [29].
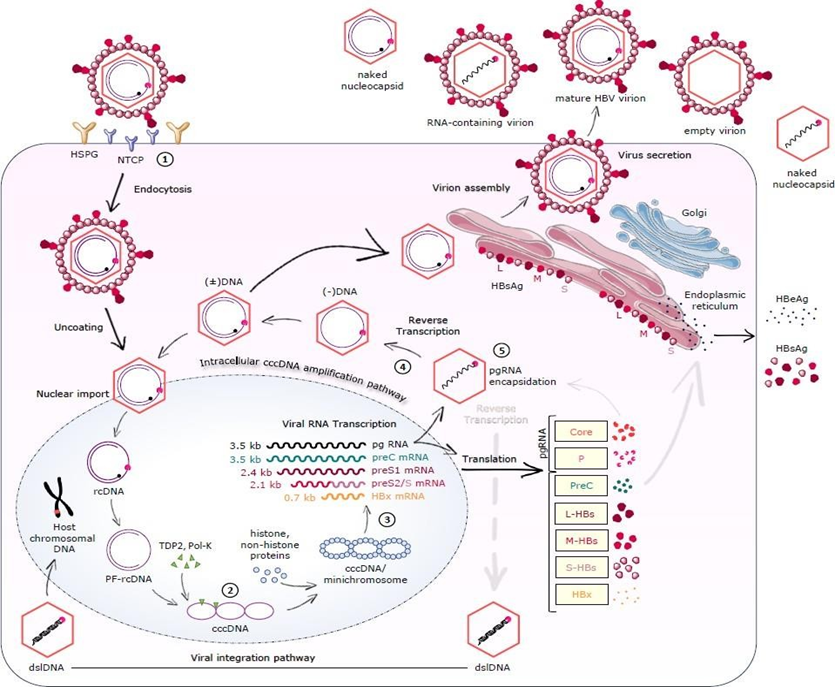
Figure 3. Main features of the hepatitis B virus replication cycle and potential therapeutic targets.
(1) HBV entry inhibitors. Lipopeptides mimicking the pre-S1 region of HBV, monoclonal antibodies, and other small molecules under evaluation.
(2) Targeting cccDNA. Damage and destruction of cccDNA via sequence-specific nucleases. Direct targeting of the HBx protein.
(3) RNA interference. Small interfering RNAs (siRNAs), antisense oligonucleotides (ASOs).
(4) HBV polymerase inhibitors. Reverse transcriptase inhibitors (nucleos(t)ide analogues) are part of the current treatment. RNaseH inhibitors are in preclinical evaluation. (5) Nucleocapsid assembly inhibitors or modulators can affect HBV capsid formation, reverse transcription, and pgRNA encapsidation. NTCP; Na(+) taurocholate co-transporting polypeptide, HSPG; heparan sulfate proteoglycan, rc-DNA; relaxed circular DNA, PF-rcDNA; protein-free rcDNA, cccDNA; covalently closed circular DNA, pgRNA; pregenomic RNA, preC; precore, mRNA; messenger RNA, P; polymerase, L-HBs; large hepatitis B surface protein, M-HBs; middle hepatitis B surface protein, S-HBs; small hepatitis B surface protein, HBx; hepatitis B X protein, HBsAg; hepatitis B surface antigen, HBeAg; hepatitis B e antigen, dslDNA; double-stranded linear DNA.
3. cccDNA Formation/Maintenance
The nucleus contains the episomal covalently closed circular DNA (cccDNA), which is formed by many cellular processes repairing the HBV rcDNA (Figure 3). The P protein of the virus, which is attached to the 5′ end of the DNA strand with minus polarity, [30The process involves the removal of the RNA primer attached to the 5′-end of the plus DNA strand, leaving a protein free rcDNA (PF-rcDNA), and the filling and circularization of the gaps in both strands to form the cccDNA. One cellular factor thought to be involved in this process is the DNA repair enzyme tyrosyl-DNA phosphodiesterase 2 (TDP2), which is thought to break the phosphodiesterase bond between the HBV P and the rcDNA [31,32]. Flap endonuclease 1 (FEN1) is an additional enzyme that degrades the RNA primer at the 5′-end of the minus strand. Following the removal of the proteins, other host enzymes like DNA ligases (LIG1 and LIG3), topoisomerases I and II (TOP1 and TOP2), and DNA polymerases (κ and α) fill in the strands and perform DNA repair [33]. It is unclear which of these components work in an infected liver, though there is significant functional redundancy among them. The viral RNA transcription template is the cccDNA. Many biological components, including the APOBEC3 protein family, which causes cccDNA degradation, control the stability of cccDNA [34,35]. After receiving nucleos(t)ide analogue therapy for over a year, the cccDNA shows only a little decline of approximately 1 log10 following antiviral therapy [36]. But in HepG2 cells, the half-life of cccDNA has only been found to be about 40 days [37]. Our research on cccDNA replacement during the therapy's withdrawal-induced reversion of nucleoside analogue resistance suggests that the liver's cccDNA half-life is 16–28 weeks.
APPROVED THERAPIES FOR TREATMENT OF CHRONIC HEPATITIS B
The FDA has approved seven medications to treat CHB: entecavir, lamivudine, adefovir, peginterferon alfa-2a, telbivudine, and tenofovir. Although interferon-based therapy has a set length of treatment, its use is constrained by significant side effects and poor tolerability in certain patients. With continued use, oral nucleoside ⁄ nucleotide treatment may cause the formation of antiviral medication resistance. When choosing the right treatment, it's important to take into account any previous medications used to treat CHB and look for signs of possible cross resistance. The potency and effectiveness of entecavir and telbivudine will be adversely affected by lamivudine resistance, which has been shown to reach up to 75% after five years of treatment. Lamivudine is no longer utilised as a first-line treatment due to its low genetic barrier to resistance. Similarly, reaching undetectable HBV DNA by week 24 of medication is a prerequisite for using telbivudine. Patients who do not reach this milestone by week 24 have a telbivudine resistance rate of 22% overall for HBeAg-positive patients and 9% overall for HBeAg-negative patients [38,39]. After reaching this goal, the crucial trial's ongoing viral suppression lasted until week 96 of treatment [40].
1. Peginterferon alfa-2a
Because of peginterferon alfa-2a's better pharmacokinetic qualities, easier injection schedule, more convenient dosage schedule, and equivalent or better efficacy, it has replaced regular interferon alfa-2b [41]. After a year of therapy, pegylated interferon continues to yield the highest rate of off-treatment sustained response. Following 48 weeks of Peginterferon alfa-2a therapy, there is a 27% HBeAg seroconversion rate and a 25% HBV DNA loss rate. The rates of HBeAg seroconversion rose to 32% six months after medication was stopped. After a year of treatment and six months of post-treatment follow-up, 4–6% of patients showed loss of HBsAg and the emergence of anti-HBs [42-44]. Twelve to sixty-five percent of patients lost HBsAg within five years of HBeAg loss, even after interferon medication was stopped [45,46]. Inducing long-term remission after ceasing medication is linked to achieving early virological response, which is defined as suppression to levels below 105 copies/mL or a decline in serum HBV DNA of more than 2 log10 during the first two weeks of therapy. [47,48]. Lamivudine added to peginterferon alfa-2a therapy leads in a more vigorous suppression of the HBV DNA during treatment, but it has no influence on serological response rates in HBeAg-positive and HBeAg-negative CHB patients [42,43]. The distribution of hepatitis B genotypes varies by nation and affects how well peginterferon therapy works [49]. While genotypes A and D are primarily found in Europe and India, genotypes B and C are more frequently found in Asia. In countries around the Mediterranean, genotype D is prevalent [50-52]. In the US, genotypes A and C are most common [53]. Only Africa and Central and South America, respectively, are home to genotypes E and F. When it comes to responsiveness, genotypes A and B outperform genotypes C and D [39]. The interferon HBV treatment index was developed from analysis of 542 individuals who were treated with peginterferon for 48 weeks. In individuals who have not yet received interferon, this treatment index provides an estimated likelihood of a sustained response based on the HBV genotype (A–D), ALT level, HBV DNA level, gender, and age. Peginterferon therapy is most suited for those with genotype A who have either HBV DNA or ALT >2 times the ULN [44].
2. Lamivudine
The FDA originally approved lamivudine in the US in 1998. Because superior oral medications with a stronger genetic barrier to resistance, like entecavir and tenofovir, are now available, their use is less widespread. Lamivudine medication for a year is linked to a 16–18% rate of HBeAg seroconversion; [39,54]. Five years of therapy results in a 50% increase in the HBeAg seroconversion rate [55,56]. After a year of treatment, lamivudine therapy also suppresses HBV DNA in 60–70% of HBeAg-negative CHB patients [39]. Regardless of the HBeAg status, the durability of response is less than that of interferon therapy and has been found to range be- tween 50% and 80% for HBeAg-positive CHB patients and 20–25% for HBeAg-negative CHB patients [57]. In HBeAg positive CHB, treatment can be continued for an extra six months or more to further cement the response's durability [58]. Lamivudine treatment for HBV has been demonstrated to reduce the incidence of HCC and slow the rate of fibrosis development. Liaw et al. skilfully presented data from follow-up of 651 patients with advanced fibrosis, primarily Asians, who were randomly assigned to receive either lamivudine or placebo. The study's primary end point was time to disease progression (hepatic decompensation, hepatic encephalopathy, HCC, spontaneous bacterial peritonitis, variceal bleeding, or liver disease death). The study had to be stopped after a median duration of 32.4 months due to a significantly lower proportion of the lamivudine group reaching the end point compared with the placebo group (7.8% vs. 17.7%). The lamivudine group exhibited a lower risk of HCC (3.9% vs. 7.4%), an increase in Child-Pugh score, and a slower rate of disease progression than the placebo group [59]. These results show that even in individuals with severe cirrhosis or fibrosis, therapy directly improves clinical outcomes. Patients with HBeAg-negative CHB are often treated indefinitely because recurrence is common after stopping treatment, even in cases when undetectable HBV DNA is present [58,39]. Long-term usage of lamivudine is also linked to a significant risk of resistance development. After five years of treatment, resistance can occur in 65–70% of cases. By including adefovir, a nucleotide analogue, YMDD lamivudine resistance was successfully managed for the first time. The rate of mutation leading to adefovir resistance was similarly reduced by the combination method [58,39,60]. Additionally, recent results have demonstrated that tenofovir monotherapy is an effective treatment for the YMDD mutation [61].
3. Adefovir dipivoxil
Tenofovir, which was just approved, is taking the place of adefovir dipivoxil, which was the first nucleotide analogue to be approved by the FDA in 2002 for the treatment of CHB. In HBeAg-positive patients, adefovir therapy results in a 12% rate of HBeAg seroconversion and a 53% rate of histopathological improvement after a year [62,63]. In 91% of individuals, HBeAg seroconversion is maintained when it happens [58,39,60]. Similar to lamivudine, ade- fovir therapy is necessary for life in HBeAg-negative individuals, and resistance is a signifi- cant issue with prolonged adefovir use. Resistance development is associated with viraemia persistence during 48 weeks of treatment [64]. Resistance rates at 1, 2, 4, and 5 years of therapy have been reported to be 0%, 3%, 18%, and 29%. Given that tenofovir is more effective at attaining quick virological suppression, the usage of adefovir is decreasing [65].
4. Entecavir
Developed in 2005, Entecavir is a nucleoside analogue that is better than lamivudine for the treatment of chronic hepatitis B. At a dosage of 0.5 mg per day, it is a strong inhibitor of HBV polymerase, resulting in a 6.98 log10 copies/mL reduction in HBV DNA levels as opposed to a 5.4 log10 copies/mL reduction with lamivudine. Phase three research comparing entecavir to lamivudine demonstrated its superiority over the latter medication. Compared to patients who got lamivudine, those who received entecavir for 52 weeks showed better virological response, with HBV DNA <400 copies⁄mL (67% vs. 36%), histological improvement (72% vs. 62%) and normalisation of ALT (78% vs. 70%) [66]. However, entecavir and lamivudine did not differ in its ability to induce HBeAg seroconversion (21% vs. 18%). In HBeAg-negative patients, entecavir is likewise more effective than lamivudine; nevertheless, it must be taken continuously to sustain viral suppression and avoid recurrence [67,68]. Better virological sup- pression (91 vs. 73%) and improved histopathology (70 vs. 61%) are demonstrated with entecavir. Furthermore, examination of two trials involving patients who were on continuous entecavir for up to five years showed that 94% of patients still had HBV DNA <300 copies/mL after five years [69]. Even in individuals with cirrhosis, up to 96% of patients (mostly HBeAg- positive CHB) experienced histological improvement and 88% showed improvement in their fibrosis score following six years of entecavir medication [70]. It has also been demonstrated that within two weeks of treatment, entecavir outperforms ade fovir in terms of quickly establishing viral suppression. There was no difference in the rate of HBeAg loss (18% vs. 22%) and HBeAg sero conversion (15% vs. 22%) during a 48-week therapy with entecavir compared with adefovir, despite the fact that it was linked with a higher rate of HBV clearance (58% vs.19%) and ALT normalisation (76% vs. 63%) [71]. Entecavir has an extremely low rate of resistance and a high genetic barrier. In individuals who have never had nucleosides, the cumulative incidence rate of resistance after six years of therapy is still very low, at 1.2%. On the other hand, in individuals who are resistant to lamivudine, the rate of resistance rises from 6% after one year to 57% after six [72,73]. Additionally, HBsAg loss has been linked to entecavir therapy. This loss is linked to improved liver histology, a lower risk of HCC, and very low to undetectable HBV DNA levels [74,75]. In nucleoside nave HBeAg-positive patients, entecavir therapy for 48 weeks causes HBsAg loss in 1.7% of patients, while lamivudine therapy causes it in 1.1% of patients. Week 96 analysis of the same cohort showed that 3% of patients treated with lamivudine and 5% of patients treated with entecavir experienced HBsAg loss. Prognostic indicators for HBsAg loss included HBV genotype A or D, male gender, Caucasian race, and HBeAg seroconversion by week 24 [76]. At a median of 21 months and 30 months, respec- tively, the analysis of an ongoing multicentre Italian research involving 418 nucleoside-nave patients with CHB taking entecavir 0.5 mg daily found 6% and 19% cumulative probability of HBsAg decrease [77]. Entecavir medication did not significantly affect HBsAgloss in HBeAg- negative CHB patients, in contrast to its impact on HBeAg positive CHB [78].
5. Telbivudine
The most recent nucleoside analogue to be authorised by the FDA for the treatment of chronic hepatitis B is telbivudine. Entecavir was found to be superior to lamivudine in phase III randomised research that included patients with CHB who were HBeAg-positive and HBeAg- negative. At one and two years, respectively, the percentage of HBeAg seroconversion with telbivudine therapy was 22% and 30% in HBeAg-positive CHB patients. In 60% and 56% of HBeAg-positive individuals, viral suppression was restricted to HBV DNA levels of less than 300 copies/mL following one and two years of therapy. At one and two years of treatment, HBV suppression was observed in 88% and 82% of HBeAg-negative CHB patients, respec- tively [79,80]. Whether patients were treated with telbivudine initially or moved from adefovir to telbivudine, telbivudine is also superior to adefovir in achieving early viral suppression at week 24 in HBeAg-positive patients (39% vs. 12%) [81]. Better rates of HBeAg seroconversion, ALT normalisation, and viral suppression were the outcomes of this early virological suppression. Additionally, 186 Asian pregnant women with HBV DNA >6,000,000,000 copies/mL have been investigated with telbivudine. The outcomes of 92 women who did not receive antiviral medication were compared with those of 94 women who got telbivudine be- tween weeks 20 and 32 of pregnancy and for four weeks following delivery. Up until postpartum week 28, women with active hepatitis B continued their medication. Within 24 hours of birth, all newborns were given hepatitis B immune globulin (HBIG). Compared to the control group, the telbivudine arm produced better results: 30% of women had undetectable HBV DNA at delivery, compared to 0%, and 6.32% of newborns had HBsAg positivity, as opposed to 30.43%. At week 28, the telbivudine arm of this trial showed that 2.11% of newborns were HBsAg positive or had detectable HBV DNA, compared to 13% in the control group, according to the intention-to-treat analysis (missing = failure). Only the neonates with HBsAg positivity had detectable levels of serum HBV DNA. Compared to 8.7% in the control group, none of the newborns born to women in the therapy group tested positive for HBsAg. In comparison to women in the control group, who had an ALT >2–5 ULN, treated women experienced fewer hepatitis flares (7.5% vs. 18.5%). The newborns in the two groups did not have any congenital abnormalities or differ in their outcomes [82].
6. Tenofovir
The FDA authorised tenofovir as the most recent nucleotide analogue in 2008. In addition to being more effective than adefovir, it is structurally related. When HBeAg-positive CHB pa- tients received tenofovir therapy for 48 weeks as opposed to adefovir therapy, more patients experienced viral suppression, which is defined as < 400 copies/mL (76% vs. 13%), ALT nor- malization (68% vs. 54%), histological improvement (67% vs. 12%), and HBsAg loss (3.2% vs. 0%) [83]. After four years of medication, HBeAg-positive and HBeAg-negative CHB showed a 100% and 99% viral suppression (HBV DNA < 400 copies/mL), respectively, ac- cording to data from the tenofovir trials. This demonstrated an exceptional durability of re- sponse [84,85]. A sub-analysis of the 145 Asian patients showed that identical efficacy (97%) could be attained in achieving viral suppression, which is defined as HBV PCR < 400 cop- ies/mL. Moreover, 41% of patients saw HBeAg loss after four years of tenofovir therapy, and 29% experienced HBeAg seroconversion.86 By week 192, 10% of patients had lost HbsAg and 7.5% had sero-converted to anti-HBs, according to the Kaplan-Meier estimate [85]. In a phase III trial of HBeAg-negative patients, tenofovir outperformed adefovir in terms of higher viral suppression (93% vs. 63%), an improved inflammatory score, and viral suppression (71% vs. 49%). After four years of follow-up, no tenofovir resistance has been found [83].
7. Emtricitabine
Though structurally similar to lamivudine, emtricitabine is not presently licenced for the treatment of chronic hepatitis B. Like lamivudine, its intermediate genetic barrier to resistance restricts its use as a monotherapy for CHB. After receiving emtricitabine for two years, there is a 13% chance that resistance will arise [86]. Emtricitabine may affect the use of entecavir in the future since it carries the same resistance mutation (M204V⁄I L180M) as lamivudine. Truvada (tenofovir 300 mg + emtricitabine 200 mg) is the kind of tenofovir therapy that is presently being studied as an adjunctive treatment. Tenofovir and Truvada (Gilead Sciences, Foster City, CA, USA) were equally effective at suppressing virus loads to less than 400 cop- ies/mL after 24 weeks of therapy, according to a randomised trial conducted in patients who had previously used adefovir.89 Patients in the randomised group were transferred to open label Truvada after 24 weeks if they had detectable HBV DNA, which was defined as >400 copies/mL. According to intention-to-treat analysis, 81% of patients in each therapy group had blood HBV DNA < 400 copies/mL by week 48 [87]. The effectiveness of tenofovir or Truvada was unaffected by the presence of baseline lamivudine or adefovir resistance. At week 168 of treatment, tenofovir and Truvada both achieved 82% viral suppression, regardless of the presence of pre-existing adefovir or lamivudine-resistant mutations [88].
Treatment of specific populations infected with hepatitis B virus
As was already established, a significant therapeutic consideration is a family history of HBV- related cirrhosis or HCC. Treatment for cirrhosis or HCC should generally be successful; this has been mentioned previously. This review highlights the following groups.
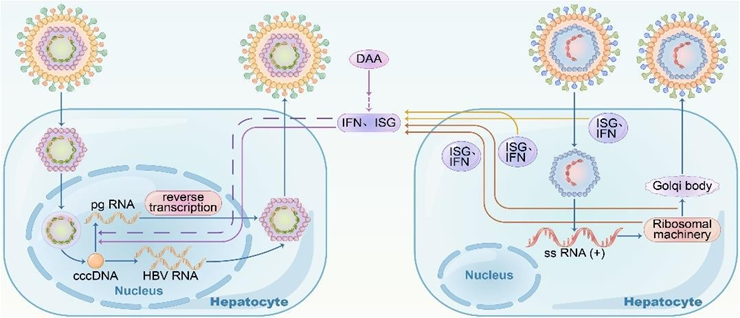
Figure 4: Coinfection of the hepatitis B and hepatitis C viruses (HBV–HCV). When HBV and HCV co- infected, HBV RNA increased and there was no direct virus-virus interference; HBV replication was inhibited by the interferon response that HCV replication produced.
Coinfection
Superinfection is quite prevalent because the hepatitis B, hepatitis C, and human immunodeficiency viruses (HIV) all share similar routes of transmission. Joint HBV/HCV infection in- creases the risk of developing cirrhosis, persistent and fulminant hepatitis, and hepatic cancer (HCC) [89,90]. Every patient who tests positive for HBsAg should have an anti-HCV screening, particularly those who have high infection risks, such as those who inject drugs or are gay men. HBV replication in coexisting HBV and HCV cases is different from HBV mono-infection and is inhibited by the IFN (interferon) response from HCV replication as opposed to direct viral interactions. Every patient who tests positive for HBsAg should have an anti-HCV screening, particularly those who have high infection risks, such as those who inject drugs or are gay men. HBV replication in coexisting HBV and HCV cases is different from HBV mono-infection and is inhibited by the IFN (interferon) response from HCV replication as opposed to direct viral interactions [91,92]. HBV infection has no effect on HCV replication in cases of HBV- HCV superinfection. According to Cheng et al., HBV suppression was caused by HCV-mediated ISG (interferon-stimulated gene) expression; however, when ISG expression was inhibited, both HBV and HCV viruses displayed high levels of replication. CXCL10 might indicate a strong IFN response in HBV-HCV coinfection and HCV elimination. Nearly all guidelines recommend treating CHB patients who test positive for HCV with direct-acting antivirals (DAAs) in addition to anti-HBV medication in clinical practice (Figure 4) In addition, patients who receive DAA and are HBsAg-negative and hepatitis virus core antigen-positive (anti-HBc+) must have their serum HBsAg and HBV DNA levels checked every month during the treatment in case of HBV reactivation. Regardless of CD4 count, early ARVT initiation is advised in patients of HIV-HBV coinfection. The therapy included two types of anti- HBV medications to prevent HIV resistance to Nas, according the 2019 China guidelines [93].
Pregnancy-related situations
It is strongly advised that women of childbearing age who are contemplating a pregnancy or who are already pregnant get screened for HBsAg. Tenofovir disoproxil fumarate (TDF) is the recommended drug for antiviral prophylaxis when the patient meets the therapy criteria. NAs can be discontinued immediately or within three months after delivery with prompt monitoring if they are used to prevent HBV perinatal transmission in a pregnant woman at weeks 24–28 of gestation with normal ALT but positive HBeAg and high levels of viremia (HBVDNA > 2 105 IU/mL) [94].
Treatment of chronic hepatitis B in children
The rate of HBV infection was reduced in young Chinese people who received the HBV vac- cination. Recent research has shown that the horizontal transmission of HBV in early children is gradually rising, with family members potentially serving as the primary source of infection. Depending on the age of the young person, possible therapy choices include NAs and interferons [95].
Initial management of hepatitis B infection
Many immunocompetent persons have self-limiting acute HBV infections, with supportive care being provided. A thorough history and physical examination to check for cirrhosis symptoms, alcohol and metabolic risk factors, and a family history of hepatocellular carcinoma should be part of the initial therapy plan for patients with chronic infections. Regular laboratory testing should include measures of HBV replication (HBeAg/antiHBe, HBV DNA quantitation), tests for coinfection with HCV, HDV, and HIV, evaluation of HAV immunity to deter- mine need for vaccination, and assessment of liver disease activity and function (complete blood count, aspartate aminotransferase, ALT, total Bili, alkaline phosphatase, albumin, inter- national normalised ratio). Patients should be informed about the need of long-term monitoring, especially considering the possibility of hepatocellular carcinoma, as well as strategies to stop the spread of the condition and stop additional liver damage (such as avoiding alcohol and potentially hepatotoxic drugs or supplements). Every six months, patients who are over 40, have cirrhosis, or have a family history of hepatocellular carcinoma should have α-fetoprotein tests and ultrasonography done. By inhibiting HBV replication and hepatic inflammation and halting the development of cirrhosis and hepatocellular cancer, antiviral treatment aims to reduce morbidity and death. The effects of antiviral therapy include ALT returning to normal, HBV DNA suppression, potential loss of HBeAg and seroconversion to anti-HBe, potential loss of HBsAg and seroconversion to anti-HBs, and improvements in histology with less inflammation and fibrosis. Seven antiviral medications have been licenced by the Food and Drug Administration to treat chronic HBV: telbivudine, pegylated interferon-a2α (peg-IFN), lamiv- udine (LAM), adefovir, entecavir (ETV), lamivudine (LAM), and adefovir (TDF). TDF, ETV, and pegIFN are the most often utilised first-line agents among them [96].
IFN monotherapy
Peg-IFN possesses both antiviral and immunomodulatory properties. Peg-IFN is better than normal IFN-− due to its more convenient dosage schedule of once weekly subcutaneous injections, even though the efficacy is not much different. Those with low HBV DNA levels, high ALT, and HBV genotype A or B rather than C or D, as well as those without severe illness, are the best candidates for peg-IFN. Peg-IFN has several benefits, including as a limited treatment duration, no resistance development, and increased rates of anti-HBe and anti-HBs seroconversion after a year of therapy
Poor tolerability and numerous side effects (such as flu-like symptoms, exhaustion, anorexia, nausea, weight loss, hair loss, emotional instability, depression, worsening of autoimmune dis- ease, and hypothyroidism) are drawbacks. Additionally, weekly subcutaneous injections are required, and the antiviral effect is only moderate. A history of suicidal thoughts or attempts, untreated autoimmune or mental health issues, severe leukopenia or thrombocytopenia, coexisting severe systemic illnesses, decompensated cirrhosis, and pregnancy are among the factors that preclude the use of peg-IFN [97-99].
NA monotherapy:
Both TDF and ETV are non-steroidal anti-HBV DNA polymerase inhibitors (NAs) that inhibit the dual function HBV DNA polymerase. Oral TDF is given at a dose of 300 mg daily, while oral ETV is given at a dose of 0.5 mg daily in individuals who have not previously received LAM treatment and 1.0 mg daily in individuals who are refractory/resistant to LAM. Adefovir, telbivudine, and LAM are not advised due to their lower barrier to resistance and limited potency. Overall, all NAs have an excellent safety profile for a wide range of people with chronic hepatitis B, and rare side effects are reported [100]. Rare side effects of TDF include proximal tubular acidosis, renal insufficiency, Fanconi's syndrome, and decreased bone density, especially in youngsters, for whom the medication is not recommended [101-104In individuals with renal impairment, the dosage of TDF needs to be modified based on creatinine clearance. The following mild to moderate adverse effects are associated with ETV: headache, upper respiratory tract infection, cough, nasopharyngitis, exhaustion, and upper stomach pain [105]. ETV should be used cautiously in patients with decompensated liver disease since severe lactic acidosis has been described in a case series of individuals with advanced cirrhosis (MELD score≥20). Additionally, ETV needs to be modified for creatinine clearance [106]. For patients with decompensated liver disease, those on immunosuppressive treatment, and those with other contraindications to or refusals of peg-IFN, TDF or ETV represent the only available therapeutic choices. After a 12-month consolidation period and proven HBeAg seroconversion with undetectable HBV DNA, therapy for HBeAg + patients can be discontinued. Nevertheless, close observation for relapse is necessary after stopping therapy. Long-term therapy is necessary for HBeAg − patients until HBsAg loss is verified. Strong antiviral action (viral suppression in 495 percent of patients over 5 years with fibrosis regression and avoidance of cirrhosis) is one of NAs' benefits [107-109]. oral administration, low adverse effects, and high tolerance. Indefinite therapy duration, especially in HBeAg− individuals, resistance risk, and unclear long- term safety are drawbacks. Thankfully, there hasn't been much of a chance of medication re- sistance up to now (1.2% with ETV after 6 years and 0% with TDF after 5 years) [110,111].
Combination therapy:
De novo combination therapy with two NAs does not confer any additional benefit. Further- more, the AASLD does not currently suggest the combination of peg-IFN with NAs because it has not resulted in increased rates of off-treatment serological or virological responses [112,113]. However, a recent randomised controlled trial has demonstrated that compared to patients receiving TDF (0%) or peg-IFN alone (2.8%) or a shorter course of peg-IFN (16 weeks) with 48 weeks of TDF (2.8%), a significantly higher proportion of patients receiving TDF plus peg-IFN for 48 weeks had HBsAg loss (9.1%) [114].
Prevention of HBV:
Treatment is much more complicated than prevention, especially when it comes to HBV, which typically requires lifelong care. In addition to preventing infection through screening of the blood supply and widespread precautions, immunisation is the most crucial way to lower the burden of disease worldwide. Adult vaccination is advised in high-risk groups who are susceptible to infection through sexual contact (such as men who have sex with men, people who have multiple sexual partners, and those seeking evaluation and treatment for STDs). Alternatively, vaccination is advised in individuals who are susceptible to infection through percutaneous or mucosal blood exposure (such as injectable drug users, household contacts of HBsAg+ pa- tients, patients receiving haemodialysis, institutionalised patients, healthcare professionals, and public safety personnel). Moreover, vaccination is advised for those with HIV infection, chronic liver illness, and travellers from other countries to areas where HBV infection is highly or moderately prevalent [115]. For healthcare professionals who are not immune to the HBV virus, postexposure prophylaxis with the hepatitis B vaccine and/or hepatitis B immune globulin is also advised. It is advised that children receive vaccinations as part of the routine child- hood immunisation programme. In 184 out of 196 countries worldwide, universal immunisation of all children is now possible, 35 years after the development of a safe and effective vaccine. 82% of people worldwide are believed to have received all three doses of the vaccination [116].
How do we cure HBV?
Given the durability and latency of cccDNA and the fact that HBV DNA replication is inde- pendent of protein (HBsAg) synthesis, a functional cure for HBV presents particular difficul- ties. In this sense, DNA suppression can be achieved using polymerase inhibitors without HBsAg being lost. A good functional cure for HBV (HBsAg loss, sAb seroconversion) will probably need a multipronged, Mult mechanism approach, involving possible strategies to at- tack both the virus and the host, because HBsAg can subvert the host immune response pro- duction [117]. It is outside the purview of this review to analyse every unique strategy for a viral target; however, we will touch on the main strategies in brief below. HBV capsid inhibi- tors, small interfering RNA directed against viral mRNA, and cccDNA targeting techniques are examples of direct virologic approaches. Because it is necessary for the packaging of the HBV genome, reverse transcription, intracellular trafficking, maintenance of cccDNA, and suppression of host innate immune responses, the HBV capsid has multiple functions. It is therefore a desirable target for HBV treatments. The capsid inhibitors NVR 3-778, GLS-4, and derivatives of phenyl propenamide are among those under evaluation. HBV RNA, proteins, and DNA concentrations might be reduced by small interfering RNAs targeted against con- served HBV RNA sequences. In order to accomplish this, a phase 2 experiment is presently assessing the HBV small interfering RNA ARC-520. cccDNA targeting strategies include physical elimination of cccDNA (e.g., zinc-finger, transcription activator like effector nucleases or TALEN, CRISPR/Cas9 nucleases), prevention of cccDNA formation (e.g., disubstituted sulphonamide DSS), and silencing of cccDNA transcription. Viral or cellular factors con- tributing to cccDNA stability/formation (e.g., APOBEC3A, B agonists) or inhibition of cccDNA [118-121]. Entry inhibitors, morphogenesis inhibitors (glucosidase inhibitors), secretion inhibitors, and epigenetic modifiers (sirtuin inhibitors, such as sirtinol) are examples of indirect acting host target inhibitors (Rep 9AC). One potential avenue for treatment is to sup- press the sodium taurocholate co-transporting polypeptide receptor, which allows HBV/HDV to infect hepatocytes. Examples of such medicines are ezetimibe, cyclosporine A, and myrcludex B [122]. Despite this, there might be restrictions on the therapeutic effects of bile salt transport inhibition. Aiming to influence both innate and adaptive immune responses are immunomodulatory techniques. IFN-α, TLR7 agonists, and STING agonists are examples of innate targets [123,124].
Challenges and Future Perspectives:
The management of hepatitis B presents a few difficulties even with notable progress. Hepatitis B surface antigen (HBsAg) loss is still uncommon despite the fact that current medications, mainly nucleos(t)ide analogues (NAs), significantly inhibit viral replication but rarely achieve complete viral eradication. Drug-resistant HBV strains can result with long-term NA use, and interferon-based therapies frequently have restricting adverse effects. In low- resource areas, access to and the expense of modern medicines present major obstacles, and many patients receive a diagnosis only after their disease has progressed due to insufficient early identification and monitoring.
There is hope for the future of hepatitis B therapy since new and creative methods are being researched. Novel antiviral drugs, such as RNA interference-based treatments, capsid assembly modulators, and entrance inhibitors, that target distinct stages of the HBV life cycle are currently under development. The goal of combination therapy combining immunomodulatory medications, novel antivirals, and NAs is to improve efficacy and raise the percentage of functional cures. To strengthen the immune response to HBV, researchers are looking into therapeutic vaccinations and immunotherapies, such as T-cell therapies and checkpoint inhibitors. Treatment could be optimised by personalised medicine techniques based on unique patient characteristics. It is essential to bolster global health programmes in order to enhance access to preventative care, treatment, and diagnostics, especially in high-burden areas. In order to reach a functional cure and lessen the incidence of hepatitis B worldwide, further research and development could lead to the creation of safer, more effective, and more widely available medicines.
CONCLUSION
Hepatitis B treatment has come a long way, but there are still many obstacles to overcome. Although available treatments, particularly nucleos(t)ide analogues, successfully inhibit viral reproduction, total viral eradication is not common and problems with medication resistance, side effects, and accessibility persist in impeding progress. Nonetheless, new antiviral medications, combination treatments, therapeutic vaccines, and immunotherapies appear to have the potential to revolutionise hepatitis B treatment in terms of both management and results. To maximise care and guarantee wider access, especially in high-burden areas, personalised medicine and enhanced global health initiatives are crucial. Seeking a functional treatment to lessen the effects of hepatitis B and enhance patient lives globally, ongoing research and innovation are essential.
REFERENCES





Rohit Leitanthem, Steven Joseph Nkuku, Anchal Sharma, Dharamvir Kaur, Laikhuram Rishikanta Khuman, Review on Hepatitis B Virus: Management & Enhancement of Chronic Disease, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 5, 1598-1620. https://doi.org/10.5281/zenodo.15381579
 10.5281/zenodo.15381579
10.5281/zenodo.15381579
