1Assistant Professor, Department of Pharmacology, DJPS College of Pharmacy Pohetakli, Maharashtra, India.
2Professor, Department of Pharmaceutics, DJPS College of Pharmacy Pohetakli, Maharashtra, India.
3B. Pharm Student Department of Pharmacy, DJPS College of Pharmacy Pohetakli, Maharashtra, India.
Polycystic Ovary Syndrome (PCOS) is a common endocrine disorder affecting women of reproductive age, characterized by hyperandrogenism, ovulatory dysfunction, and polycystic ovarian morphology. Its multifactorial nature—encompassing genetic, hormonal, environmental, and lifestyle influences—makes diagnosis and management particularly challenging. PCOS extends beyond reproductive health, with strong associations to metabolic syndrome, insulin resistance, obesity, and mental health disorders such as anxiety and depression. Factors like environmental toxins, poor dietary habits, and sedentary lifestyles further contribute to its progression. Clinically, it presents with symptoms such as irregular menstruation, hirsutism, and acne, with diagnosis typically relying on a combination of clinical signs, hormonal evaluations, and imaging. Current treatment strategies are multidimensional, including lifestyle modifications, pharmacological interventions (e.g., metformin, clomiphene citrate), and complementary therapies, such as Ayurvedic remedies. While a definitive cure remains elusive, early diagnosis and personalized management can reduce long-term risks, including cardiovascular disease and type 2 diabetes. Emerging research highlights the importance of addressing patient experiences and mental health to ensure holistic care. Advances in genetic studies and the therapeutic potential of natural compounds like inositol isomers signal promising new directions. As a chronic, multisystem condition, PCOS requires an integrated, patient centered approach for effective long-term management.
Polycystic Ovary Syndrome (PCOS) is one of the most common and complex endocrine disorders affecting women of reproductive age worldwide. It is defined by three main features: hyperandrogenism, irregular ovulation, and polycystic ovarian morphology. PCOS has widespread effects on reproductive, metabolic, and psychological health.
Despite being recognized for decades, the exact cause of PCOS remains unclear, and its symptoms vary significantly between individuals. This makes both diagnosis and treatment challenging. PCOS is a leading cause of female infertility, largely due to anovulation. However, even when ovulation is restored, many women still require assisted reproductive technologies like IVF, suggesting deeper issues such as poor egg quality or altered endometrial receptivity. Beyond fertility, PCOS is linked to hormonal imbalance, insulin resistance, obesity, and mood disorders like anxiety and depression. Oxidative stress is increasingly seen as a major factor in its development, triggering inflammation and worsening symptoms.
The global prevalence of PCOS ranges from 5% to 15% among women aged 18–44. This wide range is influenced by changing diagnostic criteria, regional disparities in healthcare access, and limited awareness. Common symptoms include irregular periods, acne, hirsutism, and weight gain, often worsened by poor lifestyle habits. Over time, diagnostic definitions have evolved—from focusing on ovarian appearance to broader criteria like the Rotterdam criteria—leading to shifts in how PCOS is recognized and reported. Many women, especially in low-resource settings, remain undiagnosed or misdiagnosed, delaying early treatment and increasing the risk of long-term complications.1,2,3,4
PCOS often presents alongside metabolic issues like obesity, insulin resistance, and systemic inflammation. Treatments include lifestyle changes, medications such as metformin, and in some cases, bariatric surgery. Women with PCOS are also at higher risk for type 2 diabetes, cardiovascular diseases, and mental health issues. Despite extensive clinical research, few studies explore the lived experiences of women with PCOS. Understanding how patients cope with symptoms, interact with healthcare systems, and manage daily life is critical for providing holistic, patient-centre care.5,6,7,8,9
Another overlooked area is how PCOS affects body weight regulation. Many women with PCOS struggle with weight loss due to complex changes in appetite, metabolism, and energy balance. Additionally, exposure to endocrine-disrupting chemicals (e.g., bisphenols, parabens, triclosan) may disrupt hormonal balance and contribute to the development of PCOS. A majority of PCOS patients also meet the criteria for metabolic syndrome, which includes high blood pressure, abnormal cholesterol levels, and glucose intolerance. The shared link—insulin resistance makes PCOS a condition requiring long-term, multidisciplinary management.10,11
Adipose (fat) tissue dysfunction also plays a key role in PCOS by promoting inflammation, androgen excess, and insulin resistance. Genetic, environmental, and epigenetic factors influence these pathways, reinforcing the need to view PCOS as a lifelong metabolic and endocrine disorder.12
Recently, natural compounds like myo-inositol (MI) and D-chiro-inositol (DCI) have shown promise in improving insulin sensitivity and restoring ovulation. These may serve as safer or complementary alternatives to standard treatments like metformin.13
In summary, PCOS is a multisystem disorder that affects women well beyond fertility. Early diagnosis, individualized treatment, and continuous care are essential to reduce the risk of long-term complications. Addressing both medical and emotional aspects of the disorder will lead to more effective and compassionate healthcare.14
Female Reproductive System: Anatomy and Physiology
The female reproductive system is a highly specialized group of organs that work in coordination to ensure the processes of sexual reproduction, menstruation, fertilization, pregnancy, and childbirth. It consists of distinct external and internal anatomical structures, each with unique physiological roles, all under the control of a finely regulated hormonal system.
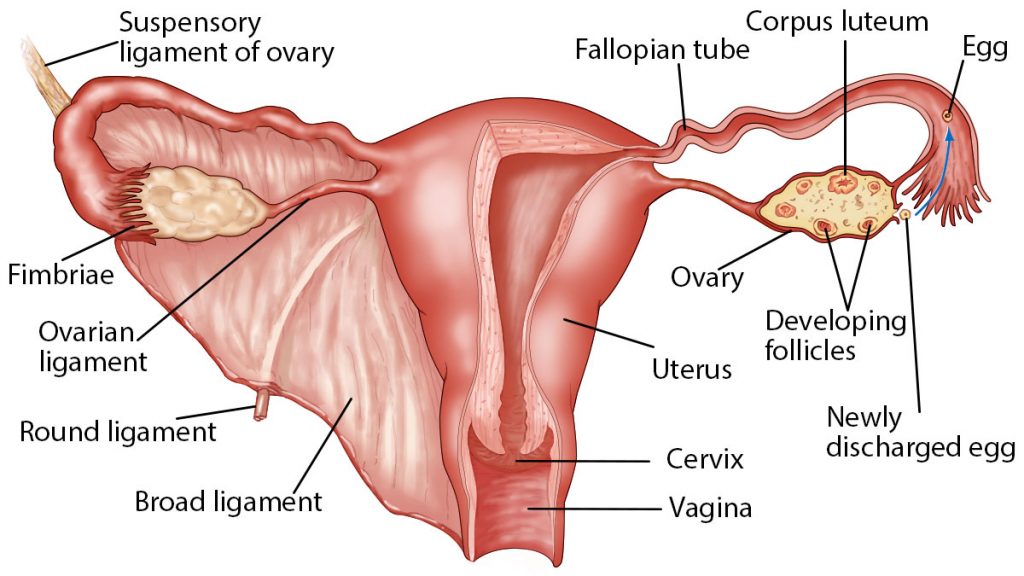
Fig No. Internal Structure of ovary
Anatomy Overview
The external genitalia, collectively called the vulva, provide protection for the internal organs and play a key role in sexual arousal and lubrication. These include:
The internal reproductive organs include:
Physiology Overview
The physiological functions of the female reproductive system are governed by a monthly menstrual cycle, typically lasting around 28 days, and controlled by a complex hormonal feedback loop involving the hypothalamus, pituitary gland, and ovaries.
1. Menstrual Cycle Phases
2. Hormonal Regulation
The cycle is regulated by a hierarchical hormonal control system:
3. Fertilization and Pregnancy
PCOS (POLYCYSTIC OVARY SYNDROME):
Polycystic Ovary Syndrome (PCOS) is a prevalent endocrine disorder affecting women, particularly during their reproductive years. Epidemiological studies estimate that PCOS affects approximately 10–15% of women of reproductive age, with at least 7% of infertile women exhibiting clinical features of the syndrome. PCOS is recognized as a heterogeneous disorder characterized by a range of clinical manifestations that vary significantly among individuals.
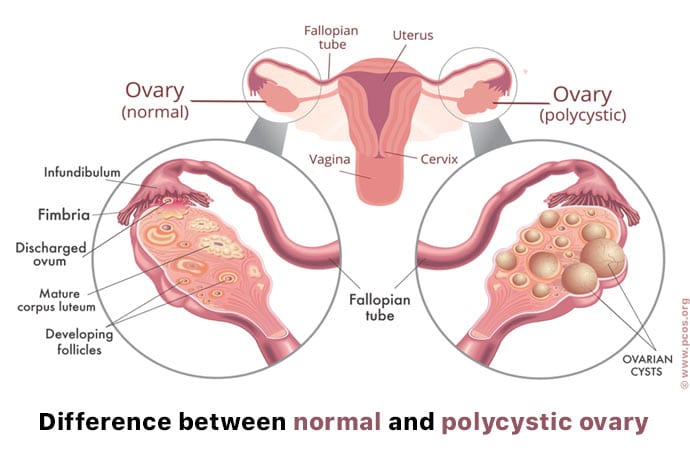
Fig No. 2 polycystic ovary
Mechanism of Action of PCOS
Polycystic Ovary Syndrome (PCOS) develops through a multifaceted interaction of genetic, epigenetic, and environmental factors that disrupt normal hormonal homeostasis. A central hormonal abnormality in PCOS is an increased luteinizing hormone (LH) to follicle-stimulating hormone (FSH) ratio, which contributes to anovulation and heightened androgen production.
This hormonal imbalance also dysregulates the hypothalamic-pituitary-adrenal (HPA) axis, heightening the body's stress response and increasing susceptibility to mood disorders such as anxiety and depression.
Insulin resistance is another key pathological feature of PCOS. Despite elevated insulin production (hyperinsulinemia), peripheral tissues such as skeletal muscle and adipose tissue exhibit decreased sensitivity to insulin. This resistance stimulates further insulin secretion, creating a self-perpetuating cycle. Elevated insulin levels suppress hepatic production of sex hormone-binding globulin (SHBG), leading to increased levels of free circulating androgens. These androgens not only exacerbate insulin resistance but also drive the clinical manifestations of hyperandrogenism such as acne, hirsutism, and oligomenorrhea.
Thus, PCOS is a systemic condition marked by a feedback loop where hormonal and metabolic disturbances mutually reinforce one another, making the condition challenging to manage without a multifactorial treatment strategy.18,19,20
Clinical Features and Pathophysiology
PCOS is commonly associated with a triad of symptoms:
Insulin resistance is a central feature in many PCOS cases and is implicated in both the reproductive and metabolic abnormalities observed. This insulin resistance may lead to metabolic syndrome, a cluster of conditions—including abdominal obesity, dyslipidemia, hypertension, and glucose intolerance—that significantly elevate the risk of type 2 diabetes and cardiovascular disease. Although obesity exacerbates the clinical manifestations of PCOS, it is important to note that the syndrome also affects lean women, underscoring its multifactorial etiology.
Impact on Health and Quality of Life
Beyond reproductive implications such as infertility, PCOS can severely affect psychological well-being and long-term health outcomes. Mood disorders, including anxiety and depression, are more prevalent in women with PCOS. The chronic nature of the condition necessitates long-term management strategies to reduce both immediate and future risks.
Therapeutic Approaches
Currently, there is no definitive cure for PCOS; however, several therapeutic interventions are effective in managing its symptoms and associated comorbidities:
Risk Factors of Polycystic Ovary Syndrome (PCOS)
Polycystic Ovary Syndrome (PCOS) is a multifaceted endocrine and metabolic disorder arising from the interplay of genetic, hormonal, metabolic, environmental, and psychological factors. Understanding the risk landscape is critical for early diagnosis, individualized management, and improved long-term outcomes.
Non-Genetic Factors
Environmental Toxins - Exposure to environmental toxins particularly endocrine-disrupting chemicals (EDCs) has been implicated in the pathogenesis of PCOS. These compounds, which include industrial pollutants, tobacco smoke, heavy metals (e.g., lead, mercury), and agricultural pesticides, disrupt endocrine homeostasis by mimicking or blocking hormonal signalling. Entry into the human body occurs via inhalation, dermal contact, or ingestion, ultimately affecting hormone receptor sensitivity and synthesis pathways, thereby exacerbating reproductive and metabolic abnormalities associated with PCOS.
Obesity and Dietary Patterns Obesity is a well-established risk factor that not only contributes to the onset of PCOS but also amplifies its clinical severity. Excess adiposity, especially visceral fat, exacerbates hyperandrogenism, insulin resistance, hirsutism, and menstrual irregularities. Modern sedentary lifestyles combined with energy-dense, nutrient-poor diets play a critical role in weight gain, metabolic dysregulation, and reproductive dysfunction. Even in non-obese individuals, unhealthy dietary patterns and poor physical activity levels can independently contribute to metabolic and reproductive manifestations of PCOS.
Genetic Factors
PCOS has a strong familial component, suggesting a heritable predisposition. Genome-wide association studies (GWAS) have identified several susceptibility genes, particularly those involved in steroidogenesis, insulin signalling, and gonadotropin action.
Women with a first-degree relative diagnosed with PCOS are significantly more likely to develop the disorder, highlighting the importance of genetic screening in at-risk populations. A deeper understanding of these genetic contributors paves the way for targeted and precision-based interventions.
Hormonal Dysregulation
PCOS is fundamentally characterized by hyperandrogenism, often evidenced by elevated serum testosterone, 17-hydroxyprogesterone, and a raised Free Androgen Index (FAI). A hallmark of the condition is an elevated LH:FSH ratio, which disrupts normal folliculogenesis and ovulatory processes, leading to anovulation and polycystic ovarian morphology.
Additionally, insulin resistance (IR)present in up to 70% of women with PCOS contributes to hyperinsulinemia, which in turn:
This complex endocrine dysfunction lies at the core of PCOS pathophysiology and contributes to its reproductive and metabolic sequelae.
Psychosocial and Emotional Factors
Emotional Disturbance
Psychological distress, including chronic stress, anxiety, and depression, has emerged as a significant modifiable risk factor in the onset and progression of PCOS. Dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis due to prolonged psychological stress can impair gonadotropin-releasing hormone (GnRH) pulsatility, exacerbating menstrual irregularities and hormonal imbalance.
The bidirectional relationship between emotional health and PCOS creates a self-perpetuating cycle whereby PCOS symptoms contribute to emotional disturbance, which in turn worsens endocrine function and metabolic health.
Stress, Anxiety, and Depression
Numerous studies have highlighted higher incidences of anxiety disorders, depression, mood instability, and sleep disturbances among women with PCOS. These conditions may arise secondary to poor self-image (due to acne, hirsutism, or infertility), but also act as contributing factors via neuroendocrine modulation particularly elevated cortisol levels which further disrupt insulin and androgen balance.
Holistic management strategies should therefore encompass mental health interventions alongside endocrine therapies to break this cycle and improve overall patient outcomes.
Family History
A positive family history especially among first-degree female relatives is a strong risk factor for developing PCOS. Familial aggregation suggests that hereditary and epigenetic mechanisms play a significant role in disease etiology. Studies report that daughters and sisters of affected individuals often share phenotypic traits such as irregular menstruation, insulin resistance, and hyperandrogenism.
Understanding familial patterns can facilitate early screening, risk stratification, and preventive lifestyle counselling in genetically predisposed populations.
Lifestyle Factors
Lifestyle behaviours, including poor nutrition, lack of exercise, smoking, and irregular sleep patterns, contribute significantly to the development and exacerbation of PCOS symptoms. Specific risk behaviours include:
Given the modifiable nature of these factors, structured lifestyle interventions focused on weight management, exercise, and dietary optimization are cornerstones of PCOS management and prevention.22,23
Clinical Diagnosis of PCOS
Diagnosing PCOS requires a comprehensive evaluation since no single test is definitive. The widely accepted Rotterdam criteria require the presence of at least two of the following three features:
To rule out other endocrine disorders and confirm the diagnosis, a PCOD panel is commonly performed, which includes testing levels of LH, FSH, TSH, Prolactin, and androgens (Testosterone, DHEAS, SHBG).
Vitamin D deficiency, commonly observed in PCOS patients, may worsen clinical outcomes. Hence, screening for serum 25(OH)D levels is also recommended.
Early and accurate diagnosis is essential for preventing long-term complications such as infertility, metabolic syndrome, type 2 diabetes, and cardiovascular disease.24,25
Scientific Studies Supporting Allopathic Approaches in PCOS
The following table highlights selected studies involving both human and animal models that demonstrate the efficacy of conventional treatments in PCOS:
|
Sr No. |
Publication |
Model Used |
Year |
|
1 |
Otaghi, M., Azami, M., Khorshidi |
Human (female subjects) |
2019 |
|
2 |
Nguo K., McGowan M., Cowan S. |
Cat, Dog, Rabbit |
2021 |
|
3 |
Srnovršnik T., Virant-Klun I., Pinter B. |
Rat, Zebrafish, Rodents |
2023 |
|
4 |
Anam S. Kalsekar |
Mouse |
2024 |
|
5 |
Laganà A. S., Myers S. H., Forte |
Mouse |
2024 |
These studies highlight the importance of both clinical and preclinical models in understanding the pharmacodynamics, therapeutic effectiveness, and systemic impact of conventional drugs on PCOS-related pathophysiology.26,27,28,29
Treatment of PCOS
While PCOS is considered a chronic, incurable condition, its symptoms and long-term risks can be effectively managed through lifestyle modification, pharmacological therapy, and nutritional supplementation.
1. Lifestyle Management
Lifestyle intervention is the first-line approach, especially for overweight or obese patients:
2. Pharmacological Interventions
3. Nutritional Supplementation
4. Behavioural and Supportive Therapies
Psychological counselling and support groups may benefit those suffering from anxiety, depression, or body image issues due to PCOS.30,31,32,33
Allopathic Treatment of Polycystic Ovary Syndrome (PCOS)
Allopathic or conventional medicine is one of the most widely used and evidence-based approaches for managing Polycystic Ovary Syndrome (PCOS). The goal of treatment is typically symptom-specific, addressing issues such as irregular ovulation, insulin resistance, hyperandrogenism, and associated metabolic dysfunctions.
Allopathic treatments remain an essential part of PCOS management, particularly for symptom control and fertility enhancement. However, patient-centered care that integrates pharmaceutical therapy with lifestyle changes and alternative remedies may offer the most balanced and effective approach for long-term health and quality of life in women with PCOS.
Allopathic medications are often prescribed as part of a comprehensive management plan that includes lifestyle modifications, dietary changes, and regular follow-up.
Commonly Prescribed Allopathic Medications
|
Medication |
Primary Action |
|
Clomiphene Citrate |
Induces ovulation by stimulating FSH and LH production. Widely used in infertility. |
|
Metformin |
Improves insulin sensitivity and helps regulate menstrual cycles. |
|
Letrozole |
Aromatase inhibitor used as an alternative to clomiphene for ovulation induction. |
|
Tamoxifen |
Selective estrogen receptor modulator; used when clomiphene resistance occurs. |
|
Troglitazone |
An insulin-sensitizing agent (withdrawn in some regions due to hepatotoxicity). |
|
Oral Contraceptives |
Regulate menstrual cycles, reduce androgen levels, and control acne and hirsutism. |
|
Anti-androgens |
Such as spironolactone, used to manage hirsutism and acne. |
Limitations of Allopathic Therapy
While effective, conventional pharmacotherapy may be associated with:
Use of Herbal Drugs in the Management of Polycystic Ovary Syndrome (PCOS)37,38,39,40
Polycystic Ovary Syndrome (PCOS) is a common endocrine disorder affecting women of reproductive age. While conventional medications such as hormonal contraceptives, metformin, and anti-androgens are widely used, many patients seek alternative therapies due to concerns about side effects and long-term use. Herbal medicines, derived from traditional systems like Ayurveda and Unani, are increasingly popular for their perceived safety, affordability, and holistic action on hormonal regulation, metabolism, and reproductive function.
Several medicinal plants have shown promising effects in reducing PCOS symptoms such as irregular menstruation, insulin resistance, obesity, and ovarian cysts. The table below summarizes key herbs commonly used in traditional medicine systems for PCOS management:
Table no.1 Use of Herbal Drugs in (PCOS)
|
Sr no |
Plant name |
Part used |
Known Benefits in PCOS |
|
1 |
Aloe barbadensis |
leaves |
Regulates menstruation, improves insulin sensitivity |
|
2 |
Saricaasoca |
bark |
Uterine tonic, regulates menstrual cycle |
|
3 |
Terminalia arjuna |
bark |
Cardioprotective, supports lipid metabolism |
|
4 |
Solanum nigrum |
leaves |
Anti-inflammatory, detoxification support |
|
5 |
Withaniasomnifera |
friuts |
Adaptogen, reduces stress, balances hormones |
|
6 |
Nardostachysjatamansi |
root |
Nervine tonic, reduces anxiety, balances endocrine function |
|
7 |
Ambromaaugusta |
Root/ root bark |
Emmenagogue, promotes menstrual flow |
|
8 |
Ficus glomerata |
Leaves, bark, friut |
Astringent, reduces excessive bleeding, anti-diabetic |
|
9 |
Symplocosracemosa |
Bark |
Uterine tonic, regulates ovulation |
|
10 |
Parmeliaperlata |
Flower |
Cooling agent, used in menstrual irregularities |
|
11 |
Mimosa pudica |
Whole plant |
Anti-inflammatory, anti-diabetic, supports fertility |
CONCLUSION
Polycystic Ovary Syndrome (PCOS) is a complex and multifactorial endocrine disorder affecting a significant proportion of women of reproductive age. Characterized by hormonal imbalance, irregular ovulation, insulin resistance, and polycystic ovaries, PCOS not only impairs fertility but also increases the risk of long-term complications such as type 2 diabetes, cardiovascular disease, and endometrial cancer. The clinical presentation of PCOS varies widely, necessitating a personalized and multidisciplinary approach to its diagnosis and management.
Conventional treatments such as hormonal therapy, insulin sensitizers, and lifestyle interventions remain the cornerstone of PCOS management. However, their limitations, including side effects and the need for lifelong use, have led to growing interest in complementary therapies, particularly herbal medicine. Various medicinal plants with hormonal, anti-inflammatory, antioxidant, and insulin-sensitizing properties have shown promising results in mitigating PCOS symptoms, either alone or as adjuncts to modern treatments.
Despite their widespread use, the clinical efficacy and safety of herbal remedies require more rigorous scientific validation through well-designed clinical trials. Future strategies should aim at an integrative treatment approach, combining the benefits of conventional medicine with evidence-based herbal therapies and lifestyle modifications.
REFERENCES


Rujuta Shinde*, Dr. Ramesh Ingole, Nisha Kanse, Polycystic Ovary Syndrome (PCOS): An Overview of Symptoms, Causes, and Therapeutic Approaches, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 2497-2509. https://doi.org/10.5281/zenodo.15650893
 10.5281/zenodo.15650893
10.5281/zenodo.15650893
