MVP Samaj's College of Pharmacy, Nashik, Maharashtra
The increasing prevalence of irrational fixed-dose combinations (FDCs) poses persistent challenges for pharmaceutical education, formulation design, and regulatory oversight, particularly in the absence of transparent tools for early-stage conceptual appraisal. Existing approaches to identifying such combinations are largely retrospective, resource-intensive, or dependent on post-marketing regulatory action, limiting their utility during preliminary formulation planning. This work presents an author-developed, conceptual framework designed to support structured reasoning around fixed-dose combinations at an early, exploratory stage. The framework employs a deterministic, rule-based and explainable logic architecture that organizes established pharmacological considerations—including mechanistic compatibility, pharmacokinetic alignment, and safety overlap—into a step-wise qualitative screening process. Inputs are knowledge-driven and literature-informed, enabling transparent, human-readable interpretation of conceptual outcomes. The proposed framework is intended solely for awareness-building, educational use, and preliminary conceptual screening. It does not involve machine learning, statistical inference, outcome prediction, or empirical validation, and it does not generate clinically or regulatorily actionable outputs. Accordingly, the framework is explicitly non-validated, non-predictive, and non-clinical, and is not intended to replace expert judgment, experimental investigation, or formal regulatory review. Its contribution lies in promoting transparent pharmacological reasoning and methodological discussion in the context of fixed-dose combination assessment
Fixed-dose combinations (FDCs), defined as pharmaceutical products containing two or more active pharmaceutical ingredients in a fixed ratio for a specific therapeutic indication, are widely employed to improve patient adherence, simplify dosing regimens, and potentially enhance therapeutic outcomes when supported by sound pharmacological rationale (1). However, the same formulation strategy has also been associated with significant concerns when combinations are developed without adequate mechanistic compatibility, pharmacokinetic alignment, or safety justification (1). The distinction between rational and irrational FDCs is fundamentally grounded in established pharmacological principles, including complementary mechanisms of action, compatible pharmacokinetic profiles, and non-overlapping or manageable safety risks (1,2). Combinations that fail to meet these criteria may expose patients to additive toxicity, unnecessary drug burden, restricted dosing flexibility, or diminished therapeutic clarity, thereby undermining clinical benefit (2). In particular, mismatches in pharmacokinetic parameters—such as half-life and dosing frequency—have been identified as critical contributors to irrational formulations, especially in therapeutic areas where precise dose optimization is essential (2). In response to these concerns, regulatory authorities have implemented large-scale policy interventions. In India, numerous fixed-dose combinations have been prohibited following systematic reviews that identified inadequate therapeutic justification, insufficient evidence of benefit, and potential risks to public health (3). These regulatory actions underscore a broader challenge within the expanding FDC landscape, wherein deficiencies are frequently identified only through post-marketing scrutiny rather than during early formulation decision-making (3,4). Concerns surrounding irrational FDCs are particularly pronounced in antimicrobial therapy. Analyses of non-recommended antibiotic fixed-dose combinations in low- and middle-income countries have demonstrated that poor pharmacological rationale, incompatible pharmacokinetic properties, and unsubstantiated combination logic may contribute to patient safety risks and antimicrobial resistance (5). Such findings reinforce the importance of structured, principle-driven appraisal of combination products prior to widespread clinical use, particularly in stewardship-sensitive therapeutic domains (5). Despite extensive regulatory actions and retrospective evaluations addressing irrational fixed-dose combinations, there remains a lack of transparent, principle-driven methodologies capable of supporting early-stage conceptual screening prior to empirical evaluation or regulatory review (1,2). Existing approaches predominantly operate post hoc, relying on clinical outcomes, regulatory intervention, or resource-intensive assessments, thereby offering limited support during early formulation planning or educational analysis. This gap highlights the absence of structured, explainable frameworks capable of organizing established pharmacological principles into a reproducible screening methodology without asserting clinical, regulatory, or predictive authority. Addressing this need, the present work introduces a conceptual framework designed to facilitate preliminary, educational, and screening-level analysis of fixed-dose combinations. The proposed framework is methodological in nature, does not claim predictive accuracy, clinical effectiveness, or regulatory acceptance, and is intended solely to support structured reasoning aligned with established pharmacological principles rather than to serve as a substitute for empirical evaluation or formal regulatory review.Accordingly, this work addresses the following research question:
Can a rule-based, explainable conceptual framew ork systematically organize established pharmacological and regulatory principles to support early-stage qualitative screening of fixed-dose combinations, while explicitly excluding clinical and regulatory decision-making?
Research Contributions of This Study
This work makes the following methodological and conceptual contributions:
1. It proposes an author-developed, rule-based conceptual framework for early-stage screening of fixed-dose combinations grounded in established pharmacological and regulatory principles.
2. It formalizes qualitative decision domains—mechanistic compatibility, pharmacokinetic alignment, and safety overlap—into a transparent, step-wise logical architecture.
3. It introduces a boundary-aware screening model that explicitly distinguishes conceptual vulnerability from clinical or regulatory judgment.
4. It demonstrates illustrative application of the framework using fixed-dose combinations discussed in regulatory and policy literature to highlight interpretive transparency rather than evaluative outcomes.
METHODOLOGY:
Framework Design and Logical Architecture
The rationality of fixed-dose combinations (FDCs) has been consistently described in the literature as dependent on well-defined pharmacological principles, including therapeutic justification, compatibility of mechanisms of action, appropriate pharmacokinetic alignment, and acceptable safety profiles(1) . Deviations from these principles have been associated with irrational formulations that may increase patient risk without demonstrable therapeutic benefit(1). Regulatory reviews in India and other low- and middle-income settings further demonstrate that many irrational fixed-dose combinations were identified only after market entry, highlighting limitations in early-stage formulation scrutiny and pre-marketing assessment processes(3,4). Pharmacological mismatches—particularly disparities in pharmacokinetic parameters and overlapping safety profiles—have been repeatedly cited as key contributors to irrational combinations, especially in therapeutic areas requiring precise dosing and stewardship, such as antimicrobial therapy(2) . These concerns are reinforced by analyses indicating that non-recommended antibiotic fixed-dose combinations often lack pharmacological coherence and may pose risks to public health, including the potential contribution to antimicrobial resistance(5). Collectively, these findings underscore the need for structured, principle-driven appraisal mechanisms capable of supporting early-stage conceptual assessment prior to clinical deployment or regulatory escalation. The framework operates using a deterministic, rule- based logic structure. All decision rules, domain-level evaluations, and interpretive pathways are predefined and literature-derived. The framework does not adapt, learn, or modify its logic based on outcomes, data exposure, or iterative feedback. As a result, identical conceptual inputs yield identical qualitative outputs, enabling reproducibility of reasoning and independent critique of the framework’s logic.
Overall Architecture and Logical Flow
The proposed framework is organized as a sequential, rule-based logical architecture designed to evaluate fixed-dose combinations through a structured progression of pharmacological reasoning. The logical flow begins with the identification of constituent drug properties, followed by layered appraisal across predefined decision domains. Each domain contributes to a qualitative categorization intended for screening and educational interpretation rather than quantitative prediction. The framework operates deterministically and does not adapt or modify its logic based on data exposure, outcome feedback, or iterative learning. All interpretive outcomes are derived from predefined rules informed by established pharmacological principles and regulatory considerations reported in the literature(1–3,5).
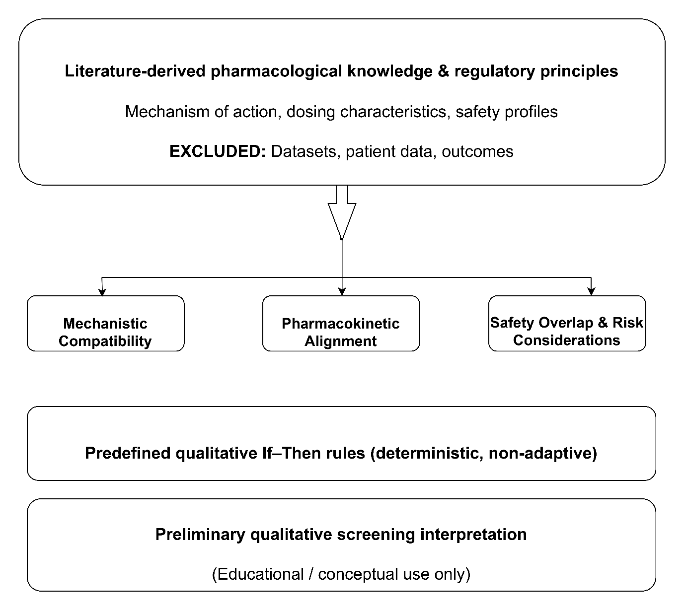
Figure 1. Conceptual architecture of a rule-based screening framework for fixed-dose combinations
The figure depicts a sequential, rule-based logical structure for the qualitative, early-stage appraisal of fixed-dse combinations, integrating mechanistic compatibility, pharmacokinetic alignment, and safety considerations into a non-predictive, conceptual screening flow derived from established pharmacological principles(1–3,5).
Logic Layers and Decision Domains
The framework is structured around three primary decision domains that reflect core pharmacological and regulatory principles relevant to the preliminary appraisal of fixed-dose combinations.
Mechanistic Compatibility
This domain assesses whether the constituent drugs exhibit complementary, redundant, or potentially conflicting mechanisms of action. The evaluation is aligned with pharmacological principles used to distinguish rational from irrational fixed-dose combinations, particularly with respect to mechanistic overlap and therapeutic justification(1).
Pharmacokinetic Alignment
This domain involves qualitative appraisal of dosing compatibility, with particular attention to disparities in dosing frequency, duration of action, and fixed-ratio rigidity that may undermine therapeutic coherence or contribute to inappropriate exposure. Such pharmacokinetic misalignments have been highlighted in analyses of irrational and non-recommended fixed-dose combinations, including those in stewardship-sensitive domains(2,5).
Safety Overlap and Risk Considerations
This domain focuses on the identification of overlapping adverse-effect profiles or safety concerns that may amplify patient risk. The assessment is consistent with regulatory reviews and policy analyses that have highlighted cumulative risk and safety concerns associated with irrational fixed-dose products(3,6). Each decision domain is evaluated independently, and the resulting conceptual flags are subsequently integrated into an overall qualitative categorization intended solely for screening and educational interpretation.
Table 1. Illustrative Rule Logic Used in Conceptual Screening of Fixed-Dose Combinations
Rules are derived from established pharmacological and regulatory principles reported in the literature(1–3,5,6).
|
Screening Domain |
Input Consideration (Qualitative) |
Illustrative Rule Logic (If–Then) |
Conceptual Flag Generated |
|
Mechanistic compatibility |
Primary pharmacological targets and pathways of constituent agents |
If multiple constituents act on the same or closely overlapping pharmacological pathways without clear complementarity, then flag potential mechanistic redundancy |
Redundancy flag |
|
Mechanistic complementarity |
Presence of protective, enabling, or mutually reinforcing mechanisms |
If one constituent enhances, protects, or enables the action of another through a distinct mechanism, then flag conceptual complementarity |
Conceptual coherence flag |
|
Pharmacokinetic alignment |
Dosing frequency, duration of action, and fixed-ratio rigidity |
If fixed-ratio administration limits independent dose optimization due to qualitatively divergent dosing characteristics, then flag pharmacokinetic misalignment |
Misalignment flag |
|
Dosing flexibility |
Ability to titrate individual components independently |
If fixed-dose formulation restricts dose adjustment in a dosing-sensitive context, then flag reduced dosing flexibility |
Flexibility limitation flag |
|
Safety overlap |
Known class-related adverse-effect profiles |
If constituents share overlapping adverse-effect tendencies that may aggregate exposure, then flag potential cumulative risk |
Cumulative risk flag |
|
Stewardship sensitivity |
Therapeutic areas requiring careful exposure control (e.g., antimicrobials) |
If pharmacokinetic or dosing misalignment occurs within a stewardship-sensitive domain, then flag contextual vulnerability |
Stewardship concern flag |
|
Integrated interpretation |
Convergence of multiple conceptual flags |
If two or more domain-level flags converge, then categorize the combination as conceptually vulnerable at the screening level |
Conceptual vulnerability category |
Nature of Inputs and Decision Logic Style
Inputs to the framework are limited to literature-derived rules, known pharmacological properties, and regulatory considerations documented in peer-reviewed sources. No empirical datasets, patient-level data, or outcome measures are incorporated. The decision logic is explicitly rule-based and hierarchical, with predefined qualitative thresholds guiding categorical outputs. No statistical inference, probabilistic modelling, machine-learning techniques, or data-driven optimization are employed at any stage.
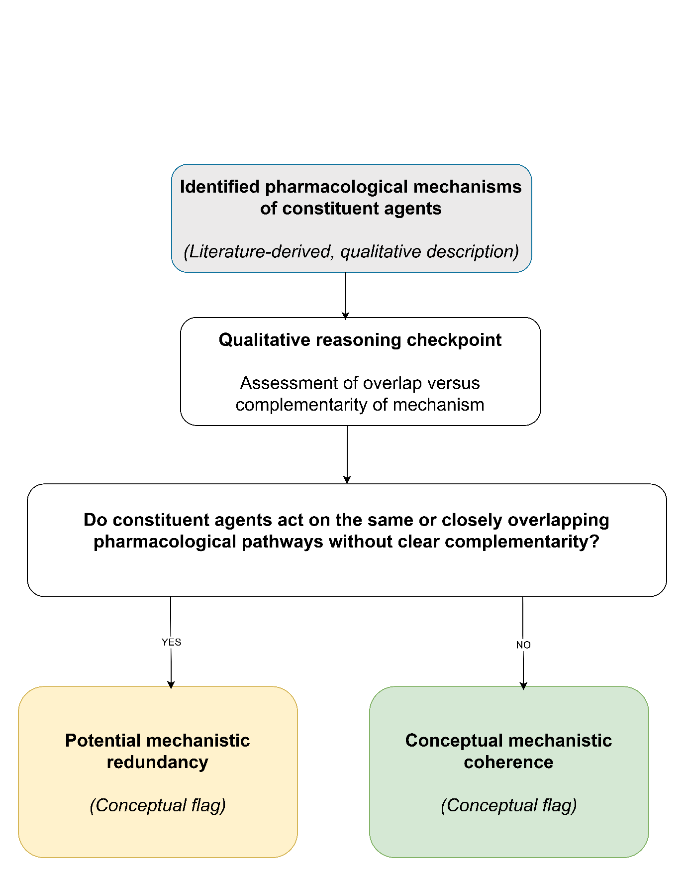
Figure 2. Illustrative Rule-Based Reasoning Flow Within the Mechanistic Compatibility Domain
The figure depicts a qualitative, rule-based reasoning pathway illustrating how mechanistic relationships between constituent drugs are interpreted within the framework, without predictive, clinical, or regulatory intent(1–3,5,6).
Explainability and Transparency Features
Explainability is a central design principle of the framework. Each logical decision is accompanied by a human-readable rationale that traces the pathway from input properties to qualitative categorization. This transparency is intended to support educational use, critical appraisal, and informed discussion rather than automated decision-making. The framework does not perform machine-learning training, does not generate predictions, and does not claim accuracy, sensitivity, or validation against clinical or regulatory outcomes. It is not intended to replace expert judgment, empirical evaluation, or formal regulatory review.
Application of the Conceptual Framework to Fixed-Dose Combinations Discussed in Regulatory and Policy Literature
To enhance interpretive clarity while preserving the explicitly non-clinical scope of the proposed framework, selected fixed-dose combinations (FDCs) that have been widely discussed in regulatory and policy literature are referenced for illustrative purposes. These examples are employed solely to demonstrate how the framework organizes established pharmacological reasoning already reported in the literature and do not constitute independent evaluative judgments, regulatory determinations, or clinical assessments
Table 2. Conceptual Mapping of Framework Decision Domains to Pharmacological Principles
|
Decision Domain |
Conceptual Rule Applied |
Pharmacological Basis (Background Literature) |
Screening Interpretation |
|
Mechanistic compatibility |
Overlapping primary therapeutic targets |
Pharmacological literature describes limited incremental benefit when multiple agents act on similar pathways(1,2) |
Mechanistic redundancy flag |
|
Mechanistic complementarity |
One component enhances or protects the activity of another |
Complementary mechanisms are cited as a foundational principle underlying rational FDC design(1) |
Conceptual coherence flag |
|
Pharmacokinetic alignment |
Divergent dosing frequency or persistence |
Fixed-ratio formulations may restrict independent dose optimization of individual components(1,3) |
Pharmacokinetic misalignment flag |
|
Safety overlap |
Shared class-related adverse-effect domains |
Literature describes cumulative exposure risks in combinations lacking clear justification(1,2) |
Cumulative risk signal |
Table 3. Illustrative Application of the Conceptual Framework to Selected Fixed-Dose Combinations
Examples are used exclusively for conceptual alignment with published pharmacological and regulatory discussions.
|
Case Illustration |
Mechanistic Compatibility |
Pharmacokinetic Alignment |
Safety Overlap |
Conceptual Screening Outcome |
|
Nimesulide-based multicomponent analgesic combinations |
Overlapping anti-inflammatory and analgesic mechanisms described in pharmacological discussions (1,2) |
Fixed-ratio dosing limits independent adjustment of component doses(1) |
Shared hepatic and gastrointestinal risk domains reported for NSAID-containing combinations(1,2) |
Conceptually vulnerable |
|
Cefixime + Azithromycin |
Distinct antibacterial mechanisms without inherent mechanistic conflict(1,3) |
Divergent duration of action and dosing persistence highlighted in regulatory discussions(3) |
Limited direct overlap; stewardship-sensitive therapeutic context (3,5) |
Pharmacokinetically incongruent |
|
Amoxicillin + Clavulanic acid |
Complementary mechanism via β-lactamase inhibition protecting antibacterial activity(1) |
Broadly compatible dosing schedules suitable for fixed-ratio administration(1) |
No disproportionate overlap beyond class-related β-lactam effects(1) |
Conceptually coherent |
Note: The examples above are intended strictly for illustrative alignment with published pharmacological and regulatory reasoning and do not imply clinical, regulatory, or safety conclusion
Table 4. Rule-Based Interpretive Logic Employed by the Proposed Framework
|
Input Observation |
Rule Triggered |
Qualitative Logic Pathway |
Output Category |
|
Same primary therapeutic target across components |
Redundancy rule |
Overlapping mechanisms without additive pharmacological justification(1,2) |
Redundancy flag |
|
Enzyme inhibition protecting an active drug |
Complementarity rule |
Functional enhancement of the primary therapeutic agent(1) |
Coherence flag |
|
Mismatch in dosing persistence or frequency |
Pharmacokinetic misalignment rule |
Fixed-dose rigidity prevents optimal scheduling(1,3) |
Misalignment flag |
|
Shared adverse-effect domains |
Safety accumulation rule |
Additive exposure without compensatory mechanistic benefit(1,2) |
Risk signal |
Important: Rules operate independently and do not generate scores, rankings, or decisions. All outputs remain qualitative and conceptual in nature.
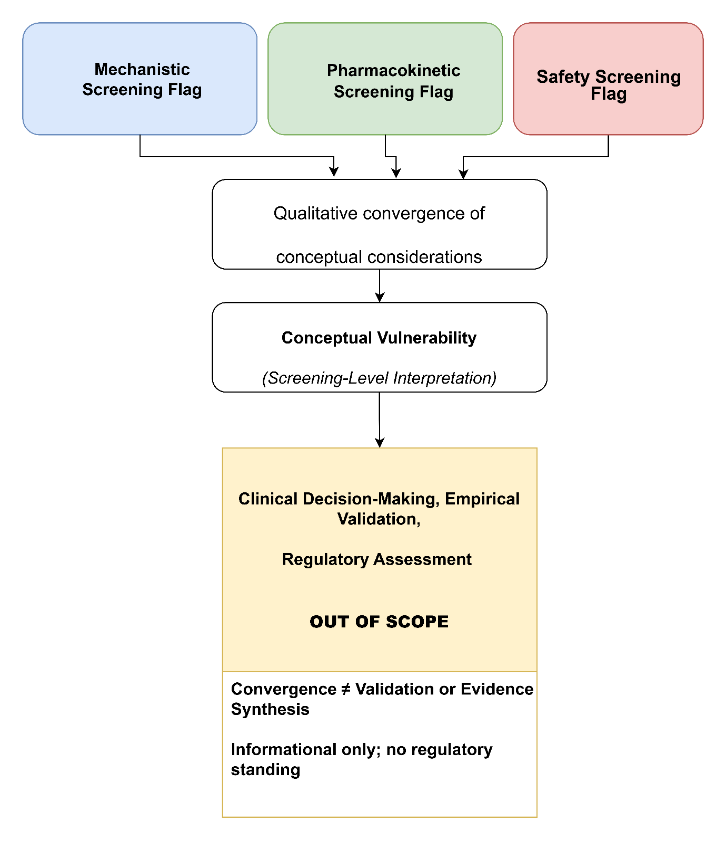
Figure 3. Conceptual Integration of Screening Flags and Interpretive Boundary
The figure illustrates the qualitative convergence of independent domain-level conceptual flags into an overall screening interpretation, while explicitly demarcating the boundary between preliminary conceptual vulnerability and clinical or regulatory judgment, which remains outside the scope of the framework(1–3,5).
Complementary Role to Expert Judgment and Regulatory Review
The framework is explicitly designed to complement, not replace, expert pharmacological judgment, empirical investigation, or regulatory assessment. Its outputs reflect structured interpretive reasoning rather than evidence-based conclusions and must not be construed as substitutes for experimental validation, clinical evaluation, or formal regulatory review.
Scope Boundary of the Research
The scope of this research is intentionally constrained. The proposed framework does not involve experimental validation, clinical outcome assessment, regulatory determination, statistical inference, or predictive modelling. It does not generate decisions, rankings, scores, or regulatory classifications. The framework is limited to the organization and transparent presentation of established pharmacological reasoning for preliminary, qualitative screening purposes. All interpretations remain conceptual in nature and must not be construed as substitutes for empirical investigation, expert judgment, or formal regulatory review.
Methodological Limitations
As a conceptual methodology, the framework necessarily simplifies complex pharmacological relationships into qualitative decision rules. It does not capture dose–response dynamics, formulation-specific variability, patient heterogeneity, or real-world therapeutic outcomes. These limitations are intrinsic to early-stage screening methodologies and underscore the need for subsequent empirical validation, expert review, and regulatory assessment. The framework is therefore unsuitable for standalone evaluation of fixed-dose combinations and must be interpreted strictly within its methodological scope.
DISCUSSION
Interpretation of the Proposed Framework
The present work introduces a conceptual, rule-based framework designed to support structured reasoning around fixed-dose combinations at an early and exploratory stage. Rather than generating evaluative, predictive, or decision-making outputs, the framework demonstrates how established pharmacological principles—specifically mechanistic compatibility, pharmacokinetic alignment, and safety considerations—can be systematically organized into an explicit and transparent screening logic. The primary contribution lies in formalizing qualitative reasoning processes that are often applied implicitly or retrospectively into a reproducible, interpretable structure suitable for preliminary appraisal.By decomposing fixed-dose combination assessment into independent yet integrable decision domains, the framework highlights how conceptual vulnerabilities may arise from overlapping mechanisms, dosing incongruence, or cumulative safety risks. Importantly, the framework does not infer clinical consequences or regulatory outcomes; instead, it illustrates how convergence of multiple conceptual flags may warrant heightened scrutiny or further investigation. This interpretive role reinforces the framework’s function as a methodological aid for reasoning rather than as an evaluative or predictive system.
Methodological Positioning and Implications
From a methodological perspective, the proposed framework operates upstream of empirical evaluation and regulatory assessment. Existing approaches to identifying irrational fixed-dose combinations predominantly rely on retrospective regulatory reviews, post-marketing safety signals, or outcome-driven analyses. While such approaches are essential for public health protection, they offer limited support for early-stage conceptual screening during formulation planning or educational analysis.In contrast, the present framework contributes a structured, explainable methodology that bridges pharmacological theory and later-stage evaluation without encroaching upon clinical or regulatory domains. Its deterministic, rule-based design ensures reproducibility of reasoning while maintaining transparency regarding assumptions and scope. By explicitly separating conceptual screening from judgment or validation, the framework addresses ethical and methodological concerns associated with premature decision-making based on incomplete evidence. This positioning distinguishes the framework as a screening and reasoning tool rather than an assessment or approval mechanism.
Implications for Education and Early-Stage Analysis
The framework may be particularly relevant for pharmaceutical education and early-stage formulation analysis, where structured understanding of rational versus irrational fixed-dose combinations is essential. By making pharmacological reasoning explicit and traceable, the framework supports learning, discussion, and hypothesis generation without substituting for empirical investigation. Its explainable logic structure may assist students, educators, and early-stage investigators in systematically applying pharmacological principles while remaining cognizant of the framework’s conceptual and non-evaluative nature.
FUTURE DIRECTIONS
Future work may explore refinement of the framework through expansion of the rule set to additional therapeutic domains or pharmacological dimensions, while preserving its conceptual and explainable design. Further development could also examine adaptation into structured educational modules or case-based learning tools to enhance pedagogical utility. Any such extensions would remain preliminary in nature and would require independent empirical evaluation and expert review prior to clinical or regulatory consideration.
CONCLUSION
This work presents an author-developed, conceptual, and non-validated framework designed to support structured, explainable reasoning around fixed-dose combinations at an early and exploratory stage. By organizing fundamental pharmacological considerations into a transparent, rule-based logic flow, the framework offers a systematic approach for preliminary appraisal without asserting empirical validity or clinical applicability.
The framework is intentionally limited in scope and is positioned as an educational and methodological aid, rather than as a tool for decision-making, prediction, or regulatory evaluation. Its primary contribution lies in clarifying how mechanistic compatibility, pharmacokinetic alignment, and safety considerations can be conceptually integrated to inform structured discussion and learning.
Importantly, the framework does not replace expert judgment, experimental investigation, or formal regulatory review. All outputs are qualitative and interpretive, and must be understood within the context of the framework’s explicit limitations.
From a methodological perspective, this work contributes to ongoing discussions on how structured, explainable reasoning can support early-stage pharmaceutical analysis without encroaching upon empirical or regulatory domains. By explicitly separating conceptual screening from decision-making, the framework offers a transparent foundation for education, discussion, and hypothesis generation in the context of fixed-dose combination assessment
REFERENCES


Omkar Ramesh Kahane, Vanshita Kishor Patil, Conceptual Screening of Fixed-Dose Combinations Using a Rule-Based Pharmacological Framework, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 1822-1832. https://doi.org/10.5281/zenodo.18299381
 10.5281/zenodo.18299381
10.5281/zenodo.18299381
