Swamy Vivekanandha college of pharmacy, Namakkal, India.
Primary Amoebic Meningoencephalitis is a severe and swiftly progressing CNS infection caused by Naegleria fowleri. The organism, commonly found in warm freshwater, gains entry through the nose and advances along the olfactory pathway to the brain, producing marked inflammation, edema, and necrotic damage. Warmer global temperatures, insufficient chlorination practices, and greater recreational freshwater exposure have increased the geographic spread of N. fowleri, resulting in new cases beyond historically endemic regions. PAM diagnosis is challenging due to its resemblance to bacterial meningitis and the limited access to rapid molecular diagnostic tools. Confirmatory testing relies on the early detection of trophozoites in CSF and PCR assays. Treatment requires urgent initiation of multi-drug regimens chiefly amphotericin B and miltefosine, combined with rigorous management of intracranial pressure. Enhancing diagnostic capabilities, exploring innovative therapies, and reinforcing public health interventions are crucial to lowering mortality. Clinical pharmacists significantly support patient outcomes through precise drug selection, monitoring, and emergency care.
Naegleria fowleri, a thermophilic free-living amoeba prevalent in warm freshwater, causes an acute, quickly progressing, and frequently deadly infection of the central nervous system. Despite being uncommon, PAM is one of the worst CNS infections known to occur in humans, with a terrible case fatality rate of over 95%. When healthy children and young adults are exposed to warm freshwater bodies while engaging in recreational activities, they are more likely to get the disease. Usually, when tainted water gets into the nasal cavity, amoebae can move along the olfactory nerves and enter the brain, causing infection. Fever, intense headache, vomiting, photophobia, and a quick progression to seizures, coma, and death in a few of days are early signs that are similar to those of bacterial meningitis.(1) According to recent epidemiological data, rising global temperatures have caused a shift in PAM regional patterns, with new cases appearing in areas that were previously thought to be low-risk. The multiplication of N. fowleri and the probability of human exposure are increased by climate-related warming of lakes, rivers, and artificial water systems. Research from the US, Pakistan, India, and a number of Middle Eastern nations shows that cases have been rising since 2018.(2,3) Despite this, because of the disease's rarity, clinician awareness is still poor, which causes delays in diagnosis and treatment initiation. The diagnosis depends on the quick detection of trophozoites in CSF by antigen-based techniques, PCR assays, or microscopy. However, these tests are frequently limited to situations in which PAM is clinically suspected. Amphotericin B must be started right away as part of treatment; it is frequently used in conjunction with miltefosine, azithromycin, rifampicin, and aggressive intracranial pressure control. Increasing physician recognition and public awareness is crucial since early detection is closely linked to survival. Using nose clips, keeping pools and water systems properly chlorinated, and preventing warm freshwater entrance into the nose are all preventive strategies.(3) The need for better diagnostic instruments, more surveillance, and innovative therapy research is emphasized in recent literature.
ETIOLOGY AND MICROBIOLOGY OF NAEGLERIA FOWLERI
Naegleria fowleri is a free-living, thermophilic amoeba that belongs to the class Heterolobosea and phylum Percolozoa. It is the organism that causes human primary amoebic meningoencephalitis. There are three types of amoebae: trophozoite, flagellate, and cyst. The active, eating, infectious stage that causes illness in humans is the trophozoite. Trophozoites transform into a temporary, motile flagellate form when nutrients are scarce, whereas encystment happens when environmental stressors like low temperature or desiccation are present. Because of its versatility, N. fowleri can survive in a variety of aquatic settings. One of the most important aspects of its existence is its ability to withstand heat. The prevalence of N. fowleri in warm freshwater bodies can be explained by the fact that it develops best at 30 to 42°C and can withstand brief exposure to even higher temperatures. Heat-shock proteins and certain membrane lipids that allow resistance to high temperatures have been found through molecular research. Secreted proteases, phospholipases, pore-forming proteins, and metalloproteases that aid in tissue destruction and immune evasion are the main causes of the organism's pathogenicity.(4) The olfactory neuroepithelium and central nervous system of the host can be quickly invaded thanks to these virulence factors.
Recent advances in genomic analysis have shed light on metabolic pathways and gene clusters linked to pathogenicity. Significant variations between non-pathogenic Naegleria species and N. fowleri are revealed by comparative genomics, especially in genes linked to cytotoxicity, thermotolerance, and proteolysis.(5) The organism's roughly 30 Mb genome contains hundreds of proteins linked to host-pathogen interactions. Immunofluorescence assays, PCR amplification of particular gene targets such as 18S rRNA or ITS regions, and culture on non-nutrient agar with a bacterial lawn are all used in laboratory identification.(6) Recent developments in qPCR and multiplex diagnostic platforms have increased detection speed and sensitivity.
LIFE CYCLE DYNAMICS AND ECOLOGICAL ADAPTATIONS
In order to survive in a variety of environmental conditions, Naegleria fowleri has a flexible three-stage life cycle that includes trophozoite, flagellate, and cyst forms. The infectious trophozoite reproduces by binary fission and exhibits aggressive phagocytic activity. In unfavourable environmental conditions, trophozoites rapidly transform into a flagellated form that can move quickly, allowing relocation to more favourable environments. In extremely harsh conditions, such as low temperature, nutrient deprivation, or dehydration, the organism encyst, which is highly resistant to environmental stress and is not infectious to humans.(7) There is a substantial correlation between the environmental range of N. fowleri and warm freshwater environments. It is frequently isolated from geothermal springs, lakes, rivers, ponds, and swimming pools with inadequate chlorination.(8) The organism's biological range has expanded due to climate change, and it does well in temperatures exceeding 30°C. Research from 2018 to 2024 shows that N. fowleri is becoming more frequently found in areas of North America, Europe, and Central Asia that were previously thought to be low risk. Static shallow waters, biofilms, and sediment are the main reservoirs. Amoebae can enter the nasal cavity more easily when there is increased water agitation, such as while diving or swimming.(9) PCR-based detection, culture, filtration, and water sampling are all used in environmental surveillance. Faster and more sensitive detection is made possible by recent developments like qPCR assays and environmental DNA (eDNA) monitoring.
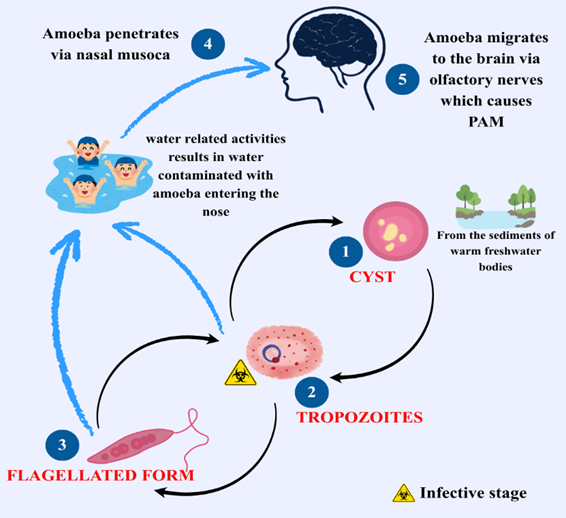
Fig 1: Lifecycle of Naegleria Fowleri
PATHOPHYSIOLOGY
Primary Amoebic Meningoencephalitis is caused by Naegleria fowleri's swift and devastating invasion of the central nervous system. The trophozoites of N. fowleri stick to and move through the olfactory neuroepithelium after exposure, usually through water entering the nasal cavity. They then migrate along olfactory nerve fibres through the cribriform plate to reach the olfactory bulbs and then deeper brain structures. After entering the brain parenchyma, amoebae quickly multiply and use a number of virulence mechanisms to cause tissue damage.(10) The release of cytolytic chemicals is a crucial component of pathogenesis. These include metalloproteinases, phospholipases, pore-forming proteins, and other proteases that break down extracellular matrix and host cell membranes to erode brain tissue. Edema, inflammation, and haemorrhagic necrosis result from this. Additionally, the infection causes a large inflammatory response in the host: pro-inflammatory cytokines are released by local microglia, recruited neutrophils, and macrophages, which intensify disruption of the blood–brain barrier and increase cerebral edema.(11) Furthermore, by breaking down endothelial cell tight junction proteins and hastening parenchymal invasion, N. fowleri may directly jeopardize the integrity of the blood-brain barrier. As the infection progresses, cerebral edema and increased intracranial pressure cause brain herniation, which frequently results in death. Autopsy examinations show localized demyelination, leptomeningeal congestion, haemorrhagic necrosis, and diffuse inflammation, particularly in the frontal lobes and olfactory bulbs. The extremely quick clinical decline observed in PAM, from nonspecific prodromal symptoms to coma and death frequently within a week, is correlated with these pathological alterations.(11)
The pace of advancement leaves little time for efficient host containment, according to recent case reports. The idea that both amoebic cytotoxicity and immune-mediated damage contribute to pathogenesis is supported by the confirmation of large amoebic burden and inflammatory markers in CSF by improvements in molecular diagnostics such as metagenomic sequencing.(12) It is essential to comprehend this dual mechanism, direct amoebic damage plus host-mediated inflammation in order to develop treatments that not only eradicate the pathogen but also regulate intracranial pressure and the immune system. The need for enhanced anti-amoebic medicines that can quickly pass the blood-brain barrier and neuroprotective techniques is highlighted by current research.
RISK FACTORS
The main risk factors for Primary Amoebic Meningoencephalitis are host behaviours, environmental exposure, and weather patterns that support Naegleria fowleri survival and spread. The main risk is nasal exposure to warm, fresh water, which is necessary for the amoeba to migrate into the brain. Water recreation is one of the main risk factors. N can be forced by swimming, diving, or jumping into lakes, rivers, ponds, or pools that aren't sufficiently chlorinated. Fowleri-contaminated water entering the nasal passages, particularly when the water is shaken.(13) Around the world, reports of such behaviours in PAM instances are common. Furthermore, non-recreational exposures are becoming more widely acknowledged. For instance, more recent publications have connected fatal PAM instances to nasal irrigation with tap water such as neti pots. Water systems in homes and businesses are another issue that is becoming more and more problematic. This emphasizes that N. fowleri can colonize man-made systems as well as natural water bodies, especially when the water is warm, stagnant, or improperly treated. Another important aspect is the climate. Because N. fowleri prefers warm temperatures, frequently above 30 °C, the amoeba's geographic and seasonal range has expanded due to climate change. In environmental investigations, N. fowleri is increasingly being found in previously low-risk areas. Heatwaves, long summer seasons, and poor water system upkeep all increase danger.(13) Additionally, age and host variables are important. The majority of PAM cases affect children and young people, perhaps as a result of their increased participation in water-based recreational activities. Additionally, anyone who often use nose water for personal cleanliness such as religious ablution may also be at risk, particularly in areas with inadequate water purification. A Pakistani woman experienced deadly PAM after ablution, according to a recent assessment, indicating that even household water use needs to be taken into account. (14) Another new risk factor is travel. After being exposed to N. fowleri in a vacation rental pool in 2020, a foreign visitor returning from India passed away from PAM, which was confirmed by PCR. Cross-regional strain similarities and molecular epidemiology were also clarified by the strain's genotype study. In conclusion, there are changing risk factors for PAM. In addition to traditional recreational water exposure, danger is increased by residential water systems, travel, climate change, and common nose habits. In order to reduce growing dangers, public health practices must change correspondingly.(15)
GLOBAL TRENDS AND OUTBREAK PATTERNS
Primary Amoebic Meningoencephalitis has a dynamic epidemiology that is influenced by both improved pathogen identification and changes in the environment. PAM was once thought to be limited to tropical and subtropical areas, but as global warming makes it easier for Naegleria fowleri habitats to spread, reports of the disease are growing in temperate zones.(14) Emerging hotspots in different places are shown by recent surveillance and case studies. Naegleria fowleri, for example, has been found in innovative water systems that were previously considered low risk, such as municipal and saline water sources. The amoeba may be harboured in contaminated municipal pipelines in metropolitan areas, according to a 2025 report from Pakistan that detailed a deadly case connected to domestic ablution fluids. Furthermore, a thorough narrative evaluation spanning 2020–2025 highlighted South Asia, particularly Pakistan and India, as a growing hub for PAM cases, highlighting weaknesses in both water infrastructure and environmental exposure. Cases pertaining to travel provide as additional evidence of the transnational character of risk. After being exposed to a vacation rental pool in India, a U.S. traveller died of PAM in a reported 2020 case; strain genotyping revealed a genotype prevalent in both regions, showing transnational strain circulation. Sporadic clusters continue to form in new environments outside of endemic areas. In Taiwan (2023–2024), a startling occurrence involving a fatal case of PAM in an indoor surfing facility using municipal water was reported. This case highlights the unconventional methods of transmission in affluent nations. The inquiry revealed N. Concerns over water system monitoring in developed environments were raised by the discovery of fowleri DNA in a stagnant, badly managed basement pool. (13) Epidemiological knowledge is also changing due to advancements in diagnosis. Early and precise detection of N. fowleri in cerebral fluid has been made possible by metagenomic next-generation sequencing, even in patients that do not respond to traditional antibiotic therapy. These technological advancements may raise incidence estimates by revealing previously undetected PAM cases. (11) Even though they are generally rare, the shifting distribution, infrastructure risk, and climate change highlight the critical need for more monitoring, regulation, and education. Public health plans must now take PAM into account in areas that were not previously thought to be at danger. Furthermore, molecular epidemiology-based genotype tracking may enhance preventive measures and forecast outbreak trends.
CLINICAL MANIFESTATION
Naegleria fowleri-caused primary amoebic meningoencephalitis manifests as a fulminant, quickly progressing infection of the central nervous system. Because the clinical presentation is so similar to acute bacterial meningitis, early identification is frequently overlooked. After nasal contact with polluted warm freshwater, the incubation period usually lasts two to seven days. Nonspecific prodromal symptoms include fever, acute frontal headache, lethargy, nausea, and vomiting are the first signs of the sickness. Initial inflammation of the meninges and olfactory bulbs is reflected in these early symptoms. (1) Neurological symptoms quickly worsen within 24 to 48 hours. Nuchal rigidity, photophobia, disorientation, and behavioural abnormalities are frequently experienced by patients as diffuse meningoencephalitis progresses. Studies reveal that by day two of symptom onset, altered mental status is typical, ranging from irritation to hallucinations and lethargy. More serious symptoms, such as seizures, cranial nerve palsies, focal neurological deficits, and ataxia, appear as cerebral edema worsens. Coma, autonomic instability, and eventually brainstem herniation are characteristics of advanced phases. Without very early care, the infection is nearly invariably fatal; even with rigorous therapy, the fatality rate surpasses 95%. Increased intracranial pressure, haemorrhagic necrosis, and widespread inflammation are the causes of this quick deterioration. (16) The majority of occurrences involve children and young people, most likely as a result of increased recreational water exposure and forceful water entry during diving or underwater swimming. According to a CDC analysis of instances in the United States between 2019 and 2022, almost all patients arrived at the hospital within three days of the onset of symptoms, but within a median of two and a half days of being admitted, they fell into a coma. Atypical presentations have also been emphasized in recent case reports. For example, a Texas case from 2021 showed early signs of viral meningitis, which postponed the need for a final course of treatment. Severe irritability and anosmia were noted as early symptoms in another Taiwanese instance from 2023, highlighting the need of identifying subtle neurological signals. (17) Clinicians should suspect PAM in patients with acute meningoencephalitis who describe recent exposure to freshwater, especially in warm months, due to the overlap with bacterial meningitis. The likelihood of starting rigorous ICP management and anti-amoebic medication on time is greatly increased by early consideration.
DIFFERENTIAL DIAGNOSIS
PAM's early symptoms are similar to those of other frequent viral and inflammatory disorders affecting the central nervous system, the differential diagnosis is wide. It's critical to differentiate PAM from these disorders because a delayed diagnosis significantly raises mortality. The acute bacterial meningitis differential diagnosis is the most crucial. Fever, headache, stiff neck, photophobia, and vomiting are common symptoms of both illnesses. PAM, on the other hand, usually advances more quickly and frequently results in significant neurological decline within a day or two.(18) Findings in PAM's cerebrospinal fluid, such as neutrophilic pleocytosis, low glucose, and increased protein, can resemble bacterial meningitis. The presence of motile trophozoites on a wet mount is the primary differentiator, however this calls for a high level of suspicion and knowledge. Another important factor is viral meningoencephalitis, especially that caused by enteroviruses, arboviruses, or herpes simplex virus. Usually progressing more slowly, viral infections can cause specific neurological impairments. Imaging of HSV encephalitis frequently reveals temporal lobe involvement, while PAM displays more widespread cerebral edema. In viral situations, lesser pleocytosis and normal CSF glucose can aid in differentiating. (18) Subacute meningoencephalitis, cranial nerve palsies, and hydrocephalus are the symptoms of tuberculous meningitis, another mimic. TBM is characterized by lymphocytic CSF, a longer duration, and a distinctive basal meningeal elevation on MRI. On the other hand, PAM changes significantly over hours as opposed to weeks.(18,19) It's also necessary to take into account other free-living amoebic infections, like those brought on by Balamuthia mandrillaris or Acanthamoeba spp. In contrast to PAM's rapid course, granulomatous amoebic encephalitis, which is caused by these organisms, develops gradually over weeks to months. Focal granulomatous lesions rather than widespread edema are commonly seen on imaging in granulomatous amoebic encephalitis.(19) Subarachnoid haemorrhage, autoimmune encephalitis, acute disseminated encephalomyelitis, and cerebral abscess are further differentials; however, these illnesses usually exhibit distinctive radiological or CSF patterns. (1)
DIAGNOSTIC METHODS
PAM progresses quickly and has a very high death rate, early and precise diagnosis is essential. Clinical suspicion is used in conjunction with laboratory and molecular techniques that can quickly identify Naegleria fowleri in cerebrospinal fluid to make the diagnosis. The initial diagnostic procedure is typically CSF analysis. Neutrophilic pleocytosis, low glucose, and increased protein are typical results that resemble bacterial meningitis. Gram stain, however, is negative. Because it can detect motile trophozoites with directed movement, wet mount microscopy is crucial. Although this approach is quick, it greatly relies on the skill of the technician. The detection of trophozoites in CSF or tissue samples is improved by direct observation using Wright-Giemsa or trichrome staining. Sensitivity, however, can be minimal, particularly in situations where amoebae are sparse or stationary. (15) PCR analysis with N. Fowleri-specific primers are currently among the most precise diagnostic instruments available. Real-time PCR tests can be used on CSF, tissue, or ambient samples to confirm the pathogen in a matter of hours. (20) Since 2020, PCR has been more accessible in reference labs and is capable of differentiating N. Balamuthia and Acanthamoeba fowleri. Metagenomic next-generation sequencing, is becoming a potent diagnostic tool, particularly when preliminary testing yields conflicting results. A 2021 investigation showed that in a fatal PAM case that was initially misdiagnosed as bacterial meningitis, mNGS found N. fowleri in CSF within 48 hours. Neuroimaging is helpful. Diffuse cerebral edema, loss of Gray-white distinction, ventriculomegaly, and indications of elevated intracranial pressure are commonly seen on CT and MRI scans. T2 hyperintensity in the frontal lobes and olfactory areas may be visible on MRI. (20) Environmental testing is crucial for investigating outbreaks. N. fowleri DNA in water systems, especially warm, stagnant, or weakly chlorinated sources, can be found using PCR-based techniques. Several evaluations highlight the necessity for clinicians to promptly inquire about recent freshwater exposure, particularly in the summer, as delays in diagnosis harm outcomes. (2)
NEUROIMAGING INSIGHTS
When evaluating Primary Amoebic Meningoencephalitis, neuroimaging is both supportive and crucial. Imaging results are not unique to Naegleria fowleri, but they do offer important details regarding intracranial pressure (ICP), consequences, and the severity of the disease. Imaging may appear normal at first, but abnormalities change quickly as the infection worsens. Computed tomography (CT) is frequently the first modality used in emergency situations. Diffuse cerebral edema, effacement of sulci, lack of Gray-white matter distinction, and ventriculomegaly are typical findings. A primary cause of death, uncal or tonsillar herniation, may be detected by CT in advanced cases. Sometimes haemorrhagic foci are seen as a result of amoebic invasion-induced necrotizing vasculitis. (21) The sensitivity of magnetic resonance imaging (MRI) in identifying early parenchymal involvement is higher. In the frontal lobes, olfactory bulbs, temporal lobes, and brainstem, T2-weighted and FLAIR sequences frequently display hyperintense signals. These regions correspond to the olfactory nerve's initial invasion route. Restricted diffusion may be seen on diffusion-weighted imaging (DWI), which is consistent with cytotoxic edema. Leptomeningeal enhancement from severe inflammation may be seen on gadolinium-enhanced imaging. (21) MRI often reveals bilateral frontal lobe edema, which can help distinguish PAM from viral or bacterial meningitis, which usually affects particular lobes or the meninges more significantly, according to a 2021 assessment of PAM cases. Rapid neurological decline was correlated with substantial frontal lobe swelling and diffuse cortical edema in the Taiwan PAM case from 2023, according to MRI. (16,21) The inability of imaging to differentiate between bacterial meningitis and PAM is a major restriction, which makes clinical and laboratory correlation crucial. Imaging, however, is essential for tracking ICP-related problems and directing aggressive treatment, such as hypothermia, hyperosmolar therapy, or CSF diversion. (19) Serial imaging is crucial, particularly for patients undergoing intense anti-amoebic treatment, according to recent research. Because of how quickly the disease progresses, improvements are rarely seen, but MRI alterations can monitor response to treatment.
TREATMENT AND MANAGEMENT
PAM is difficult to treat because of its quick progression and the poor effectiveness of current treatments. Although early, intensive, multi-drug therapy in conjunction with intracranial pressure (ICP) control has produced a few confirmed recoveries, survival is still uncommon. Amphotericin B, administered intravenously and intrathecally, is the mainstay of treatment because it attacks the trophozoite membrane directly. The suggested dosage is 0.7–1.5 mg/kg/day intravenously; in extreme circumstances, intrathecal injection is frequently used in addition. Amphotericin B's inconsistent effectiveness can be partially explained by its strong amoebicidal activity but restricted penetration into brain tissue. (1) Miltefosine, an anti-leishmanial medication with potent amoebicidal effects, is now a crucial part of contemporary therapy plans. Numerous survivors treated with a combination of amphotericin B, miltefosine, azithromycin, fluconazole, and rifampicin are documented in case reports from 2014 to 2022. One of the few drugs with reliable in vitro activity, miltefosine is useful against N. fowleri because it can interfere with membrane lipid metabolism. Rifampicin and fluconazole provide antifungal and antibacterial coverage during uncertain early diagnosis, whereas azithromycin is employed for its synergistic effects.(1,3) Supportive management is also essential. Herniation and uncontrolled cerebral edema account for the majority of deaths. Using treatments including mannitol, hypertonic saline, CSF drainage (EVD), hyperventilation, and therapeutic hypothermia, vigorous ICP management is crucial. Survival is best predicted by early diagnosis. Therapy started within 24 to 30 hours of the beginning of symptoms for many survivors. Effectiveness is drastically decreased by delays after this window. Posaconazole, nitroxoline, and medications delivered via nanoparticles are examples of emerging treatments that are being researched; nevertheless, there is still little clinical data. (5)
EMERGING & EXPERIMENTAL THERAPIES
Due to the extremely high mortality of PAM, significant research has focused on identifying novel therapeutic agents with better brain penetration, amoebicidal potency, and reduced toxicity. Miltefosine remains the most important emerging drug. Although now integrated into standard treatment protocols, ongoing studies explore optimal dosing, pharmacokinetics, and combination therapy. Recent in vitro studies confirm its potent amoebicidal activity at clinically achievable concentrations. (6) Posaconazole, a triazole antifungal, has shown significant promise. Its ability to inhibit ergosterol synthesis in amoebic membranes makes it effective against trophozoites and cysts. Case reports from 2021 and 2022 document successful use of posaconazole as adjunctive therapy. Animal studies have demonstrated high CNS penetration and strong synergy with Amphotericin B. (1) Nitroxoline, a urinary antimicrobial used in Europe, emerged as a novel candidate in 2020 after researchers discovered strong amoebicidal effects in vitro. Subsequent studies confirmed its ability to inhibit trophozoite proliferation at low micromolar concentrations. Other promising experimental approaches include nanoparticle-based drug delivery systems to improve brain penetration, iron-chelating therapies, and photothermal therapy using targeted nanoparticles. While still experimental, these technologies aim to overcome challenges related to drug permeability across the blood–brain barrier. (1,5) Immunomodulatory therapy is another important area, because host inflammatory response contributes significantly to CNS damage, controlled suppression using corticosteroids or cytokine inhibitors may improve outcomes. Research from 2021–2023 suggests that dexamethasone may reduce cerebral edema when combined with anti-amoebic therapy. CRISPR-based genomic studies are identifying molecular targets in N. fowleri, including proteins involved in motility, membrane structure and cytolysis, paving the way for future targeted therapies. (5)
PUBLIC HEALTH STRATEGIES FOR PAM PREVENTION
Preventing primary amoebic meningoencephalitis involves two principal approaches: minimizing environmental exposure to Naegleria fowleri and enhancing public health infrastructure to effectively detect and respond to contaminated water sources. Since infection occurs predominantly via the nasal route, primary preventive measures emphasize limiting direct nasal contact with warm freshwater, particularly during periods of increased risk. Recommendations from health authorities include abstaining from diving or immersing the head in warm freshwater bodies, utilizing nose clips during aquatic activities, and avoiding disturbance of sediments in shallow, warm waters, where the amoeba is commonly present. It is also critical to ensure that water used for nasal irrigation such as neti pots or religious ablutions is sterile, distilled, or boiled and cooled, as recent incidents implicate tap water in fatal cases of infection. (3) This highlights the importance of consistent and clear public health messaging regarding water safety for nasal rinsing practices. At the community level, prevention emphasizes maintaining safe water through proper disinfection and regular monitoring. Key actions include ensuring swimming pools, splash pads, and public water systems are adequately chlorinated, checking disinfectant levels, controlling biofilms, and repairing water infrastructure promptly. Outbreaks have shown that lapses in these controls or stagnant water increase risk, highlighting the critical role of engineering measures alongside personal behavioural guidelines. (10) Effective surveillance and rapid health responses are also essential. Because PAM is rare but quickly fatal, prompt environmental testing after suspected exposure can guide timely interventions, such as closing and disinfecting affected sites. Public health efforts focus on seasonal risk messaging and educating clinicians to ask about freshwater exposure to enable early diagnosis and treatment. (22) Policy steps, including routine water quality records for public splash parks and clear safety labels on nasal irrigation products, are being implemented in some regions to further reduce risk. Prevention at an individual level, such as using nose clips and sterile irrigation water, is important, but effective control on a larger scale relies on well-coordinated public health infrastructure, vigilant management of water systems, and continuous community education to transform awareness into fewer exposures and earlier detection.
BARRIERS TO EARLY IDENTIFICATION AND EFFECTIVE THERAPY
Diagnosis and treatment of primary amoebic meningoencephalitis (PAM) involve several interconnected challenges that contribute to its high mortality. Early symptoms like fever, headache, and nausea are nonspecific and mimic bacterial meningitis, often leading to initial antibacterial treatment and delayed amoeba-specific testing. Laboratory diagnosis requires immediate lumbar puncture and skilled personnel for wet-mount microscopy, resources often unavailable at all hours. Although PCR and molecular tests are more accurate, they are usually limited to specialized labs, causing delays. Metagenomic sequencing is helpful in complex cases but is expensive and not widely accessible. (19) Therapeutic options are limited. Amphotericin B remains the main treatment but has poor brain penetration and notable toxicity. Miltefosine has recently become an important adjunct, with survivors often receiving combination therapy including it, though controlled clinical data are lacking. Effective treatment is complicated by drug delivery challenges across the blood-brain barrier and the amoeba’s rapid growth. (6) Managing severe cerebral edema and intracranial pressure is critical; the prognosis worsens significantly if treatment is delayed despite aggressive ICU interventions. Systemic barriers include limited clinician awareness, lack of standardized rapid diagnostics, restricted miltefosine availability, and difficulties in conducting clinical trials for such a rare, rapidly fatal disease. (22) Current guidelines stress quick referral to specialized labs, stockpiling essential medications regionally, and standardized emergency protocols combining early multi-drug treatment with aggressive management of intracranial pressure to improve survival chances.
FUTURE DIRECTIONS AND RESEARCH NEEDS
Given the poor survival rates in PAM, research focuses on early diagnosis, better treatments, and prevention informed by environmental data. Rapid point-of-care tests that detect N. fowleri in cerebrospinal fluid or clinical samples within hours are a high priority. Emerging methods like fast PCR, isothermal amplification, and lateral-flow antigen tests could allow bedside diagnosis and faster targeted treatment. Efforts should prioritize validating these tools and expanding access to regional hospitals. Drug research and delivery also need urgent progress. Although miltefosine has shown improved outcomes in some cases, detailed pharmacokinetic and pharmacodynamic data especially regarding central nervous system penetration and dosing are limited. Research into new amoebicidal compounds that penetrate the blood-brain barrier, repurposing existing CNS-active antimicrobials, and combination therapies is necessary. (5) Nanoparticle and liposomal drug delivery systems show promise for improving CNS drug delivery and reducing side effects, warranting further development and translation from preclinical studies. Investigating therapies that control damaging neuroinflammation without compromising pathogen elimination is important. Given that PAM involves both direct amoeba-induced brain damage and immune-mediated injury, combining amoebicidal agents with targeted anti-inflammatory strategies such as cytokine modulation could improve patient outcomes. Controlled animal studies are needed before clinical use of anti-inflammatory drugs like corticosteroids or cytokine inhibitors. Important research also involves environmental surveillance and predictive tools, including standardized sampling, advanced DNA detection, and climate-based prediction models that support targeted interventions. Strain-specific genomic epidemiology can trace infection sources and guide cleanup efforts. (19) Due to PAM’s rarity, building global registries and research networks is critical for pooling data on disease progression and treatment efficacy, and for clinical trial readiness. Adaptive trial designs and pre-approved emergency investigational protocols can speed up evaluation of novel treatments. Integrated investment in diagnostics, therapeutics, environmental monitoring, and clinical collaboration remains crucial to lowering PAM mortality.
ROLE OF CLINICAL PHARMACIST IN PRIMARY AMOEBIC MENINGOENCEPHALITIS
Primary amoebic meningoencephalitis (PAM), caused by Naegleria fowleri, is a swiftly progressing and highly fatal central nervous system infection. Clinical pharmacists play a vital part in improving prognosis by guiding early therapeutic decisions, selecting appropriate drugs, and collaborating within the healthcare team. Their major role includes ensuring immediate administration of key antimicrobials such as amphotericin B, miltefosine, rifampicin, fluconazole, and azithromycin, adjusted according to patient-specific needs. They also support clinicians by optimizing dosing regimens, evaluating drug–drug interactions, and monitoring for significant toxicities, particularly amphotericin B–associated kidney damage. (1) Pharmacists further contribute by providing evidence-based advice on combination therapy, drug level monitoring, and preparation of specialized formulations like intrathecal or intraventricular treatments when needed. During emergencies, they assist in rapid medication sourcing, preventing delays that could reduce survival chances. (19) Beyond direct treatment, clinical pharmacists promote public health by educating clinicians and communities about exposure risks, early symptoms, and safe water practices. They also help develop treatment protocols, document adverse drug reactions, and reinforce antimicrobial stewardship for rare infections like PAM. Collectively, their efforts enhance patient safety, optimize therapeutic outcomes, and support swift management of this life-threatening disease.
REFERENCES


R. Subashini*, S. Arthanareeswaran, V. Sandhiya, C. Shifa Sidhiq Fatima, Y. Sneha, B. Rashmi Avanticaa, C. Rifa Sidhik Fathima, Naegleria Fowleri and Primary Amoebic Meningoencephalitis: Emerging Threats in A Warming World, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 1577-1589 https://doi.org/10.5281/zenodo.17865420
 10.5281/zenodo.17865420
10.5281/zenodo.17865420
