Ideal Institute of Pharmacy, Posheri, Wada
The most frequent cause of dementia is Alzheimer's disease (AD), a neurodegenerative illness. There is no permanent cure, so better treatment approaches are required despite the significant financial burden on the world and the effects on the patients' immediate families. Although AD has a severe impact on memory and cognition, the precise cause is still unknown. The utility of the suggested approach is then confirmed by a number of interesting numerical examples, one of which has been confirmed by a real-world application of the benchmark problem that is associated with the designed. Despite the progress we've made, there haven't been many clinical trials focused on proving neuroprotection. The authors aimed to pinpoint potential neuroprotective agents that could be tested in future clinical trials. It’s thought that using natural product mixtures or extracts that contain various bioactive compounds could be a promising strategy in discovering drugs for Alzheimer’s disease. These compounds might work together, either additively or synergistically, to provide multiple neuroprotective benefits. In this review, we take a fresh look at the neurobiological effects of lithium, considering the evidence that highlights its neurotrophic and neuroprotective qualities. We also explore the reasons behind its use in treating and preventing neurodegenerative diseases. These days, most of the new treatments being developed aim to modify diseases by focusing on amyloid plaques or the neurofibrillary tangles associated with tau. There's a growing emphasis on spotting and proactively treating patients who are in the early stages of Alzheimer's disease, as well as those who have risk factors for cognitive decline.
Alzheimer’s disease acknowledges that it is a progressive dementia's primary cause, neurodegenerative disease in late adulthood. (1) AD is a progressive neurodegenerative disease that causes memory loss, cognitive decline, physical function loss, and eventually death from brain cell death. One of the most prevalent causes of dementia in the general population is Alzheimer's disease (AD). There are two main categories of AD: sporadic AD (SAD) and early onset/familial AD (FAD).(2) According to estimates, the prevalence of AD will reach 13.8 million by 2050, with a new case occurring every 33 seconds, or almost a million new cases annually.(3) These changes in AD are brought on by low levels of neurotransmitters in the brain, synaptic loss, and neuronal degeneration.(4) Clinical features are used to make the diagnosis of AD, but brain histopathological analysis should be performed to confirm it.(5) Understanding normal memory and brain function is crucial before delving into the specifics of the mechanisms underlying the progression of AD.(6) In this review article, we aimed to review the neuro-protective properties of riluzole, a glutamate modulator, in AD, which could benefit patients with the disease. ) The onset and progression of AD are related to Neuroinflammation, oxidative damage, and neurotrans-Mitter dysregulation. (7) The cognitive decline Is accompanied by impaired performance of daily activi-Ties, behavior, speech and visual-spatial perception. (8) However, neuroinflammation can be harmful too, leading to neuronal damage. Benefits and detriments balance depends largely on the magnitude of the immune response.(9) As people are living longer and the baby boomer generation hits the milestone of 65, the number of individuals aged 65 and older in the world is on the rise.(10) While we still don’t have a complete grasp on the exact biological causes of Alzheimer’s Disease (AD) for most individuals, it’s widely accepted that the key features of this condition include the unusual buildup of insoluble β-amyloid peptide (Aβ) and the formation of neurofibrillary tangles (NFTs) made up of phosphorylated tau protein within the neurons. This process ultimately leads to neuron atrophy and death. (11)
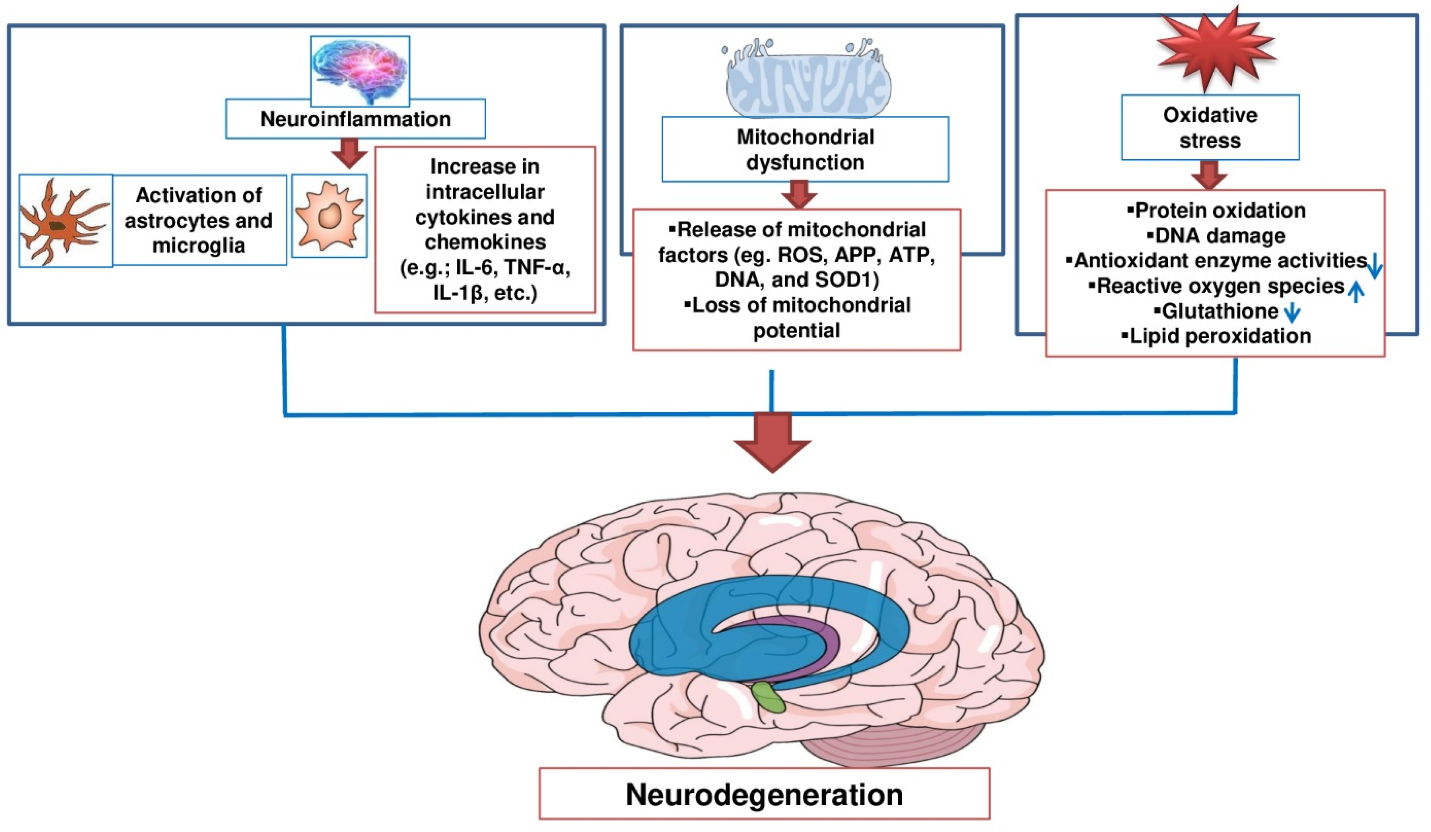
Fig.1: Therapeutic potential of natural product in treating neurodegenerative (77).
In this section, we’ll take a closer look at the latest insights into Alzheimer’s disease, covering everything from its epidemiology and genetics to its pathology and how it develops. After that, we’ll dive into how the disease presents clinically, explore the treatment options available today, and discuss potential future therapies (12). Many of these pathological features can be directly tied to metabolic abnormalities, and it's becoming increasingly clear that metabolic dysfunction plays a significant role in Alzheimer's disease (13). These diseases have multiple causes and often lack early warning signs, which leads to them being diagnosed much later than they should be (14). In simpler terms, the medications used to treat these conditions typically don’t have the ability to stop neurodegeneration or address the progressive nature of the diseases. They mainly focus on alleviating symptoms. This limitation is partly due to a lack of understanding about the underlying pathology that leads to these central nervous system disorders (15). They point out that there's some unusual processing happening with two key proteins: amyloid precursor protein (APP) and tau. The current evidence from neuropathology, genetics, and molecular biology backs up the neurobiological theory, suggesting that these changes affect the series of events that play a crucial role in how APP and tau protein are metabolized as we age (16). Detecting Alzheimer's disease (AD) in its early, asymptomatic stages is crucial. By validating biomarkers as reliable indicators of AD pathology, we could use them as diagnostic tools. This would mean we wouldn't need to rely on brain samples or autopsies to confirm a diagnosis (17).
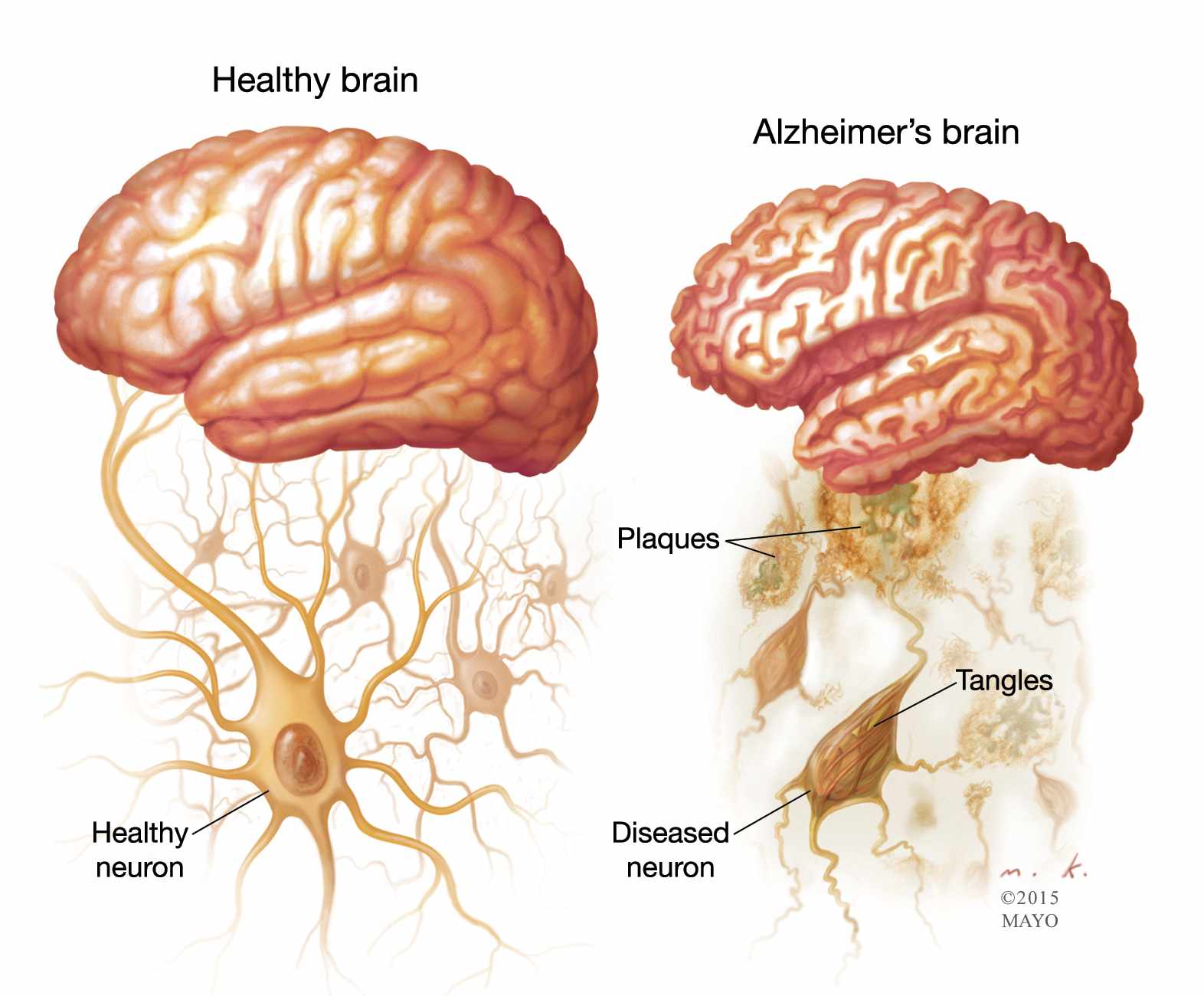
Fig. 2: Two Hit Treatment to Combat Alzeimer’s Disease (78).
While most of the known monogenic forms of Alzheimer's disease (AD) have been identified in cases of familial early-onset AD, recent research suggests that the clinical presentation is actually much broader, encompassing late-onset and sporadic forms as well. In fact, monogenic AD can manifest a variety of symptoms that go beyond just memory loss, highlighting the need for careful evaluation (41). AD presents unique challenges when it comes to picking out relevant information, as it can be tough to distinguish what's important from what's not. This often leads to difficulties in focusing on multiple stimuli and managing attention effectively. Additionally, it seems that while lexical and semantic skills might be affected, phonological and syntactic abilities tend to remain relatively intact (43). Numerous studies have indicated that structural MRI scans, which assess tissue damage or loss in key brain areas like the hippocampus and entorhinal cortex, can predict the progression to Alzheimer's disease (AD) (44). There's a growing interest in finding ways to prevent Alzheimer's Disease. Ideally, we should base our prevention strategies on the findings from large-scale primary prevention trials. Unfortunately, very few of these trials are currently underway. Designing one of these trials is quite complex, and even if we were to start one today, it could take decades before we see any results (45). Alzheimer's disease (AD) typically starts with a gradual decline in memory, which may be accompanied or followed by various cognitive issues. These can include problems with visuospatial skills, difficulties with navigation, challenges in executive functioning, and disturbances in language (46). While most patients tend to develop Alzheimer's disease (AD) later in life, it's actually the research on the rare autosomal dominant early-onset form of AD that has shed significant light on how the disease develops. Researchers have pinpointed fully penetrant (causal) mutations in three specific genes that lead to early-onset familial AD (47). The biological role of tau, which is mainly a protein found in neurons, is crucial for promoting the assembly and stability of microtubules, and this process is influenced by how much it is phosphorylated. Typically, normal tau has about 2 to 3 moles of phosphate for every mole of the protein, which is the ideal level for it to function effectively. However, when tau becomes hyperphosphorylated, it actually hinders its ability to assemble microtubules and bind to them properly (48). Developing drugs for Alzheimer’s disease (AD) is notoriously challenging, with a high rate of failure. However, we can enhance our decision-making in drug development by learning from previous trials. By improving how we interpret animal models, refining pharmacologic characterization during phase I and II trials, ensuring we have the right sample size, using biomarker support for AD diagnosis, optimizing global recruitment strategies, and steering clear of inappropriate subgroup analyses, we can significantly boost the chances of success in drug development (49).
Etiology and it’s risk factors:
Both genetic and environmental factors contribute to the development of Alzheimer's disease (AD). The most significant risk factor is age. By the time someone reaches 65, the chance of having AD is about 3%, and this jump to over 30% by age 85. For those under 65, the numbers are a bit murkier, but estimates indicate that this group makes up roughly 3% of AD cases. While the overall prevalence is on the rise due to an aging population, the age-specific incidence seems to be declining in several countries. (24) The ways in which vascular risk factors could affect Alzheimer's disease (AD) are still not fully understood, especially since there are only a handful of epidemiological studies that have confirmed diagnoses through pathology. It's possible that these vascular risk factors heighten the risk of clinical AD by creating a ‘double-hit’ effect, where cerebrovascular damage compounds the issue, or that vascular damage might directly contribute to the development of AD pathology (27).
People who have first-degree relatives with Alzheimer's disease (AD) face a greater lifetime risk of developing the condition compared to the general population. This heightened risk is influenced by both genetic factors and other elements that contribute to the clustering of AD cases within families. We've looked into a bunch of other candidate genes that have variations influencing the risk of developing Alzheimer's disease. Other genes play a role in the development of this mental disorder as well. The apoE4 allele stands out as the only confirmed genetic factor linked to both early- and late-onset forms of Alzheimer's disease (AD). While this allele does increase the risk of developing AD, it's important to note that it's not the sole cause. Essentially, the more apoE4 alleles a person has, the greater their risk of AD and the earlier they might experience symptoms. Interestingly, the impact of the apoE4 allele on risk tends to lessen as people age (18).
Many epidemiological studies, including those quoted by Henderson, agree that of the various demographic factors such as age, gender, race and social class, age is one of the most important risk factors for cognitive decline and AD. With advancing age, the prevalence of AD increases to an estimated 19% in individuals 75-84 years of age and to 30-35%, possibly up to 50% for those older than 85 years. That AD could therefore be an accelerated form of normal aging is largely based on the observation that many of the patho logical changes identified in AD are similar, apart from their severity, to those present in normal aging. Hence, in cognitively normal brain, there is an age-related reduction in brain volume and weight, enlargement of ventricles, and loss of syn apses and dendrites in selected areas accompanied by SP and NFT. Hence, a cross-sectional study by Miller et al. investigated changes in density of SP and NFT with age in 199 individuals and observed from age 71, an abrupt increase in the numbers of both lesions. In addition, in 60 normal elderly cas es, 32/60 had no SP, although 30/60 were younger than 65 years, 13/60 had SP in the HC, and 12/60 had SP in temporal cortex. It was concluded that it was not possible to distinguish early AD from normal aging at post-mortem (19).
Recent studies have shown that both low and high body weight can raise the risk of cognitive impairment and Alzheimer's disease, suggesting a U-shaped relationship that varies depending on the age at which body weight is assessed. This relationship appears to be influenced by central obesity. Additionally, there's some evidence indicating that weight loss due to malnutrition in the years leading up to dementia onset may also play a role in this dynamic (20).
The connection between smoking and cognitive decline can partly be attributed to the vascular issues that smoking causes. However, newer research also points to neurotoxins found in cigarette smoke and tobacco, like certain metals and polycyclic aromatic hydrocarbons, as factors that heighten the risk of Alzheimer's disease and related disorders, along with increasing biomarkers associated with Alzheimer's. In a recent study involving 2,037 women aged 55 to 64 who had never smoked, researchers looked into passive smoking as a potential risk factor for these disorders. They discovered that for every additional year of exposure to second-hand smoke, there was a 0.01-point drop in memory scores during follow-up assessments (t score, −2.07; P < 0.05). Lastly, findings indicate that quitting smoking could help prevent cases of dementia, as the risk for those who have stopped smoking eventually aligns with that of individuals who have never smoked (22).
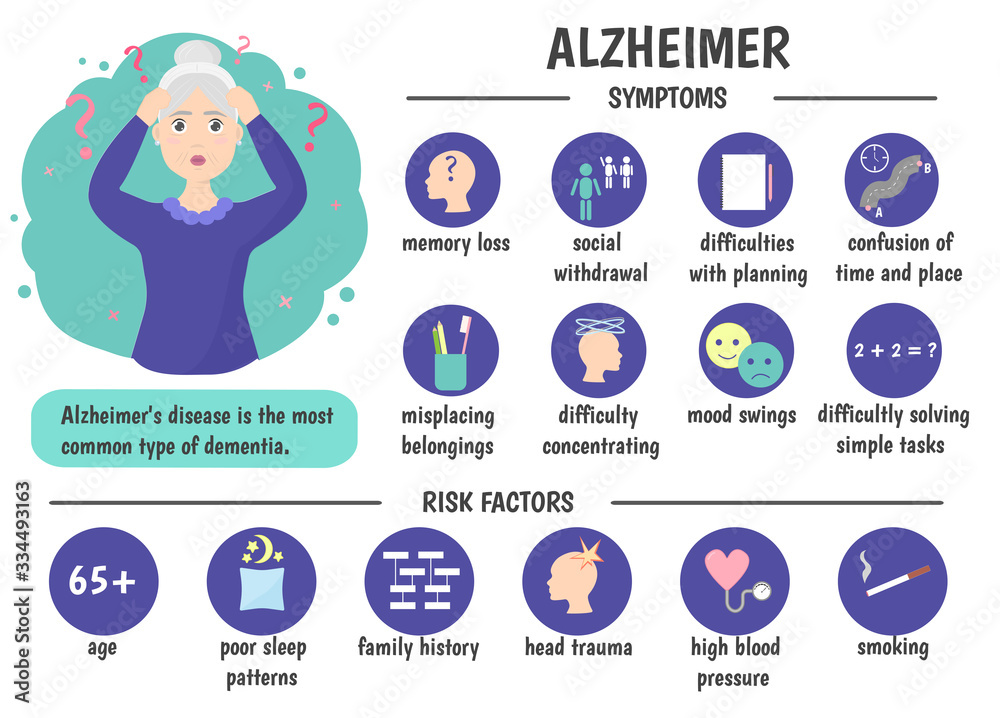
Fig.3: Symptoms of Older People
Hypertension, often seen as a risk factor for cardiovascular diseases, has been linked to dementia and Alzheimer's disease in various studies, but interestingly, this connection seems to depend on age. Research has shown that high blood pressure during midlife is associated with a greater risk of developing dementia or Alzheimer's later on. Even having high blood pressure in your later years might raise that risk, although some studies suggest the opposite could be true for older adults, possibly due to reverse causality. A recent study added weight to this idea, revealing that hypertension in midlife was connected to a thinner cortex in several brain regions, including the insular cortex, which plays a role in regulating blood pressure (23).
Research shows a significant connection between cardiovascular health and brain health in individuals with Alzheimer’s disease. Conditions like heart disease, high blood pressure, or high cholesterol can heighten the risk of developing Alzheimer’s. This happens because these issues can damage the blood vessels in the brain, leading to reduced blood flow and potentially severe brain cell death (24).
Vitamin D is created from 7-dehydrocholesterol in the skin through a photochemical reaction. This active form functions like a hormone, influencing various tissues beyond its well-known role in calcium and phosphate metabolism. To keep track of vitamin D3 levels in the body, we usually measure 25-hydroxy vitamin D3 in the serum. Vitamin D exhibits both genomic and non-genomic effects, which are mediated by nuclear and membrane receptors, respectively. Interestingly, the vitamin D reptor (VDR) is the same in both locations (25).
The connection between smoking and cognitive decline can partly be attributed to the vascular issues that smoking causes. However, newer research also points to neurotoxins found in cigarette smoke and tobacco, like certain metals and polycyclic aromatic hydrocarbons, as factors that heighten the risk of Alzheimer's disease and related disorders, along with increasing biomarkers associated with Alzheimer's. In a recent study involving 2,037 women aged 55 to 64 who had never smoked, researchers looked into passive smoking as a potential risk factor for these disorders. They discovered that for every additional year of exposure to second-hand smoke, there was a 0.01-point drop in memory scores during follow-up assessments (t score, −2.07; P < 0.05). Lastly, findings indicate that quitting smoking could help prevent cases of dementia, as the risk for those who have stopped smoking eventually aligns with that of individuals who have never smoked (21).
Pathophysiology of AD:
Neuronal loss or changes in structure can often be observed, especially in areas like the hippocampus, amygdala, entorhinal cortex, and the cortical association regions of the frontal, temporal, and parietal lobes. Additionally, this can also affect subcortical nuclei, including the noradrenergic locus coeruleus, and the cholinergic basal nucleus (1). Cell dysfunction and the death of neurons in specific nuclear groups that are crucial for maintaining certain neurotransmitter systems can result in deficits in acetylcholine, norepinephrine, and serotonin (26). Several criteria have been put forward for diagnosing Alzheimer's Disease (AD) pathologically. Early efforts that focused on either amyloid plaques or neurofibrillary tangles (NFT) faced challenges due to their low specificity and sensitivity. The previous pathological criteria for AD established by the National Institute on Aging and the Reagan Institute combined the CERAD neuritic plaque score with the Braak and Braak NFT staging, resulting in three diagnostic categories: high, intermediate, and low likelihood (27). Basic scientists refer to the preclinical stage of Alzheimer’s disease as the cellular phase. During this time, changes in neurons, microglia, and astroglia contribute to the slow and stealthy advancement of the disease, often before any cognitive decline is noticeable (28). There's a wealth of evidence highlighting the intricate nature and multiple causes of dementia overall. As a result, there's been a growing interest in understanding the complex interactions involved in Alzheimer's disease (30). The buildup of Aβ leads to the formation of τ-tangles, which can be found in areas like the locus coeruleus, as well as the transentorhinal and entorhinal regions of the brain. During this critical phase, the tangles begin to spread to the hippocampus and neocortex (31). The intricate interactions between various neurotransmitter systems play a crucial role in how we adapt and respond, whether in normal physiological situations or in the context of disease (32).
Human astrocytes are significantly larger and more intricate than their rodent counterparts, showcasing a fascinating diversity that varies by brain region. In humans, we identify four distinct types of glial fibrillar acidic protein (GFAP) expressing cells, while rodents have only two (panel 2). Both protoplasmic and fibrous astrocytes can be found in humans and rodents, but interlaminar and varicose-projection astrocytes are exclusive to humans (33).
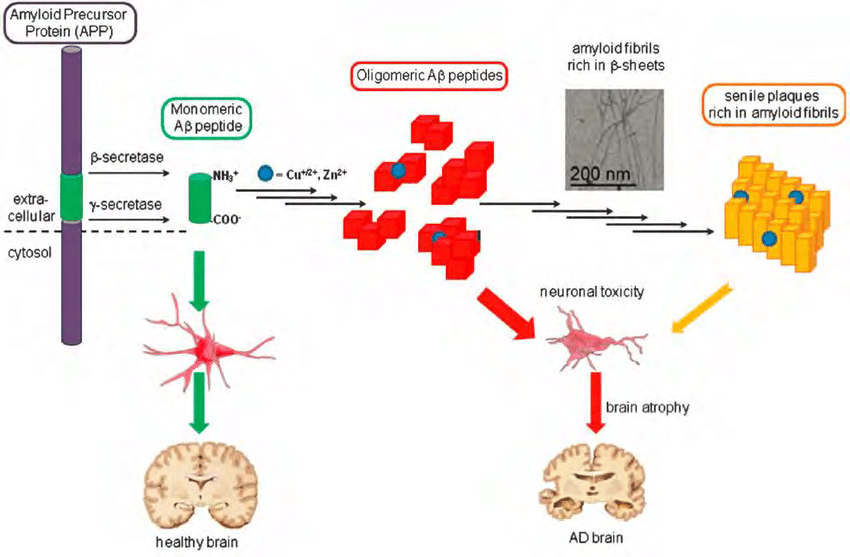
Fig.4: Amyloid Cascade Hypothesis.
One common method used to create intestinal dysbiosis is by injecting broad-spectrum antibiotics. This practice diminishes both the diversity and the number of gut microbiota in experimental animals. Such an imbalance in the gut microbiota can lead to the formation of Aβ, as mentioned earlier, and may result in neurocognitive impairments that ultimately contribute to Alzheimer's disease (34).
Clinical Features:
The clinical diagnosis of Alzheimer’s disease follows a clear and logical path: first, the patient's history should include information from an informant; next, a mental state assessment should incorporate a validated cognitive function test; and finally, the physical examination should focus on vascular and neurological signs, supported by further investigations. Assessing dementia involves a two-step approach. Initially, it’s crucial to differentiate dementia syndromes from other conditions that can resemble them, like depression, delirium, and mild cognitive impairment. Once a dementia syndrome is identified, determining its subtype becomes essential, as it can influence the treatment options available (24). As the condition advances, cognitive challenges become increasingly severe and widespread, making it harder to carry out everyday activities (27). Patients with Alzheimer's disease often experience complex visual disturbances. These can include issues with constructional and visuoperceptual orientation, particularly when it comes to searching for objects—like distinguishing between the figure and the background—and navigating through familiar places (35). Genetic testing for patients who are experiencing early-onset dementia, especially those with a positive family history, can be incredibly helpful. It aids in pinpointing the specific mutations responsible, ensuring the right diagnosis is made, and ruling out other possible conditions (36). When it comes to understanding dementia, it's important to recognize that other neuro-pathological changes can present symptoms similar to those seen in Alzheimer's disease (AD). That's why one of the key goals of a dementia clinical evaluation is to figure out if the dementia syndrome we're observing is actually caused by Alzheimer's neuropathology or if it's due to other factors like strokes, Lewy bodies, or even depression. To make this determination, healthcare professionals rely on a combination of clinical history, physical exams, and laboratory tests to rule out other degenerative conditions (37). The earliest age at which symptoms show up for PSEN1 mutations has been noted; typically, they start appearing between 30 and 50 years old, although some mutations can lead to symptoms emerging even earlier (38). Participants underwent in-person evaluations conducted by a neurologist or geriatrician who is either board-certified or board-eligible. Based on these assessments, participants were categorized regarding Alzheimer's Disease (AD) and other prevalent neurological disorders that may lead to cognitive impairment. This classification followed the guidelines set by the joint working group of the National Institute of Neurological and Communicative Disorders and Stroke, along with the Alzheimer’s Disease and Related Disorders Association (39). The goal of a clinical evaluation is to figure out whether the dementia symptoms we see are caused by Alzheimer’s disease or if they stem from something else, like strokes, Lewy bodies, or even depression. To get to the bottom of this, we rely on a combination of clinical history, physical exams, and lab tests to check if another degenerative, psychiatric, or medical condition might be behind the dementia symptoms. Research shows that Alzheimer’s disease is the most common type of pathology found in people with dementia (40). When we look at it broadly, the way monogenic Alzheimer's disease (AD) presents clinically is quite similar to sporadic AD. That said, the range of symptoms linked to monogenic AD tends to be a bit wider than what we usually observe in sporadic cases (38). After pinpointing the clinical practice guidelines, we gathered recommendations for screening, testing, diagnosing, treating, and monitoring Mild Cognitive Impairment (MCI) related to Alzheimer's Disease (AD) and Alzheimer's dementia. One researcher took the lead on data extraction, while another double-checked all the information against the original sources to maintain quality control. The recommendations we focused on were specifically aimed at identifying and treating individuals with cognitive impairments or dementia linked to Alzheimer's, rather than those that looked into other potential causes of cognitive decline or dementia (41). Some drugs have moved into the crucial phase III trial for Alzheimer's Disease (AD) with significantly less efficacy testing than what is typically expected. Among these are drugs that were originally approved for other conditions and later repurposed for AD treatment. For these products, safety was already established, at least for the doses used in their original approvals. However, the evidence supporting their effectiveness for treating AD usually comes from epidemiological studies and a limited number of clinical trials (42). When it comes to sample sizes, they tend to grow with the square of the standard deviation of how measurements change within the relevant clinical group. This means that achieving precision and minimizing variance are crucial if we want to keep sample sizes manageable. In clinical trials, it's important for markers to be sensitive to changes, but they also need to have strong biological relevance and connect to the key clinical or biological aspects of the disease (44). Clinical trials aimed at early or preventive interventions based on the amyloid/tau theory, as well as those focusing on other pathophysiologies, are currently underway or have recently started. A significant number of these ongoing clinical trials for Alzheimer's Disease (AD) are centered around disease-modifying therapies (DMTs) that address the underlying causes and have the potential to alter the progression of AD (46).
Table .1: Stages wise clinical Features Table.
|
Stages |
Cognitive Features |
|
Recent memory loss, word-finding difficulty, disorientation. |
|
Severe memory loss, language impairment, confusion. |
|
Profound memory loss, loss of recognition mutism. |
Table.2: Progression Timeline Table.
|
Time Course |
Key Clinical Features |
|
Mild forgetfulness, trouble with names, subtle personality changes. |
|
Moderate memory impairment, confusion difficulty with daily activities. |
|
Severe cognitive decline, loss of speech, bedridden state. |
Diagnosis:
The way we diagnose Alzheimer’s disease has really evolved over time. Back in the days of Alois Alzheimer (1864–1915), it was all about looking at the pathology. Fast forward to 1984, and we shifted to a more clinical, exclusionary method. This new approach was based on the criteria set by the National Institute of Neurological and Communicative Disorders and Stroke, along with the Alzheimer’s Disease and Related Disorders Association (28). The activation of the complement cascade, which plays a crucial role in our innate immune system, serves two important purposes. On one hand, it helps eliminate unsuitable synapses during development, and on the other hand, it contributes to the overall functioning of the immune response (29). To be diagnosed with Alzheimer’s dementia, a patient needs to meet the criteria for all-cause dementia. This means they must show neuropsychiatric symptoms that disrupt their ability to function socially or at work, indicate a decline from their previous level of functioning, cannot be attributed to delirium or another mental health issue, and must show signs of cognitive impairment (50). The “suggestive” clinical syndrome usually shows a significant decline in episodic memory, but it can also present other patterns, like visuo-spatial impairment. These variations can indicate underlying Alzheimer's disease (AD) pathology and align with a diagnosis of mild cognitive impairment due to Alzheimer's (MCI-AD) (51). Diagnosing Alzheimer's Disease (AD) can be quite challenging, especially in older adults who often have other health issues that can affect their cognitive abilities. Another complicating factor is the lack of awareness about the patient’s previous cognitive state, which makes it tough for doctors to accurately assess whether there has been any decline in their mental and functional capabilities (52). Taking care of cardiovascular risk factors plays a crucial role in maintaining brain health, especially when it comes to both cerebrovascular and neurodegenerative diseases (53). Alois Alzheimer first identified the neurodegenerative disease that now carries his name over a century ago. Even today, the key characteristics he noted—amyloid plaques and neurofibrillary tangles—are still essential for diagnosing the condition (54). Diagnosing Alzheimer's Disease (AD) is more about including potential cases rather than excluding them. Typically, we can rely on standardized clinical criteria to make this diagnosis. It's important to look into any potentially reversible causes of dementia as well. The good news is that AD can be diagnosed accurately, even in individuals with very mild impairments. However, it's concerning that only about 60% of patients with AD receive the correct diagnosis, and of those, only around 50% actually get treated. This trend holds true across all stages of the disease (59).
When it comes to diagnosing individuals with cognitive complaints, getting it right is crucial. Whether it's a patient, a family member, or a healthcare professional who raises concerns about cognitive decline, addressing these issues is key to providing the best care for those experiencing cognitive impairment. While awareness of dementia has certainly grown among primary care and specialist providers, there's still a pressing need to recognize the early signs of cognitive issues in clinical settings. The diagnostic journey kicks off with assessing the presence and severity of cognitive impairment. Gathering insights from someone who knows the patient well, along with a thorough cognitive evaluation conducted by a skilled clinician, forms the backbone of an accurate diagnosis. Neuropsychological testing can also play a vital role, especially for mild or high-functioning patients, as it helps pinpoint the severity of cognitive impairment and identifies which cognitive areas are affected. This information can be invaluable for clinicians when predicting outcomes and considering potential underlying causes. Once a preliminary diagnosis is made, it can be validated with biomarkers. While technology can certainly aid in the diagnostic process, the real art of diagnosis lies in the clinician's ability to weave together information from the informant, the mental status exam, the neurological exam, and any technological insights. If cognitive impairment is confirmed, a provisional assessment of the underlying cause is made, drawing from the patient's history, insights from the informant, the mental status exam (and sometimes neuropsychological testing), as well as the broader neurological examination (55). Getting an early diagnosis of Alzheimer's Disease (AD) is crucial for ensuring that patients can maintain a good quality of life. To achieve this, we rely on the criteria set out in the Diagnostic and Statistical Manual of Mental Disorders (DSM IV) along with the standards established by the National Institute of Neurological and Communicative Disorders and Stroke (NINCDS) and the Alzheimer's Disease and Related Disorders Association (ADRDA). Various neuropsychological and psychometric tests are conducted to evaluate the cognitive functions of patients. Additionally, a range of tests including blood work, structural and functional neuroimaging, cerebrospinal fluid analysis, electroencephalograms (EEG), and evoked potentials are performed. Genetic studies also play a vital role as complementary tests, helping to create a more comprehensive diagnosis of the disease (56). To get a comprehensive understanding, it's important to gather a detailed medical, psychiatric, and substance use history. This helps identify other potential causes, like medication side effects, depression, alcohol or substance dependence, and delirium. Additionally, a thorough physical examination, including a complete neurological assessment, should be conducted to check for both acute and chronic illnesses, as well as any specific focal issues (57).
1. It should pinpoint a core aspect of the underlying processes that drive AD.
2. It needs to be validated in cases where AD has been confirmed through neuropathological examination.
3. The biomarker must be precise enough to catch AD early on and differentiate it from other types of dementia.
4. Its measurement should be reliable, easy to perform, minimally invasive, and cost-effective (58).
1. In the early days of Alzheimer's disease (AD) research, scientists used fMRI to explore how brain activation during tasks differed between AD patients and healthy older adults.
2. These studies highlighted several brain changes associated with AD that linked to functional impairments. For instance, Figure 4B shows a decrease in cortical activity when processing repeated face-name pairs, a typical fMRI image taken from AD patients compared to healthy controls.
3. Since memory loss is the most significant indicator of AD during its symptomatic phase, researchers often found reduced activation in the hippocampus or medial temporal lobe during memory tasks in patients with mild cognitive impairment (MCI) or AD.
4. Interestingly, the level of activation detected by fMRI in AD patients varied widely. Yet, there’s some evidence suggesting an increase in activation during the early stages of AD.
5. Longitudinal fMRI studies on older adults indicated that those with the highest initial hippocampal activations experienced the fastest declines in activation, along with increases in amyloid and tau proteins in the brain and activated pathways (60).
Current Treatment Approaches:
Alzheimer’s disease is the fourth largest cause of death for people over the age of 65 years. As depression is commonly seen in AD patients, dual inhibitors of AChE-SERT (serotonin transporters) would be a better therapeutic option. (8) It’s been quite a while since the FDA approved a new drug for Alzheimer’s disease—back in 2003, to be exact. And even though there have been numerous trials, there still aren’t any approved disease-modifying therapies (DMTs) for Alzheimer’s. In fact, over the past decade, more than 200 research projects have either failed or been abandoned (61). It's important to note that treating older animals, where amyloid formation and related issues were already significant, resulted in a noticeable reduction in AD-like neuropathologies. There's still a lot of work to be done to gain a deeper understanding of the methods involved. This, in turn, supports the idea that adjusting Aβ-peptide levels by inhibiting the processing of Alzheimer precursor protein (APP) or exploring other therapeutic strategies could lead to effective treatments for Alzheimer's disease (62). The current treatment approach for Alzheimer’s disease (AD) involves a combination of both pharmacological and non-pharmacological strategies aimed at slowing down the progressive loss of cognitive and functional abilities (63). These agents do offer some important symptomatic relief, but they really don’t do much for the underlying biology of Alzheimer’s disease, nor do they significantly affect how the disease progresses (64). Drugs like NSAIDs and glucocorticoid steroids have been the focus of various studies (65). One significant issue with the lack of a specific treatment for the underlying condition is that the pathological changes associated with Alzheimer's disease start to develop quite early—often nearly a decade before any symptoms actually appear (66). There’s another type of FDA-approved medication that works by blocking NMDAR. In Alzheimer’s disease, damaged cells release too much glutamate, which leads to a huge influx of calcium into the neurons when NMDAR is activated. This process causes excitotoxicity and ultimately results in the death of neurons. Memantine is one such medication that helps manage this issue (67). Right now, we're focusing on two main areas: creating therapies that can modify the disease's progression and developing drugs that can block the pathways involved in the disease (68). These last two examples really highlight the growing trend of drug repurposing that we've already discussed (69). One area of research that still needs validation is the development of Aβ vaccines. While some agents have already progressed to phase II and III clinical trials, the most extensively studied method involves immunotherapy that utilizes Aβ antibodies (70) The current approach to treating Alzheimer's disease focuses on a comprehensive management of symptoms. The goal is to maintain a good quality of life, lessen the impact of the illness, and slow down any long-term decline in health (78). Starting CI treatment early in the course of Alzheimer's Disease (AD) is the way to go. A year-long study looked at how effective rivastigmine is for patients with mild to moderately severe AD. It found that those who began the treatment six months after their diagnosis had poorer cognitive performance compared to those who started right after being diagnosed (79). It looks like this new approach to the problem leans more towards the technical and mathematical side rather than the biological aspect. This raises a red flag about whether the clinical endpoints chosen for the trials might be a bit too early. Plus, the differences in diagnostic markers and endpoints could lead to some pretty inaccurate diagnoses of patients' disease states, which is definitely a source of error we need to watch out for (81). Neuroinflammation has been shown to play a crucial role in the pathological process of Alzheimer's disease. In particular, microglia are recognized as key players in orchestrating inflammation (82). There's a noticeable gap in proof that these methods actually protect human brains; the data we do have from animal studies suggests that this way of working is the most likely explanation (83). These medications can only help manage the symptoms of Alzheimer's disease and slow down its progression (84). Recent breakthroughs in pharmacology have mostly focused on creating cholinesterase inhibitors (85).
Future perspective:
In developed countries, the rising number of patients with Alzheimer's Disease (AD) has become a significant concern. Thanks to advanced diagnostic methods like imaging tests and cerebrospinal fluid biomarkers, the precision of diagnosing AD in clinical environments has seen remarkable improvements (71). When it comes to classifying data related to dementia, there are several categories or targets to consider. One key target is the comparison between Mild Cognitive Impairment (MCI) and Alzheimer's Disease (AD), which plays a crucial role in the early diagnosis of AD. This gap definitely needs attention in future studies to enhance early detection of AD. Additionally, other comparisons like MCIc versus MCInc and MCIc versus MCIs have also received limited coverage in the literature. Therefore, researchers should consider diving into these specific areas to improve early detection of dementia linked to Alzheimer’s disease (72). Alzheimer’s disease (AD) is a complex condition that arises from multiple factors, including the buildup of misfolded proteins, inflammation in the brain, the loss of nerve cells, and issues with insulin regulation. One promising approach to tackle this is drug repositioning, which could prove to be an effective strategy (73). The integration of complementary and alternative therapies is becoming more common in mainstream medical education, research, and practice. When it comes to treating patients with Alzheimer’s disease, it’s essential to have thoughtful discussions with patients and engage in shared decision-making. Ultimately, the choice to use these therapies should rest with the patient and their caregivers (74). Growth factors (GFs) are another group of molecules that might help enhance the pathology of Alzheimer's disease (75). Taking all this into account, Elan and several other companies have kicked off new trials that are currently in progress, focusing on passive or safer active immunization for patients dealing with Alzheimer's disease (AD)(76). Agents known as DMTs are thought to influence the underlying mechanisms of Alzheimer's disease, particularly concerning Aβ and tau. If they prove effective, these agents could potentially slow down the progression of the disease, leading to long-term benefits that might be seen clinically over several months or even years, ultimately reducing the rate of decline (78). A balanced diet can definitely boost your chances of avoiding Alzheimer's disease. That said, relying solely on the Mediterranean diet, cutting calories, or following an antioxidant-rich diet won't guarantee that you'll prevent or slow down the onset of Alzheimer’s (80).
CONCLUSION:
Alzheimer's disease is the leading cause of dementia and is expected to impact an increasing number of individuals as the US population continues to age. It's now evident that Alzheimer's can be both diagnosed and treated. Since most patients with Alzheimer's receive care in primary settings, it's crucial for primary care providers to accurately identify and effectively manage this condition. It's essential to carefully identify the target symptoms and understand their consequences. We should start with initial trials of non-pharmacological approaches and opt for the least harmful medication for the shortest time possible. These principles should guide us in managing agitation and aggression in individuals with dementia. Severe Alzheimer’s disease poses a significant challenge for society due to its widespread impact, high costs, and the emotional toll it takes on both patients and their caregivers. The recommendations from the Third Canadian Consensus Conference on the Diagnosis and Treatment of Dementia, grounded in the best available evidence, have the potential to enhance the quality of life for patients in this advanced stage of the disease, as well as for those caring for them. Ultimately, finding an effective therapy that modifies the disease in its earlier stages could help prevent the need for treatment during the severe phase. More research is essential to improve the care for those affected by this heartbreaking condition.
REFERENCES


Kajal Dhum*, Dr. Sonali Uppalwar, Neuroprotective Agents in the Management of Alzheimer’s Disease, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 3303-3321. https://doi.org/10.5281/zenodo.18015044
 10.5281/zenodo.18015044
10.5281/zenodo.18015044
