1Department of Pharmaceutics, Karnataka College of Pharmacy
2Department of Industrial pharmacy, Karnataka College of Pharmacy
Acne is a multicausal dermatological condition in people of different age groups that tends to produce physical pain and psychological distress. Traditional treatment measures, such as topical and systemic drugs, have proven effective but are commonly related to side effects, patient compliance issues, and the development of antibiotic resistance. Recent developments in nanotechnology, especially nanogels, have created new avenues for the treatment of acne by facilitating targeted drug delivery, controlled release, and enhanced skin penetration. Customized nanogel formulations provide a new strategy that individualizes treatment according to patient requirements, optimizing therapeutic effects with reduced side effects. This review considers the position of tailored nanogel-based therapies in acne treatment, their strengths compared to traditional therapies, how they can solve present limitations in treatments, and where research is heading in this emerging field.
Skin disease acne presents as a persistent inflammatory condition that affects hair follicles and sebaceous glands due to Propionibacterium acnes colonization and the resulting inflammatory response [1]. The development of acne results from diverse skin microbes, including Propionibacterium acnes and Malassezia species, which impact sebum production and both comedones generation and inflammation formation in the skin tissue [2]. Acne development symptoms develop due to Propionibacterium acnes which exists as a human skin bacterium that lives alongside humans. Acne represents a widespread skin issue that affects everyone across different age groups, according to the Global Burden of Disease Study 2010, which recorded a global prevalence rate of 9.38%. Pustules, papules, and comedones form part of acne, alongside cysts and nodules, which appear only in severe cases. This dermatological condition is the most frequent skin diagnosis treated by medical professionals, who work with dermatological patients, as its occurrence mainly targets young people throughout adolescence and early adulthood, while existing beyond treatment years [1-2]. Nanogels form through physical and chemical crosslinking between polymers and hydrogels produced at nanometer dimensions, ranging from 20 to 200 nm. The unique characteristics of these nanogels include a significant surface area and hygroscopic properties, as well as a deformable morphology. The three-dimensional structure of nanogels enables them to release medications and liquids or polymers in controlled, sustained deliveries. This specific structure allows them to hold molecules that are larger in size. Because nanogels transport drugs, they establish biomolecular bond interactions, which involve hydrophobic contacts, hydrogen bonds, and salt bridges with pharmaceutical compounds. Nanogels possess exclusive characteristics of both solid and liquid phases simultaneously in their material composition. The treatment impact is directly proportional to the amount of time nanoparticles spend attached to the skin after being captured inside nanogel structures [3]. Personalized care plays a crucial role in managing chronic skin conditions, as the success of treatment largely depends on how well patients stick to their prescribed routines. Several factors can influence treatment adherence, including the patient's own characteristics and beliefs, the relationship between the healthcare provider and the patient, and aspects related to the treatment itself. These aspects include how effective the treatment is, its acceptability, side effects, how easy it is to tolerate, how often it needs to be used, the duration of the treatment, and how it is administered [4].
Current acne treatment is multi-faceted and targeted at the severity and type of acne. For mild cases that present with many comedones, topical retinoids such as adapalene or tretinoin are first-line treatments, often with a progression to systemic isotretinoin when needed. Benzoyl peroxide is the first-line treatment for papulopustular acne, and it may be used in combination with topical antibiotics or retinoids. In nodulocystic acne, oral tetracyclines are given, and isotretinoin is reserved for severe cases. Treatments of acne scars also include non-ablative laser therapy and chemical peels. The choice of treatment is determined by the specific clinical manifestations of acne and must balance efficacy with minimizing side effects [5].
Classification of acne
Table: Clinical classification of acne [6-8]
|
Sn |
Type |
Type of Injury |
Type of Acne |
Degree |
Gravity |
|
1 |
Inflammatory |
Pustule |
Papular-pustular |
II |
Moderate |
|
Pimple |
|||||
|
Nodule |
Nodular |
III |
Moderate to severe |
||
|
Scar |
IV or conglobate |
Severe |
|||
|
Cyst |
V or fulminant |
Serious |
|||
|
2. |
Non-inflammatory |
Blackhead |
Comedonica |
I |
Mild |

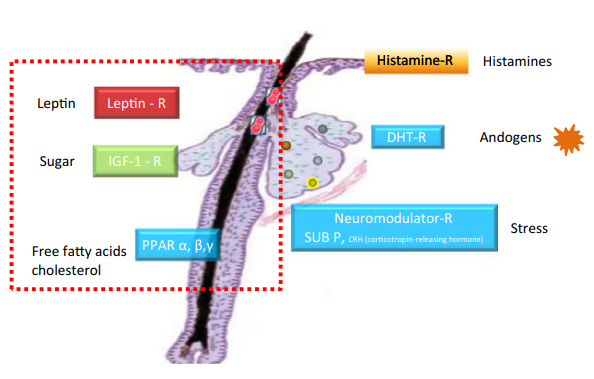
Pathophysiology of Acne
Sebum production is regulated by various receptors in the sebaceous gland. In addition to histamine receptor activated by histamines, DHT receptor activated by androgens and corticotrophin releasing hormone (CRH) receptor which are mainly activated by stress [9]. Recent research has identified three more: peroxisome proliferator-activated receptors (PPARα, β, and γ) are activated by free fatty acids and cholesterol, IGF-1 receptor stimulated by sugar, and the leptin receptor triggered by fat [10]. Leptin, a hormone linked to lipid metabolism and inflammation, promotes lipid droplet formation and induces proinflammatory cytokines (IL-6, IL-8), suggesting a connection between diet and inflammatory acne. Studies also indicate a correlation between high BMI and acne risk, particularly in adolescent girls, though further evidence is needed [11].
Women with hyperandrogenism show their acne symptoms before their menstruation cycle and maintain elevated serum DHEAS concentrations and raised antimullerian hormone together with vellus hair growth at their upper lips and peri-ocular areas and around their cheeks [12]. The health ministry's regulatory change in 2013 which reached French participants caused acne symptoms to worsen for 83.9% of people due to peripheral hyperandrogenia activated androgen receptor mechanisms [13]. Research demonstrated that spironolactone holds greater promise than isotretinoin since it regulates sebum that hormones trigger and controls hair growth simultaneously. The pilot study demonstrated that sixteen women taking 75-150 mg per day of spironolactone with third-generation contraceptives alongside topical treatment showed positive results in their condition during 6-12 months [14]. Research shows that topically applied spironolactone delivery through lipid nanoparticles needs further scientific testing of delivery methods.
Lipid mediators known as endocannabinoids fulfil multiple roles in biological processes because they participate in skin functions such as proliferation, differentiation, apoptosis, and immune regulation [15]. The cutaneous endocannabinoid system functions to maintain balance between skin cells; however, any disturbance within it can cause skin conditions [16]. Acne treatment research into the Endocannabinoid System pathways shows potential for cannabidiol because a 2014 in vitro investigation indicated its lipostatic, antiproliferative, and anti-inflammatory actions, which suggest therapeutic benefits for acne vulgaris [17].
A distinctive microbial print shapes the microbial community that exists on the skin surface, which contains bacteria, along with fungi, viruses, and parasites [18]. This structure maintains proper microbial relationships and helps defend our body through its immune defences. The human skin develops under the effects of both internal hormonal and genetic, as well as external cosmetic and dietary factors. The skin condition P. acnes contribute to acne development, whereas Malassezia furfur causes seborrheic dermatitis, and S. aureus and S. pyogenes disrupt skin balance. The presence of S. epidermidis maintains P. acnes inhibition, which subsequently decreases the numbers of S. aureus and S. pyogenes populations [19]. The development of dysbiosis through disruptions results in reduced skin barrier strength and produces inflammatory responses. Acne-related dysbiosis affects sebum production and P. acnes levels, so that inflammation worsens due to TLR-2 activation and cytokine release. Acne treatment requires achieving a balance of the microbiome as one of its main therapeutic objectives [20].
Immunity in human skin relies on native and adaptive immune system responses [21]. Keratinocytes control immune response activation because they express pattern recognition receptors (PRRs), including TLRs and PARs, that detect microbes, enabling them to release antimicrobial peptides (AMPs) and cytokines to enhance immune responses [22]. The activation of the NLRP3 inflammasome through P. acnes causes monocytes and sebocytes to produce IL-1β, while proteases and ROS regulate this process. P. acnes simultaneously stimulate the secretion of IL-17A and IFN-γ to drive Th17/Th1 responses, which demonstrates the essential role of Th17 cells in acne pathogenesis [23]. The use of nitric oxide nanoparticles (NO-np) brings effective control of P. acnes-induced inflammation through their ability to lower inflammatory cytokine production. The antibacterial function of P. acnes rests on linoleic and sapienic acid FFAs, together with hBD-2, which facilitates AMP production [24]. Heat-sensitive antimicrobial peptides demonstrate properties that make them candidates for acne treatment enhancement of topical retinoids.
Top of Form
The biofilm structure formed by P. acnes from extracellular polysaccharides helps the bacteria bind to follicles while it alters integrin function to support bacterial multiplication. P. acnes biofilm formation increases both drug resistance and prevents host immune activity, which worsens acne severity [25]. Microcomedone in acne patients form due to propionic acid secretion from P. acnes, while the bacteria affect keratinocyte structure. The application of antibacterial benzoyl peroxide or botanical agents may work as alternatives to defeat P. acnes biofilm formation without causing bacterial resistance [26].
Current treatment strategies
Current treatment strategies for acne focus on addressing the various factors contributing to its pathogenesis, including abnormal keratinization, increased sebum production, microbial colonization, and inflammation [27].
|
Treatment |
Mechanism of action |
Common side effects |
Indications |
References |
|
Benzoyl peroxide |
Release free oxygen radical that kills bacteria; peels out the inner lining of the hair follicle, causing skin peeling |
Dryness, irritation, potential bleaching of clothes |
Mild to moderate acne |
28,29 |
|
Retinoids (e.g., tretinoin, adapalene) |
Normalizes keratinocyte differentiation, comedolytic effect, anti-inflammatory |
Dryness, photosensitivity, irritation, burning
|
Mild to severe acne, depending on the formulation |
30 |
|
Antibiotics (e.g., clindamycin, minocycline) |
Antimicrobial; reduces inflammation |
Skin irritation, resistance development |
Mild to moderate inflammatory acne |
31
|
|
Azelaic acid |
comedolytic; normalizes keratinization; anti-inflammatory |
Skin irritation, burning, redness, and itching |
Mild to moderate acne |
32,33 |
|
Treatment |
Formulation |
Dose, Frequency |
Common Side Effects |
References |
|
Tretinoin/Clindamycin |
Gel |
0.025%/1.2% daily |
Xerosis, irritation, allergic contact dermatitis, erythema |
34 |
|
Tretinoin/Benzoyl peroxide |
Cream |
0.1%/3% once daily |
Xerosis, irritation, allergic contact dermatitis, erythema |
35 |
|
Benzoyl peroxide/Erythromycin |
Gel |
5%/3% once daily |
Xerosis, irritation, allergic contact dermatitis, erythema, bleaching of fabrics |
36
|
|
Clindamycin/Benzoyl peroxide/Adapalene (IDP-126) |
Gel |
1.2%/3.1%/0.15% |
Xerosis, irritation, allergic contact dermatitis, erythema |
37
|
|
Treatment |
Mechanism of Action |
Common Side Effects |
Indications |
References |
|
Isotretinoin |
Reduces sebaceous gland size and sebum production, anti-inflammatory |
Dryness, teratogenicity, elevated liver enzymes |
Severe scarring acne or acne not responsive to other treatments |
38,39 |
|
Oral antibiotics (e.g., tetracycline, doxycycline) |
Antimicrobial, anti-inflammatory actions |
Gastrointestinal upset, photosensitivity |
Moderate to severe acne |
40 |
|
Hormonal therapies (e.g. oral contraceptives) |
Regulate hormonal imbalance, reduce sebum production |
Mood changes, breast tenderness, thrombosis risk |
Hormonally influenced acne, adult women |
41,42 |
|
Treatment |
Mechanism of Action |
Indications |
Common Side Effects |
References |
|
Photodynamic therapy |
Activates photosensitizing agents that kill bacteria and reduce sebum production |
Severe acne, acne resistant to other treatments |
Redness, swelling, skin sensitivity to sunlight |
43 |
|
Blue-light therapy |
Kills C. acnes bacteria using blue light without damaging the skin |
Mild to moderate acne |
Temporary redness and dryness |
44 |
|
Supplement |
Mechanism of Action |
Common Side Effects |
Indications |
References |
|
Vitamin D |
Modulates immune system, may reduce skin inflammation
|
Rare, potentially increased calcium levels |
Various acne types
|
45
|
|
Omega-3 fatty acids |
Anti-inflammatory, modulates sebum production
|
Fishy aftertaste, gastrointestinal upset |
Various acne types |
46 |
Limitations of conventional treatment [47-50]
Rationale for Personalized Acne Treatment:
Nanogels
The term "nanogels" refers to microscopic particles made of cross-linked polymer networks that expand quickly when a solvent penetrates them. The term “nanogel” (NanoGel™) originally referred to two-part bifunctional systems where polyionic and non-ionic polymers combined.
Advantages
Nanogels can be considered a superior drug-delivery system due to its numerous advantages.
Disadvantages
a) The technique to completely remove the solvent and surfactants at the end of the preparation process is expensive.
b) Surfactant or monomer traces may remain and can impart toxicity [59].
Classification of nanogels
|
SN |
Based on types |
Types |
Examples
|
|
|
|
Structured based nanogel
|
|
Artificial chaperone, cholesterol-bearing pullulan nanogel [62] |
|
|
Stimuli sensitive/responsive nanogel [63] |
|||
|
Stimuli sensitive/responsive nanogel [64] |
|||
|
Stimuli-responsive nanogel [65] |
|||
|
|
Stimuli sensitive/responsive nanogel [66] |
|||
|
|
Polyethyleneglycol-b-poly (methacrylic acid) [PEG-b-PMA] with PEG terminal aldehyde functionality [67] |
|||
|
|
Response based nanogel [68,69] |
|
|
|
|
|
|||
|
|
Linkage based nanogel [69,70] |
|
|
|
Interaction |
|
|||
|
|
|||
|
|
|
||
|
|
|||
|
|
|||
Drug release mechanisms [71-75]
When an aqueous medium enters the nanogel structure through its porous surface, the nanogel absorbs the liquid and expands. This swelling process facilitates the gradual release of the drug contained within the gel. The speed and extent of drug release depend on how much the nanogel swells in response to the surrounding environment. The mechanism of drug release may be classified in three categories:
1. Diffusion-Controlled Release
2. Swelling-Controlled Release
3. Chemically Controlled Release
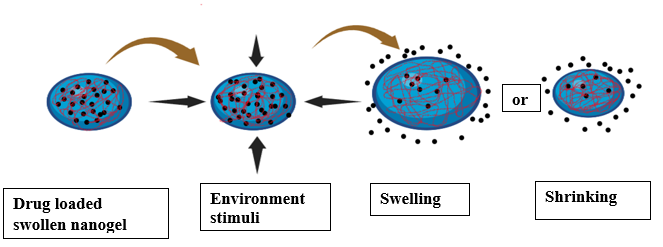
Fig: Drug release mechanism of nanogel
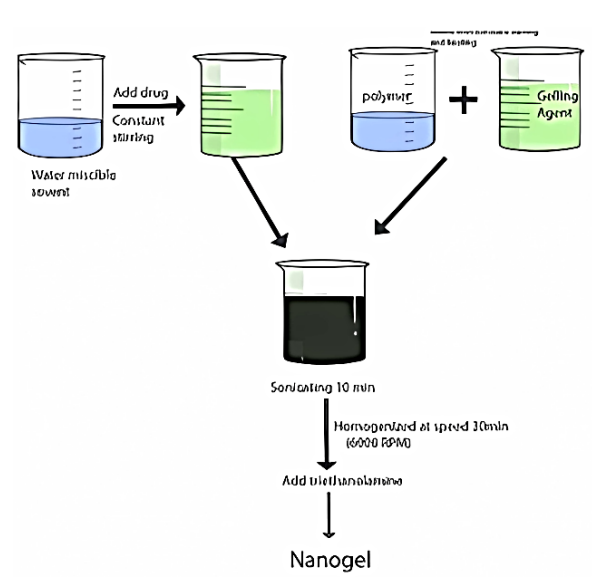
Nanogel Preparation Methods
The drug in the aqueous solution is solubilized in an organic solvent. A gelling agent and polymer are dissolved in water to form the drug phase. Later it is added dropwise to the aqueous phase. This mixture is homogenized at 6000 rpm for 30 minutes, resulting in an oil-in-water emulsion with droplet sizes typically under 200 nm, enhancing solubility and stability [76]. To form the nanogel, triethanolamine is introduced to the emulsion and stirred continuously at 8000 rpm for one hour. This step is crucial as triethanolamine acts as a stabilizer, improving the emulsion's thermodynamic stability and enhancing drug delivery efficiency [77].
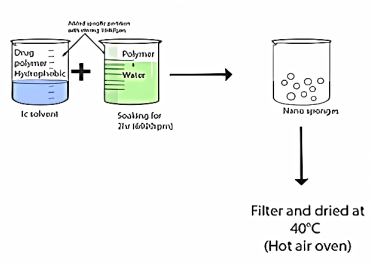
Initially, a drug-polymer mixture is injected into an aqueous phase while continuously stirred at 1000 rpm for two hours [78]. Following this, the resulting nanosponges undergo filtration and are dried in a hot air oven at 40°C for 24 hours. For optimal dispersion, it is recommended to immerse the polymer in water for two hours before gel formation, followed by agitation at 6000 rpm [79]. The pH of the mixture is then adjusted using a pH-modifying agent, and finally, the aqueous dispersion is combined with the optimized nanosponges suspension and permeation enhancers [80].
In this method, the organic phase, which contains both the drug and polymer, is introduced into an aqueous surfactant solution. This interaction causes the polymer to precipitate out, forming nanoparticles. Once the excess solvent is removed, the resulting polymeric nanoparticles are collected [81]. Gelling agent and necessary amounts of nanoparticle dispersion are added after moistening the particles. The pH is stabilized by using triethanolamine [82].

The initial step involves dissolving the polymer, drug and surfactant in an organic solvent. A cross-linking agent is added, it must be incorporated over an extended period of time during the night [83]. The formed nanoparticles undergo purification, followed by solvent evaporation to yield a solid form. Mixing the dried nanoparticles with an aqueous gelling agent leads to the formation of a nanogel. The application of a neutralizing substance modifies the pH [84].

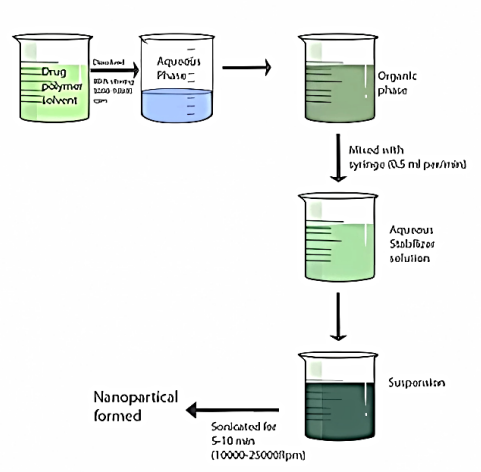
The drug-polymer mixture is agitated in an aqueous phase at a high rotational speed of 5000 to 10,000 rpm, facilitating the formation of an organic phase [85]. A syringe fitted with a needle is used to add the organic phase at a rate of 0.5 mL per minute to the aqueous stabilizer solution. After six minutes of agitation at speeds between 10,000 and 25,000 rpm, sonication is applied for five to ten minutes to further stabilize the suspension.
Characterization [86,87]
Among the techniques for measuring nanoparticle size distributions in liquids stands dynamic light scattering (DLS) as a valuable method. The analysis of nanogel solution behaviour depends on the microsecond-range light scattering capabilities of this technique. Nanogel size relationship to cross-linkers and polymer chain charge becomes more feasible through DLS-powered determination of effective hydrodynamic radii. The measurement technique monitors the size behaviour of nanogels in multiple solution conditions.
The analysis of particle surfaces and sizes utilizes electron microscopy for its effectiveness. Using scanning electron microscopy (SEM) enables users to study nanogel morphology and milli-meter size measurements between 50 and 80 nm can be done. Circular Dichroism (CD) Spectroscopy The optical activity of final products can be measured effectively via Circular dichroism (CD) spectroscopy. CD operates best for identifying chiral molecules among nanogels. CD spectroscopy interacts with helical molecular formations that result in macromolecular arrangements detectable by the technique. The structures feature a core with chirality.
Materials separate by size through the application of Size-exclusion chromatography (SEC) technique. The main purpose of SEC is to analyse both the molar weight distribution of nanogels and measure molar fractions' volume.
Field-flow fractionation (FFF) uses a cross-flow to separate suspensions or solutions that pass through elongated narrow channels. The perpendicular motion of the cross-flow operates independently from the primary flow direction treatment. The technique depends on particle movement throughout the solution while components separate at different speeds resulting from their size and mass differences.
Evaluation [88]
|
Application:
Nanogels can incorporate bioactive compounds that have beneficial effects, such as antioxidants, anti-inflammatory agents, or antimicrobial substances. Being nano in size, they will most likely penetrate the skin layers better and help deliver the active ingredients to the focused area of action [89].
Nanogels can provide the controlled and sustained release of encapsulated active ingredients. This could lead to an extended therapeutic action, reducing application frequency while enhancing treatment efficacy for acne prone skin [90].
An injectable nanogel system has been developed for diabetes management, responding to blood glucose levels by releasing insulin. It consists of oppositely charged particles forming a pH-sensitive gel matrix. Using dextran, the nanogel delivers insulin and enzymes that convert glucose into gluconic acid, lowering pH and triggering insulin release during hyperglycaemia. While promising, further research is needed for clinical application [91].
Nanogels enhance local anaesthetic delivery in dental treatments, improving pain control and prolonging effects. Procaine hydrochloride, loaded into methacrylic acid ethyl acrylate nanogels via hydrophobic and hydrogen bonds, shows increased release at high pH. Deprotonation of the nanogel acid triggers osmotic swelling, increasing porosity and drug release. With minimal pain and extended circulation, nanogels are a promising anaesthetic delivery system [92].
Nanogels offer an effective system for delivering oligodeoxynucleotides (ODN) to the brain, which is essential for treating neurodegenerative diseases. High-molecular-weight molecules struggle to cross the blood-brain barrier (BBB) and are rapidly cleared from circulation. However, when ODN is encapsulated or bound to nanogels, it forms stable polyelectrolyte complexes with particle sizes under 100 nm, enabling successful BBB penetration. Modifying the nanogel surface with insulin or transferrin further enhances transport efficiency [93].
Vaginal nanogels loaded with antibacterial drugs are used to treat various vaginal infections and alleviate symptoms like irritation, excessive secretion, and other sexual health issues. However, they are not recommended during menstruation or pregnancy. Some nanogels containing antiretroviral drugs have shown potential in reducing the risk of HIV infection in women. One such example is Tenofovir, a vaginal gel studied for HIV prevention. It was formulated using gelatin nanoparticles through a two-step desolvation method, with HPMC K15M serving as both a gelling and bio adhesive agent. Studies on membrane permeability and bio-adhesion demonstrated strong adhesion properties and enhanced drug absorption [94].
The nanogel protects the active compound resulting degradation from environmental factors such as light, heat, or oxygen. Such stability is an important aspect for cosmetic formulations; it ensures the maintenance of ingredient efficacy over time [89].
Treatment challenges [95-98]
AFA often presents with both inflammatory and non-inflammatory lesions, which complicates treatment strategies. This mixed presentation requires tailored approaches that differ from traditional acne treatment aimed at younger population.
The chronic and ongoing nature of AFA means that patients can necessitate long-term management strategies. Improvements in skin condition may take up to three months, which can be frustrating for the patient who seeks timely results.
In most cases, adult female acne causes a significant impact on the patient’s quality of life that is often independent of the severity of their acne. This would require dermatologic treatment coupled with psychological rehabilitation.
The disease condition is partly hormonal in causes related to menstrual cycles and stress, and entirely related factors such as diet and sleep patterns. These issues make the treatments even more complex.
The patient needs to sometimes alter many habits and routines to control the condition. Complying with therapeutic regimens, perhaps including dietary modification, skincare modification, and medications can be challenging.
The next requirement in favour of the problem is dealing with pregnancy plans, breastfeeding and individual sensitivity to skin, which makes it difficult to select the anti-acne drugs. This treatment requires a tailored approach.
Future direction
Future directions in acne treatment focus on several key advancements. These include the development of microencapsulated medications for improved drug delivery and reduced side effects, as well as combination therapies that simplify treatment regimens. Research into targeted treatments, such as engineered antimicrobial peptides to combat antibiotic resistance, is also promising. Furthermore, innovative compounds like cannabinoids and probiotics are being explored for their potential benefits. Lastly, a shift towards personalized medicine aims to tailor treatments to individual patient profiles, enhancing efficacy and adherence
CONCLUSION
Personalized nanogel formulations for acne treatment are evolving as an advanced approach that resolves the problems of conventional therapies. Nanogels demonstrate properties that enable effective acne treatment through the targeted delivery of medications, controlled substance release, and improved skin absorption capability. Detailed patient-tailored care treatments both analyse specific medical attributes and personal needs, leading to better medication adherence and better treatment satisfaction outcomes. Developments in nanotechnology support the integration of patient-specific treatments into medical practice, which promises improved results and a better quality of life for patients suffering from acne. Future studies should work to optimize these formulations and analyse their prolonged effectiveness and safety in different patient groups.
REFERENCES




Sara Rai*, Beny Baby, S. Rajarajan, Survi Barnawal, Enhanced Acne Treatment Efficacy: The Role of Personalized Nanogel Formulation, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 1296-1396. https://doi.org/10.5281/zenodo.15191340
 10.5281/zenodo.15191340
10.5281/zenodo.15191340
