1-3Student , Department of Pharmacology, Devaki Amma Memorial College of Pharmacy, Chelembra
4Professor and Head, Department of Pharmacology ,Devaki Amma Memorial College of Pharmacy, Chelembra
5Principal, Devaki Amma Memorial College of Pharmacy, Chelembra
Salmonella and E. coli are two of the bacteria that can cause urinary tract infections. Women are more likely to get UTIs, which typically affect the urethra and bladder. Commonly, the gastrointestinal (GI) tract contains E. coli. This rod-shaped, Gram-negative bacterium belongs to the Enterobacteriaceae family and can survive in both an airborne and an atmosphere-filled environment. Different forms of urinary tract infections include complicated, uncomplicated, recurrent urosepsis, bladder infection (cystitis), kidney infection (pyelonephritis), and vaginal infection (vaginal infection). Anemia is a disorder when there are insufficient amounts of healthy red blood cells in the blood. The body's RBCs are either absent or malfunctioning in anemia. A 60-year-old female patient was admitted to the hospital after suffering a low-grade fever that persisted for five days along with chills and rigidity. In addition, the patients have burning micturition, a history of low back pain, arthralgia for the previous six years, a 20-day reduced food intake, and seven years of steroid use (tablet dexamethasone 0.5mg). After evaluating the patients, the doctor started to give IV fluids, antibiotics, antiemetics, antiulcer agents, antihypertensive medications, vitamins, and analgesics. For this patient, the steroid withdrawal process is now complete.
Males and women can both contract urinary tract infections, but because of differences in physiology, women are more likely to contract them than males. Put simply, it can be described as a condition that women will undoubtedly experience at some point in their lives, with a higher prevalence among pregnant women [1]. In general practice, it is one of the most prevalent diseases and one of the most common bacterial infections in women. In their lives, more than 50% of women will experience at least one episode of an uncomplicated UTI, and 20–30% will experience repeated episodes. 10 percent or so of post-menopause women say they experienced a UTI in the previous 12 months. This frequency is highest (17.5%) in the 18–24 age group, although it remains significantly higher (9% in women 50 years of age and older). According to research studies, the most prevalent type of bacterial illness is a urinary tract infection. While conditions like high fever and flank pain are frequently experienced in cases of kidney contagion, also known as pyelonephritis, the symptoms of kidney contagion include dysuria, burning pain, urgency, frequency, and low volume of urine, as well as pain in the lower abdomen, low back pain, and a change in urine smell. Typically, the definitions listed below are applied: Simple UTIs are periods of cystitis in women without impaired immune systems, no morphological or functional abnormalities of the urogenital tract, and no signs of tissue invasion or systemic infection. Any UTI that is not simple is considered difficult [2]. Another technique to diagnose UTIs is to compare the differences between UTIs obtained in the community and hospital. Complicated UTIs are typically those that are acquired within a hospital or those that are treated there. Escherichia coli, sometimes known as E. coli, is not the only uropathogen that causes problems. Moreover, bacteria that exhibit greater resistance are grown in comparison to community-acquired UTIs. The best way to determine whether resistant-causing germs are present is to treat them with antibiotics early on [3]. Patients with healthcare-associated (as compared to hospital-associated) UTIs were older, more co-morbid, and had received antibiotic treatment more frequently in the past than patients with community-acquired UTIs. Extended-spectrum beta-lactamase (ESBL)-positive pseudomonas aeruginosa and E. coli infections were also more frequently cultured. Consequently, residents of assisted living facilities may have UTIs that originated in a hospital [4]. Asymptomatic bacteriuria (ASB), which is mainly found in women, is a common but usually normal condition defined as the presence of a positive urine culture acquired from a patient who does not exhibit UTI symptoms, with at least 105 cfu/ml [5]. Both host- and bacterium-related factors influence the possibility that ASB will resolve on its own or progress into a symptomatic UTI. In a Swedish study involving 116 patients with ASB, only 30% had a medical history consistent with a prior UTI [6]. Of the girls, 10.3% showed a baseline renal parenchymal reduction, whereas 20.7% had reflux. The cause of E.coli bacteriuria is yet unknown, although it may increase the risk of hypertension in the future [7].
CASE REPORT
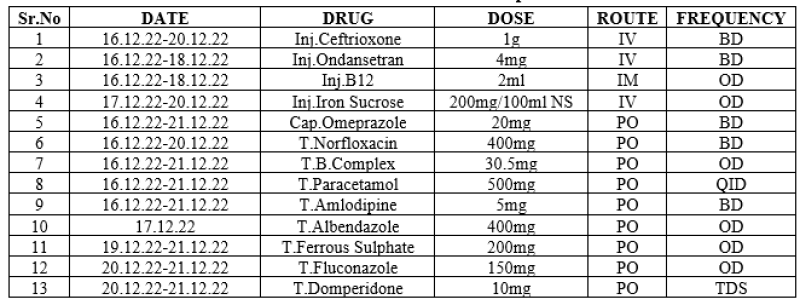
A 60-year-old female patient was taken to the Virudhunagar Medical College and Hospital due to burning micturition and a history of low-grade fever that had been persistent for the previous 5 days, along with chills, rigors, decreased food intake, mild backache, and arthralgia. They gave us an ethical certificate for performing this study, with reference number R. No. 110/HS/GHQH-VNR/SEP 2019. The patient does not have a history of bleeding symptoms, oliguria, facial puffiness, vomiting, loose stool, CVA, CAD, or seizures. For the previous seven years, the patient had been taking steroid tablets, such as dexamethasone, by mistake. She believed the tablet to be a sign of elevated blood pressure. The patient was dehydrated, but the systemic examination and vitals were normal. The patient has been diagnosed with hypertension and a urinary tract infection. Hemoglobin, packed cell volume, and red blood cell counts are low in the patient. They came to the conclusion that the patient had anemia. The patient was advised to take the prescription listed in Table 2.
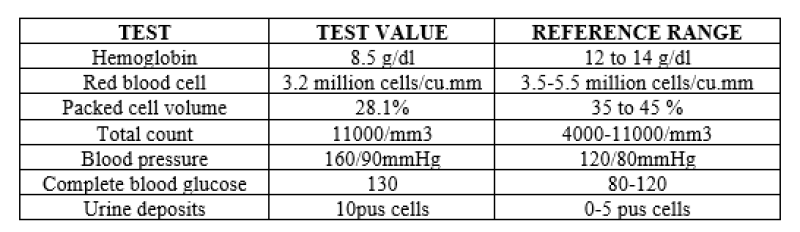
Table 1: Clinical laboratory investigation report.
Table 2: A chart of treatments with the specified date
DISCUSSION:
Urinary Tract Infection (UTI) is a common bacterial infection characterized by inflammation of the urinary tract, typically caused by pathogenic bacteria such as Escherichia coli (E. coli), Klebsiella, or Proteus species. In the case of the 60-year-old female patient admitted to Virudhunagar Medical College and Hospital, presenting with burning micturition, fever, and other systemic symptoms, the diagnosis of UTI is supported by clinical findings and laboratory investigations. The patient's symptoms, including burning micturition, are classic manifestations of lower urinary tract involvement, while the associated fever, chills, and rigors suggest systemic involvement and potential upper urinary tract infection. Given the patient's age and gender, postmenopausal changes, such as vaginal atrophy and decreased estrogen levels, may predispose her to UTIs by altering the urogenital flora and reducing the protective effects of the vaginal epithelium [8]. The treatment approach for UTI typically involves empirical antibiotic therapy targeting the most common uropathogens, such as E. coli. In this case, the patient received a combination of intravenous Ceftriaxone and oral Norfloxacin, which are broad-spectrum antibiotics effective against many urinary pathogens. Additionally, supportive measures, such as adequate hydration and symptomatic relief with antiemetics and analgesics, play a crucial role in managing UTI-associated symptoms and promoting recovery. Preventive strategies for UTIs in older adults, particularly postmenopausal women, may include promoting good genitourinary hygiene, encouraging regular voiding, and considering the use of vaginal estrogen therapy to restore the vaginal epithelial barrier and reduce the risk of recurrent infections [9]. Patient education regarding the importance of completing antibiotic courses as prescribed, avoiding unnecessary antibiotic use, and recognizing symptoms of UTI recurrence is essential for long-term management and prevention. Furthermore, given the patient's history of chronic steroid use, which can suppress the immune response and increase susceptibility to infections, careful consideration of potential predisposing factors and comorbidities is warranted in the evaluation and management of UTI [10]. Close monitoring for treatment response, resolution of symptoms, and potential complications, such as urosepsis or pyelonephritis, is crucial, particularly in older adults who may present with atypical or more severe manifestations of UTI. In summary, UTI is a common and often recurrent condition, particularly in older adults, necessitating a comprehensive approach to diagnosis, management, and prevention [11]. Tailored treatment regimens, appropriate supportive care, and preventive strategies are essential components of UTI management in this patient population, with a focus on optimizing outcomes and reducing the risk of recurrence and complications [12].
CONCLUSION:
Bacterial infections cause most cases of UTIs. When patients exhibit anomalies related to function, metabolism, or structure, UTIs become complicated. E. coli (80%) and S. saprophyticus (5%–15%) have been and continue to be the most frequent causal pathogens linked to simple cystitis or acute pyelonephritis in the recent past. The treatment regimen implemented reflects a comprehensive approach targeting the underlying infections and addressing the anemia and hypertension. Antibiotic therapy with Ceftriaxone and Norfloxacin targets the urinary tract infection, while adjunctive medications such as Ondansetron alleviate symptoms of nausea and vomiting. Nutritional supplementation with Vitamin B12, Iron Sucrose, Ferrous Sulphate, and B.complex addresses the patient's anemia, aiming to restore hemoglobin levels and improve overall well-being. Antihypertensive therapy with Amlodipine aims to control blood pressure and mitigate cardiovascular risks associated with hypertension. The inclusion of other medications such as Omeprazole for gastrointestinal protection, Paracetamol for analgesia and antipyresis, and Fluconazole for potential fungal infection demonstrates a holistic approach to addressing the patient's diverse clinical needs. Moving forward, the patient will require close monitoring to assess treatment response, resolution of symptoms, and the need for further intervention or adjustment of management strategies. This case underscores the importance of a comprehensive and patient-centered approach to clinical care, integrating thorough assessment, targeted interventions, and ongoing monitoring to optimize outcomes and ensure patient well-being.
REFERENCE:


Vigneswaran R., Natarajan P., Thiruppathi M., Ganesh H., Kodishwaran R, A Case Report On Uti, Anemia, And Steroid Withdrawal In A Post-Menopausal Geriatric Patient, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 3, 958-962. https://doi.org/10.5281/zenodo.10869139
 10.5281/zenodo.10869139
10.5281/zenodo.10869139
