Institute of Pharmaceutical Science & Research, Balaghat (M.P.).
Anemia is one of the most common nutritional and hematological disorders worldwide, characterized by a reduction in hemoglobin concentration and a decreased oxygen-carrying capacity of blood. It affects individuals of all age groups, particularly women and children, and remains a major public health concern, especially in developing countries. Despite the availability of conventional iron supplements, their use is often limited due to side effects such as gastrointestinal irritation, poor absorption, and low patient compliance.In recent years, there has been growing interest in herbal and phytopharmaceutical approaches as safer and more effective alternatives for the management of anemia. Medicinal plants rich in iron, antioxidants, and bioactive compounds offer a multi-targeted mechanism, including enhancement of hemoglobin synthesis, protection of red blood cells, and improvement of overall health status.The present review focuses on the therapeutic potential of selected medicinal plants, namely Moringa oleifera, Boerhavia diffusa, Rubia cordifolia, and Phoenix dactylifera, which have been traditionally used for their hematinic and restorative properties. These plants are known to contain essential nutrients such as iron, vitamins, flavonoids, and alkaloids that contribute to their anti-anemic activity. Literature evidence suggests that these herbs not only help in increasing hemoglobin levels but also exhibit antioxidant, hepatoprotective, and immunomodulatory effects, which further support erythropoiesis.
1.1 Anemia: Definition & Global Burden
Anemia is a clinical condition characterized by a decrease in the number of red blood cells (RBCs) or a reduction in hemoglobin concentration, leading to impaired oxygen transport in the body. According to the World Health Organization, anemia is defined as a hemoglobin level below 13 g/dL in men and 12 g/dL in women. It is considered a major global health issue affecting both developed and developing nations.
The burden of anemia is particularly high in countries like India, where nutritional deficiencies, poor dietary habits, and socioeconomic factors contribute significantly to its prevalence. Women of reproductive age, pregnant women, and children are the most affected groups. Anemia not only reduces physical performance and cognitive function but also increases morbidity and mortality rates. [1]
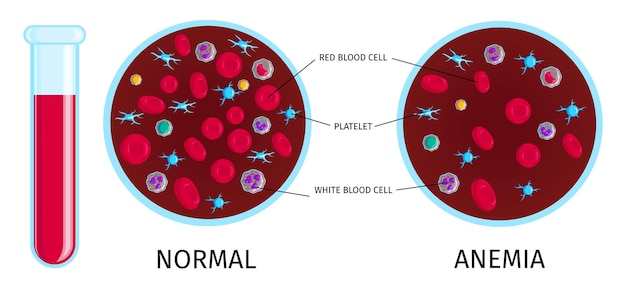
Figure 1: Anemia
1.2 Types of Anemia
Iron Deficiency Anemia
Iron deficiency anemia is the most common type of anemia worldwide and occurs due to insufficient iron levels required for hemoglobin synthesis. It may result from poor dietary intake, chronic blood loss, or malabsorption. Symptoms include fatigue, weakness, pale skin, and shortness of breath.
Hemolytic Anemia
Hemolytic anemia arises from the premature destruction of red blood cells, exceeding the body’s ability to produce new ones. This condition may be caused by genetic disorders, infections, autoimmune diseases, or exposure to certain drugs and toxins.
Megaloblastic Anemia
Megaloblastic anemia is characterized by the presence of abnormally large and immature red blood cells due to impaired DNA synthesis. It is mainly caused by deficiencies of vitamin B12 and folic acid, leading to ineffective erythropoiesis. [2]
1.3 Pathophysiology of Anemia
The development of anemia involves multiple underlying mechanisms, primarily related to impaired red blood cell production, increased destruction, or blood loss. Iron plays a crucial role in hemoglobin formation, and its deficiency directly affects oxygen transport capacity.
In addition, an imbalance between RBC production and destruction contributes significantly to the condition. Factors such as nutritional deficiencies, bone marrow dysfunction, oxidative stress, and chronic diseases can disrupt normal erythropoiesis, resulting in decreased hemoglobin levels and reduced oxygen delivery to tissues. [3]
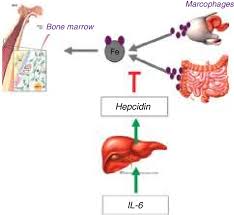
Figure 2: Pathophysiology of Anemia
1.4 Limitations of Conventional Therapy
Conventional treatment of anemia mainly involves iron supplementation and vitamin therapy. Although these treatments are effective, they are often associated with several limitations. Common side effects of iron supplements include gastrointestinal discomfort, nausea, constipation, and metallic taste, which reduce patient compliance.
Furthermore, poor absorption of iron and the need for long-term therapy can lead to inconsistent treatment outcomes. In some cases, excessive iron intake may also cause toxicity and oxidative stress, further complicating the condition. [4]
1.5 Need for Herbal/Phytopharmaceutical Approach
Due to the limitations of conventional therapy, there is increasing interest in the use of herbal and phytopharmaceutical approaches for the management of anemia. Medicinal plants offer a safer and more holistic alternative, as they are generally well-tolerated and have fewer side effects.
Herbal formulations often contain a combination of bioactive compounds such as iron, flavonoids, alkaloids, and vitamins, which act synergistically to improve hemoglobin levels, enhance iron absorption, and protect red blood cells from oxidative damage. This multi-targeted action makes phytopharmaceuticals a promising approach for effective and sustainable anemia management. [5]
2. Plants Profiles
2.1 Moringa oleifera (Sahjan)
Botanical Description
Moringa oleifera is a fast-growing, drought-resistant tree commonly found in tropical and subtropical regions. [6]It belongs to the family Moringaceae and is widely known as the drumstick tree. The leaves are small, green, and highly nutritious, while the pods are long and slender. Almost all parts of the plant are used in traditional medicine. [7]
Phytoconstituents
The leaves of Moringa oleifera are rich in essential nutrients and bioactive compounds, including iron, calcium, vitamin C, β-carotene, flavonoids, and phenolic compounds. These constituents contribute to its strong antioxidant and nutritional properties. [8]
Anti-Anemic Activity Studies
Several experimental studies have demonstrated that Moringa oleifera leaf extract significantly increases hemoglobin levels and red blood cell count. Its high iron content, along with vitamin C, enhances iron absorption and improves hematological parameters, making it a potent natural remedy for anemia. [9]

Figure 3: Moringa oleifera (Sahjan)
2.2 Boerhavia diffusa (Punarnava)
Traditional Uses (Ayurveda)
Boerhavia diffusa, commonly known as Punarnava, has been extensively used in Ayurvedic medicine for treating liver disorders, edema, inflammation, and anemia. It is considered a rejuvenating herb that helps restore normal body functions. [11]
Hepatoprotective Role
Punarnava exhibits strong hepatoprotective activity, helping to protect liver cells from damage caused by toxins and oxidative stress. [12]Since the liver plays a key role in iron metabolism and erythropoiesis, its protection indirectly supports the management of anemia. [13]
Hematopoietic Activity
Studies suggest that Boerhavia diffusa enhances the production of blood cells by stimulating bone marrow activity. It also improves overall blood quality and supports the recovery of hemoglobin levels in anemic conditions. [14]

Figure 4: Boerhavia diffusa (Punarnava)
2.3 Rubia cordifolia (Manjistha)
Blood Purification Properties
Rubia cordifolia is widely known for its blood-purifying properties in traditional systems of medicine. It helps in removing toxins from the blood and improving circulation, thereby supporting overall hematological health. [15]
Antioxidant Role in RBC Protection
Manjistha contains potent antioxidant compounds that protect red blood cells from oxidative damage. By reducing oxidative stress, it helps prevent premature destruction of RBCs and maintains their structural integrity. [16]

Figure 5: Rubia cordifolia (Manjistha)
2.4 Phoenix dactylifera (Khajoor)
Nutritional Profile
Phoenix dactylifera, commonly known as dates, is a highly nutritious fruit rich in carbohydrates, iron, vitamins, and minerals. [17] It serves as a natural source of energy and essential nutrients required for maintaining healthy blood levels. [18]
Iron and Energy Boosting Role
Dates are particularly beneficial in anemia due to their iron content, which supports hemoglobin synthesis. Additionally, their natural sugars provide instant energy, helping to combat fatigue and weakness associated with anemia. [19]

Figure 6: Phoenix dactylifera (Khajoor)
Table 1: Selected Medicinal Plants and Their Anti-Anemic Properties
|
Plant Name |
Part Used |
Key Constituents |
Pharmacological Activity |
Role in Anemia |
|
Moringa oleifera |
Leaves |
Iron, Vitamin C, Flavonoids |
Hematinic, Antioxidant |
Increases Hb, enhances iron absorption |
|
Boerhavia diffusa |
Root/Whole plant |
Alkaloids, Punarnavine |
Hepatoprotective, Hematopoietic |
Stimulates RBC production |
|
Rubia cordifolia |
Root |
Anthraquinones, Tannins |
Blood purifier, Antioxidant |
Protects RBCs |
|
Phoenix dactylifera |
Fruit |
Iron, Sugars, Vitamins |
Hematinic, Energy booster |
Improves Hb & energy |
3. Phytochemical Constituents Responsible for Anti-Anemic Activity
The effectiveness of herbal formulations in anemia management is largely attributed to the presence of various bioactive compounds:
Iron Content
Iron is a vital component required for hemoglobin synthesis. Plant-based iron, when combined with absorption enhancers, contributes significantly to improving blood parameters.
Flavonoids
Flavonoids possess strong antioxidant properties that help in reducing oxidative stress and protecting red blood cells from damage. [20]
Alkaloids
Alkaloids are known to stimulate physiological processes, including hematopoiesis, and contribute to overall blood health.
Phenolic Compounds
Phenolic compounds act as antioxidants and play a protective role against cellular damage, thereby supporting RBC stability.
Vitamins (Role of Vitamin C in Iron Absorption)
Vitamin C enhances the absorption of non-heme iron from plant sources by converting it into a more absorbable form, thereby improving its bioavailability and effectiveness in treating anemia. [21]
Table 2: Phytochemicals Responsible for Anti-Anemic Activity
|
Phytochemical |
Source |
Mechanism |
Effect |
|
Iron |
Moringa, Dates |
Hemoglobin synthesis |
↑ Hb levels |
|
Flavonoids |
All plants |
Antioxidant action |
Protect RBCs |
|
Alkaloids |
Punarnava |
Stimulate bone marrow |
↑ RBC production |
|
Phenolics |
Manjistha |
Reduce oxidative stress |
Prevent RBC damage |
|
Vitamin C |
Moringa |
Enhances iron absorption |
↑ Bioavailability |
4. Mechanism of Action of herbal Formulation
The polyherbal formulation exerts its anti-anemic effect through multiple mechanisms:
Iron Supplementation
Herbs like Moringa oleifera and Phoenix dactylifera provide a natural source of iron, which directly contributes to hemoglobin synthesis.
Enhancement of Erythropoiesis
The formulation stimulates the production of red blood cells by supporting bone marrow function and improving overall nutritional status. [22]
Antioxidant Protection
The presence of flavonoids and phenolic compounds helps in reducing oxidative stress, thereby protecting RBCs from premature destruction.
Liver Support (Erythropoietin Regulation)
Herbs such as Boerhavia diffusa support liver function, which plays an important role in regulating erythropoietin and maintaining normal blood cell production. [23]
Polyherbal Syrup
↓
Active Phytoconstituents
(Iron, Flavonoids, Alkaloids)
↓
Multiple Actions:
↓ ↓ ↓
Iron Supply Antioxidant Liver Support
↓ ↓ ↓
↑ Hb Synthesis ↓ RBC Damage ↑ Erythropoietin
↓ ↓ ↓
Improved RBC Production
↓
Management of Anemia
Figure 7: Mechanism of Action of herbal Formulation
5. Formulation Aspects of Herbal Syrup
5.1 Advantages of Syrup Dosage Form
Patient Compliance
Herbal syrups are generally well accepted by patients due to their pleasant taste and ease of administration. The liquid form allows for flexible dosing and is especially beneficial for individuals who have difficulty swallowing tablets or capsules. The addition of natural or artificial sweeteners further improves palatability, thereby enhancing patient adherence to treatment. [24]
Pediatric and Geriatric Suitability
Syrup formulations are particularly suitable for pediatric and geriatric populations. Children often prefer liquid medications due to their sweet taste, while elderly patients benefit from the ease of swallowing and reduced risk of choking. Moreover, syrups allow for accurate dose adjustment according to age and body weight.
5.2 Excipients Used
Sweeteners
Sweeteners such as sucrose, glucose syrup, or honey are commonly used in herbal syrups to improve taste and mask the bitterness of plant extracts. They also contribute to the viscosity and overall stability of the formulation. [25]
Preservatives
Preservatives like sodium benzoate or parabens are added to prevent microbial growth and extend the shelf life of the syrup. Since herbal preparations are more prone to contamination, the use of suitable preservatives is essential for maintaining product safety.
Flavoring Agents
Flavoring agents such as fruit flavors (orange, lemon) or natural aromatic substances (cardamom, peppermint) are incorporated to enhance the organoleptic properties of the syrup. These agents make the formulation more appealing and acceptable to patients. [26]
5.3 Stability Considerations
pH
The pH of the herbal syrup plays a crucial role in maintaining its stability and effectiveness. An optimal pH helps in preventing degradation of active constituents and ensures compatibility of all ingredients in the formulation.
Microbial Stability
Due to the aqueous nature of syrups, they are susceptible to microbial contamination. Proper formulation with preservatives, along with hygienic manufacturing practices, is necessary to ensure microbial stability and safety during storage. [27]
6. Evaluation Parameters
6.1 Physicochemical Evaluation
pH
The pH of the formulation is measured to ensure stability, compatibility, and patient acceptability. It also influences the solubility and activity of the herbal constituents. [28]
Viscosity
Viscosity is an important parameter that affects the pourability and consistency of the syrup. An optimal viscosity ensures ease of administration while maintaining uniform distribution of active ingredients. [29]
Density
Density measurement helps in assessing the uniformity and concentration of the formulation. It is also useful for quality control and batch-to-batch consistency. [30]
Table 3: Evaluation Parameters of Herbal Syrup
|
Parameter |
Method |
Significance |
|
pH |
pH meter |
Stability & compatibility |
|
Viscosity |
Viscometer |
Pourability & consistency |
|
Density |
Pycnometer |
Uniformity |
|
Phytochemical tests |
Standard qualitative tests |
Presence of active compounds |
|
Microbial load |
Plate count method |
Safety |
6.2 Phytochemical Screening
Qualitative Tests
Preliminary phytochemical screening is carried out to identify the presence of various bioactive constituents such as alkaloids, flavonoids, tannins, saponins, and phenolic compounds. [31] These tests provide an initial confirmation of the therapeutic potential of the herbal formulation and ensure the presence of desired active components. [32]
DISCUSSION
The present review highlights the therapeutic potential of a polyherbal formulation composed of Moringa oleifera, Boerhavia diffusa, Rubia cordifolia, and Phoenix dactylifera in the management of anemia. The selection of these medicinal plants is based on their well-documented pharmacological activities and traditional use in improving blood health.
Synergistic Effect of Selected Herbs
The combination of these herbs exhibits a synergistic effect, where each component contributes through a different mechanism to enhance overall efficacy. Moringa oleifera and Phoenix dactylifera act as natural sources of iron and essential nutrients, directly supporting hemoglobin synthesis. Boerhavia diffusa plays a supportive role by improving liver function and promoting hematopoiesis, while Rubia cordifolia helps in blood purification and protection of red blood cells through its antioxidant properties. Together, these herbs work in a complementary manner to address multiple aspects of anemia.
Justification of Combination
The rationale behind combining these plants lies in their multi-dimensional therapeutic actions. Anemia is a complex condition involving nutritional deficiency, oxidative stress, and impaired erythropoiesis. A single-drug approach may not be sufficient to target all these factors effectively. Therefore, a polyherbal formulation provides a holistic approach by simultaneously enhancing iron availability, stimulating RBC production, improving metabolic functions, and protecting blood cells from damage.
Advantages over Synthetic Drugs
Compared to conventional iron supplements, herbal formulations offer several advantages. They are generally associated with fewer side effects, better tolerability, and improved patient compliance. Synthetic iron preparations often cause gastrointestinal discomfort and poor absorption, whereas plant-based formulations provide iron in a more bioavailable and natural form, often accompanied by absorption enhancers such as vitamin C. Additionally, the presence of antioxidants in herbal drugs helps in reducing oxidative stress, which is not addressed by conventional therapies.
CONCLUSION
The findings of this review suggest that polyherbal formulations possess significant potential in the management of anemia. The selected medicinal plants demonstrate promising hematinic, antioxidant, and supportive pharmacological activities, which collectively contribute to improving hemoglobin levels and overall blood health.
The use of a polyherbal approach offers a more comprehensive and balanced therapeutic strategy compared to single-agent treatments. It not only addresses iron deficiency but also supports erythropoiesis and protects red blood cells from oxidative damage.
Overall, such herbal formulations can be considered as a safe, effective, and economical alternative to conventional therapy. However, further experimental validation, including well-designed preclinical and clinical studies, is essential to establish their efficacy, safety, and standardization for wider clinical application.
REFERENCES



Shikha Lanjewar, Dr. Rajesh Mujariya, Dr. Atul Bisen, Dr. Manjeet Singh, Phytopharmaceutical Development and Assessment of Herbal Syrup for the Management of Anemia, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 4, 865-874 https://doi.org/10.5281/zenodo.19436708
 10.5281/zenodo.19436708
10.5281/zenodo.19436708
