School of Pharmacy, G H Raisoni University, Saikheda, Pandhurna, Madhya Pradesh, India
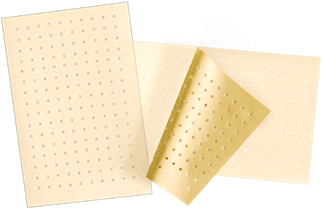
Recent strides in non-invasive drug delivery have spurred innovation in alternatives to traditional needle injections. Transdermal medication administration systems have surfaced as a notably auspicious methodology, exhibiting reduced incidences of rejection, straightforward application, and heightened patient compliance. The reviewed literature explores the use of transdermal patches and the anaesthetic drug mepivacaine as innovative means for controlled drug administration. Transdermal delivery functions by using body heat to activate the release of medication from the patch—either through dissolving fine drug layers within the adhesive or allowing diffusion from a reservoir through a semi-permeable membrane. Various analytical techniques are employed to assess the quality and performance of these patches, and quantifying film thickness, endurance of folding, and uniformity of drug content as well as release in vitro. In dental applications, these systems aim to address pain management while reducing anxiety associated with traditional injection-based anaesthesia. Mepivacaine, introduced in dental practice in the 1960s, remains a widely preferred local anaesthetic due to its balanced efficacy and safety. It is used both as a standalone option and as an alternative to lidocaine or articaine. Clinical results suggest that a 2-per cent mepivacaine solution with 1:20,000 levonordefrin films provides the same level of success (P = 0.69) and a similar degree of pain during the injection procedure, which proves its consistency in the handling of dental pain.
This is because the skin happens to be the largest organ in the body and it has an estimated surface area of about 1.5 to 2.0 square meters in adults, depending on individual body size and composition. From ancient times, as evidenced by humanity's most initial medical papers, substances have been put on the skin both for dealing with surface-level problems and as transdermal methods of giving medications to tackle health issues impacting the whole body, in addition to for beauty reasons. Regular application for transdermal delivery systems didn't become a widespread practice until the last third of the 20th century. Nicotine, a transdermal agent from the New World, was already being utilized in a plaster at that time. Unlike the more sophisticated medicated patches which were originally invented in China, early Western medicated plasters were relatively very basic, with only a single active ingredient in them. Documentaries available in the United States Pharmacopoeia (USP) some seventy years ago report a couple of instances of such plasters such as belladonna as a local anaesthetic, mustard used as an effective counterirritant, and salicylic acid as a keratolytic agent used to heal skin problems. These initial theories formed the basis of the development of contemporary transdermal drug delivery mechanisms.

Mustard plaster Belladonna plaster
Fig 1: 1800s-1900s
Delivering therapeutic substances via the skin enables them to avoid breakdown in the digestive system and the metabolic processing that occurs in the liver. This method allows the medication to be absorbed straight into the bloodstream, enhancing its effectiveness, preserving its chemical stability, and reducing adverse effects commonly linked to oral administration (Pastore, M.N., Kalia, Y.N., Horstmann, M. and Roberts, M.S.,, 2015).
Composition and operations of the skin
The biggest organ that is located in the body constitutes about 15 percent of body weight of an adult that is linked with mucous membrane of body surface.
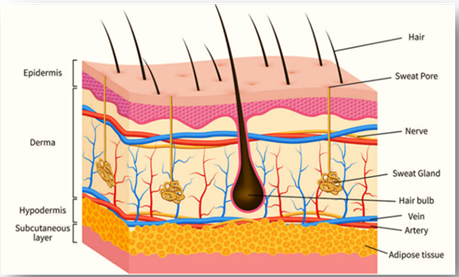
Fig. 2 Skin Anatomy
Epidermis
Epidermis refers to a stratified squamous cell mass that is made up largely by two type of cells, the keratinocytes and the immune cells. Other four typical categories of epidermis layers are classified by the placement and structure of the keratinocytes in their differentiation into horn-like cells and include: Skin consists of several layers, with the basal layer (stratum germinativum or basal cell layer) forming the lowest layer (Fig.1A), where new skin cells are produced; the squamous or spinous layer (stratum spinosum) that gives skin its basic structure and strength; the granular layer (stratum granulosum), in which cells begin to die and become hard, with the outermost keratinized strata corneum formed from toughened dead cells protecting body surfaces. The skin and its appendages are found in the integumentary system. The skin has 3 primary layers, epidermis, dermis and subcutaneous tissue.
The skin layer
Highly fibrous, filomasson and amorphous connective tissue in order to allow the transmission stimulus conduction when passing through the nerve systems and vessels, appageges with epiderm, fibroblasts, macrophages and mast cells compose the dermis. It has the dermis that forms the larger part of the skin that makes it flexible, elastic, and also, it is strong. The two sides have an agreement on the maintenance of the traits of each through the involvement of the germinal layers. The primary dermal material is collagen which is a fibrous protein family that comprises of at least 15 different and genetically different varieties that are found in human skin. The collagen fibers are in a dynamic process replacing the existing ones with new ones as they are being continuously degraded by proteolytic enzymes known as the sparse collagenases. The skin consists of 70 % of collagen. (Kolarsick, P.A., Kolarsick, M.A. and Goodwin, C, 2011).
Transdermal Drug Delivery System
Topical, cosmetic, and systemic delivery of medicine is now widely implemented with the use of transdermal patches. Their evolution reflects major progress in skin-related science and technological innovation, supported by continuous experimentation, laboratory testing, and clinical validation that trace their origins to some of the earliest forms of medical documentation in human history. TDDS systems are viewed as patient being friendly since they are Minimally invasive, they don’t require administration by professionals, reduce (GI) gastrointestinal side effects, and enhance patient adherence (Bird, D. and Ravindra, N.M., 2020). There are various advantages associated with the use of transdermal drug delivery systems, such as drug release that is controlled, and bioavailability, fewer adverse effects, and convenient application for patients. This delivery mechanism bypasses the first pass metabolism of the medication while eliminating the discomfort linked to injections; furthermore, the approach provides extended drug release with less frequent dosing through zero order kinetics, and the treatment can be conveniently activated at any moment (Sarangi, M.K. and Padhi, S., 2018).
Medication can enter the skin through three routes:
a) Via hair follicles.
b) Via sebaceous glands.
c) Via the sweat gland (Sharma, N., 2025).
Study Objectives
The following objectives are (Tayal, S., Jain, A. and Ansari, M.M.,, 2025)-
Advantages
Disadvantage
Transdermal Patch Types
a) Single-layer Adhesive Drug Delivery
The medicine in these kinds of patches is contained in the adhesive layer. The adhesive is one that does not only hold the different levels intact and hold the patch onto the skin but helps the drug to release itself. The system is also secured through a supporting layer and removable liner that cover the adhesive before it is used (Singh, S., Rajput, D.S., Gupta, N., Sharma, B., Rathi, S. and Singh, A.,, 2025).
b) The layered adhesive patch containing medication
A multilayer transdermal adhesive system operates in a manner similar to a single-layer type, as medication is released through its adhesive surfaces. The main difference is that it includes an extra layer infused with the active substance, sometimes divided by a thin barrier film. This design also incorporates a detachable liner and a durable support layer to maintain structure and protection (Mali, A.D., 2015).
c) Reservoir of drugs within the adhesive
In this configuration, the drug storage compartment is located between a non-permeable backing film and a membrane that precisely controls the rate of drug diffusion. This membrane—whether porous or solid—determines how quickly the medication is delivered. Inside the reservoir, the drug can exist as a liquid solution, gel, suspension, or be uniformly distributed within a polymer base. A skin-friendly adhesive polymer may serve as the external layer to ensure compatibility with the active compound (Galge, A.G. and Pagire, D., 2022). The backing film offers mechanical strength and protection, while the release of the drug occurs in a steady, zero-order manner. (Dhiman, S., Singh, T.G. and Rehni, A.K.,, 2011).
d) Drug matrix-in-adhesive
In a matrix-type system, the medication is embedded within a semisolid matrix layer. The adhesive layer of the patch only partially covers this drug-containing section. This configuration operates as a single-unit system, meaning the entire patch functions as one integrated delivery mechanism (Dhiman, S., Singh, T.G. and Rehni, A.K.,, 2011).
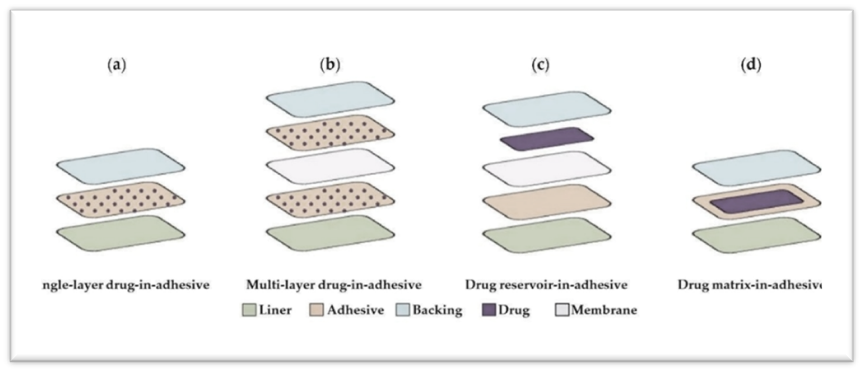
Fig 3 Types of transdermal Patch
Limitations of Transdermal Drug delivery System
Mechanism of transdermal Patch
Transdermal drug delivery systems (TDDS) are commonly grouped into three forms: matrix, reservoir, and drug-in-adhesive (DIA) types. In a matrix design, the medication is uniformly dispersed within a polymer network that modulates its diffusion rate. A DIA system embeds the therapeutic substance directly into the sticky layer that secures the patch to the skin. Conversely, the reservoir configuration stores the drug in a gel or liquid-filled chamber positioned beneath a rate-regulating membrane, which maintains controlled release and prevents seepage.The DIA patch is normally adopted when the medicine is easily absorbed through the skin and matrix as compared to the reservoir formulation which is normally used when the drug is either not compatible or has low solubility in the transdermal system. (Bird, D. and Ravindra, N.M., 2020).
Factors Affecting Transdermal Permeation
Factor affecting in transdermal permeation are
Biological factors
1) Dermatological issue
2) Age of the skin
3) Circulation of blood
4) Localised skin area
5) Metabolism of the skin
6) Variations among species
Physicochemical elements
1) Moisturising the skin
2) pH and Temperature
3) Coefficient of diffusion
4) Concentration of the drug
5) Coefficient of partition
6) Size and shape of molecules
Environmental influences
1) Sunlight
2) Chilly time of year
3) Pollution of the air (Gudur, A.S., Gode, S.S., Malpure, M.S. and Ghosalkar, N.S.,, 2025)
Evaluation parameters of transdermal patch
The evaluation parameter are (Bathe, R. and Kapoor, R., 2015):
A) Evaluation of physicochemical properties
B) Evaluation in vitro
C) Evaluation in living organisms
A) assessment of physicochemical properties
a) Width
b) Consistency of weight
c) Determination of drug content
d) Consistency of medication
e) Water content
f) Levelness
g) Endurance in Folding
h) Strength in tension
i) Characteristics of a tack
B) Assessment in a test tube
a) The disc under paddle
b) The USP Basket with modifications to the cylinder
c) The oscillating disc
d) Skin permeation system with horizontal design
e) Franz diffusion apparatus
f) Diffusion cell with flow-through system
C) In-vivo research
a) Models involving animals
b) Models of humans
A) Physicochemical Evaluation
a) Thickness: The use of a digital micrometer is necessary to calculate the distance between points that are marked on the medicated patch. The average thickness and standard deviation are calculated based on the obtained measurements and this assists in the determination of uniformity of the patch. The film’s thickness at various locations can also be assessed using tools like a handheld microscope, dial gauge, screw gauge, or micrometer. (Mahajan, K.C., Hande, A.S., Dama, G.Y., Shingote, A.H., Thorat, D.B. and Dambe, A.R.,, 2025).
b) Weight consistency: To measure consistency of weight, 4 patches of each giving were weighed on a digital scale individually. To ensure consistency during the formulation, the average weight and standard deviation were calculated. This evaluation ensures even drug distribution and reliable reproducibility of the transdermal patches (Karnakoti, A., Borade, A., Birajdar, P., Bodke, V., Dagale, M. and Badekar, R., 2025).
c) Determination of drug content: A film segment is cut off and carefully measured and dissolved in 100 milliliters of the solution which has the day in it. This mixture is continuously stirred in a magnetic stirrer for a duration of twenty-four hours. Before filtration, the entire solution undergoes sonication, and the drug concentration is measured spectrophotometrically with a suitable dilution (Manjhi, S. and Sahu, B., , 2025).
d) Evaluation of content consistency: Ten samples are chosen, and the content of the drug in them is tested separately. Provided that 9 of ten patches have between 85 percent and 115 percent of the target amount of drug and another patch has an amount between 75 percent and 125 percent, then the batch has passed the uniformity test. However, if up to three patches show drug content between 75% and 125%, an additional twenty patches are tested. If the results of these twenty samples fall within the 85% to 115% range, the transdermal patches are deemed to comply with the uniformity standards (Bathe, R. and Kapoor, R., 2015).
e) Moisture content: The stability and water-content of the transdermal patches were checked through the moisture analysis. The patches were weighed and then put in a desiccator with anhydrous calcium chloride in 72 hours to ascertain the percentage decrease in weight, the weight was calculated against the original. To test their hygroscopic characteristic, the patches were moved to a desiccator with a 75 percent relative humidity solution of potassium chloride (KCl) and the weight gain percentage was noted (Rao, N.R., Thejomoorthy, K., Mammen, M.V., Arora, P.K., Waidya, K.P., Kulkarni, P.A. and Rathi, S.,, 2025). The percentage of moisture content was calculated using the formula: % Moisture Content = (Initial Weight – Final Weight) / Initial Weight × 100 (Bathe, R. and Kapoor, R., 2015).
f) Flatness: A transdermal patch needs to be smooth, non-contractional over time in addition to an even surface and this can be checked by flatness test. In order to test flatness, a strip is selected out of the middle of the patch and two out of the sides. Measurements of the first and last length of each strip are taken and the percentage change is determined by the formula (I 1 1 -I 2 2)/I 1 1 ×100), the I 1 is the initial length of the strip and I 2 the final length of the strip (Bathe, R. and Kapoor, R., 2015). A value of 0% constriction indicates complete flatness (100 % flat).
g) Folding endurance is tried by repeated folding of a patch at the same point till it breaks or cracks. Its endurance value is determined by the number of times it can be folded without being torn (Kumari, R. and Sharma, V.K.,, 2025). This parameter indicates the flexibility and mechanical strength of the film. (Bathe, R. and Kapoor, R., 2015).
h) Tensile Strength: In tensile strength analysis, the polymer films are placed between two fixed plates made of iron. One terminal of the movie is fixed on a metal hook and the other on the string going over a pulley with weights added slowly on the other terminal. A pointer thread is applied to indicate the growth of the film till it ruptures. A pointer thread is used to note the extension of the film until it breaks. The tensile strength is then calculated based on the force required to rupture the film.
Tensile strength = F/a.b (1 + L/l)
Where,
i) Tack characteristics: Tack refers to a polymer’s capacity to stick to a surface under minimal pressure. This property depends on factors such as the polymer’s molecular weight, structural composition, and the presence of tackifying resins (Bathe, R. and Kapoor, R., 2015).
B) In vitro evaluation
a) The Paddle above Disc: (USP apparatus 5/ Ph Eur 2.9.4.1) This system is similar to the typical paddle dissolution device, only that the transdermal patch will be attached to a disc or cell attached to the bottom of a vessel holding the dissolution solvent at 32 ± 5 °C.
b) The Cylinder USP changing Basket: (USP apparatus 6 / Ph Eur 2.9.4.3) This kind is like the basket dissolution type except that the transdermal system is mounted on the outer side of a hollow rotating cylinder that is suspended in a medium of temperature 32 ± 5 0C.
c) The reciprocating disc: Here the patches are placed on holders which swing up and down in small containers of dissolution medium and is thus appropriate in systems that emit low drug levels. Similar purposes can also be served with the help of the Paddle over Extraction Cell (Ph. Eur. 2.9.4.2) method.
d) Horizontal skin permeation system: Widely applied to assess drug diffusion through the skin, this system features donor and receptor chambers, each holding around 3.5 ml of solution and covering a 0.64 cm² membrane area. Star-head magnetic stirrers rotating at 600 rpm ensure continuous mixing, while a thermostatic water jacket maintains constant temperature.
e) Franz diffusion cell: The model is composed of a donor and a receptor compartment, and the latter has volume of 5-12 ml and effective surface area of 1-5 cm². A magnetic stirrer operating at 600 rpm keeps the diffusion buffer in motion, while a surrounding water jacket regulates temperature via thermostatic circulation.
f) Flow-through diffusion cell: These cells are ideal for drugs with limited solubility in the receptor medium. The system can be automated and connected to HPLC for precise analysis. It includes a large donor chamber for adequate sample loading and a small receiving chamber (≈0.3 ml) to allow rapid removal of the permeated drug at controlled flow rates.
C) In vivo studies
In vivo evaluations provide accurate evidence of a drug’s therapeutic performance and enable the examination of physiological variables that cannot be effectively assessed through in vitro testing. Transdermal drug delivery systems (TDDS) are commonly studied both in animal and human models to determine their efficiency and safety. (Bathe, R. and Kapoor, R., 2015)
a) Animal Models: Since conducting clinical research on humans requires considerable time, cost, and ethical approval, preliminary studies are often carried out on animals. Species such as mice, hairless rats, rabbits, guinea pigs, hairless dogs, and rhesus monkeys are frequently chosen for these experiments. Hairless species are preferred because their skin more closely mimics human permeability and eliminates interference from fur. The rhesus monkey is regarded as one of the most reliable animal models for predicting human transdermal absorption and drug delivery outcomes.
b) Human Models: The final stage in developing a transdermal patch involves testing on human subjects to gather pharmacokinetic (drug movement) and pharmacodynamic (drug effect) data. The safety, efficacy and adverse effects of the patch are determined through clinical trials. Phase I is pre-clinical to establish the safety of the healthy volunteers, Phase II is to study the short-term safety and treatment efficacy in a sick individual, and Phase III is to confirm these results in a larger sample. Phase IV that takes place after the market launch, continues to monitor long-term safety and identifies any previously undetected side effects during real-world use. In as much as human studies are resource consuming, it is the most viable option of determining how the drug performs. (Bathe, R. and Kapoor, R., 2015)
Uses
Transdermal drug delivery systems are utilized for multiple skin conditions, as well as in treating angina pectoris, pain relief, smoking cessation, and neurological issues like Parkinson's
Table 1: List of marketed product
|
S.N. |
Product |
Active drug |
Types |
Purpose |
Reference |
|
1. |
Estraderm |
Estradiol |
Membrane |
Postmenstrual syndrome |
(Dhiman, S., Singh, T.G. and Rehni, A.K.,, 2011) |
|
2. |
MatrifenR |
Fentanyl |
Reservior |
Pain relief patch |
|
|
3. |
Ministran |
Nitroglycerine |
Drug in adhesive |
Angina pectoris |
|
|
4. |
Nicoderm CQ |
Nicotine |
Drug in adhesive |
Smoking cessation |
|
|
5. |
OxytrolR |
Oxybutynin |
Matrix |
Overactive bladder |
|
|
6. |
Captopress TTS |
Clonidine |
Membrane |
Hypertension |
|
|
7. |
Lidoderm |
Lidocaine |
Drug in adhesive |
Anesthetic |
|
|
8. |
Nuvelle TS |
Estradiol |
Drug in adhesive |
Hormone replacement therapy |
|
|
9. |
Habitraol |
Nicotine |
Drug in adhesive |
Smoking cessation |
|
|
10. |
Androderm |
Testesterone |
Membrane |
Hypogonadism in male |
Characterization Techniques for transdermal drug delivery systems
One of the most important items of TDDs is the assessment of its efficiency and effectiveness of delivery. The assessment procedures depend on the type and purposes of the drug. The three most used methods are the tape stripping, diffusion cells, and microscopic and spectroscopic examination among others with each having a different analysis technique. These techniques of characterization operate through either counting the quantity of drug in each layer of the surface being absorbed or by reflecting an imaged material in place of the drug in order to visually identify the pattern of absorption (Shah, S.W.A., Li, X., Yuan, H., Shen, H., Quan, S., Pan, G., Ishfaq, M., Shah, A.U., Xie, H. and Shao, J., , 2025).
Local anaesthetic
The initial anaesthetic, cocaine, was extracted in 1859 from the coca plant by Albert Niemann and utilized locally by Carl Koller in an eye surgery in 1884 (Ho, J.P.T., van Riet, T.C., Afrian, Y., Sem, K.T.C.J., Spijker, R., de Lange, J. and Lindeboom, J.A.,, 2021). Pain is the most common miseries in human and one of the most unbearable clinical symptoms in patient. At present, painkiller mainly include opioids and non-steroidal anti-inflammatory drug. However, these two type of drug have some side effect, for example opioids may causes respiratory depression, addiction, nausea, vomiting. Anti-inflammatory drug may cause coagulopathy, digestive tract ulcers, liver and kidney dysfunction, etc.The local anaesthetics, produced by a local reversible inhibition of sensory nerve impulses, has a long history of clinical use of over a hundred years. Local anaesthetic inhibit the possibility of the uploading of noxious stimuli to the central nervous system (Yu, S., Wang, B., Zhang, J. and Fang, K., , 2019). Among the different methods for pain management, local anaesthetics (LAs) are essential because they can deliver precise, reversible nerve block without causing overall sedation (Jeong, J.O., Kim, M., Kim, S., Lee, K.K. and Choi, H.,, 2025).
Mechanism of action of local anesthetics
Pain-block drugs have found number of ideas that have been trying to narrate how it works over many years. The most popular thought at this point is the receptor theory. It states that pain-block drugs attach to areas on wall of nerves. Then, they prevent the entry of Na + to the cell. In 1976, Strichartz wrote a piece. He said vigorous words of another thought. Like the mix of Ca+ & pain drugs, or shifts in the power at the cell & water line. He said drugs with amine (like lidocaine & others) go into the nerve. They cling to spots inside the wall, at spots that wake up when nerves fire. This blocks Na+ from getting in. So, the nerve sign can't travel. If the nerve's sign stops, the brain gets no call, & no pain is felt. (Rodrigues, G.A. and Bronzato, J.D, 2025).
Mepivacaine
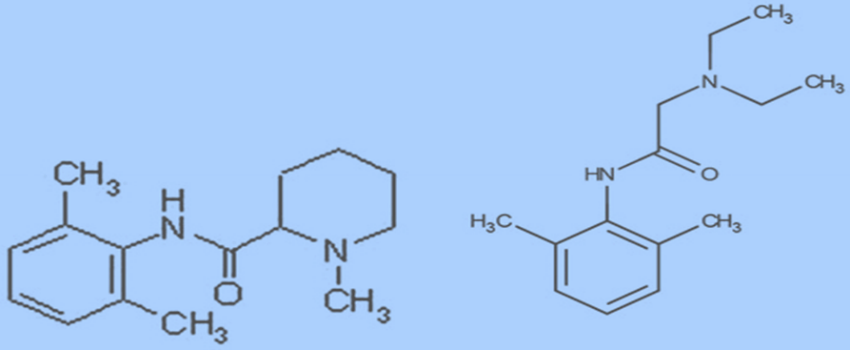
Fig 4: Structure of mepivacaine
Right now, used pain blocks all show key traits. These traits let them work well in the clinic. They keep their spot on the market too.Many see the mepivacaine type as a "safe" pick over lidocaine. It is for old or heart issue folks. It has no tight blood drug. It comes with levonordefrin. This drug is thought to have less strong heart press effects. It has 25% of the heart push effect. (Brockmann, W.G., 2014).Mepivacaine ranks as the third most commonly utilized anesthetic in dentistry, following articaine and lidocaine in certain regions.In tooth care, they give mepivacaine as a 3% mix. No vaso stuff in it. Or as a 2% mix. It has vaso stuff. Like 1:20,000 levonordefrin & 1:10,000 adrenaline. They give lidocaine as a 2% mix too. It has 1:10,000 or 1:50,000 adrenaline in it. (Su, N., Liu, Y., Yang, X., Shi, Z. and Huang, Y., 2014).The most you can take is 4.4 mg per kg. The top set dose is 300 mg. This is shown on the drug pack. Anvisa gave it a green light. Each shot is 3% mix & has 54 mg of mepivacaine. It is the most in it. For an 80 kg grown-up, the dose is 5.5 shots. (Rodrigues, G.A. and Bronzato, J.D., 2025). Mepivacaine acts as a numbing drug of medium length & shows low blood-vessel growth. It fits well for folks who can't stand epinephrine. (Datta, A., Mukherjee, B., Sood, S.K., Dutta, S., Barve, R., Pympallil, U., Ravindran, S., DUTTA, S. and PYMPALLIL, U.,, 2025).
Metabolism and distribution in relation to other local anesthetics
raw drug comes out in pee. It breaks down by adding OH to the main drug to make 3-OH-mepivacaine & 4-OH-mepivacaine. This is done by CYP1A2. CYP1A1 helps too but is not always there. CYP3A also helps make 4-OH-mepivacaine. A lot (over 50%) of the drug that goes out turns into OH types & they join with other stuff to leave the body. Pee tests show 3-OH-mepivacaine comes first. Then comes the 4-OH type, but there's less of it. This shows CYP1A does a lot. CYP3A takes a bit off the drug to make pipecoloxylidide, a small bit in pee. It's about 1%.Lidocaine breaks down in steps. Yet, CYP3A4 plays a big part in changing it to the main break-down part, mono ethyl glycinexylidide (MEGX). MEGX is a part that keeps the brain's nerve dead. CYP1A makes MEGX & 3-OH-lidocaine. 3-OH-lidocaine turns into 3-OH-MEGX.41 All end up as parts joined with glucuronide. MEGX turns to the not active part glycinexylidide (GX) & goes out the most via the kidneys. The rest of MEGX & GX break into 2,6-xylidine parts. The xylidine ring leaves by water-split acts with liver parts carboxylesterases or amidases.Prilocaine breaks down in the liver & kidneys. It does so by carboxylesterases & CYP3A4. This makes o-toluidine. CYP2E1 then makes toluidine forms. These are more than 40% of prilocaine in pee. O-toluidine & its forms can turn hemoglobin into methemoglobin. This is a big limit for using prilocaine. Prilocaine reacts with some drugs. Mostly with CYP3A4 inducers like carbamazepine, phenytoin, & rifampin. Or with stuff that leads to methemoglobinemia, like benzocaine, nitrates, or acetaminophen. Articaine breaks down fast & easy. This is due to its ester link with the carboxyl group. It turns into articainic acid fast by plasma carboxylesterases. Its half-life in the body is 20 minutes. Forty to 70% goes out as articainic acid. Four to 15% goes out as articainic acid glucuronide. Most key P450 cytochromes are in play in breaking down articaine. Yet, only 10% of the total dose is dealt with by cytochromes. This makes articaine not so prone to drug interaction issues. (Brockmann, W.G., 2014).
Table 2: List of transdermal patches containing drugs
|
Sr. No. |
Drug name |
Bioavailability |
Dose |
Release |
Ingredient |
Method |
Reference |
|
1. |
Fentanyl |
90% |
25-100 μg/h |
72h |
Ethylene vinyl acetate adhesive |
Reservoir |
(Nelson, L. and Schwaner, R., , 2009) |
|
2. |
Buprenorphine |
60% |
5-20 μg/h |
7days |
Polyisobutylene adhesive |
Matrix |
(Poliwoda, S., Noor, N., Jenkins, J.S., Stark, C.W., Steib, M., Hasoon, J., Varrassi, G., Urits, I., Viswanath, O., Kaye, A.M. and Kaye, A.D.,, 2022) |
|
3. |
Nicotine |
80-90% |
7-21 mg/h |
16-24h |
Hydrogel adhesive |
Matrix |
(Davaran, S., Rashidi, M.R., Khandaghi, R. and Hashemi, M.,, 2005) |
|
4. |
Lidocaine |
35% |
700 mg |
12hr |
Polyacrylate adhesive |
Matrix |
(Chopra, N., Chaudhuri, A., Kumar, H., Gurjar, A. and Sharma, N.,, 2023) |
|
5. |
Selegiline |
80% |
6-12 mg |
24hr |
Acrylic adhesive |
Matrix |
(Lee, K.C. and Chen, J.J.,, 2007) |
|
6. |
Clonidine |
60-70% |
0.1-0.3 mg |
7days |
EVA adhesive |
reservoir |
(Ke, G.M., Wang, L., Xue, H.Y., Lu, W.L., Zhang, X., Zhang, Q. and Guo, H.Y.,, 2005) |
|
7. |
Rivastigmine |
50% |
4.6-9.5 mg |
24hr |
Acrylic adhesive |
Matrix |
(Kurz, A., Farlow, M. and Lefevre, G., 2009) |
|
8. |
Testosterone |
30% |
2.5-5 mg |
24hr |
Hydrony propyl cellulose |
Matrix |
(Hadgraft, J. and Lane, M.E.,, 2015) |
|
9. |
Heparin |
Investigational |
Investigational |
- |
adhesive |
matrix |
(Bhuvaneshwaran, A.,, 2019) |
|
10. |
Rotigotine |
45% |
2-8 mg |
24hr |
Silicon adhesive |
Matrix |
(Sanford, M. and Scott, L.J.,, 2011) |
|
11. |
Nitroglycerine |
|
0.2-0.8mg |
24hr |
EVA adhesive plasticizer |
Reservoir matrix |
(Mathews, L. and Roy, A., , 2016) |
|
12. |
Diclofenac |
Low systemic local high level |
1.3% patch |
12-24hr |
Gel adhesive matrix |
Matrix topical |
(Mathews, L. and Roy, A., , 2016) |
|
13. |
Ketoprofen |
Low systemic |
100mg |
12-24hr |
Adhesive matrix permeation enhancer |
Matrix topical |
(Monica, R., Vijay, S., Sayali, K., Mayuri, M., Abhishek, Z. and Pooja, K.,, 2019) |
|
14. |
Granisetron |
Transdermal provide continuous plasma |
3.1mg |
Upto 7days |
Acrylic adhesive backing |
Matrix |
(Li, J., Hu, P., Zhou, L., Nagahama, F. and Chen, R.,, 2023) |
|
15. |
Sumatriptan |
Investigational |
6mg |
Investigational(hr) |
Adhesive |
Matrix |
(Vikelis, M., Spingos, K.C. and Rapoport, A.M., , 2015) |
|
16. |
Ketamine |
Investigational |
Experimental |
Investigational(hr) |
Adhesive permeation enhancer |
Matrix |
(Kubota, R., Maruyama, Y., Wada, Y., Okamoto, A., Tsukamoto, A. and Komiyama, T.,, 2018) |
|
17. |
Ropinirole HCl |
30-50% |
- |
12hr |
HPMC, eudragit RL 100 |
Solvent casting |
(Bhosale, N.R., Hardikar, S.R. and Bhosale, A.V.,, 2011) |
|
18. |
Carvedilol |
Investigational |
Experimental |
Investigational |
Adhesive enhancer |
Matrix |
(Mo, L., Lu, G., Ou, X. and Ouyang, D., 2022) |
|
19. |
Stavudine |
86% |
40mg |
- |
Eudragit RS100, Eudragit RL 100 |
- |
(Kumar, S.S., Behury, B. and Sachinkumar, P.,, 2013) |
|
20. |
Piroxicam |
Low systemic topical |
Product dependent |
24hr |
Adhesive matrix, permeation enhancer |
Matrix |
(Agrahari, S., Sharma, A., Kumar, S., Sharma, A. and Sagar, M.K., , 2019) |
|
21. |
Capsaicin |
Negligible systemic |
179mg |
Applied |
30-60min |
Matrix |
(Baranidharan, G., Das, S. and Bhaskar, A., , 2013) |
|
22. |
Donepezil |
Investigational |
Experimental |
24-72hr |
Adhesive enhancer |
Matrix |
(R Madan, J., S Argade, N. and Dua, K.,, 2015) |
|
23. |
Scopolamin |
Sufficient for effect |
1.5mg |
72hr |
Acrylic adhesive backing |
Matrix |
(Antor, M.A., Uribe, A.A., Erminy-Falcon, N., Werner, J.G., Candiotti, K.A., Pergolizzi, J.V. and Bergese, S.D., 2014) |
|
24. |
Galantamine |
Investigational |
Experimental |
Investigational |
Adhesive enhancer |
Matrix |
(Ameen, D. and Michniak-Kohn, B.,, 2019) |
|
25. |
Zolmitriptan |
Investigational |
Experimental |
Investigational |
Adhesive enhancer |
Matrix |
(Liu, C. and Fang, L.,, 2015) |
|
26. |
Methylphenidate |
Moderate systemic |
10-40mg |
12hr |
Acrylic adhesive polyester film |
Matrix |
(Anderson, V.R. and Scott, L.J.,, 2006) |
|
27. |
Bupivacaine |
Minimal systemic |
Product dependent |
3days |
Adhesive |
Matrix |
(Mathews, L. and Roy, A., , 2016) |
|
28. |
Ropivacaine |
Local systemic |
Product dependent |
|
Adhesive |
Matrix |
(Yu, T., Zhang, S., Cao, X. and Liu, C, 2019) |
|
29. |
Timolol |
Investigational |
Investigational |
|
Adhesive |
Matrix |
(El-Laithy, H.M., 2009) |
|
30. |
Aector |
Low systemic |
180mg |
|
Acrylic adhesive |
Matrix |
(Rhee, Y.S., Nguyen, T., Park, E.S. and Chi, S.C.,, 2013) |
|
31. |
Levodopa |
Investigational |
Investigational |
24hr |
Adhesive |
Matrix |
(Lee, K.E., Choi, Y.J., Oh, B.R., Chun, I.K. and Gwak, H.S.,, 2013) |
|
32. |
Zolpidem |
Investigational |
Investigational |
|
Adhesive |
Matrix |
(Rani, T.N.,, 2017) |
|
33. |
Cariestatic fluoride |
Minimal systemic |
Product dependent |
|
Adhesive |
Matrix |
(Pacheco-Quito, E.M., Avila-Cunalata, D. and Cuenca-León, K.,, 2025) |
|
34. |
Fluconazole |
Investigational |
Investigational |
|
Adhesive |
Matrix |
(Patel, M.R., Patel, R.B., Parikh, J.R., Solanki, A.B. and Patel, B.G.,, 2009) |
|
35. |
Acyclovir |
Investigational |
Investigational |
|
Adhesive |
Matrix |
(Chandravanshi, S.L., Kaur, C.D., Verma, A., Khute, S., Baghel, T., Prasad, J., Mishra, S.P. and Sahu, B.,, n.d.) |
|
36. |
Losartan |
33% |
30mg |
2hr |
Polymer,ethyl cellulose, PVP |
Solvent casting |
(Nautiyal, U. and Singh, D.,, 2013) |
|
37. |
Anti-obesity drug |
Investigational |
Investigational |
|
Adhesive |
Matrix |
(Sánchez-Trasviña, C., Coronel-Meneses, D., Escobar-Fernández, A.M. and Mayolo-Deloisa, K.,, 2024) |
|
38. |
Antisecretory drug |
Investigational |
Investigational |
|
Adhesive |
Matrix |
(Borghi, S.M., Zaninelli, T.H., Carra, J.B., Heintz, O.K., Baracat, M.M., Georgetti, S.R., Vicentini, F.T., Verri, W.A. and Casagrande, R.,, 2022) |
|
39. |
Metoclopromide |
32-100% |
0.1-0.15mg |
4hr |
Eudragit L100 PVPK-30 |
Solvent casting |
(Eraga, S.O., Arhewoh, M.I. and Meko, O.A.,, 2020) |
|
40. |
Ondansetron hcl |
60% |
|
12hr |
Eudragit L-100 |
Solvent casting |
(David, S.R.N., Rajabalaya, R. and Zhia, E.S.,, 2015) |
Difficulties and Future Outlooks
TDD is a non-cut way to give meds. It is seen as easy to use, even for kids & old folk. It dodges some drug take-in woes that pop up with pill form. This is due to fears of soak-in & break-down. The skin's big open space & ease of reach make it a top & nice spot for med give-out. The skip of first-go break-down, steady give, better stick-to by the sick, low whole body drug mix-ups, long med flow, & top drug help are all key pros of skin med give.
Despite the excessive growth, a substantial number of difficult blocks remain that restrict the use of TDD to a handful of drugs. It has only gone to the market with a few drugs that employ chem TDD tricks. Things like niosomes & nanocrystals are not the final drug forms & must change to a right drug form (e.g., patches, creams, gels) before use. The add of helpers, needed for all drug forms, bumps the cost & complex of the make method but also adds many fail points. Such as the need to fix the size of the bits & the risk of drug leaks. These must be well watched to keep the drug form's power high. Plus, chem tricks have a big limit on the move of water-love big bits like insulin & many proteins. Moving past old ways of drug test, new ways now work to put drugs through the skin. Most of these new ways are still in test phases & work to give out many drugs, like water-love drugs & big drugs. More than 1000 drug tests, which examine skin drug ways, now are listed at the U.S. National Library of Medicine (NLM; clinicaltrials.gov). It enumerates the top 10 drug tests on skin ways as per NLM. (Zaid Alkilani, A., Hamed, R., Musleh, B. and Sharaire, Z.,, 2024).
CONCLUSION
In short, when we check how well & safe both picks are, 2% mepivacaine with stuff that tightens blood flow beats 2% lidocaine with epinephrine in teeth fix jobs. Yet, 3% plain mepivacaine works better to kill pain in folks. Still, we need more tests to be sure. TDDS is a fresh way to dose forms for many drugs taken by shot or mouth that fit well in terms of their make-up & drug traits. The TDD makes sure the drug hits the right live spot with less bad sides. As TDDS has a lot of good points, a lot of work is now done to put more drugs in the mix. Tools aimed at better soak & soak-in rates of the drug are now checked. TDDSs lean much on things like toppers, soak aids, back layers, soft makers, & lines to make sure of good stick & timed drug flow to the blood from skin for hours or days. Skin patches split into groups, like pool system, grid system, & tiny pool system. After making skin patches, set ways are used to test the parts. With new tech & the skill to send drugs to the target spot sans skin break, the skin way is now a top pick for drug send. This drug send way solves the hang-ups seen in much-used drug send ways, showing a bright view ahead. Based on how long the fix lasts, drugs are in the market as skin patches.
REFERENCES


Sakshi Kautkar, Chetan Bhange, Harsha Sonaye, Dimak Chand Sahu, Novel Transdermal Delivery System for Local Anaesthesia: Focus on Mepivacaine Hydrochloride, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 4338-4357. https://doi.org/10.5281/zenodo.18790962
 10.5281/zenodo.18790962
10.5281/zenodo.18790962
