Oriental College of Pharmacy
Central nervous system (CNS) disorders represent a major global health burden and remain difficult to treat due to the restrictive nature of the blood–brain barrier (BBB), which prevents nearly all large molecules and approximately 98% of small molecules from entering the brain in therapeutic concentrations [1–4]. Conventional systemic delivery approaches often fail to achieve effective CNS drug levels while producing systemic side effects. Nose-to-brain (N2B) drug delivery has emerged as a promising, non-invasive alternative that bypasses the BBB by exploiting direct anatomical connections between the nasal cavity and the brain via olfactory and trigeminal pathways [5–7]. This review summarises the anatomical and physiological basis of N2B delivery, mechanisms of drug transport, factors influencing nasal absorption, advanced formulation strategies including nanocarriers and in situ systems, and current challenges affecting clinical translation
Neurological disorders are among the leading causes of disability-adjusted life years and mortality worldwide, with their prevalence continuing to rise due to aging populations and lifestyle factors [1]. Disorders such as Alzheimer’s disease, Parkinson’s disease, epilepsy, depression, and brain tumors impose a substantial clinical and socioeconomic burden [2].Despite advances in medicinal chemistry and molecular targeting, CNS drug development remains associated with high attrition rates and prolonged development timelines [3]. The primary reason for this failure is the BBB, a highly selective physiological barrier formed by endothelial cells connected through tight junctions, supported by astrocytic end-feet and pericytes [4]. The BBB exhibits low paracellular permeability, limited vesicular transport, and high expression of efflux transporters, thereby severely restricting drug entry into the brain [4,5]. As a result, nearly 98% of small molecules and almost all biologics fail to reach the CNS in therapeutic concentrations following systemic administration [2,3].
Fig.1.1. Formulation strategies employed for enhanced nose-to-brain drug delivery through the intranasal route

Nose-to-brain drug delivery has gained significant attention as an alternative strategy capable of bypassing the BBB via direct neuronal connections between the nasal cavity and the brain [5–7]. Evidence from preclinical and clinical studies demonstrates rapid brain uptake, reduced systemic exposure, and improved therapeutic outcomes following intranasal administration [8–10].
ANATOMICAL AND PHYSIOLOGICAL BASIS OF NOSE-TO-BRAIN DELIVERY
The human nasal cavity is divided into two symmetrical chambers by the nasal septum and is lined with nasal mucosa, excluding the vestibular region [11]. The nasal mucosa is functionally divided into the respiratory and olfactory regions.
The respiratory region constitutes the majority of the nasal cavity and is lined with ciliated pseudostratified epithelium. It is responsible for air humidification, filtration, and temperature regulation and is innervated by branches of the trigeminal nerve [11,12]. Due to its high vascularization, drugs deposited in this region are readily absorbed into systemic circulation.
Fig.2.1. Anatomy of the nasal cavity highlighting olfactory and trigeminal nerve pathways involved in nose-to-brain drug delivery
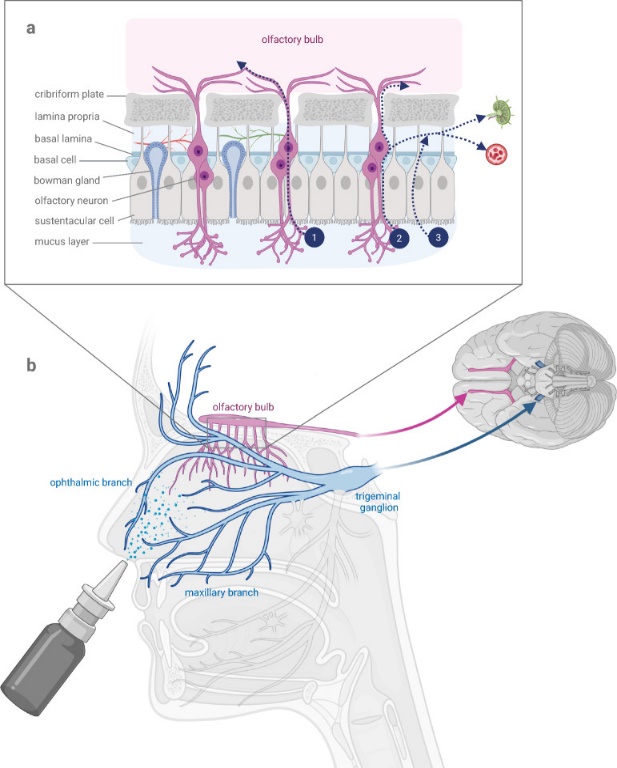
The olfactory region is located in the upper posterior part of the nasal cavity and is lined with specialized olfactory epithelium containing olfactory receptor neurons [11]. These neurons project directly into the olfactory bulb through the cribriform plate, creating a unique anatomical pathway between the nasal cavity and the CNS [11,13]. This direct connection forms the structural basis for nose-to-brain drug transport.
In humans, the olfactory epithelium accounts for less than 10% of the total nasal surface area, compared with 40–50% in rodents, which partly explains the reduced translational efficiency observed in clinical studies [11,14]. Additionally, mucociliary clearance, with an average transport rate of approximately 6 mm/min, rapidly removes particles and formulations from the nasal cavity, limiting drug residence time [15].
MECHANISMS OF NOSE-TO-BRAIN DRUG TRANSPORT
Nose-to-brain drug delivery exploits unique anatomical and physiological connections between the nasal cavity and the central nervous system (CNS) to bypass the restrictive blood–brain barrier (BBB). The primary mechanisms involve direct neuronal transport, extracellular diffusion, perivascular and perineural bulk flow, and auxiliary indirect routes through systemic circulation or lymphatics. These mechanisms are not mutually exclusive; rather, their relative contributions depend on drug properties, formulation characteristics, and site of nasal deposition [5,12,17,22].
1. Overview of Routes
The major routes through which intranasally administered drugs can reach the brain are:
These pathways collectively enable drugs to access multiple brain regions without crossing the BBB directly [1,5,12].
2. Olfactory Neuronal Pathways
2.1 Anatomical Basis
The olfactory region is located in the upper part of the nasal cavity and contains specialized olfactory sensory neurons (OSNs) whose axons traverse the cribriform plate to enter the olfactory bulb. This forms a direct anatomical conduit between the nasal cavity and the CNS [2,13].
2.2 Intracellular Axonal Transport
After intranasal administration, certain substances may be internalized by OSNs via receptor-mediated endocytosis or pinocytosis. Once inside the neuron, they are transported along microtubules via axonal transport mechanisms to the olfactory bulb and subsequently to other brain regions (e.g., cortex, hippocampus) through synaptic relays. This intracellular route, although direct, is typically slow and suited for drugs that can be actively transported within neurons [5,8,9].
2.3 Extracellular Routes Across Olfactory Epithelium
Evidence strongly supports extracellular transport as the dominant mechanism for rapid nose-to-brain delivery. In this case, drugs move through paracellular spaces between epithelial cells, or through perineural channels surrounding the olfactory nerve bundles, reaching the lamina propria. From there, they diffuse along perineural and perivascular routes into the subarachnoid space and cerebrospinal fluid (CSF), often observed within minutes of administration [1,12,13].
Importantly, extracellular transport does not rely on active neuronal processes and is facilitated by bulk flow movements within the perineural and lymphatic compartments [1].
Fig.3.1. Mechanisms of nose-to-brain drug transport via olfactory and trigeminal pathways following intranasal administration

2.3 Cerebrospinal Fluid–Mediated Transport
Several studies have reported rapid detection of intranasally administered drugs in the cerebrospinal fluid, indicating a nose-to-CSF pathway [11,16]. Drugs reaching the subarachnoid space via olfactory or trigeminal routes may distribute throughout the brain via CSF circulation, allowing widespread CNS exposure.
This mechanism is particularly relevant for small molecules and peptides that exhibit high CSF permeability and stability [11].
2.4 Role of Nanocarriers in Mechanistic Transport
Nanocarrier-based systems significantly influence nose-to-brain transport mechanisms by protecting drugs from enzymatic degradation, enhancing mucosal penetration, and modulating interaction with neuronal pathways [17,18].
Polymeric nanoparticles and lipid-based carriers may undergo direct transport along trigeminal pathways while releasing the encapsulated drug during transit or upon reaching the brain [17]. Surface-modified nanoparticles, especially those exhibiting mucoadhesive or charge-mediated interactions, enhance retention in the olfactory region and increase the probability of extracellular diffusion into neural pathways [17].
Micelles and lipid nanoparticles have demonstrated improved brain bioavailability by facilitating both extracellular diffusion and sustained drug release within the nasal cavity [15-17].
2.5 Systemic Absorption and Indirect Brain Entry
In addition to direct neuronal transport, a portion of the intranasally administered dose is absorbed into systemic circulation via the respiratory epithelium [11]. While this fraction does not contribute to direct nose-to-brain targeting, it may reach the brain through conventional BBB transport mechanisms. However, this route is associated with delayed onset and potential systemic side effects and is considered secondary to direct pathways [5,6].
2.6 Comparative Contribution of Transport Pathways
Overall, rapid brain targeting following intranasal administration is primarily attributed to extracellular transport via olfactory and trigeminal pathways, while intracellular axonal transport and systemic absorption play supporting roles [6,16]. The relative contribution of each pathway depends on drug properties, formulation type, particle size, and nasal deposition site [10,15].
3. Trigeminal Nerve Pathway
The trigeminal nerve provides sensory innervation to both the respiratory and olfactory regions of the nasal cavity and represents an additional direct route for nose-to-brain transport [6,12]. Its ophthalmic and maxillary branches project to the brainstem, pons, and spinal cord, enabling drug delivery to regions beyond the olfactory bulb.
Following intranasal administration, drugs deposited in the respiratory epithelium may enter trigeminal nerve endings and be transported to trigeminal nuclei within the brainstem [6]. Compared to the olfactory pathway, trigeminal transport contributes more significantly to drug distribution in posterior brain regions and the spinal cord [12,16].
Both extracellular diffusion along trigeminal nerve fibers and limited intracellular axonal transport have been proposed, with extracellular mechanisms again dominating due to faster kinetics [6].
3.1 Anatomical Basis
The trigeminal nerve (cranial nerve V) innervates the respiratory and olfactory regions of the nasal cavity via its ophthalmic and maxillary branches. These branches carry sensory fibers that project into the brainstem at the level of the pons [5,12,13].
3.2 Trigeminal Transport Mechanisms
Drugs deposited on the respiratory mucosa or within the olfactory region can be taken up by trigeminal nerve endings. Transport can occur via:
Compared with the olfactory pathway, the trigeminal route connects to different CNS regions, including brainstem nuclei and spinal cord, and may contribute to broader brain distribution [1,12].
4. Perineural and Perivascular Bulk Flow
4.1 Perineural Channels
Once substances cross the olfactory epithelium into the lamina propria, they may enter perineural channels — fluid-filled conduits that surround nerve bundles. These channels provide a low-resistance path for drugs to reach the subarachnoid space and mix with CSF, enabling distribution to wide brain areas [1,6].
4.2 Perivascular Routes
Drug molecules can also spread along perivascular spaces around cerebral blood vessels. Convection within these spaces, driven by arterial pulsations, facilitates rapid central distribution beyond the initial site of entry, contributing significantly to the brain distribution of small tracers after intranasal dosing [11]. This perivascular bulk flow is particularly important for achieving more homogeneous CNS exposure than axonal transport alone.
5. Systemic Absorption and Secondary Brain Entry
The highly vascularized nasal respiratory epithelium allows a portion of the administered dose to be absorbed into systemic circulation. Although this does not constitute direct nose-to-brain delivery, once in the bloodstream, drugs may still reach the brain by crossing the BBB via conventional mechanisms (e.g., passive diffusion, carrier-mediated transport) [1,10]. However, this systemic route is slower and less targeted than direct neuronal pathways.
6. Lymphatic Pathways and CSF Exchange
Emerging evidence indicates that the nasal lymphatic system contributes to drug movement into the CNS. Substances reaching lymphatic vessels in the nasal mucosa may travel to the deep cervical lymph nodes and eventually enter the CSF, providing an alternative indirect route that can supplement direct neuronal mechanisms [17].
7. Time Course and Relative Contribution
Experimental studies in animals and humans consistently show that detectable levels of intranasal drugs appear in the olfactory bulb or CSF within minutes, supporting the dominance of extracellular transport over slower intracellular axonal routes [1,12]. Intracellular transport can require hours to days, making it less significant for rapid therapeutic effects, though it may contribute to long-term distribution [5,8].
8. Factors Influencing Mechanistic Pathways
The relative importance of these mechanisms depends on:
For instance, small, lipophilic molecules are more likely to cross mucosa rapidly and enter extracellular pathways, whereas macromolecules and particulates may require carrier systems or enhanced permeation strategies to access neuronal routes effectively [1,22].
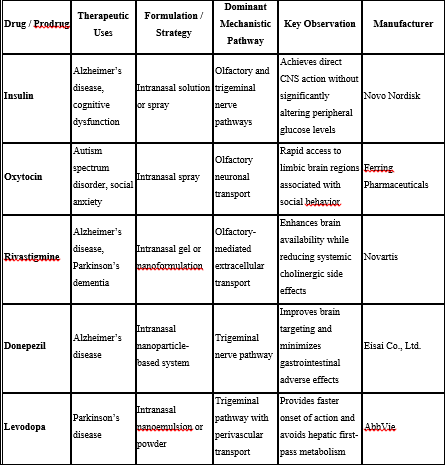
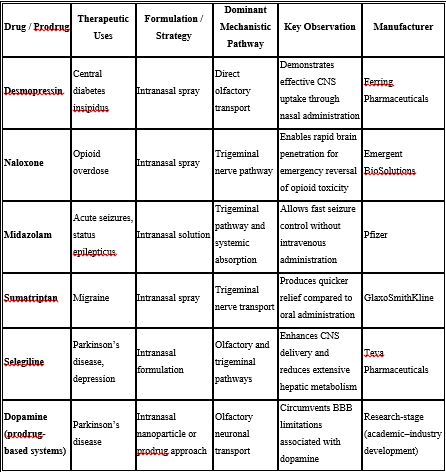
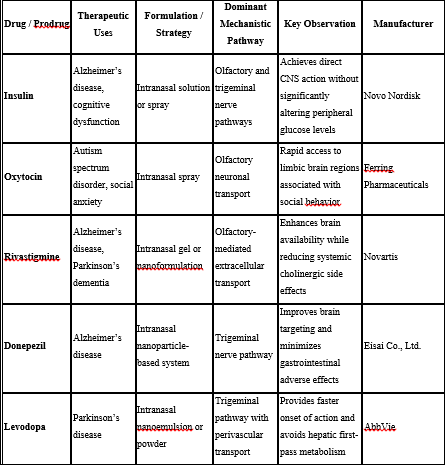
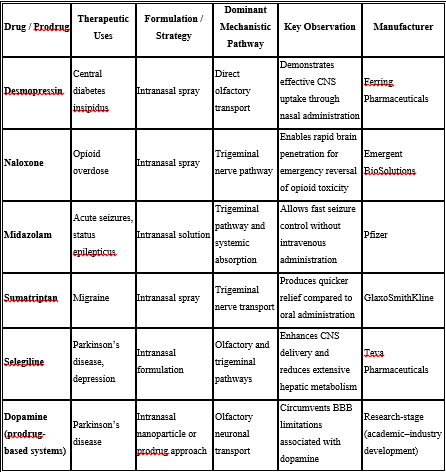
EXAMPLES OF DRUGS INVESTIGATED FOR NOSE-TO-BRAIN DELIVERY
ADVANTAGES AND LIMITATIONS OF NOSE-TO-BRAIN DELIVERY
A key advantage of nose-to-brain delivery is its ability to bypass the BBB while minimizing systemic exposure and peripheral side effects [5,9]. Clinical studies involving intranasal insulin have demonstrated improved attention, memory, and cognitive performance in patients with Alzheimer’s disease without significant increases in plasma insulin levels [10,18].
However, several limitations hinder the widespread clinical application of this approach. These include limited dosing volume (25–200 μL per nostril), low olfactory surface area in humans, variability in nasal anatomy, rapid mucociliary clearance, and substantial loss of drug to systemic circulation through the respiratory epithelium [11,14,19].
FACTORS AFFECTING NOSE-TO-BRAIN DRUG DELIVERY
The effectiveness of nose-to-brain drug delivery depends on a complex interaction between physicochemical properties of the drug, formulation-related variables, and physiological characteristics of the nasal cavity. These factors collectively influence nasal deposition, residence time, epithelial permeation, neuronal transport, and ultimately drug concentration achieved in the brain [12]. Inadequate consideration of any one of these parameters can significantly compromise therapeutic outcomes.
5.1 Drug-Related Factors
5.1.1 Molecular Weight and Molecular Size
Low molecular weight drugs (<400 Da) preferentially traverse nasal epithelial barriers through paracellular or transcellular diffusion, enabling rapid access to extracellular perineural pathways and cerebrospinal fluid [1,2]. In contrast, macromolecules such as peptides and proteins are sterically restricted and rely more heavily on intracellular neuronal uptake or carrier-mediated systems to access the CNS [3].
Mechanistic impact:
5.1.2 Lipophilicity
Moderately lipophilic drugs exhibit enhanced epithelial membrane permeation and are more likely to enter extracellular diffusion routes rapidly [2]. Excessively lipophilic compounds, however, may become trapped within epithelial membranes or display poor solubility, limiting effective transport.
Mechanistic impact:
5.1.3 Aqueous Solubility and Dissolution Rate
Sufficient solubility in nasal fluids is essential for maintaining drug availability at the absorption site. Poorly soluble drugs may precipitate within the nasal cavity, resulting in erratic absorption and rapid clearance. Formulation approaches such as nanosystems and lipid carriers are often required to address this limitation [12].
5.1.4 Chemical Form of the Drug and Prodrug Strategy
The chemical form of a drug (salt, ester, free base) significantly affects nasal absorption and pathway selection. Prodrug approaches have been used to enhance lipophilicity or enzymatic stability, thereby improving penetration into neuronal pathways before conversion to the active drug within the brain [4].
Mechanistic impact:
5.1.5 Polymorphism
Polymorphic forms of a drug may differ in solubility, dissolution rate, and stability, which in turn affect nasal absorption and bioavailability [12]. Selection of an appropriate polymorphic form is therefore critical during formulation development.
5.1.6 Biopharmaceutic Properties
Biopharmaceutic characteristics such as permeability, metabolism, and clearance play a crucial role in determining the extent of nose-to-brain transport. Drugs with high permeability but rapid systemic clearance may still achieve effective brain targeting when delivered intranasally due to direct neuronal transport pathways [12].
5.1.7 Stability Against Nasal Enzymes
Drugs susceptible to nasal enzymatic degradation may fail to reach neuronal pathways intact. Encapsulation or chemical modification becomes essential to preserve the drug long enough for transport via perineural or intracellular routes [3].
5.2 Formulation-Related Factors
5.2.1 Dosage Form and Release Profile
Solutions are rapidly cleared from the nasal cavity, favoring systemic absorption over direct brain targeting. In contrast, gels, powders, and mucoadhesive systems prolong residence time in the olfactory region, enhancing neuronal transport [2,5].
Mechanistic impact:
5.2.2 Nanocarrier Systems
Nanoparticles, liposomes, micelles, and lipid carriers protect drugs from degradation and facilitate interaction with neuronal membranes. Particle size and surface charge critically influence whether nanocarriers undergo extracellular diffusion or are internalized by neurons [6,7].
Mechanistic impact:
5.2.3 Surface Modification
Surface functionalization with mucoadhesive polymers or targeting ligands increases retention in the olfactory region and promotes neuronal uptake, biasing transport toward olfactory and trigeminal routes [6].
5.2.4 Drug Concentration
Drug concentration directly affects the concentration gradient across the nasal epithelium and thus influences absorption. However, increasing drug concentration is limited by nasal irritation, solubility constraints, and dose volume restrictions [12].
5.2.5 pH and Buffer Capacity
The pH of nasal formulations should ideally lie between 4.5 and 6.5 to minimize mucosal irritation and maintain ciliary function [11]. Excessive buffer capacity may disrupt the physiological nasal environment and impair mucociliary clearance.
5.2.6 Osmolarity
Isotonic or slightly hypotonic formulations are preferred for nasal administration. Hypertonic formulations can cause epithelial dehydration, discomfort, and increased mucociliary clearance, reducing drug residence time [11].
5.2.7 Viscosity
Formulation viscosity influences nasal retention and clearance. Moderate increases in viscosity can prolong residence time and enhance absorption, whereas excessive viscosity may interfere with ciliary movement and reduce drug diffusion [11].
5.2.8 Preservatives
Preservatives are commonly added to multidose nasal formulations to prevent microbial growth. However, certain preservatives may cause mucosal irritation or ciliotoxicity, necessitating careful selection and concentration optimization [11].
5.2.9 Antioxidants
Antioxidants are incorporated to prevent oxidative degradation of susceptible drugs during storage and administration. Their compatibility with nasal tissues and formulation components must be carefully evaluated [11].
5.2.10 Humectants
Humectants help maintain moisture within the nasal cavity and prevent mucosal drying, thereby improving patient comfort and formulation tolerability [11].
5.3 Physiological and Pathological Factors
5.3.1 Effect of Deposition Site on Absorption
The site of drug deposition within the nasal cavity critically influences absorption and brain targeting. Deposition in the olfactory region favors direct nose-to-brain transport, whereas deposition in the respiratory region leads predominantly to systemic absorption [11,14]. Improper deposition significantly reduces targeting efficiency.
Mechanistic impact:
5.3.2 Mucociliary Clearance
Mucociliary clearance rapidly removes administered formulations from the nasal cavity, limiting the time available for drug absorption. Clearance typically occurs within 15–30 minutes and represents a major physiological barrier to effective nasal delivery [12].
5.3.3 Nasal Blood Flow
High blood flow in the respiratory epithelium promotes systemic uptake, which may reduce the fraction of drug available for direct neuronal transport to the brain [11].
5.3.4 Enzymatic Activity
Metabolic enzymes present in nasal mucosa can degrade drugs prior to absorption, particularly peptides and proteins, thereby reducing bioavailability [12].
5.3.5 Effect of Pathological Conditions
Pathological conditions such as rhinitis, sinusitis, nasal polyps, and infections alter mucus composition, epithelial permeability, and clearance rates, leading to significant variability in drug absorption and therapeutic response [12].
5.3.6 Time-Dependent Transport Dynamics
Extracellular pathways enable drug detection in the brain within minutes, whereas intracellular axonal transport requires hours to days. Thus, drugs intended for rapid onset of action rely predominantly on extracellular diffusion rather than neuronal axonal transport [1,4].
FORMULATION STRATEGIES FOR ENHANCED NOSE-TO-BRAIN DRUG DELIVERY
To overcome anatomical, physiological, and biochemical barriers associated with intranasal administration, advanced formulation strategies have been developed to enhance drug retention, stability, absorption, and neuronal transport to the brain [14,15].
6.1 Conventional Nasal Dosage Forms
Conventional nasal solutions, suspensions, and powders are simple to formulate but suffer from rapid clearance and limited targeting efficiency. Their use is generally restricted to drugs with favorable physicochemical properties [16].
6.2 Mucoadhesive Drug Delivery Systems
Mucoadhesive systems utilize polymers such as chitosan, carbopol, and cellulose derivatives to increase adhesion to nasal mucosa, thereby prolonging residence time and enhancing absorption [14]. Chitosan additionally enhances paracellular transport by transiently opening tight junctions while maintaining an acceptable safety profile [14,15].
6.3 In Situ Gelling Systems
In situ gelling systems undergo sol-to-gel transition upon exposure to physiological conditions, resulting in increased viscosity at the administration site. This property reduces clearance and allows sustained drug release, leading to improved brain bioavailability [14].
6.4 Nanocarrier-Based Drug Delivery Systems
Nanocarriers play a central role in modern nose-to-brain delivery by improving solubility, stability, controlled release, and interaction with neuronal pathways [15,16].
6.4.1 Polymeric Nanoparticles
Polymeric nanoparticles protect drugs from enzymatic degradation and enable controlled release, facilitating transport along olfactory and trigeminal pathways [15].
6.4.2 Lipid-Based Nanocarriers
Lipid-based carriers such as liposomes, solid lipid nanoparticles, and nanostructured lipid carriers enhance mucosal interaction and neuronal uptake due to their lipidic composition [16].
6.4.3 Polymeric Micelles
Micelles improve the delivery of poorly water-soluble drugs and have demonstrated significantly enhanced brain exposure following intranasal administration [15,16].
6.4.4 Surface-Modified Nanocarriers
Surface modification with mucoadhesive polymers or charge-based ligands enhances retention in the olfactory region and increases the probability of neuronal transport to the brain [16].
REFERENCES
Neurological disorders are among the leading causes of disability-adjusted life years and mortality worldwide, with their prevalence continuing to rise due to aging populations and lifestyle factors [1]. Disorders such as Alzheimer’s disease, Parkinson’s disease, epilepsy, depression, and brain tumors impose a substantial clinical and socioeconomic burden [2].Despite advances in medicinal chemistry and molecular targeting, CNS drug development remains associated with high attrition rates and prolonged development timelines [3]. The primary reason for this failure is the BBB, a highly selective physiological barrier formed by endothelial cells connected through tight junctions, supported by astrocytic end-feet and pericytes [4]. The BBB exhibits low paracellular permeability, limited vesicular transport, and high expression of efflux transporters, thereby severely restricting drug entry into the brain [4,5]. As a result, nearly 98% of small molecules and almost all biologics fail to reach the CNS in therapeutic concentrations following systemic administration [2,3].
Fig.1.1. Formulation strategies employed for enhanced nose-to-brain drug delivery through the intranasal route
Nose-to-brain drug delivery has gained significant attention as an alternative strategy capable of bypassing the BBB via direct neuronal connections between the nasal cavity and the brain [5–7]. Evidence from preclinical and clinical studies demonstrates rapid brain uptake, reduced systemic exposure, and improved therapeutic outcomes following intranasal administration [8–10].
ANATOMICAL AND PHYSIOLOGICAL BASIS OF NOSE-TO-BRAIN DELIVERY
The human nasal cavity is divided into two symmetrical chambers by the nasal septum and is lined with nasal mucosa, excluding the vestibular region [11]. The nasal mucosa is functionally divided into the respiratory and olfactory regions.
The respiratory region constitutes the majority of the nasal cavity and is lined with ciliated pseudostratified epithelium. It is responsible for air humidification, filtration, and temperature regulation and is innervated by branches of the trigeminal nerve [11,12]. Due to its high vascularization, drugs deposited in this region are readily absorbed into systemic circulation.
Fig.2.1. Anatomy of the nasal cavity highlighting olfactory and trigeminal nerve pathways involved in nose-to-brain drug delivery
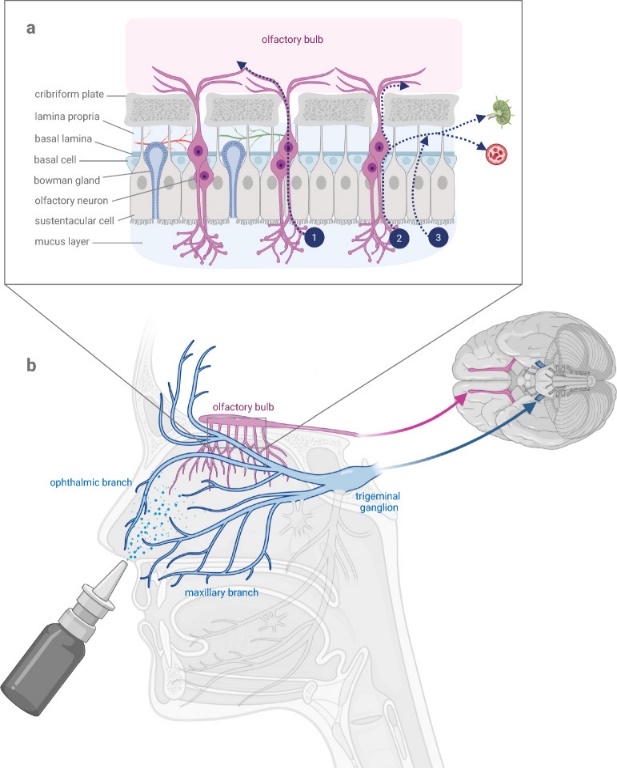
The olfactory region is located in the upper posterior part of the nasal cavity and is lined with specialized olfactory epithelium containing olfactory receptor neurons [11]. These neurons project directly into the olfactory bulb through the cribriform plate, creating a unique anatomical pathway between the nasal cavity and the CNS [11,13]. This direct connection forms the structural basis for nose-to-brain drug transport.
In humans, the olfactory epithelium accounts for less than 10% of the total nasal surface area, compared with 40–50% in rodents, which partly explains the reduced translational efficiency observed in clinical studies [11,14]. Additionally, mucociliary clearance, with an average transport rate of approximately 6 mm/min, rapidly removes particles and formulations from the nasal cavity, limiting drug residence time [15].
MECHANISMS OF NOSE-TO-BRAIN DRUG TRANSPORT
Nose-to-brain drug delivery exploits unique anatomical and physiological connections between the nasal cavity and the central nervous system (CNS) to bypass the restrictive blood–brain barrier (BBB). The primary mechanisms involve direct neuronal transport, extracellular diffusion, perivascular and perineural bulk flow, and auxiliary indirect routes through systemic circulation or lymphatics. These mechanisms are not mutually exclusive; rather, their relative contributions depend on drug properties, formulation characteristics, and site of nasal deposition [5,12,17,22].
1. Overview of Routes
The major routes through which intranasally administered drugs can reach the brain are:
These pathways collectively enable drugs to access multiple brain regions without crossing the BBB directly [1,5,12].
2. Olfactory Neuronal Pathways
2.1 Anatomical Basis
The olfactory region is located in the upper part of the nasal cavity and contains specialized olfactory sensory neurons (OSNs) whose axons traverse the cribriform plate to enter the olfactory bulb. This forms a direct anatomical conduit between the nasal cavity and the CNS [2,13].
2.2 Intracellular Axonal Transport
After intranasal administration, certain substances may be internalized by OSNs via receptor-mediated endocytosis or pinocytosis. Once inside the neuron, they are transported along microtubules via axonal transport mechanisms to the olfactory bulb and subsequently to other brain regions (e.g., cortex, hippocampus) through synaptic relays. This intracellular route, although direct, is typically slow and suited for drugs that can be actively transported within neurons [5,8,9].
2.3 Extracellular Routes Across Olfactory Epithelium
Evidence strongly supports extracellular transport as the dominant mechanism for rapid nose-to-brain delivery. In this case, drugs move through paracellular spaces between epithelial cells, or through perineural channels surrounding the olfactory nerve bundles, reaching the lamina propria. From there, they diffuse along perineural and perivascular routes into the subarachnoid space and cerebrospinal fluid (CSF), often observed within minutes of administration [1,12,13].
Importantly, extracellular transport does not rely on active neuronal processes and is facilitated by bulk flow movements within the perineural and lymphatic compartments [1].
Fig.3.1. Mechanisms of nose-to-brain drug transport via olfactory and trigeminal pathways following intranasal administration
2.3 Cerebrospinal Fluid–Mediated Transport
Several studies have reported rapid detection of intranasally administered drugs in the cerebrospinal fluid, indicating a nose-to-CSF pathway [11,16]. Drugs reaching the subarachnoid space via olfactory or trigeminal routes may distribute throughout the brain via CSF circulation, allowing widespread CNS exposure.
This mechanism is particularly relevant for small molecules and peptides that exhibit high CSF permeability and stability [11].
2.4 Role of Nanocarriers in Mechanistic Transport
Nanocarrier-based systems significantly influence nose-to-brain transport mechanisms by protecting drugs from enzymatic degradation, enhancing mucosal penetration, and modulating interaction with neuronal pathways [17,18].
Polymeric nanoparticles and lipid-based carriers may undergo direct transport along trigeminal pathways while releasing the encapsulated drug during transit or upon reaching the brain [17]. Surface-modified nanoparticles, especially those exhibiting mucoadhesive or charge-mediated interactions, enhance retention in the olfactory region and increase the probability of extracellular diffusion into neural pathways [17].
Micelles and lipid nanoparticles have demonstrated improved brain bioavailability by facilitating both extracellular diffusion and sustained drug release within the nasal cavity [15-17].
2.5 Systemic Absorption and Indirect Brain Entry
In addition to direct neuronal transport, a portion of the intranasally administered dose is absorbed into systemic circulation via the respiratory epithelium [11]. While this fraction does not contribute to direct nose-to-brain targeting, it may reach the brain through conventional BBB transport mechanisms. However, this route is associated with delayed onset and potential systemic side effects and is considered secondary to direct pathways [5,6].
2.6 Comparative Contribution of Transport Pathways
Overall, rapid brain targeting following intranasal administration is primarily attributed to extracellular transport via olfactory and trigeminal pathways, while intracellular axonal transport and systemic absorption play supporting roles [6,16]. The relative contribution of each pathway depends on drug properties, formulation type, particle size, and nasal deposition site [10,15].
3. Trigeminal Nerve Pathway
The trigeminal nerve provides sensory innervation to both the respiratory and olfactory regions of the nasal cavity and represents an additional direct route for nose-to-brain transport [6,12]. Its ophthalmic and maxillary branches project to the brainstem, pons, and spinal cord, enabling drug delivery to regions beyond the olfactory bulb.
Following intranasal administration, drugs deposited in the respiratory epithelium may enter trigeminal nerve endings and be transported to trigeminal nuclei within the brainstem [6]. Compared to the olfactory pathway, trigeminal transport contributes more significantly to drug distribution in posterior brain regions and the spinal cord [12,16].
Both extracellular diffusion along trigeminal nerve fibers and limited intracellular axonal transport have been proposed, with extracellular mechanisms again dominating due to faster kinetics [6].
3.1 Anatomical Basis
The trigeminal nerve (cranial nerve V) innervates the respiratory and olfactory regions of the nasal cavity via its ophthalmic and maxillary branches. These branches carry sensory fibers that project into the brainstem at the level of the pons [5,12,13].
3.2 Trigeminal Transport Mechanisms
Drugs deposited on the respiratory mucosa or within the olfactory region can be taken up by trigeminal nerve endings. Transport can occur via:
Compared with the olfactory pathway, the trigeminal route connects to different CNS regions, including brainstem nuclei and spinal cord, and may contribute to broader brain distribution [1,12].
4. Perineural and Perivascular Bulk Flow
4.1 Perineural Channels
Once substances cross the olfactory epithelium into the lamina propria, they may enter perineural channels — fluid-filled conduits that surround nerve bundles. These channels provide a low-resistance path for drugs to reach the subarachnoid space and mix with CSF, enabling distribution to wide brain areas [1,6].
4.2 Perivascular Routes
Drug molecules can also spread along perivascular spaces around cerebral blood vessels. Convection within these spaces, driven by arterial pulsations, facilitates rapid central distribution beyond the initial site of entry, contributing significantly to the brain distribution of small tracers after intranasal dosing [11]. This perivascular bulk flow is particularly important for achieving more homogeneous CNS exposure than axonal transport alone.
5. Systemic Absorption and Secondary Brain Entry
The highly vascularized nasal respiratory epithelium allows a portion of the administered dose to be absorbed into systemic circulation. Although this does not constitute direct nose-to-brain delivery, once in the bloodstream, drugs may still reach the brain by crossing the BBB via conventional mechanisms (e.g., passive diffusion, carrier-mediated transport) [1,10]. However, this systemic route is slower and less targeted than direct neuronal pathways.
6. Lymphatic Pathways and CSF Exchange
Emerging evidence indicates that the nasal lymphatic system contributes to drug movement into the CNS. Substances reaching lymphatic vessels in the nasal mucosa may travel to the deep cervical lymph nodes and eventually enter the CSF, providing an alternative indirect route that can supplement direct neuronal mechanisms [17].
7. Time Course and Relative Contribution
Experimental studies in animals and humans consistently show that detectable levels of intranasal drugs appear in the olfactory bulb or CSF within minutes, supporting the dominance of extracellular transport over slower intracellular axonal routes [1,12]. Intracellular transport can require hours to days, making it less significant for rapid therapeutic effects, though it may contribute to long-term distribution [5,8].
8. Factors Influencing Mechanistic Pathways
The relative importance of these mechanisms depends on:
For instance, small, lipophilic molecules are more likely to cross mucosa rapidly and enter extracellular pathways, whereas macromolecules and particulates may require carrier systems or enhanced permeation strategies to access neuronal routes effectively [1,22].
EXAMPLES OF DRUGS INVESTIGATED FOR NOSE-TO-BRAIN DELIVERY
ADVANTAGES AND LIMITATIONS OF NOSE-TO-BRAIN DELIVERY
A key advantage of nose-to-brain delivery is its ability to bypass the BBB while minimizing systemic exposure and peripheral side effects [5,9]. Clinical studies involving intranasal insulin have demonstrated improved attention, memory, and cognitive performance in patients with Alzheimer’s disease without significant increases in plasma insulin levels [10,18].
However, several limitations hinder the widespread clinical application of this approach. These include limited dosing volume (25–200 μL per nostril), low olfactory surface area in humans, variability in nasal anatomy, rapid mucociliary clearance, and substantial loss of drug to systemic circulation through the respiratory epithelium [11,14,19].
FACTORS AFFECTING NOSE-TO-BRAIN DRUG DELIVERY
The effectiveness of nose-to-brain drug delivery depends on a complex interaction between physicochemical properties of the drug, formulation-related variables, and physiological characteristics of the nasal cavity. These factors collectively influence nasal deposition, residence time, epithelial permeation, neuronal transport, and ultimately drug concentration achieved in the brain [12]. Inadequate consideration of any one of these parameters can significantly compromise therapeutic outcomes.
5.1 Drug-Related Factors
5.1.1 Molecular Weight and Molecular Size
Low molecular weight drugs (<400 Da) preferentially traverse nasal epithelial barriers through paracellular or transcellular diffusion, enabling rapid access to extracellular perineural pathways and cerebrospinal fluid [1,2]. In contrast, macromolecules such as peptides and proteins are sterically restricted and rely more heavily on intracellular neuronal uptake or carrier-mediated systems to access the CNS [3].
Mechanistic impact:
5.1.2 Lipophilicity
Moderately lipophilic drugs exhibit enhanced epithelial membrane permeation and are more likely to enter extracellular diffusion routes rapidly [2]. Excessively lipophilic compounds, however, may become trapped within epithelial membranes or display poor solubility, limiting effective transport.
Mechanistic impact:
5.1.3 Aqueous Solubility and Dissolution Rate
Sufficient solubility in nasal fluids is essential for maintaining drug availability at the absorption site. Poorly soluble drugs may precipitate within the nasal cavity, resulting in erratic absorption and rapid clearance. Formulation approaches such as nanosystems and lipid carriers are often required to address this limitation [12].
5.1.4 Chemical Form of the Drug and Prodrug Strategy
The chemical form of a drug (salt, ester, free base) significantly affects nasal absorption and pathway selection. Prodrug approaches have been used to enhance lipophilicity or enzymatic stability, thereby improving penetration into neuronal pathways before conversion to the active drug within the brain [4].
Mechanistic impact:
5.1.5 Polymorphism
Polymorphic forms of a drug may differ in solubility, dissolution rate, and stability, which in turn affect nasal absorption and bioavailability [12]. Selection of an appropriate polymorphic form is therefore critical during formulation development.
5.1.6 Biopharmaceutic Properties
Biopharmaceutic characteristics such as permeability, metabolism, and clearance play a crucial role in determining the extent of nose-to-brain transport. Drugs with high permeability but rapid systemic clearance may still achieve effective brain targeting when delivered intranasally due to direct neuronal transport pathways [12].
5.1.7 Stability Against Nasal Enzymes
Drugs susceptible to nasal enzymatic degradation may fail to reach neuronal pathways intact. Encapsulation or chemical modification becomes essential to preserve the drug long enough for transport via perineural or intracellular routes [3].
5.2 Formulation-Related Factors
5.2.1 Dosage Form and Release Profile
Solutions are rapidly cleared from the nasal cavity, favoring systemic absorption over direct brain targeting. In contrast, gels, powders, and mucoadhesive systems prolong residence time in the olfactory region, enhancing neuronal transport [2,5].
Mechanistic impact:
5.2.2 Nanocarrier Systems
Nanoparticles, liposomes, micelles, and lipid carriers protect drugs from degradation and facilitate interaction with neuronal membranes. Particle size and surface charge critically influence whether nanocarriers undergo extracellular diffusion or are internalized by neurons [6,7].
Mechanistic impact:
5.2.3 Surface Modification
Surface functionalization with mucoadhesive polymers or targeting ligands increases retention in the olfactory region and promotes neuronal uptake, biasing transport toward olfactory and trigeminal routes [6].
5.2.4 Drug Concentration
Drug concentration directly affects the concentration gradient across the nasal epithelium and thus influences absorption. However, increasing drug concentration is limited by nasal irritation, solubility constraints, and dose volume restrictions [12].
5.2.5 pH and Buffer Capacity
The pH of nasal formulations should ideally lie between 4.5 and 6.5 to minimize mucosal irritation and maintain ciliary function [11]. Excessive buffer capacity may disrupt the physiological nasal environment and impair mucociliary clearance.
5.2.6 Osmolarity
Isotonic or slightly hypotonic formulations are preferred for nasal administration. Hypertonic formulations can cause epithelial dehydration, discomfort, and increased mucociliary clearance, reducing drug residence time [11].
5.2.7 Viscosity
Formulation viscosity influences nasal retention and clearance. Moderate increases in viscosity can prolong residence time and enhance absorption, whereas excessive viscosity may interfere with ciliary movement and reduce drug diffusion [11].
5.2.8 Preservatives
Preservatives are commonly added to multidose nasal formulations to prevent microbial growth. However, certain preservatives may cause mucosal irritation or ciliotoxicity, necessitating careful selection and concentration optimization [11].
5.2.9 Antioxidants
Antioxidants are incorporated to prevent oxidative degradation of susceptible drugs during storage and administration. Their compatibility with nasal tissues and formulation components must be carefully evaluated [11].
5.2.10 Humectants
Humectants help maintain moisture within the nasal cavity and prevent mucosal drying, thereby improving patient comfort and formulation tolerability [11].
5.3 Physiological and Pathological Factors
5.3.1 Effect of Deposition Site on Absorption
The site of drug deposition within the nasal cavity critically influences absorption and brain targeting. Deposition in the olfactory region favors direct nose-to-brain transport, whereas deposition in the respiratory region leads predominantly to systemic absorption [11,14]. Improper deposition significantly reduces targeting efficiency.
Mechanistic impact:
5.3.2 Mucociliary Clearance
Mucociliary clearance rapidly removes administered formulations from the nasal cavity, limiting the time available for drug absorption. Clearance typically occurs within 15–30 minutes and represents a major physiological barrier to effective nasal delivery [12].
5.3.3 Nasal Blood Flow
High blood flow in the respiratory epithelium promotes systemic uptake, which may reduce the fraction of drug available for direct neuronal transport to the brain [11].
5.3.4 Enzymatic Activity
Metabolic enzymes present in nasal mucosa can degrade drugs prior to absorption, particularly peptides and proteins, thereby reducing bioavailability [12].
5.3.5 Effect of Pathological Conditions
Pathological conditions such as rhinitis, sinusitis, nasal polyps, and infections alter mucus composition, epithelial permeability, and clearance rates, leading to significant variability in drug absorption and therapeutic response [12].
5.3.6 Time-Dependent Transport Dynamics
Extracellular pathways enable drug detection in the brain within minutes, whereas intracellular axonal transport requires hours to days. Thus, drugs intended for rapid onset of action rely predominantly on extracellular diffusion rather than neuronal axonal transport [1,4].
FORMULATION STRATEGIES FOR ENHANCED NOSE-TO-BRAIN DRUG DELIVERY
To overcome anatomical, physiological, and biochemical barriers associated with intranasal administration, advanced formulation strategies have been developed to enhance drug retention, stability, absorption, and neuronal transport to the brain [14,15].
6.1 Conventional Nasal Dosage Forms
Conventional nasal solutions, suspensions, and powders are simple to formulate but suffer from rapid clearance and limited targeting efficiency. Their use is generally restricted to drugs with favorable physicochemical properties [16].
6.2 Mucoadhesive Drug Delivery Systems
Mucoadhesive systems utilize polymers such as chitosan, carbopol, and cellulose derivatives to increase adhesion to nasal mucosa, thereby prolonging residence time and enhancing absorption [14]. Chitosan additionally enhances paracellular transport by transiently opening tight junctions while maintaining an acceptable safety profile [14,15].
6.3 In Situ Gelling Systems
In situ gelling systems undergo sol-to-gel transition upon exposure to physiological conditions, resulting in increased viscosity at the administration site. This property reduces clearance and allows sustained drug release, leading to improved brain bioavailability [14].
6.4 Nanocarrier-Based Drug Delivery Systems
Nanocarriers play a central role in modern nose-to-brain delivery by improving solubility, stability, controlled release, and interaction with neuronal pathways [15,16].
6.4.1 Polymeric Nanoparticles
Polymeric nanoparticles protect drugs from enzymatic degradation and enable controlled release, facilitating transport along olfactory and trigeminal pathways [15].
6.4.2 Lipid-Based Nanocarriers
Lipid-based carriers such as liposomes, solid lipid nanoparticles, and nanostructured lipid carriers enhance mucosal interaction and neuronal uptake due to their lipidic composition [16].
6.4.3 Polymeric Micelles
Micelles improve the delivery of poorly water-soluble drugs and have demonstrated significantly enhanced brain exposure following intranasal administration [15,16].
6.4.4 Surface-Modified Nanocarriers
Surface modification with mucoadhesive polymers or charge-based ligands enhances retention in the olfactory region and increases the probability of neuronal transport to the brain [16].
REFERENCES


Dr Sudha Rathod, Anjali Rai, Govind Vishwakarma*, Nose-To-Brain Drug Delivery: Mechanisms, Influencing Factors, And Formulation Strategies, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 1027-1038. https://doi.org/10.5281/zenodo.18513242
 10.5281/zenodo.18513242
10.5281/zenodo.18513242
