Vidya Niketan Institute of Pharmacy Research and Centre.
Psoriasis is a chronic, immune-mediated, multisystem disease characterized by well-demarcated, erythematous, and scaly plaques that affects an estimated 2–3% of the world’s population. Although classically considered a dermatologic disorder, psoriasis is increasingly recognized as a systemic inflammatory condition with substantial extracutaneous involvement, including psoriatic arthritis, cardiometabolic disease, nonalcoholic fatty liver disease, depression, and reduced health-related quality of life. Over the last two decades, fundamental insights into the interleukin (IL)-23/T helper (Th)17/TNF-? axis have reshaped the understanding of disease mechanisms and catalyzed the development of highly effective targeted therapies. Contemporary management integrates precise clinical phenotyping, validated measures of severity and patient-reported impact, and shared decision-making to achieve treat-to-target goals such as “clear” or “almost clear” skin and improved life participation. This narrative review synthesizes current evidence on the epidemiology, pathophysiology, clinical variants, diagnosis, and treatment of psoriasis; summarizes important advances including IL-23/IL-17 pathway inhibition and oral TYK2 inhibition; and highlights unresolved challenges such as persistent undertreatment, comorbidity prevention, long-term pharmacovigilance, and equitable global access. Five original figures illustrate the pathogenic immune cascade, clinical subtypes and body sites, severity assessment framework, a pragmatic treatment ladder, and the spectrum of systemic comorbidities. The aim is to provide an up-to-date, clinically relevant, and plagiarism-free overview suitable for academic submission and for informing multidisciplinary care.
Psoriasis is among the most prevalent chronic inflammatory skin diseases and can present across the lifespan, with peaks in adolescence/early adulthood and later adulthood. The clinical course is typically relapsing–remitting, with periods of quiescence punctuated by flares related to infections, stress, medications, or skin trauma. Stigma and visible disfigurement contribute to social isolation and psychological distress, while pruritus, pain, and fissuring impair sleep, work productivity, and daily activities. The disease carries substantial direct and indirect economic costs attributable to medical care, lost productivity, and comorbid conditions. Over the past 20 years, a paradigm shift has reframed psoriasis from a keratinocyte-centric hyperproliferative disorder to a prototypical immune-mediated disease driven by maladaptive crosstalk among dendritic cells, T cells, keratinocytes, endothelial cells, and peripheral nerves. Parallel advances in genetics and immunology have identified susceptibility loci—most prominently HLA-C*06:02—and cytokine circuits that sustain a self-amplifying inflammatory loop in lesional skin. At the same time, rigorous randomized trials and real-world studies have validated an expanding armamentarium of topical, phototherapeutic, systemic, and biologic treatments that can deliver rapid, durable skin clearance for many patients. Yet large gaps persist in care: many individuals remain undiagnosed or undertreated; high-impact “special site” disease (scalp, face, genitals, palms/soles, nails) is too often minimized; and the broader burden of psoriatic disease—including arthritis and cardiovascular risk—may be overlooked in siloed settings. This review provides a comprehensive, evidence-informed synthesis to support nuanced, patient-centered management.
Background and Pathophysiology
The immunopathogenesis of psoriasis involves aberrant activation of both innate and adaptive immunity at the skin–immune interface. In genetically susceptible hosts, exogenous triggers such as streptococcal pharyngitis, cutaneous trauma (Koebner phenomenon), or certain medications activate plasmacytoid and myeloid dendritic cells. These antigen-presenting cells elaborate type I interferons and the key polarizing cytokine IL?23, which promotes differentiation and maintenance of Th17 cells. Th17 and Th1 effector T cells traffic to the skin and release canonical cytokines—IL?17A/F, IL?22, interferon?γ, and TNF?α—that stimulate keratinocytes. Activated keratinocytes proliferate and produce chemokines (e.g., CCL20), antimicrobial peptides (e.g., LL?37), and additional cytokines, thereby recruiting more immune cells and sustaining a feed-forward inflammatory loop. IL?17A and IL?17F accelerate keratinocyte turnover and neutrophil chemotaxis; IL?22 drives acanthosis and impaired differentiation; TNF?α amplifies dendritic cell activation and endothelial adhesion molecule expression. The centrality of the IL?23/Th17 axis is underscored by the clinical success of agents targeting IL?23 p19 and IL?17A/F, as well as the efficacy of oral TYK2 inhibition that selectively modulates signaling for IL?23, IL?12, and type I interferons via the JH2 pseudokinase domain.
Genetic studies identify more than 60 susceptibility loci, with HLA?C*06:02 (PSORS1) exerting the strongest effect, particularly in early-onset disease. HLA?C*06:02 may shape antigen presentation in the skin and has been associated with differential responses to certain biologics. Non-HLA loci implicate pathways of NF?κB activation, skin barrier regulation, and cytokine signaling. Epigenetic modifications and microRNAs also contribute to lesional transcriptional programs. Beyond immune circuits, vascular changes (increased dermal capillaries with tortuous loops) and neural factors (neuropeptides, pruritus pathways) participate in symptom generation.
Psoriasis is systemic. Low-grade inflammation extends beyond the skin and likely contributes to increased prevalence of insulin resistance, metabolic syndrome, obesity, nonalcoholic fatty liver disease, chronic kidney disease, and accelerated atherosclerosis. Shared inflammatory mediators and clonal hematopoiesis may underlie this enhanced cardiovascular risk. Psoriatic arthritis affects up to a third of patients and can present with peripheral arthritis, enthesitis, dactylitis, and axial disease; early recognition is critical to prevent irreversible damage. Figure 1 provides a conceptual schematic of the immune cascade linking genetic susceptibility, dendritic cell activation, Th17/Th1 polarization, and keratinocyte hyperproliferation.
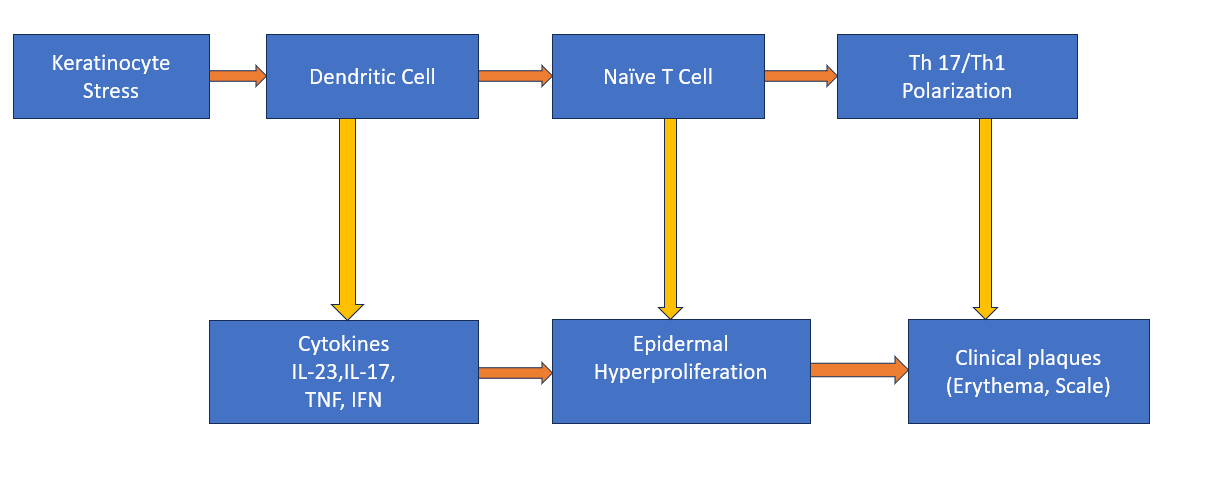
Figure 1. Conceptual immune cascade in psoriasis involving dendritic cells, Th17/Th1 polarization, and keratinocyte hyperproliferation.
Types of Psoriasis
Psoriasis manifests through several overlapping phenotypes:
• Chronic plaque psoriasis (psoriasis vulgaris) is the most common form, characterized by sharply demarcated, erythematous plaques with overlying micaceous (silvery-white) scale on extensor surfaces, scalp, and trunk. Lesions are often symmetrical and may fissure or become painful.
• Guttate psoriasis presents with numerous 2–10 mm “drop-like” papules and fine scale, frequently following streptococcal infection; it can remit spontaneously or evolve into chronic plaque disease.
• Inverse (intertriginous) psoriasis affects axillae, inframammary folds, groin, and other flexural sites. Friction and maceration reduce scaling and accentuate erythema; secondary candidiasis may complicate.
• Pustular psoriasis is heterogeneous. Localized palmoplantar pustulosis features sterile pustules on palms/soles and may severely impair function. Generalized pustular psoriasis is a systemic illness with fever, leukocytosis, and diffuse sterile pustules on erythematous skin; it requires urgent care.
• Erythrodermic psoriasis involves >90% body surface area with diffuse erythema, scaling, thermoregulatory instability, fluid–electrolyte imbalance, and risk of high-output cardiac failure; hospitalization is often necessary.
• Nail psoriasis occurs in up to half of patients and is marked by pitting, onycholysis, subungual hyperkeratosis, and oil-drop discoloration. Nail involvement correlates with risk of psoriatic arthritis.
• Scalp and genital psoriasis, though sometimes limited in extent, are disproportionately burdensome owing to pruritus, pain, dyspareunia, and psychosocial impact.
Clinical phenotypes may coexist and shift over time under the influence of triggers, treatment, and comorbidities
Causes and Risk Factors
Psoriasis reflects the interplay of inherited susceptibility and environment. Family history is common, and monozygotic twin concordance greatly exceeds dizygotic concordance, consistent with a substantial heritable component. HLA?C*06:02 remains the strongest single genetic association and is enriched in early-onset disease; numerous non-HLA loci implicate innate immune sensing, antigen presentation, and barrier biology.
Well?recognized triggers include infections (particularly streptococcal pharyngitis), skin injury (Koebnerization after cuts, tattoos, or surgery), psychosocial stressors, smoking, and alcohol misuse. Medication triggers and exacerbators include lithium, antimalarials, beta?blockers, interferons, and abrupt systemic corticosteroid withdrawal (which can precipitate pustular flares); several biologics used for other conditions can rarely paradoxically induce psoriasiform eruptions. Obesity and metabolic syndrome are risk enhancers and may adversely affect treatment response, possibly via adipokines and chronic low-grade inflammation. Vitamin D deficiency, air pollution, and dysbiosis are under investigation as modulators. Pregnancy can alter disease activity, and post?partum flares may occur. Finally, socioeconomic barriers, limited access to dermatology, and stigma contribute to delayed diagnosis and undertreatment, magnifying risk of downstream complications such as psoriatic arthritis and cardiovascular disease.
Symptoms and Clinical Presentation
Patients commonly report pruritus, burning, soreness, and skin tightness. Plaques are classically symmetrical with sharply demarcated borders and thick, adherent scale; removal of scale may elicit the Auspitz sign (pinpoint bleeding). Scalp disease can mimic seborrheic dermatitis but typically extends beyond the hairline; facial involvement often affects the hairline, eyebrows, and glabella. Inverse psoriasis features bright erythema with minimal scale and is frequently misdiagnosed as intertrigo or candidiasis. Palmoplantar disease presents with hyperkeratotic plaques and fissures and leads to functional impairment. Nail findings include pitting, oil-drop (salmon patch) discoloration, onycholysis, and subungual hyperkeratosis. Generalized pustular and erythrodermic variants may cause fever, malaise, lymphadenopathy, and laboratory abnormalities. The psychosocial impact can be profound; patients may avoid social situations, intimacy, or careers requiring public interaction. Screening for psoriatic arthritis is essential; clues include morning stiffness, swollen fingers or toes (dactylitis), enthesitis (heel pain), and nail disease. Figure 5 lists common systemic comorbidities that warrant proactive assessment.
Diagnosis
Psoriasis is fundamentally a clinical diagnosis. The history should explore triggers, prior treatments and responses, effect on work and life participation, and symptoms suggestive of psoriatic arthritis. Physical examination maps lesion morphology and distribution, including scalp, nails, inverse areas, and genitals. Dermoscopy often shows regularly distributed dotted vessels on a red background with diffuse white scale. Skin biopsy is reserved for atypical cases (e.g., suspected tinea, cutaneous T?cell lymphoma, or pityriasis rubra pilaris) or unusual sites; it typically reveals acanthosis with elongated rete ridges, diminished or absent granular layer, parakeratosis with neutrophils (Munro microabscesses), and dilated tortuous dermal capillaries.
Severity assessment guides therapy and follow?up. Common metrics include body surface area (BSA) using the “rule of nines” or the palmar method (~1% per patient palm), the Psoriasis Area and Severity Index (PASI)—an area?weighted composite of erythema, induration, and scaling across body regions—and patient?reported outcome measures such as the Dermatology Life Quality Index (DLQI). Many guidelines adopt a “rule of tens” to define severe disease (PASI > 10, BSA > 10%, or DLQI > 10), but location (face, hands, genitals, scalp), symptom burden, and occupational impact can justify systemic therapy even with limited BSA. Emerging simplified tools (e.g., PGA×BSA) and digital assessments enhance feasibility in routine practice. Baseline laboratory evaluation depends on the chosen therapy (e.g., CBC, LFTs for methotrexate; tuberculosis and hepatitis screening before biologics). Figure 3 summarizes major assessment instruments and treat?to?target concepts.
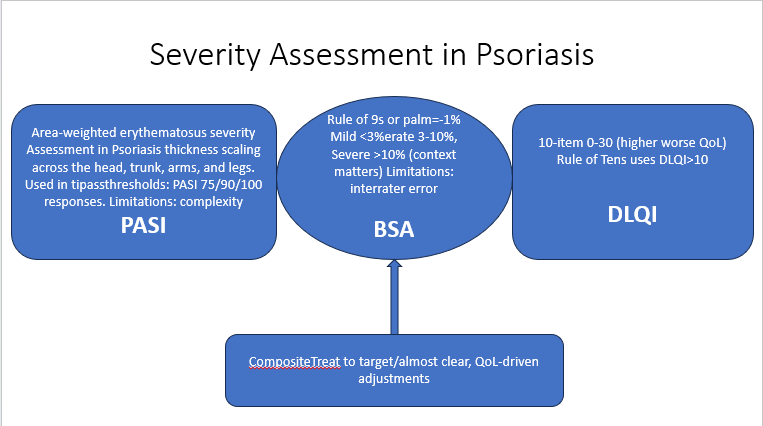
Figure 3. Overview of severity and outcome measures (PASI, BSA, DLQI) and treat?to?target concepts
Current Treatment Options (medical, lifestyle, and alternative approaches)
Management is individualized and iterative, aligning treatment intensity with disease severity, phenotype, comorbidities, and patient preferences, while addressing modifiable risk factors and health literacy.
Lifestyle, education, and psychosocial care. Patient education on chronicity, trigger avoidance, and adherence substantially improves outcomes. Emollients reduce scale and itch and may enhance penetration of topical agents. Structured weight reduction in patients with obesity, regular physical activity, smoking cessation, and moderation of alcohol intake diminish systemic inflammation and may improve treatment response. Mind–body interventions (mindfulness, cognitive behavioral therapy), sleep optimization, and stress reduction are useful adjuncts.
Topical therapy. For mild to moderate plaque psoriasis, topical corticosteroids remain first?line because of rapid efficacy and versatility across body sites. Potency is selected according to location and thickness; strategies to minimize atrophy and tachyphylaxis include intermittent dosing, proactive weekend therapy for maintenance, and steroid?sparing combinations. Vitamin D analogues (e.g., calcipotriol) normalize keratinocyte differentiation and are effective alone or in fixed?dose combinations with corticosteroids. Tazarotene is useful for plaque thinning; keratolytics (salicylic acid, urea) aid scale reduction. Calcineurin inhibitors (tacrolimus, pimecrolimus) are preferred for face, genitals, and intertriginous areas. For scalp disease, medicated shampoos, foams, and solutions improve practicality.
Phototherapy. Narrowband UVB (NB?UVB) is effective for widespread plaque disease and offers a favorable risk–benefit profile; targeted UVB devices can treat localized plaques. PUVA (psoralen plus UVA) is reserved for refractory cases given long?term carcinogenesis concerns. Phototherapy can be combined with systemic or topical treatments to shorten time to clearance.
Conventional systemic agents. Methotrexate is a cornerstone for moderate?to?severe disease, nail psoriasis, and psoriatic arthritis. It reduces keratinocyte proliferation and modulates T?cell function; careful monitoring for hepatotoxicity, cytopenias, and teratogenicity is necessary, and folate supplementation is standard. Cyclosporine induces rapid control in severe or unstable disease but is limited by nephrotoxicity and hypertension. Acitretin is keratinocyte?directed and useful for pustular and palmoplantar variants; it is highly teratogenic and can be combined with phototherapy (Re?PUVA). Apremilast, an oral phosphodiesterase?4 inhibitor, provides modest efficacy with favorable monitoring and is particularly attractive for patients averse to injections or with multiple comorbidities.
Targeted small molecule therapy. Deucravacitinib, an oral, selective TYK2 inhibitor, allosterically binds the regulatory pseudokinase (JH2) domain, thereby modulating IL?23, IL?12, and type I interferon signaling without direct JAK1/2/3 inhibition. Phase III trials demonstrated superiority to placebo and apremilast with meaningful PASI 75/90 responses and a generally well?tolerated safety profile. Long?term extension studies report durable efficacy up to two years, with nasopharyngitis, headache, and acne among common adverse events and a safety profile that differs from pan?JAK inhibitors.
Biologic therapy. Biologics targeting upstream cytokines deliver high levels of skin clearance and improved quality of life. TNF?α inhibitors (adalimumab, etanercept, infliximab) improve skin and joint disease but are relatively less effective than newer classes for complete clearance. Ustekinumab targets IL?12/23 (p40) and has convenient dosing but has been eclipsed by IL?23 p19 inhibitors (guselkumab, risankizumab, tildrakizumab), which offer durable PASI 90/100 responses and favorable safety. IL?17 pathway inhibitors—secukinumab and ixekizumab (IL?17A) and bimekizumab (IL?17A/IL?17F)—produce rapid clearance; candidiasis risk reflects mucocutaneous IL?17 biology. Choice of agent is shaped by comorbidities (e.g., IBD favors IL?12/23 or IL?23 over IL?17; demyelinating disease favors IL?23/IL?17 over TNF?α), patient preferences, pregnancy plans, and payer policies. Vaccinations should be updated before initiating immunomodulators; live vaccines are generally avoided during therapy. Figure 4 presents a pragmatic treatment ladder, emphasizing integration of lifestyle change with escalating pharmacologic options.
Complementary and integrative approaches. Evidence supports weight loss for overweight patients and suggests benefits of Mediterranean?style dietary patterns and smoking/alcohol reduction. Data on specific supplements (e.g., vitamin D repletion in deficiency) and herbal preparations are limited and heterogeneous; clinicians should counsel regarding quality, potential hepatotoxicity, and drug–herb interactions. Such approaches should complement, not replace, guideline?based medical therapy.
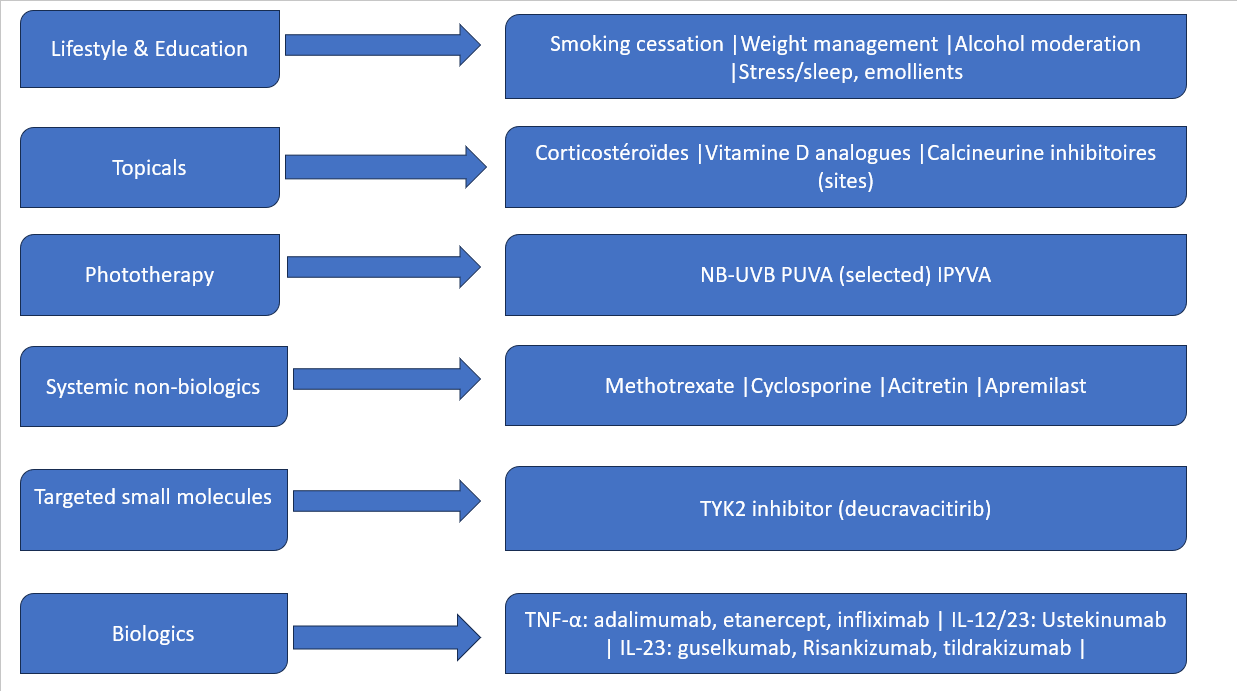
Figure 4. Pragmatic treatment ladder for psoriasis care.
Advances in Research
Recent years have witnessed accelerated progress in multiple domains. Single?cell and spatial transcriptomics have refined understanding of lesional ecosystems, identifying pathogenic T?cell states, myeloid subsets, and keratinocyte programs that may underlie interpatient heterogeneity and therapeutic response. Systems immunology has clarified kinetics of cytokine suppression and pathways of disease memory in clinically resolved skin. Genetics continues to inform endotyping: HLA?C*06:02 status associates with earlier onset and may predict differential response to certain agents, while polygenic risk scores are being explored for early detection. Therapeutically, highly selective monoclonal antibodies against IL?23 p19 and IL?17A/F—and the oral TYK2 inhibitor deucravacitinib—represent major advances, with long?term extensions demonstrating sustained efficacy and quality?of?life benefits. Novel modalities under investigation include oral peptide antagonists of IL?23 receptor, inhibitors of RORγt (the Th17 transcriptional driver), and approaches aimed at durable disease modification by targeting tissue?resident memory T cells. Digital health tools, including teledermatology, home phototherapy, and patient?reported outcome platforms, are expanding access and enabling treat?to?target implementation. Cardiometabolic science is probing whether effective inflammatory control can translate into reduced atherosclerotic risk—a key question for the next decade.
Challenges and Future Perspectives
Despite unprecedented therapeutic potency, real?world implementation lags. Many patients with moderate?to?severe psoriasis remain undertreated or cycle through topical therapies without escalation. Barriers include limited specialist access, administrative burden of prior authorization, treatment costs, and concerns about immunosuppression. Health disparities persist across geography, race/ethnicity, and socioeconomic status. Long?term safety surveillance must continue, with registries tracking rare events, infection risk, and pregnancy outcomes. Clinicians should maintain vigilance for comorbidities—particularly psoriatic arthritis (where early treatment prevents damage) and cardiovascular disease (where aggressive risk?factor control is warranted). Research priorities include disease interception in high?risk individuals, biomarkers that predict optimal therapy, strategies to sustain remission after withdrawal, and trials that incorporate patient?important outcomes such as itch, fatigue, and life participation. Multidisciplinary models that integrate dermatology, rheumatology, cardiology, primary care, and behavioral health will be essential to deliver holistic, equitable care globally.
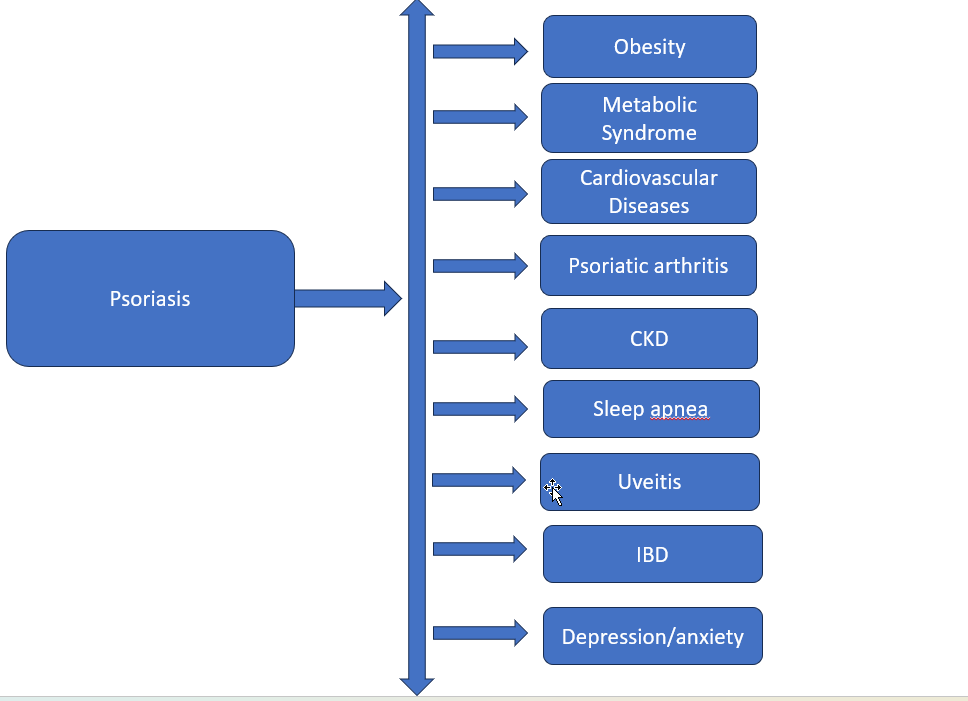
Figure 5. Major systemic comorbidities associated with psoriasis.
CONCLUSION
Psoriasis exemplifies a chronic, immune?mediated disease in which mechanistic discovery has rapidly translated into therapeutic progress. Recognition of the IL?23/Th17/TNF?α axis has generated targeted interventions capable of near?complete clearance for many patients, while attention to lifestyle, mental health, and comorbidity screening anchors comprehensive care. Persistent challenges—undertreatment, inequitable access, and prevention of long?term complications—demand coordinated clinical, scientific, and policy efforts. With patient?centered, treat?to?target strategies and continued innovation, the prospects for individuals living with psoriasis continue to improve.
REFERENCES

Ghuge Tanuja*, Pokale Shraddha, Bhise Gorakhnath, Salve Aniket, Kolhe Vishakha, Psoriasis: An Updated Review of Pathophysiology, Clinical Spectrum, and Management, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 10, 800-809 https://doi.org/10.5281/zenodo.17301525
 10.5281/zenodo.17301525
10.5281/zenodo.17301525
