1 Department of Pharmacology, Government Medical College, Nagapattinam, Tamil Nadu, India.
2,3,4 Edayathangudy. G. S Pillay College of Pharmacy, Nagapattinam, Tamil Nadu, India.
Steven–Johnson syndrome is one of the serious adverse drug reactions affecting the skin and mucous membrane. The causative drugs include Sulfonamides, Anticonvulsants, NSAIDs, Anti-gout medications etc. Here, a 52-year-old female developed peeling of skin, swelling and blackish discoloration in the lips, and generalized itching all over the body after the administration of 1 g of INJ. Ceftriaxone. This drug was suspected to have caused the serious reaction and was stopped after the first dose. The patient was treated with corticosteroids and antihistamines.
An eruptive fever with stomatitis and ophthalmia was described as a severe form of erythema multiforme and was named by Steven and Johnson in 1922. By the 1940s, it was commonly referred to as "Steven Johnson's syndrome (SJS)." The concept of the spectrum of erythema multiforme has been widely acknowledged since that time.[1]
SJS is an immune-mediated hypersensitivity reaction that can be triggered by various etiological factors, including medications like vaccinations, infections, cancer, and radiation therapy. Among these, drug-induced reactions are the most common cause for SJS.[3]
Stevens-Johnson syndrome and toxic epidermal necrolysis (SJS/TEN), are characterized by the detachment of the epidermis and mucous membranes, which are rare but severe cutaneous adverse reactions. SJS/TEN can be life-threatening, with mortality rates ranging from 4.8% to 14.8%.[4]
CASE PRESENTATION:
A 52-year-old female presented with the complaint of dysuria and fever, diagnose as Urinary tract infection. Patient was treated with INJ. Ceftriaxone 1g IV BD. Within an hour of first dose, the patient developed peeling of skin and lips, blackish discoloration of lips and itching all over the body.
PAST HISTORY:
Patient is known hypertensive and is on regular medication with Tab. Amlodipine 5mg BD.
Patient had no significant previous drug allergies and had no familial history of similar cutaneous conditions or autoimmune disorders.
VITAL SIGN AND PHYSICAL EXAMINATION
Examination revealed stable hemodynamics with a temperature of 37.2°C, blood pressure of 140/80 mmHg, and a normal heart rate of 82 beats per minute. The respiratory rate remained stable at 16 breaths per minute, with oxygen saturation maintaining at 99% on room air. Cardiovascular examination demonstrated normal heart sounds without any murmurs or additional heart sounds. Respiratory examination revealed normal vesicular breath sounds bilaterally without any added sounds.
LAB INVESTIGATION:
The total white blood cell count was marginally elevated at 21.8 x 103 cells/µL. Hemoglobin was 11.9 g/dl and platelet were 325 x 103/µL counts remained within normal parameters [20]. Biochemical analysis of liver function tests, alanine aminotransferase (ALT) at 29 U/L and aspartate aminotransferase (AST) at 29 U/L were within normal range. Renal function tests including serum creatinine was 0.9 mg/dL and urea was 26 mg/dL, which were within normal limits.
COURSE IN THE HOSPITAL:
This serious adverse reaction was reported to Adverse drug monitoring center, Government Medical College, Nagapattinam.
The decision made was to stop the drug and casualty assessment was done using Naranjo scale and was found to be Probable. The patient was referred to the dermatologist for opinion and was diagnosed as Ceftriaxone-induced Steven-Johnson Syndrome. And the patient was treated with antihistamines (Tab. Cetirizine 10mg HS) and systemic corticosteroids (INJ. Dexamethasone 6mg IM OD). Over the next 7 days, there was marked clinical improvement in patient. The patient was discharged on day 14, after partially recovering from the reaction.
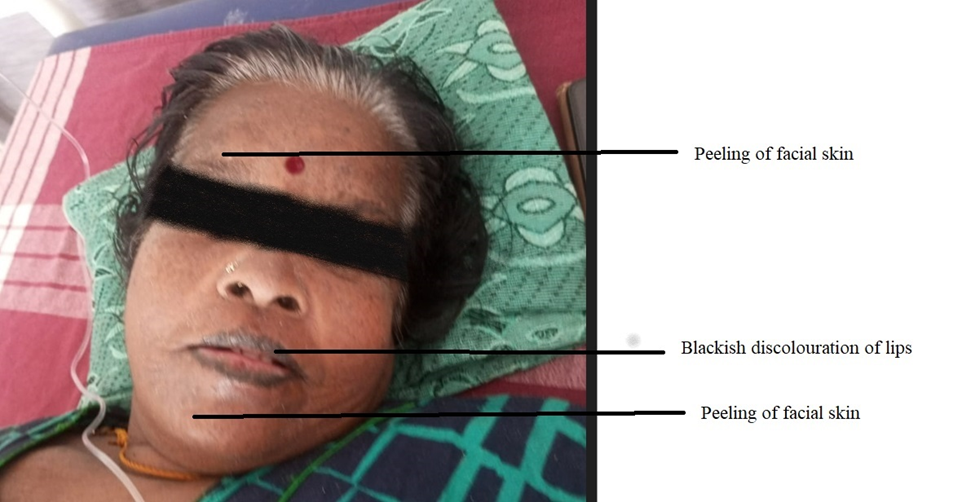
FIG:1 This figure shows peeling of facial skin; blackish discoloration of lips: which was attributed to Ceftriaxone-induced SJS.
DISCUSSION:
Early identification of the adverse reaction, along with the swift action and cessation of the potential causative drugs, is crucial for achieving a favorable outcome. The early commencement of substantial oral nutrition is essential to minimize protein loss, thereby promoting healing and reducing the risk of stress-induced ulcers. For many years, corticosteroids have been the cornerstone of therapy for SJS in most instances.[2]
If any primary symptoms arise, they must be reported to a healthcare professional or physician regarding the drug and treated with anticoagulants, corticosteroids, carbamazepine, lamotrigine, phenytoin, phenobarbital, allopurinol, nevirapine, sulfamethoxazole, etc. Monitoring often provides essential initial care for the patient and helps prevent complications associated with the disease. [5,6]
A 2024 study of the Russian National Pharmacovigilance database found ceftriaxone was the third most implicated drug in Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN) cases, after lamotrigine and ibuprofen. Which implicates the necessary for cautious prescription of an empirical antibiotic.[7]
Specific drug hypersensitivity leads to the presentation of drugs that are restricted by major histocompatibility class I, followed by an increase in cytotoxic T -lymphocytes. This results in the infiltration of skin lesions with cytotoxic T-lymphocytes and natural killer cells. Granulysin is likely the key mediator responsible for the widespread death of keratinocytes in SJS/TEN.[6] The levels of granulysin in the sera of patients with SJS/TEN are significantly higher than those found in patients with standard drug-induced skin reactions or healthy individuals.[6] Moreover, granulysin levels correlate with the severity of the clinical condition. The mechanism is not mediated by IgE, and desensitization to the triggering drug is not an option.[1]
CONCLUSION:
Steven–Johnson syndrome (SJS) is a rare yet serious adverse drug reaction that necessitates early diagnosis to mitigate morbidity and mortality. Immediate cessation of the suspected offending drug is crucial for preventing further progression of the reaction and can enhance better patient outcomes. Administering test dose prior to Ceftriaxone administration can assist in identifying potential hypersensitivity and decrease the likelihood of severe reactions. Clinical pharmacists play an essential role in reporting adverse drug reactions (ADRs) to pharmacovigilance programs, thus raising awareness among healthcare professionals and students in various institutions. Educational initiatives and the dissemination of such case reports can enhance drug safety practices and boost preparedness for managing severe ADRs.
REFERENCES




Dr. Deepak Kumar T., Ramakrishnan S., Padhma M., Siddha Vidhyar Dhani R., Ceftriaxone Induced Steven-Johnson Syndrome: A Rare Case Report, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 9, 1419-1422. https://doi.org/10.5281/zenodo.17112851
 10.5281/zenodo.17112851
10.5281/zenodo.17112851
