Amrutvahini Institute of Pharmacy, Sangmner.
This review article highlights the formulation approaches of nanosuspensions for ophthalmic drug delivery, with the primary goal of enhancing the solubility and bioavailability of poorly soluble drugs. Recent progress in nanotechnology has significantly advanced the use of nanoscale systems to address limitations of conventional formulations. Nanosuspensions are particularly beneficial for Biopharmaceutical Classification System (BCS) Class II drugs, which exhibit low solubility yet high permeability. By reducing particle size, these systems improve dissolution, promote ocular absorption, and prolong drug retention at the target site. In addition to ocular use, nanosuspensions can be administered via oral, parenteral, and pulmonary routes, demonstrating their versatility. Various preparation techniques, such as wet milling, high-pressure homogenization, emulsion-solvent evaporation, melt emulsification, and supercritical fluid processing, have been developed to achieve stable formulations. Overall, nanosuspension technology offers a promising platform for efficient and sustained intraocular drug delivery, ultimately improving therapeutic outcomes and patient compliance.
Developing an ocular drug delivery system that can precisely target specific tissues of the eye continues to be a significant challenge in pharmaceutical sciences.Traditionally, eye drops remain the most common treatment for ocular disorders, particularly those affecting the anterior segment. While they are convenient to use and provide quick relief, their therapeutic efficiency is often compromised by physiological and anatomical barriers. Factors such as rapid tear turnover, blinking, reflex tearing, and drainage into the nasolacrimal duct drastically reduce the drug's residence time, resulting in poor bioavailability. Because of these limitations, conventional formulations fail to deliver adequate concentrations of drugs to deeper ocular tissues. To address these challenges, researchers have shifted their focus toward novel drug delivery systems (NDDS) such as nanosuspensions and nanoemulsions. These advanced approaches are designed to prolong drug retention at the target site, enhance corneal penetration, and enable controlled release, thereby offering improved treatment outcomes and patient compliance in the management of ocular diseases.
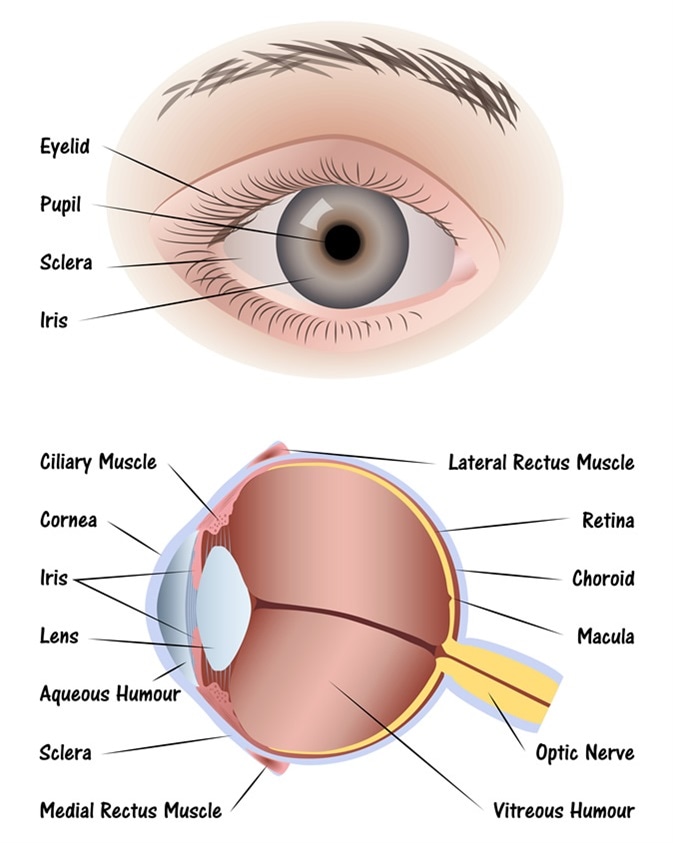
Fig. Anatomy of Eye.
Ocular Barriers and Routes of Administration
The eye is protected by several anatomical and physiological barriers that significantly restrict the penetration of drugs to their therapeutic targets (Fig. 1). Whether delivered through corneal or non-corneal pathways, drugs must undergo complex biological processes to cross these barriers and reach either the anterior or posterior chambers. Conventional eye drops are widely used, yet they are quickly washed away from the ocular surface by tear drainage and blinking. As a result, their bioavailability remains very low, with only about 1-7% of the applied dose able to reach the aqueous humor. This limitation makes it difficult for topically applied medications to achieve effective concentrations in the posterior segment of the eye.Several routes have been explored for ocular drug administration, including topical delivery, systemic (parenteral) injection, oral administration, and periocular or intravitreal injection. Among these, topical administration is the most preferred method because it is non-invasive, patient-friendly, and capable of directly targeting the anterior seg while bypassing first-pass metabolism.
Mechanisms of Topical Absorption
When drugs are placed in the conjunctival sac, absorption occurs primarily through two routes: the corneal and non-corneal pathways. The corneal route plays a dominant role, but its efficiency is limited due to the tight barrier function of the corneal epithelium. Alternatively, non-corneal absorption involves drug diffusion across the conjunctiva and sclera. In both cases, however, a considerable portion of the drug is removed by lacrimal fluid, further reducing its effective concentration at the target site.
Drug Absorption via Non-Corneal Pathways
In non-corneal routes, drug delivery to intraocular tissues is generally limited due to the presence of local capillary networks, which reduce the amount of drug reaching the target site. However, certain medications, such as gentamicin and timolol maleate, have successfully penetrated the intraocular space through diffusion across the conjunctiva and sclera. The efficiency of this absorption is largely determined by the drug's physicochemical properties, including solubility, molecular size, and lipophilicity.
Ophthalmic Formulations
Ophthalmic preparations are sterile dosage forms designed for application to the eye, and may be in liquid, semi-solid, or solid form. They usually contain one or more active pharmaceutical ingredients (APIs) dissolved or suspended in an aqueous medium. Excipients are carefully chosen to ensure that they do not compromise the stability of the formulation or the availability of the API at the site of action.
For multidose ophthalmic products, antimicrobial agents are added if the API does not possess inherent antimicrobial activity, and these agents must remain effective throughout the product's usage period. Oily eye drop formulations must use sterilized vehicles, commonly treated by heating at 160 °C for one hour. Ophthalmic products are formulated to be approximately isotonic with tear fluid, often using agents like sodium chloride. After opening, these products should be used within one month to maintain their safety and effectiveness.
Ophthalmic Dosage Forms
Ophthalmic dosage forms are specially formulated to deliver medication directly to the eye while ensuring safety, sterility, and effectiveness. The main types include:
1. Eye Drops (EDS)
a. Ophthalmic Solutions (OS)
These are sterile, clear liquid preparations free of any foreign particles, intended for direct eye application. Careful formulation is essential to ensure the drug is safe and comfortable for the eye, taking into account factors like drug toxicity, isotonicity, buffering agents, and preservatives.
Examples: Ketorolac tromethamine solution,
Levocabastine solution
b. Ophthalmic Suspensions (OSS)
Suspensions are sterile preparations in which tiny solid particles are dispersed throughout a liquid medium. The particles should be finely micronized to avoid corneal irritation or damage. Suspensions showing clumping or settling should not be administered.
Examples: Neomycin with Polymyxin B and Hydrocortisone suspensior Fluorometholone suspension
2.Eye Lotions (EL)
Eye lotions are aqueous formulations used primarily to cleanse the surface of the eye. They can also be applied to dressings placed over the eye and help relieve minor irritation or discomfort.
3. Eye Ointments (EO)
Ophthalmic ointments must be sterile. Compared to other eye medications like solutions or suspensions, achieving sterility in ointments can be more challenging. They can either be sterilized after preparation (terminal sterilization) or made aseptically using sterile ingredients in a Class A (highly controlled) environment. The ointment base should be non-irritating and allow the active drug to diffuse effectively throughout the eye's secretions. Ointments generally provide a longer contact time with the eye than solutions, often lasting 2-4 times longer
4. Ophthalmic Emulsions (OE)
Ophthalmic emulsions are preparations in which tiny oil droplets are dispersed within an aqueous phase. The formulation must remain stable, showing no signs of phase separation or coalescence.
Examples: Tromethamine eye emulsion, Cetalkonium chloride eye emulsion, Ciclosporin eye emulsion
5. Ocuserts
Ophthalmic inserts, also known as ocular systems, are solid dosage forms designed in suitable sizes and shapes for placement in the conjunctival fornix or the lacrimal punctum. Ocuserts can be classified as either soluble (erodible) or insoluble (non-erodible). These devices offer precise drug delivery, reduce or eliminate the need for preservatives, and can significantly improve ocular bioavailability.
For soluble inserts, drug release occurs in two stages:
1. Initial fast release: A portion of the drug is rapidly released as tear fluid penetrates the insert.
2. Sustained slow release: A gel layer forms on the surface of the insert, allowing gradual drug release over time.
Example: Hydroxypropyl celose ophthalmic
Novel Ophthalmic Dosage Forms
Colloidal Dosage Forms (CD)
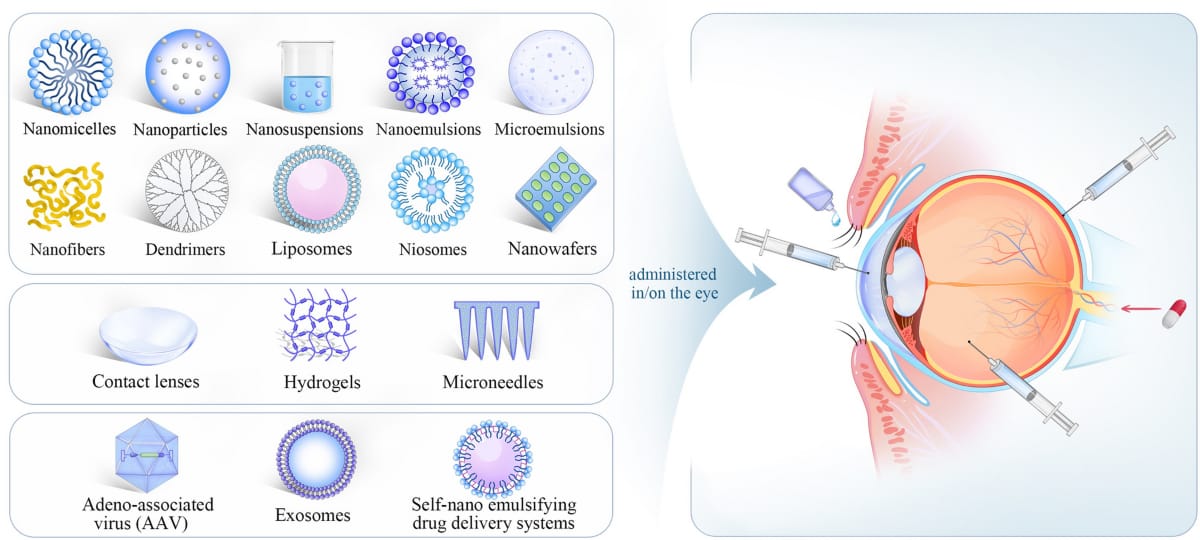
Colloidal dosage forms, such as liposomes, nanoparticles, microemulsions, and nanoemulsions, have been extensively explored in ocular drug delivery.
They offer several advantages:
a. Controlled and sustained drug release at the target site
b. Reduced dosing frequency
c. Ability to overcome the Blood-Ocular Barrier (BOB)
d. Enhanced drug stability and protection from degradation by ocular enzymes
Improved drug permeation across ocular membranes
Biodegradable colloidal carriers can serve as alternatives to non-biodegradable implants, which require surgical removal after a certain period .Despite their promise, commercial development of these systems is still limited due to manufacturing challenges, particularly maintaining stability during sterilization, which currently outweighs the pharmacokinetic and pharmacological benefits in many cases.
1.Microemulsions (ME)
Microemulsions are mixtures of water and oil, either as water-in-oil (W/O) or oil-in-water (O/W) systems, stabilized by a combination of surfactants and co-surfactants to lower interfacial tension. These systems are thermodynamically stable, have very small droplet sizes (typically around 100 nm), and appear clear and transparent. The transparency is due to the high degree of dispersion of the internal phase, with droplet sizes ranging from approximately 100 to 1000 angstroms.
Beyond improving drug solubility, microemulsions have been used to enhance drug permeation across the cornea. They can also provide sustained or extended drug release, which reduces the frequency of administration. However, microemulsions have certain limitations, including the careful selection required for the surfactant and co-surfactant system and the potential toxicity associated with high concentrations of these excipients.
The requirement for specific surfactant and co-surfactant combinations can limit the practical use of microemulsions, particularly due to concerns about toxicity or irritation at higher concentrations.
2.Nano Suspensions (NS)
Nano suspensions are sub-micron colloidal systems in which poorly water-soluble drugs are dispersed in an appropriate medium and stabilized using surfactants. These formulations often incorporate inert colloidal carriers, such as polymeric resins, which help improve drug solubility and bioavailability. Unlike microemulsions, nano suspensions are generally non-irritating to the eye. Additionally, the surface charge of the nanoparticles promotes adhesion to the corneal surface, enhancing drug retention and efficacy.
3.Nano Particles (NP)
Nanoparticles are particles with diameters smaller than 1 µm, composed of biodegradable or non-biodegradable polymers, lipids, phospholipids, or metals. They can be classified as:
a.Nanospheres (NS): the drug is uniformly dispersed throughout the polymeric matrix.
b. Nanocapsules (NC): the drug is confined within a polymeric coating
The uptake, distribution, and ocular retention of nanoparticles largely depend on their size and surface characteristics.
4.Liposomes
Liposomes are lipid-based vesicles with an aqueous core, widely used in ocular drug delivery for various drugs. The properties of liposomes, such as lipid composition, determine whether they provide extended drug release, rapid degradation, or non-biodegradability. For certain polymers like cellulose derivatives (e.g., hypromellose), gelation occurs through hydrophobic interactions at higher tempertures. Alternatively, polymers dissolved in a l decreased patible carrier can precipitate upon contact with water in tissues.
5. Niosomes
Niosomes are bilayered vesicles made of nonionic surfactants and cholesterol, capable of encapsulating both hydrophilic and lipophilic drugs. Unlike liposomes, niosomes are pH-independent, allowing consistent drug release and improved ocular bioavailability. Structurally, they resemble liposomes, but their bilayers are composed of nonionic surfactants rather than phospholipids. Niosomes can be unilamellar or multilamellar depending on the preparation method. They offer higher stability than liposomes and avoid some of their limitations, such as high cost and variable phospholipid purity.
6. Dendrimers
Dendrimers are nanoscale, highly branched polymeric structures built around a central core. Their well-defined architecture and small size make them easy to synthesize, modify, and functionalize with various surface groups. Because of these properties, dendrimers serve as promising carriers for ocular drug delivery (ODD). They are capable of encapsulating both hydrophilic and lipophilic drugs within their framework. Moreover, the choice of surface functional groups-such as amine, carboxyl, or hydroxyl groups-allows for tailoring their interactions, drug-loading capacity, and biocompatibility.
7.Hydrogels
Hydrogels are three-dimensional, hydrophilic polymeric networks that can absorb and retain large amounts of water or biological fluids. When applied in ocular formulations, they significantly improve the residence time of drugs on the ocular surface. Gelation can be triggered by variations in pH or temperature. Among the commonly used materials, poloxamers are popular due to their amphiphilic structure, where a hydrophobic core is surrounded by hydrophilic chains. Despite their effectiveness in prolonging drug contact time, hydrogels generally exhibit poor mechanical strength, which limits their performance in some applications.
8. Microneedle
Microneedle, Ultrasound, and lontophoresis-Based ODD Advanced non-invasive strategies such as microneedles, ultrasound, and iontophoresis are increasingly being explored to enhance ocular drug delivery, particularly for ta diseases. ng posterior eye
Microneedles: Drug-coated microneedles, usually 500-750 µm in length, can penetrate ocular tissues and rapidly release therapeutic molecules. The drug is often coated onto solid metal needles; after insertion and dissolution, the needles are removed, achieving much higher local drug concentrations compared to free-drug solutions.
Ultrasound-assisted delivery: Ultrasound has been
shown to improve the permeability of the cornea, thereby enhancing drug penetration. For example, beta-blockers such as Timolol maleate and Atenolol have been successfully delivered across the cornea with ultrasound application (20 kHz for 1 hour), showing promise in glaucoma treatment.
Ocular iontophoresis: This technique employs a mild
electric current to drive ionizable drugs across the cornea and sclera. It has demonstrated successful delivery of various drugs, including Ciprofloxacin hydrochloride, Gentamicin, and Dexamethasone, providing higher intraocular concentrations while minimizing systemic exposure.
Nanosuspensions offer several benefits that make them highly suitable for ophthalmic preparations (OP) and other drug delivery systems:
Improved solubility and bioavailability: They significantly enhance the dissolution rate of poorly water-soluble drugs.
Applicability to hydrophilic and hydrophobic drugs:
Types of Nanosuspension Preparation Methods: -
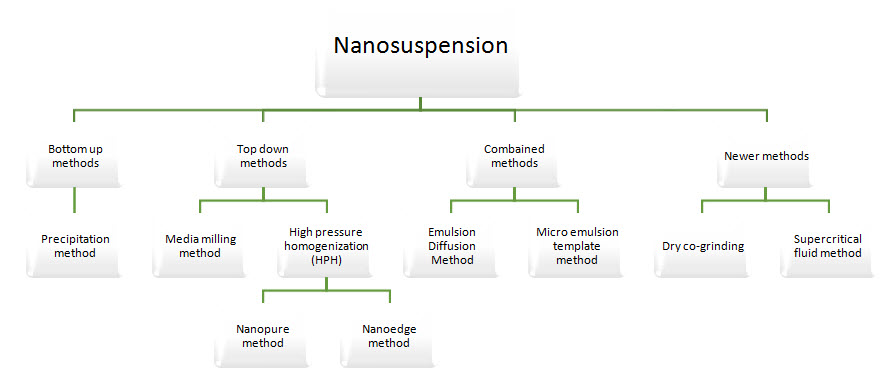
Nanosuspensions are typically produced using two main approaches:
1. Bottom-Up Technology
2. Top-Down Technology
1. Precipitation Method (PM):
2. High-Pressure Homogenization
In this method, the drug is first dispersed in a stabilizer solution to form a pre-suspension. This pre-suspension undergoes homogenization, initially at low pressure and then at high pressure, for about 10-25 cycles until nanoparticles of the desired size are obtained (Fig. 5).
3. Homogenization in Aqueous Media (Dissocubes?)
This approach involves forcing the suspension through a narrow gap using a high-pressure plunger pump. As the fluid passes through the orifice, the static pressure drops below the vapor pressure of water, causing instantaneous boiling and the formation of gas bubbles. Upon exiting the orifice, the pressure normalizes, leading to bubble collapse (cavitation). This implosion creates intense shear forces, which break down particles into nanosized ranges.
4. Homogenization in Non-Aqueous Media (Nanopure®)
In this variation, homoger on is performed in a mixture containing little c ater. The process is usually carried out at sub-zero or freezing temperatures, often referred to as deep-freeze homogenization. This technique is particularly suitable for thermolabile drugs, as it minimizes the risk of heat-induced degradation.
5. Nanoedge Technology
Nanoedge combines the principles of precipitation and homogenization to yield smaller and more stable nanoparticles within a shorter processing time. Here, a drug suspension is first prepared by precipitation and then subjected to high-pressure homogenization, further reducing particle size and enhancing stability.
6. Nanojet Technology (Opposite Stream Technique)
Also referred to as the opposite stream method, this technique involves dividing a drug suspension into two or more streams, which are then forced to collide with each other under high pressure. The intense shear forces generated during this collision break down the particles, leading to the formation of nanoparticles.
7. Media Milling
In this process, drug particles are subjected to mechanical attrition using milling media. The milling chamber is loaded with the drug, stabilizers, water (or buffer), and milling beads. When rotated at high shear rates, the collision between the drug and milling media provides sufficient energy to disintegrate microparticles into nanoparticles. The resulting nanosuspension is collected after separating the milling residues (Fig. 6).
8. Dry Co-Grinding
This is a relatively simple and economical technique for preparing nanosuspensio? does not require the use of organic solvents, making more environmentally friendly. During the process, poorly soluble drugs are co-ground with stabilizers, which improves their physicochemical properties, enhances dissolution rate, and increases bioavailability.
9. Emulsification-Solvent Evaporation Technique
In this method, the drug is first dissolved in a volatile organic solvent, which is then emulsified into a second liquid phase that acts as a non-solvent for the drug. On evaporation of the solvent, the drug precipitates out as fine nanoparticles. The risk of crystal growth and aggregation can be minimized by applying high shear forces using high-speed stirring during the process.
10. Melt Emulsification Method
In this technique, the drug is dispersed in an aqueous solution containing a stabilizer and heated above its melting point. The heated mixture is then homogenized to form an emulsion. During the process, the system is kept at a constant temperature using a heating tape fitted with a temperature controller to ensure it remains above the drug's melting point. Once emulsification is achieved, the mixture is cooled either gradually at room temperature or rapidly using an ice bath, leading to the formation of nanoparticles.
11. Solvent Evaporation Method
This method involves dissolving the drug (and polymer, if used) in a volatile organic solvent, followed by emulsification into an aqueous phase. High-speed homogenization or ultrasonication is applied to create fine droplets. The organic solvent is then evaporated either by continuous stirring at room temperature or under reduced pressure, leaving behind nanosized drug particles suspended in the aqueous phase.
12. Supercritical Fluid Method
Evaluation of Ophthalmic Suspensions
1. Description
A qualitative assessment of the drug product, including its appearance, color, and clarity.
Acceptance criteria must ensure uniformity and stability of the dosage form.
2. Identification (ID Test)
Confirms the identity of the active drug(s).
Should distinguish the drug from structurally related compounds.
Techniques such as infrared (IR) spectroscopy, near-infrared (NIR), Raman spectroscopy, or chromatographic methods are commonly employed.
3. Assay
Determines the actual drug content (strength) within the formulation to ensure dose accuracy.
4. Impurities
Identifies and quantifies potential impurities such as synthetic by-products, organic residues, or inorganic contaminants from both drug substances and excipients
5. pH Measurement
The natural tear fluid has a pH around 7.4.
Ophthalmic products should ideally be close to this pH but are generally tolerated within a range of Evaluation Parameters of Ophthalmic Suspensions (OP)
The quality, safety, and efficacy of ophthalmic preparations must be established through systematic evaluation.
Below are the key parameters:
1. pH
The pH should be adjusted to the value at which the drug product remains most stable.
The eye can tolerate a wide range (pH 3.0-8.6), but the physiological tear fluid pH is 7.4.
2. Osmolarity
Ophthalmic products are tolerated within 0.5-5% sodium chloride equivalence (171-1711 mOsm/kg).
Hypotonic solutions are generally better tolerated than hypertonic ones.
Osmolarity must remain consistent throughout the product's shelf life, co ↓ing possible effects from packaging materials .
3. Particulate and Foreign Matter
Suspensions must be checked for package integrity and visible particles.
Extrinsic matter: foreign contaminants unrelated to the product.
Intrinsic matter: product-related particles from manufacturing or degradation.
Inherent matter: predictable physical states/particles intrinsic to the formulation.
4. Sterility
Ophthalmic products must pass sterility testing.
Containers must be sterile, sealed, and tamper-proof from filling until first use.
5. Antimicrobial Preservatives
Required in multidose containers unless:
The formulation contains a radioisotope with a short half-life (<24 h), or
The product is inherently microbicidal.
6. Uniformity of Dosage Units
Ensures consistent
dr?
tent per dose.
Tested via content uniformity or weight
7. Container Contents
Must comply with the stated fill quantity and ensure dose accuracy.
8. Leachables and Extractables
Packaging should not release chemicals that alter the drug's quality, safety, or purity.
Risk assessments must evaluate potential toxicological impacts of leachables on ocular tissues.
9. Container-Closure Integrity
Packaging must be tamper-proof and provide protection against contamination and product loss.
Specific Tests for Ophthalmic Suspensions
1. Viscosity
Increased viscosity prolongs ocular residence time but may slow drug diffusion.
2. Antioxidant Content
If antioxidants are added, their levels must be monitored to ensure stability during the entire shelf life.
3. Re-suspend ability/Re-dispersibility
Suspensions must redisperse easily after sedimentation to maintain dose uniformity.
4. Particle Size and Size Distribution
Stability testing ensures that no aggregation or significant size changes occur during storage.
5. Drop Size
Typical drop volume: 20-70 μL.
Drop size influences dosing accuracy and is assessed during product development.
6. Added Substances
Stabilizers, antioxidants, or viscosity enhancers may be included if? and non-interfering.
Use of additives solely for color, odor, or flavor is prohibited.
Characterization of Nanosuspensions (NS)
In addition to standard suspension tests, nanosuspensions require specialized evaluations:
1 Particle Size & Polydispersity Index (PDI)
Critical for solubility, dissolution rate, and stability.
Methods:
Photon Correlation Spectroscopy (PCS): 3 nm-3 µm range.
Laser Diffraction (LD): 0.05-80 µm range.
Coulter Counter Multisizer (CCM): Provides absolute particle counts.
2. Zeta Potential
Indicates surface charge and stability. A minimum of ±30 mV ensures electrostatic stabilization of NS.
3. Crystalline State
Assessed using X-ray diffraction (XRD) or Differential Scanning Calorimetry (DSC) to determine if the drug is amorphous or crystalline.
4. Dissolution Studies
Measured according to the Noyes-Whitney equation, relating particle size reduction to faster dissolution rates and enhanced bioavailability.
5. In Vivo Studies
Required to confirm therapeutic performance, pharmacokinetics, and ocular tolerability.
Common Stabilizers: Surfactants: Tween 80, sodium lauryl sulfate, poloxamer 188.
Polymers: Polyvinylpyrrolidone (PVP), hydroxypropyl methylcellulose (HPMC), hydroxypropyl cellulose (HPC), polyvinyl alcohol (PVA).Mixtures of surfactants and polymers are often applied for enhanced stabilization .
Table no 1. Nanosuspension technology employed in eye preparation.
|
Drugs |
Technique Applied |
Formulation / Purpose |
Authors |
|
Ibufrofen
|
Freez Drying |
Eduragit RS1000 Nanosuspension for controlled ocular drug delivery |
Pignatello et al. |
|
Flurbiprofen |
Freez Drying |
Acrylate Polymer nanosuspension For ophthalmic therapy |
Pignatello et al. |
|
Hydrocortison Prednisolone Dexmethasone |
High-Pressure Homogenization |
Corticosteriod nanosuspensions designed for ocular administration |
Kassem et al. |
|
Diclofenac |
Freez Drying |
Biopolymeric nanosuspension Of diclofenac for ophthalmic application |
Sagar et al. |
|
Brinzolamide |
High- Pressure Homogenization |
Nanosuspension formulation for brinzolamide for intraocular drug delivery |
Songxiangrong And Weiyuquan |
|
Vitamin A |
High-pressure Homogenization |
Vitamin A nanosuspension prepared Evaluated for ophthalmic use |
Abbas Akhgari et al. |
CONCLUSION
From the reviewed literature, it can be concluded that nanosuspension (NS) technology effectively addresses the challenges of poor solubility in drugs. Commonly employed large-scale production methods include media milling, high-pressure homogenization, and freeze-drying, which have proven feasible and efficient. Compared to other novel drug delivery systems (NDDS), nanosuspensions are advantageous due to their relatively simple preparation process, minimal excipient requirements, and significant improvements in dissolution velocity and saturation solubility. The versatility and scalability of this technology position nanosuspensions as a powerful tool in pharmaceutical development. By advancing and applying NS formulations, society stands to gain substantial therapeutic benefits, potentially transforming future research and clinical practices in pharmacy.
REFERENCES



Pramila Wakchaure*, Pooja Phad, Vaishnavi Bhangare, Khodke Kiran, Shirbhate P., Nanosuspension Technology for Intraocular Delivery: A Promising Approach to Overcome Ocular Barriers, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 1819-1832 https://doi.org/10.5281/zenodo.17590120
 10.5281/zenodo.17590120
10.5281/zenodo.17590120
