Senghundhar College of Pharmacy, Kumaramangalam, Tiruchengode-637 205, Namakkal
Fungal skin infections are among the most common infectious diseases worldwide, particularly in tropical and subtropical regions, and are caused mainly by dermatophytes, yeasts, and non-dermatophyte molds. Increasing resistance to commonly used antifungal agents, such as terbinafine-resistant Trichophyton indotineae, along with drug-related adverse effects, has created an urgent need for alternative and adjunct therapeutic options. In recent years, natural remedies and plant-derived products have gained attention due to their traditional use, accessibility, and reported antifungal properties. This review provides an overview of common superficial fungal skin infections, including tinea corporis, tinea pedis, tinea capitis, cutaneous candidiasis, pityriasis versicolor, and onychomycosis, along with their causative organisms and conventional treatments. It also summarizes published evidence on natural remedies such as neem, turmeric, garlic, tea tree oil, coconut oil, and other medicinal plants, highlighting their proposed mechanisms of antifungal action based on in vitro and limited clinical studies. Furthermore, the review discusses current challenges in antifungal therapy, including emerging resistance and treatment failures, and outlines future directions for integrating phytomedicine with conventional dermatological practice. Overall, this article aims to critically summarize existing literature on natural and synthetic antifungal agents for skin infections and to identify gaps that require further clinical investigation.
1.1 Fungi:
Fungi are a large group of eukaryotic organisms that include Molds, yeasts, mushrooms, and more. They are not plants, so they don’t have a single "botanical name" like plants do, but here are some examples of fungi with their scientific names:
The scientific term for fungi is Eumycota, also known as true fungi or Eumycetes.
Ringworm (skin infection) Trichophyton rubrum, Microsporum spp. Dermatophyte fungi
Candida (yeast infection) Candida albicans Yeast (Ascomycota)
Penicillin Mold Penicillium notatum or Penicillium chrysogenum Ascomycete fungus
Decomposition
Nutrient cycling
Symbiotic relationships (e.g., mycorrhizae, lichen)
Examples of fungi include:
Mushrooms
Molds
Yeasts
Lichens
Fungi can be beneficial (e.g., food, medicine) or harmful (e.g., causing diseases in plants, animals, and humans) (Levetin E et al., 2015).
1.2 Fungal Infection:
A fungal infection is a condition caused by the growth and spread of fungi, which are microorganisms that can infect various parts of the body, such as the skin, nails, lungs, or internal organs.Fungal infections can range from mild and superficial (e.g., athlete's foot, ringworm) to severe and lifethreatening (e.g., invasive aspergillosis, cryptococcosis) (Pujalt et al., 2015).


Fig. No 1.1: Fungal Infection
Out of the estimated 50,000 to 250,000 known fungal species, fewer than 500 are linked to human disease, and only about 100 can infect healthy individuals. Most fungi cause illness only in those who are immunocompromised or weakened. Typically, these fungi live freely in the environment and do not rely on humans or animals for survival. Human infections usually arise from environmental sources and are acquired through inhalation, ingestion, or traumatic implantation (Thambugala, K.M et al., 2024).
Humans generally coexist peacefully with the vast array of microorganisms in their environment. However, when the immune system is compromised or when pathogens accumulate to unusually high levels, infections can develop. While many infections go unnoticed, there are instances where the invading organisms trigger the body's immune response, resulting in visible signs and symptoms—this condition is referred to as an infectious disease (Wisplinghoff H et al., 2003).
1.3 Types Of Fungal Infections:
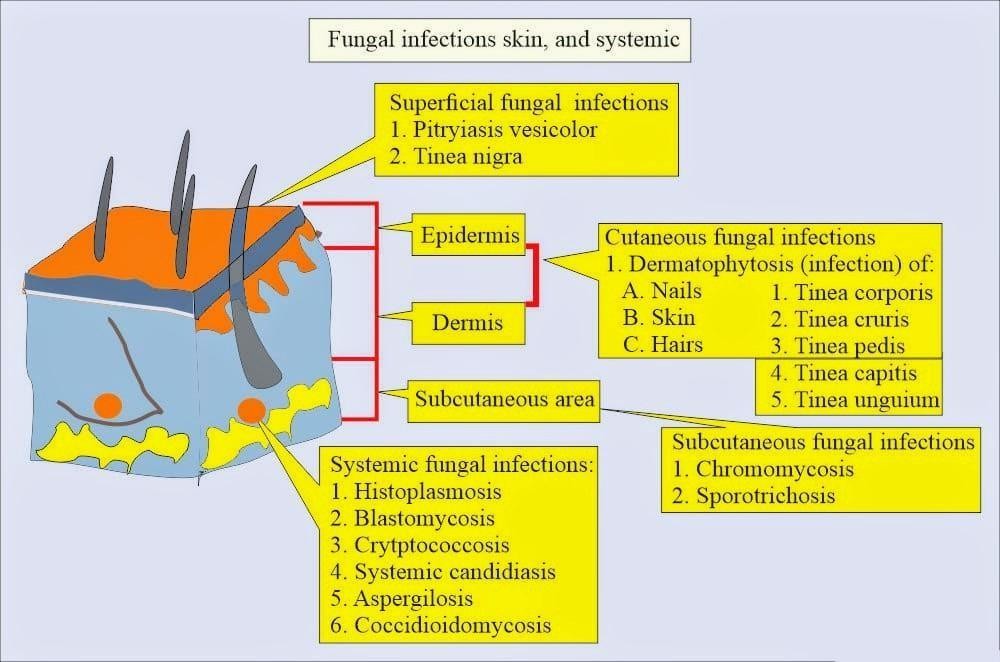
Fig. No 1.2: Fungal Infection Types
1.Superficial Fungal Infections:
Dermatophytosis (Ringworm): A fungal infection that affects the skin, hair, and nails, often causing itchy, red, and scaly patches.
Candidiasis (Yeast Infection): Caused by Candida fungi, it can affect the skin, mucous membranes (oral, genital), and nails.
Tinea Pedis (Athlete's Foot): A fungal infection that affects the skin on the feet, often causing itching, cracking, and scaling.
Pityriasis Versicolor: A superficial skin infection that causes discoloured patches, typically on the chest, back, and shoulders (Nobile CJ et al., 2015).
2.Subcutaneous Fungal Infections:
Sporotrichosis: A subcutaneous fungal infection caused by the fungus Sporothrix schenkii, often acquired through a skin wound.
Chromoblastomycosis: A chronic, localized infection of the skin and subcutaneous tissue caused by certain types of fungi (Bonifaz A et al., 2010).
3.Systemic Fungal Infections:
Aspergillosis: A lung infection caused by Aspergillus fungi, which can spread to other parts of the body.
Cryptococcosis: A fungal infection that can affect the lungs, brain, and other organs.
Histoplasmosis: A lung infection caused by Histoplasma fungi, often spread through bird and bat droppings.
Coccidioidomycosis (Valley Fever): A lung infection caused by Coccidioides fungi, common in certain regions of the United States (Galimberti R et al., 2012).
Other Types of Fungal Infections:
Invasive Candidiasis: A serious infection caused by Candida fungi, often in individuals with weakened immune systems.
Pneumocystis Pneumonia: A serious lung infection caused by the fungus Pneumocystis jirovecii, primarily affecting people with weakened immune systems.
Mucormycosis: A rare but serious fungal infection caused by mucormycetes fungi, often affecting people with diabetes or weakened immune systems (Perfect, J.R et al., 2017).
1.4 Antifungal:
Antifungal agents are drugs used to treat fungal infections by inhibiting fungal growth or killing fungi.Most antifungal drugs target cell wall or membrane metabolism, but many are limited by low effectiveness and high toxicity. Rising resistance further complicates treatment. Consequently, there exists a substantial demand for novel antifungal compounds characterized by reduced toxicity and enhanced efficacy."Sordarins are recognized as highly effective agents in antifungal treatment, and disturbing the protein synthesis. They accomplish this by selectively binding to fungal elongation factor 2 (EF2), thereby interfering with the translocation step involved in protein production (Shao Y et al., 2022).
1.5 Mechanism Of Action:
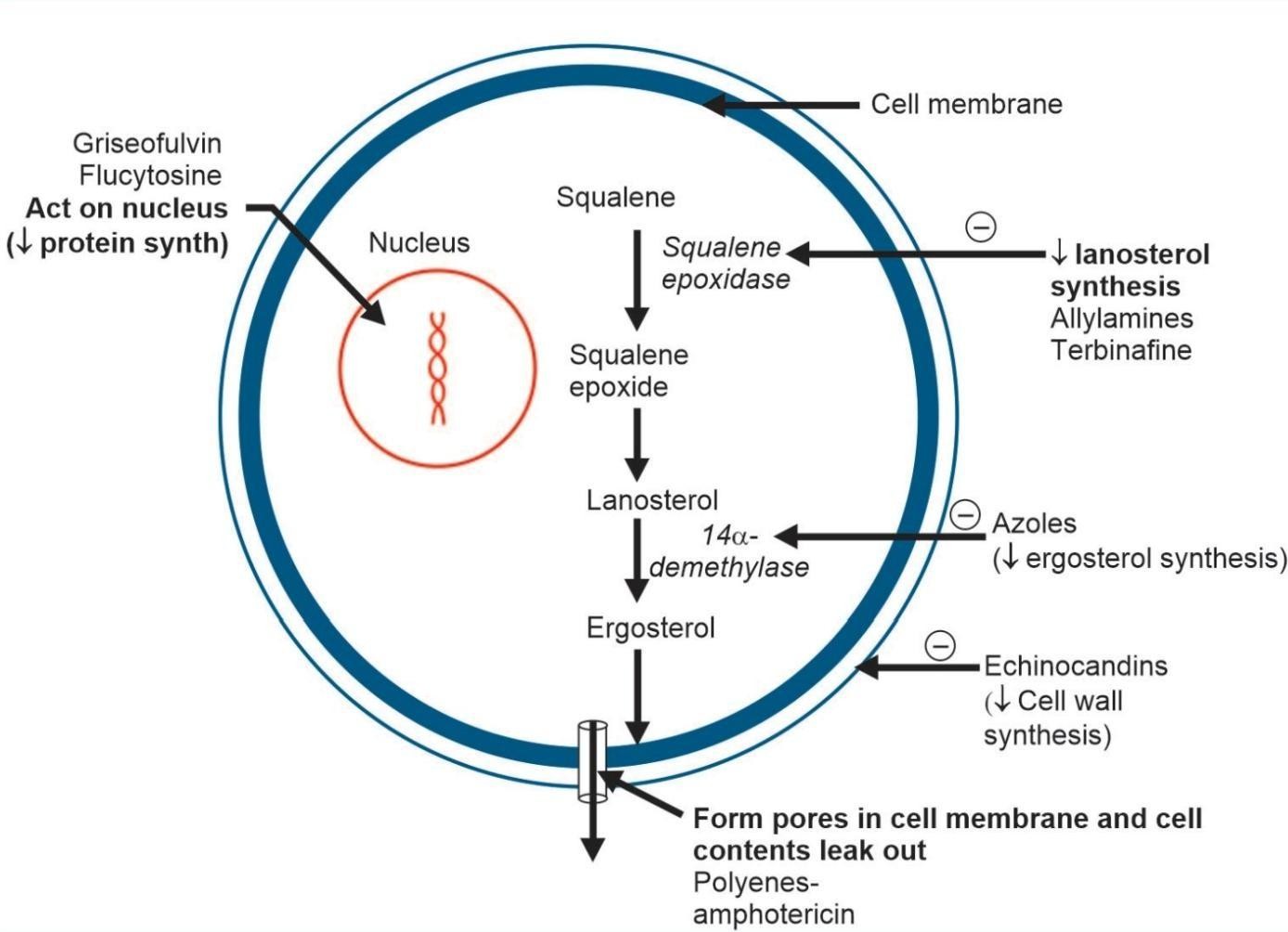
Fig. No 1.3: Mechanism of Action
II. AIM AND OBJECTIVES
AIM
To review published literature on fungal skin infections, conventional antifungal drugs, and natural remedies, with focus on treatment challenges and emerging resistance.
OBJECTIVES
To summarize common fungal skin infections and their causative organisms.
To outline available synthetic antifungal drugs and their mechanisms.
To review natural remedies with reported antifungal activity from literature.
To compare evidence for herbal and synthetic treatments.
To highlight antifungal resistance and future research needs.
III. BACKGROUND OF THE STUDY
Fungal infections, or mycoses, are caused by pathogenic fungi that can affect humans, animals, and plants. Common pathogens include Candida, Aspergillus, Cryptococcus, and dermatophytes, causing conditions from mild skin infections to life-threatening systemic diseases. The prevalence of fungal infections has risen due to immunocompromised populations, poor hygiene, tropical climates, and misuse of antimicrobials.In developing countries like India, these infections are often underdiagnosed and undertreated due to limited awareness, diagnostic challenges, and antifungal resistance. The toxicity of some drugs further complicates treatment.This has led to growing interest in natural antifungal agents from medicinal plants, which offer bioactive compounds with safer, sustainable therapeutic potential. This study explores fungal infections, their challenges, and potential plant-based antifungal alternatives to improve healthcare outcomes.
4.1 Sources of Literature
Relevant literature was collected from electronic databases including PubMed, Google Scholar, and Science Direct. Additional articles were identified through manual screening of reference lists from selected publications.
4.2 Search Strategy
The literature search was performed using combinations of keywords such as fungal skin infections, dermatophytosis, tinea corporis, tinea pedis, cutaneous candidiasis, onychomycosis, antifungal drugs, terbinafine resistance, Trichophyton indotineae, herbal antifungal agents, medicinal plants, and phytotherapy.
4.3 Inclusion and Exclusion Criteria
Articles published in English between 2010 and 2024 were included. Original research articles, clinical studies, and review articles related to superficial fungal infections and plant-based antifungal agents were considered. Studies focusing exclusively on systemic fungal infections, non-cutaneous diseases, or unrelated microorganisms were excluded.
4.4 Data Collection and Organization
Relevant information regarding causative organisms, clinical features, treatment options, antifungal mechanisms, resistance patterns, and reported efficacy of natural remedies was extracted from selected articles. The collected data were organized into thematic sections covering different types of fungal skin infections and corresponding therapeutic approaches.
4.5 Data Analysis
A qualitative analysis of the selected literature was performed to compare findings across studies. Laboratory-based evidence was distinguished from clinical outcomes to avoid overestimation of therapeutic effectiveness. Emphasis was placed on identifying consistent trends, treatment limitations, and gaps in current research.
4.6 Ethical Considerations
As this study was based solely on published data and did not involve human participants, animals, or biological specimens, ethical approval was not required.
VI. OVERVIEW OF COMMON FUNGAL SKIN INFECTIONS AND TREATMENTS
Superficial fungal infections affect keratinized tissues such as the skin, hair, and nails and are mainly caused by dermatophytes, yeasts, and non-dermatophyte molds. These infections are widely prevalent in tropical and subtropical regions and are associated with environmental, socioeconomic, and host-related risk factors. The major clinical types, their causative organisms, and treatment options are summarized below.
6.1 Tinea Corporis (Ringworm of the Body)
Tinea corporis is a superficial dermatophyte infection characterized by annular, erythematous, scaly lesions with central clearing and raised borders. It commonly affects the trunk, neck, and limbs and is more prevalent in warm and humid climates. (Satchell AC et al., 2002).
Causative Organisms:
Trichophyton rubrum, Microsporum canis, and Epidermophyton floccosum are the most common etiological agents(Hay RJ & Jones TC et al., 2001)..
Treatment:
Topical antifungals such as clotrimazole, miconazole, and terbinafine are first-line therapies for localized infections, usually applied for 2–4 weeks. Oral antifungals including terbinafine, itraconazole, or fluconazole are recommended for extensive, recurrent, or steroid-modified infection (Sharma M & Sharma N et al., 2012).
Natural remedies such as neem, turmeric, garlic, and tea tree oil have shown antifungal activity in laboratory studies, but clinical evidence remains limited.

Fig. No 6.1: Tinea Corporis (Ringworm of the body)
6.2 Tinea Pedis (Athlete’s Foot)
Tinea pedis is a common fungal infection of the feet, especially between the toes, and is associated with excessive sweating and occlusive footwear. (Sharma M, Sharma N et al., 2012).
Causative Organisms:
Trichophyton rubrum, Trichophyton interdigitale, and Epidermophyton floccosum.
Treatment:
Topical allylamines and azoles are effective for most cases, while oral therapy is reserved for chronic or widespread disease.
Herbal agents such as tea tree oil, garlic extract, and lemongrass oil have demonstrated antifungal effects in vitro and in small clinical studies.

Fig. No 6.2: Tinea Pedis (Athlete’s Foot)
6.3 Tinea Capitis (Scalp Ringworm)
Tinea capitis is predominantly seen in children and spreads easily in crowded environments through direct contact or contaminated fomites. (Coulibaly O et al.,2018).
Causative Organisms:
Trichophyton tonsurans, Microsporum audouinii, and Microsporum canis.
Treatment:
Systemic antifungal therapy is required, commonly with griseofulvin or terbinafine for 6–8 weeks. Topical agents are used only as adjuncts to reduce surface fungal load.
Traditional remedies such as coconut oil, neem, and henna are used in some communities, but reliable clinical data are lacking.
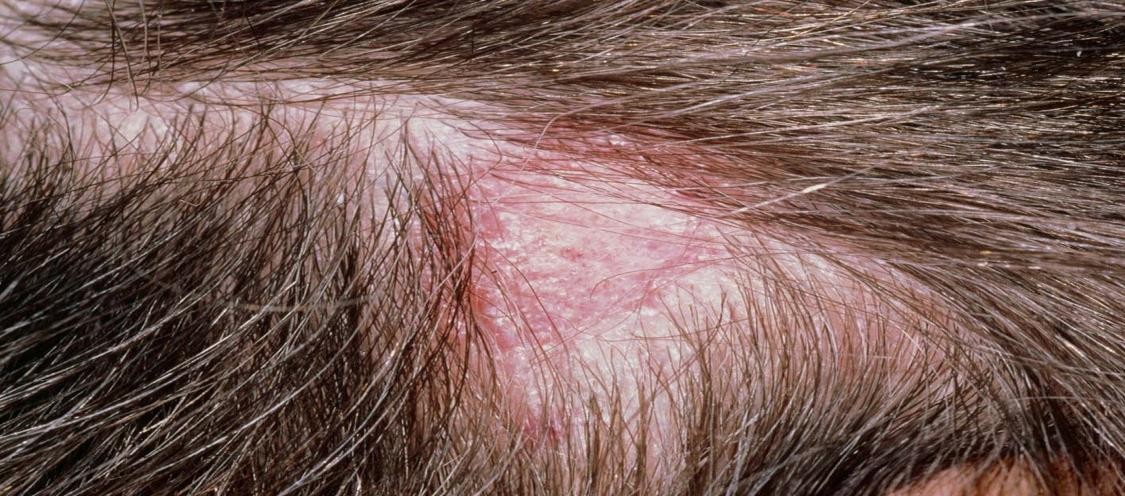
Fig. No 6.3: Tinea Capitis (Scalp Ringworm)
6.4 Cutaneous Candidiasis
Cutaneous candidiasis affects moist skin folds and mucosal areas, particularly in diabetics, infants, obese individuals, and immunocompromised patients. (Silva S et al., 2012).Causative Organisms:Candida albicans is the mostcommon species, followed by C. glabrata and C. tropicalis.
Treatment:
Topical azoles and nystatin are commonly used, while oral fluconazole is reserved for recurrent or extensive cases.
Natural products such as clove oil, cinnamon extract, and garlic have shown anti-Candida activity in laboratory studies, but standardized clinical formulations are not well established.

Fig. No 6.4: Cutaneous Candidiasis
6.5 Pityriasis Versicolor (Tinea Versicolor)
Pityriasis versicolor is caused by overgrowth of lipophilic yeasts that are part of the normal skin flora and is characterized by hypo- or hyperpigmented scaly patches. (Ravindran R et al., 2018).
Causative Organisms:
Malassezia furfur and related species.
Treatment:
Topical ketoconazole, selenium sulfide, and zinc pyrithione shampoos are effective. Oral azoles may be required in recurrent cases.
Herbal preparations such as aloe vera, green tea, and basil oil are traditionally used, though clinical validation is limited.
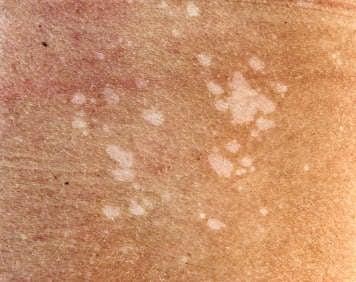
Fig. No 6.5: Pityriasis Versicolor (Tinea Versicolor)
6.6 Onychomycosis (Nail Fungal Infection)
Onychomycosis is a chronic infection of the nail unit that is difficult to treat and associated with high relapse rates. (Pinto E et al., 2009).
Causative Organisms:
Trichophyton rubrum, T. mentagrophytes, Candida species, and non-dermatophyte molds.
Treatment:
Oral terbinafine and itraconazole are the most effective treatments, while topical agents such as ciclopirox and efinaconazole are used in mild cases.Essential oils such as tea tree and oregano oil have demonstrated antifungal activity, but their penetration into the nail plate and long-term efficacy remain uncertain.
Bottom of Form

Fig. No 6.6: Onychomycosis (Nail Fungal Infection)
VII. CURRENT STATUS AND FUTURE PERSPECTIVES
Current Status
Superficial fungal skin infections are highly prevalent worldwide, especially in tropical regions, and are mainly caused by dermatophytes, Candida, and Malassezia species. Although azoles and allylamines are effective treatments, increasing cases of treatment failure and recurrence are being reported. The emergence of terbinafine-resistant strains, particularly Trichophyton indotineae associated with SQLE gene mutations, has become a major clinical challenge. Misuse of topical steroid combinations, poor treatment adherence, and limited diagnostic facilities further contribute to persistent infections.
FUTURE PERSPECTIVES
Future strategies should focus on resistance surveillance, development of new antifungal drugs with novel mechanisms, and improved topical drug delivery systems. Natural products remain a promising source of antifungal compounds, but their clinical usefulness requires proper standardization and controlled clinical trials. Public awareness, rational drug use, and early diagnosis are essential to reduce disease burden and prevent recurrence.
VIII. LIMITATIONS OF THE REVIEW
This review is based on a narrative literature search and not on a systematic review methodology, which may introduce selection bias. Most of the evidence supporting natural remedies is derived from in vitro studies, while well-designed clinical trials are limited, making it difficult to draw firm conclusions about clinical effectiveness. Variations in plant sources, extraction methods, and formulations across studies also affect result consistency and comparability. In addition, publication bias toward positive findings may overestimate the potential benefits of herbal antifungal agents.
IX SUMMARY AND CONCLUSION
Fungal skin infections remain highly prevalent worldwide and continue to pose significant clinical and public health challenges, particularly in tropical regions. Although conventional antifungal agents such as azoles and allylamines are generally effective, increasing treatment failures and emerging resistance, especially terbinafine-resistant Trichophyton species, have complicated disease management. Natural remedies and plant-derived products show promising antifungal activity in laboratory studies and limited clinical reports; however, strong clinical evidence supporting their routine therapeutic use is still insufficient. Therefore, natural products should be considered complementary to standard antifungal therapy rather than replacements. Future research should focus on standardized formulations, safety evaluation, and well-designed clinical trials to validate the clinical potential of herbal antifungal agents. Strengthening antifungal stewardship, improving patient awareness, and promoting rational drug use are essential to reduce recurrence and resistance.
REFERENCES

Dr. Astalakshmi N, Deepa S., Gokul V., Mayilvel S., Praveenkumar S., Ravindharan R., Sakthivel S., Sathishkumar G., Sona S. P., Vimalkumar V., Dr. Surendra Kumar M., Natural Remedies and Antifungal Agents for Skin Infections: An Overview, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 2255-2264. https://doi.org/10.5281/zenodo.18639519
 10.5281/zenodo.18639519
10.5281/zenodo.18639519
