1,3 Department of Materia Medica, Government Homoeopathic Medical College, Trivandrum
2 Department of Materia Medica, Maria Homoeopathic Medical College, Thiruvattar, Kanyakumari
Cholesteatoma is a locally destructive middle-ear disease for which surgery is considered definitive treatment. Reports on non-surgical homoeopathic management are scarce. This case report describes the constitutional homoeopathic management of a confirmed cholesteatoma case and its clinical and radiological outcome. Case Presentation :A 40-year-old male presented with chronic, purulent, foul-smelling right-sided otorrhoea for one year, associated with mild hearing impairment. HRCT of the temporal bone confirmed right-sided cholesteatoma with bony erosion. Intervention and Outcome :Based on constitutional assessment and repertorization, Tuberculinum was prescribed. Over follow-up, the patient showed marked reduction and eventual cessation of otorrhoea with improvement in general well-being. Follow-up HRCT demonstrated stability of previously noted bony destruction with no further progression. Conclusion: This report is unique in documenting constitutional homoeopathic management of HRCT-confirmed cholesteatoma with radiological stabilization assessed through follow-up imaging and MONARCH criteria. Further controlled studies are needed to validate these observations.
Cholesteatoma is a benign but potentially destructive lesion of the temporal bone, formed by keratinizing squamous epithelium that can cause chronic inflammation, progressive bone erosion, and hearing impairment.[1]The term is a misnomer, as these lesions do not contain cholesterol or fat, and was first introduced by Johannes Müller in 1863. Cholesteatomas most commonly occur in the pneumatized areas of the middle ear and mastoid, rarely affecting the external auditory canal.[1]
They may be congenital or, more commonly, acquired, often resulting from tympanic membrane retraction due to eustachian tube dysfunction, infection, trauma, or previous surgery.[2–4] Negative middle-ear pressure promotes retraction pockets, allowing keratin accumulation to form a cholesteatoma sac, while secondary-acquired forms may follow acute otitis media or direct injury.[3–5] Pathogenetic theories include epithelial migration through tympanic membrane defects, squamous metaplasia, and basal cell hyperplasia proliferating into Prussak’s space.[3–6]
Clinically, cholesteatomas are usually unilateral, presenting with persistent or recurrent foul-smelling otorrhea, hearing loss, vertigo, and occasionally facial palsy or intracranial complications.[2,7] Otoscopically, they appear as pearly white or yellow masses, often in the posterior superior quadrant of the tympanic membrane or within retraction pockets. Assessment of ossicles, mastoid air cells, and facial nerve, along with audiometry and imaging, is essential.[2,8]
High-resolution computed tomography (HRCT) is the preferred imaging for evaluating bony destruction, while diffusion-weighted MRI helps distinguish soft-tissue pathology and detect postoperative recurrence.[9–12]Combining CT and MRI improves diagnostic accuracy and may reduce second-look surgeries.[10–12]
Surgical excision remains the mainstay, aiming to create a safe, dry ear, preserve or restore hearing, and prevent progression. Tympanomastoidectomy with ossicular reconstruction may be canal wall-up or canal wall-down depending on disease extent, each with its own benefits and recurrence risk. Postoperative follow-up with otomicroscopy and audiometry is essential, with complications being uncommon but potentially including facial nerve weakness, hearing loss, persistent otorrhea, balance issues, or intracranial infection.[2,13]
Epidemiologically, cholesteatoma affects 6–9 per 100,000 individuals, more common in children, with a slight male predominance and higher incidence among patients with cleft palate or familial predisposition. Socioeconomic factors and access to specialized care also influence outcomes.[2,7]
PATIENT INFORMATION
A 40-year-old male presented to the OPD of Government Homoeopathic Medical College , Thiruvananthapuram on 07-10-2023 with a one-year history of persistent right-sided otorrhoea. The discharge was purulent, foul-smelling, and occurred 5–6 times daily, with a progressive increase over the last four months. The profuse discharge caused marked discomfort, often wetting the pillow and preventing him from lying on the right side. The patient was apparently healthy prior to the onset of symptoms. Initially, he experienced offensive discharge 3–4 times per day and received allopathic treatment without relief. A high-resolution CT scan of the temporal bone confirmed the diagnosis of right-sided cholesteatoma, for which surgical intervention was advised. Seeking alternative management, he underwent Ayurvedic treatment but experienced no improvement, following which he visited the homoeopathic OPD for further evaluation. He has a history of recurrent allergic rhinitis, and the family history revealed tuberculosis in his father.
CLINICAL FINDINGS
After detailed analysis and evaluation of the case, the totality of symptoms was constructed by considering both the mental and physical characteristics of the patient. Mentally, he was markedly obstinate, reserved, and exhibited a strong desire for unplanned travelling along with a tendency to explore new foods. His preference for spicy food and aversion to sour items reflected a distinct individuality and restlessness in temperament.
On physical evaluation, he had profuse perspiration over the scalp, moderate appetite and thirst, and regular bowel habits. Due to continuous discharge from the right ear, he preferred sleeping on the left side to avoid discomfort. Local examination revealed purulent, offensive discharge from the right ear, and otoscopy showed debris within the external auditory canal. HRCT findings confirmed bony involvement, supporting the diagnosis of cholesteatoma.
Based on the clinical presentation, HRCT findings, and constitutional characteristics, the case was diagnosed as right-sided cholesteatoma. The miasmatic evaluation of the presenting symptoms suggested a predominance of the Tubercular miasm, as described in classical homoeopathic literature, owing to the recurrent suppuration, chronicity, offensive discharge, and destructive pathology. His emotional restlessness, desire for change, obstinacy, and family history of tuberculosis further supported a tubercular diathesis.
REPERTORIAL ANALYSIS
The case was repertorized (cross repertorization )using Zomeo Elite homoeopathic software, and the repertorisation chart yielded Calcarea carbonica, Silicea, Belladonna, Sulphur, Aurum metallicum, and Tuberculinum as the top remedies. Also verified in the Synthesis repertory, Tuberculinum emerged as the only remedy listed under the rubric EAR – Discharges, chronic – right. On the basis of repertorial analysis, consultation of Materia Medica, and the patient’s constitutional profile, Tuberculinum was selected as the first prescription. The drug is well known for its affinity toward recurrent suppurative conditions, chronic destructive processes, restlessness, obstinate temperament, and tubercular predisposition, making it the most suitable constitutional remedy for this case.
THERAPEUTIC INTERVENTION
On 10th October 2023, after detailed assessment of the mental, physical, and pathological characteristics of the patient, Tuberculinum 200C was prescribed as a single dose advised to take in morning empty stomach, followed by placebo (Saccharum lactis) . The patient was advised regular follow-up to monitor symptomatic response and disease progression.
BASIS OF SELECTION[14,15]
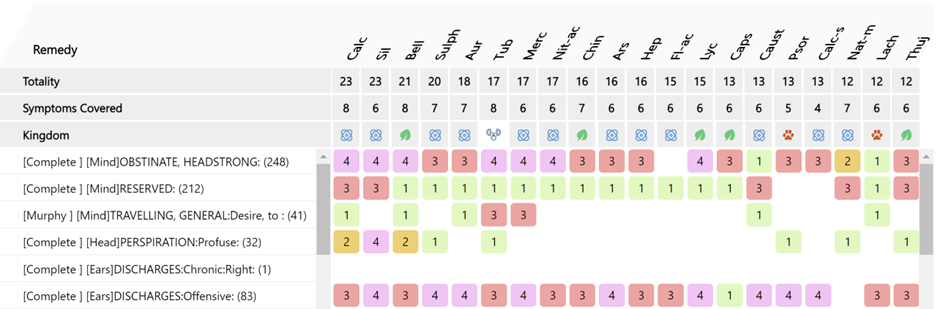
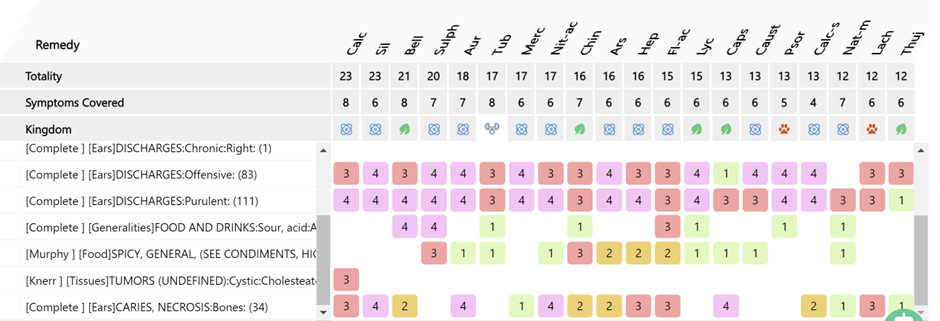
FIG 1 Repertorial chart
FOLLOW UP
During the follow-up visits, progressive improvement was noted both in the local ear pathology and in the patient’s general condition. On 25th October 2023, the patient reported a significant reduction in the frequency of right ear discharge, which had decreased to two episodes per day. General well-being had improved, and Saccharum lactis was prescribed for two days, to be taken once weekly.
On 15th November 2023, the patient experienced only occasional right-sided ear discharge and reported continued general improvement. No new complaints were observed, and Saccharum lactis was continued in the same dosage weekly.
By 29th November 2023, the patient continued to improve with no new symptoms and only minimal residual discomfort. The placebo (Sac lac) was maintained as previously.
On 13th January 2024, the patient reported no reappearance of ear discharge, along with subjective improvement in hearing. General health remained stable, and Sac lac was again prescribed. The improvement persisted on the follow-up visit dated 27th January 2024, and the same prescription was continued.
On 10th February 2024, the patient remained asymptomatic with no recurrence of discharge, and placebo was continued weekly.
However, on 2nd March 2024, the patient reported acute symptoms of sneezing with coryza for one week, accompanied by slight right-sided ear discharge for four days. Considering the recurrence of discharge along with the patient’s constitutional background and miasmatic evaluation, Tuberculinum 1M was prescribed as a single dose.
On 4th May 2024, the patient reported significant improvement with complete relief from the recent complaints and no new symptoms. The patient was maintained on Sac lac for two days. No adverse or unanticipated effects were observed during the treatment period.
TABLE 1 FOLLOW UP TABLE
|
Date |
Clinical Findings |
Prescription |
|
25.10.2023 |
Significant reduction in right ear discharge (≈2 times/day). General well-being improved. |
Saccharum lactis for 2 days, once weekly. |
|
15.11.2023 |
Occasional right-sided discharge. Continued general improvement. No new complaints. |
Saccharum lactis continued weekly. |
|
29.11.2023 |
General improvement. No new symptoms. Minimal residual discomfort. |
Saccharum lactis continued. |
|
13.01.2024 |
No reappearance of discharge. Subjective improvement in hearing. [Formal audiometric evaluation could not be performed; hearing improvement was subjectively reported.] General health stable. |
Saccharum lactis continued weekly.
|
|
27.01.2024 |
Sustained improvement. No new symptoms. |
Saccharum lactis continued weekly |
|
10.02.2024 |
Asymptomatic. No recurrence of discharge |
Saccharum lactis continued weekly. |
|
02.03.2024 |
Sneezing with coryza for 1 week. Mild right-sided discharge for 4 days. Acute exacerbation. |
Tuberculinum 1M/1 dose [stat] Rubrum pills [3-3-3] |
|
04.05.2024 |
Significant improvement. No new symptoms. Complete relief from recent complaints. |
Saccharum lactis for 2 days. |
TABLE 2 MODIFIED NARANJO CRITERIA FOR HOMOEOPATHY [MONARCH]
|
Sr. No |
DOMAINS |
YES |
NO |
NOT SURE |
|
1.
2.
3. 4.
5.
6A.
6B.
7.
8.
9.
10. |
Was there an improvement in the main symptom or condition for which the homoeopathic medicine was prescribed? Did the clinical improvement occur within a plausible timeframe relative to the medicine intake? Was there a homeopathic aggravation of symptoms? Did the effect encompass more than the main symptom or condition (i.e., where other symptoms, not related to the main presenting complaint, improved or changed? Did overall well-being improve? (Suggest using a validated scale or mention about changes in physical, emotional and behavioural elements) Direction of cure: Did some symptoms improve in the opposite order of the development of symptoms of the disease? Direction of cure: Did at least one of the following aspects apply to the order of improvement in symptoms: -from organs of more importance to those of less importance? -from deeper to more superfcial aspects of the individual? -from the top downwards? Did “old symptoms” (defned as non-seasonal and non-cyclical symptoms that were previously thought to have resolved) reappear temporarily during the course of improvement? Are there alternative causes (i.e., other than the medicine) that- with a high probability- could have produced the improvement? (Consider know course of disease, other forms of treatment and other clinically relevant interventions) Was the health improvement confrmed by objective evidence? (e.g., investigations, clinical examination, etc.) Did repeat dosing, if conducted, create similar clinical improvement?
Total: +10 |
+2
+1
-
+1
+2
-
+1
-
-
+2
+1 |
-
-
0
-
-
-
-
0
0
-
- |
-
-
-
-
-
0
0
-
-
0
- |
The total MONARCH score was +10, suggesting a probable causal relationship between the homoeopathic intervention and clinical outcome.
HRCT SCAN REPORT
Pre- and post-treatment HRCT scans showing stabilization of osteolytic changes.
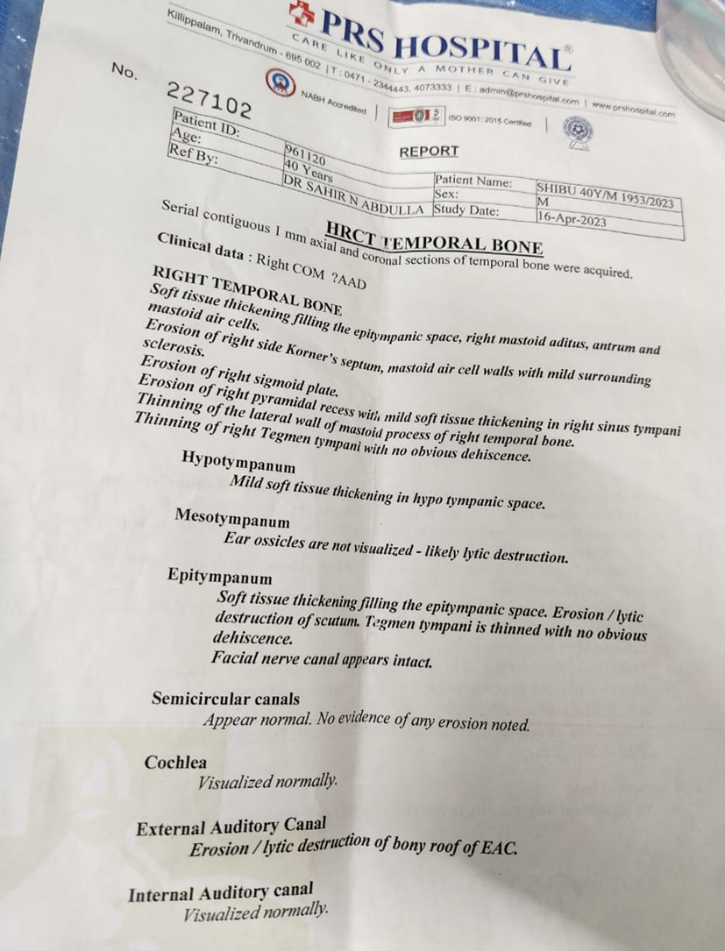
FIG 2 A BEFORE TREATMENT
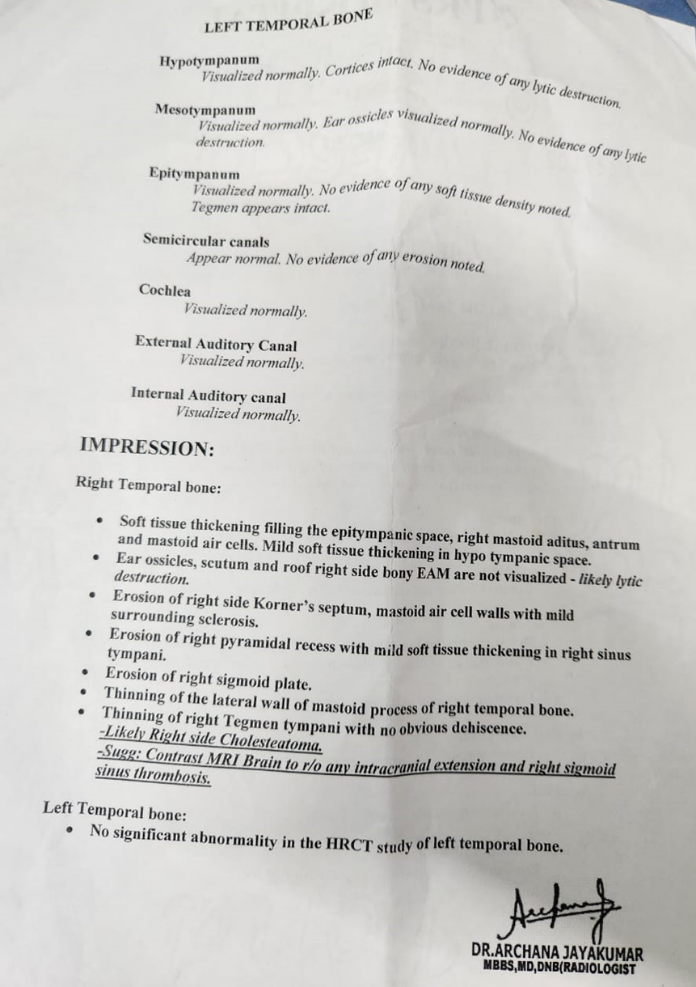
FIG 2 B
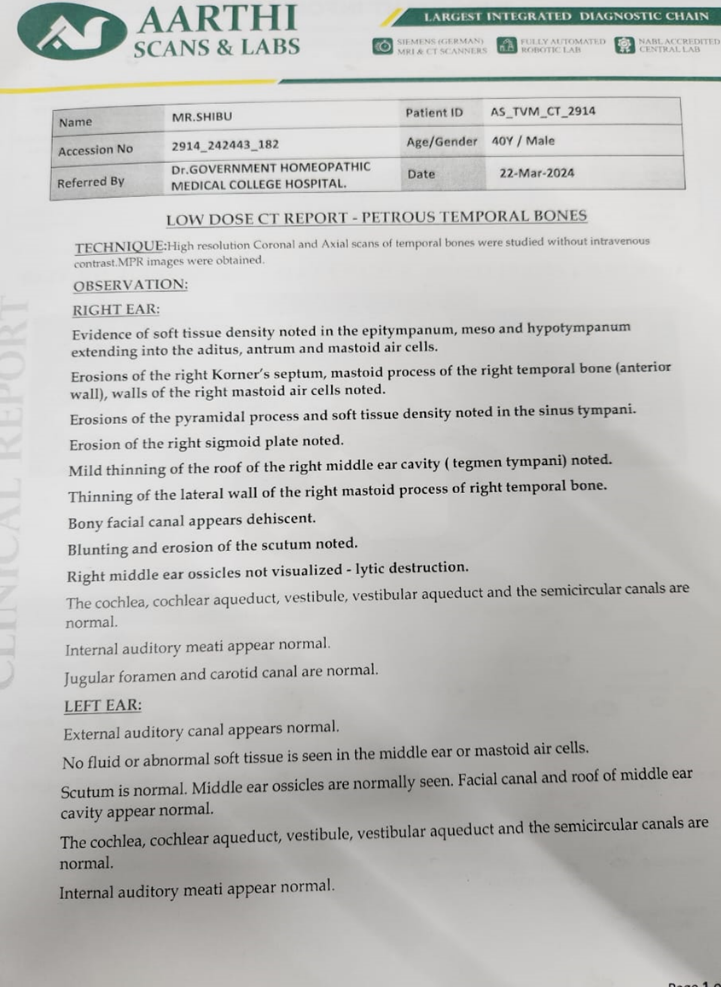
FIG 3 A AFTER TREATMENT
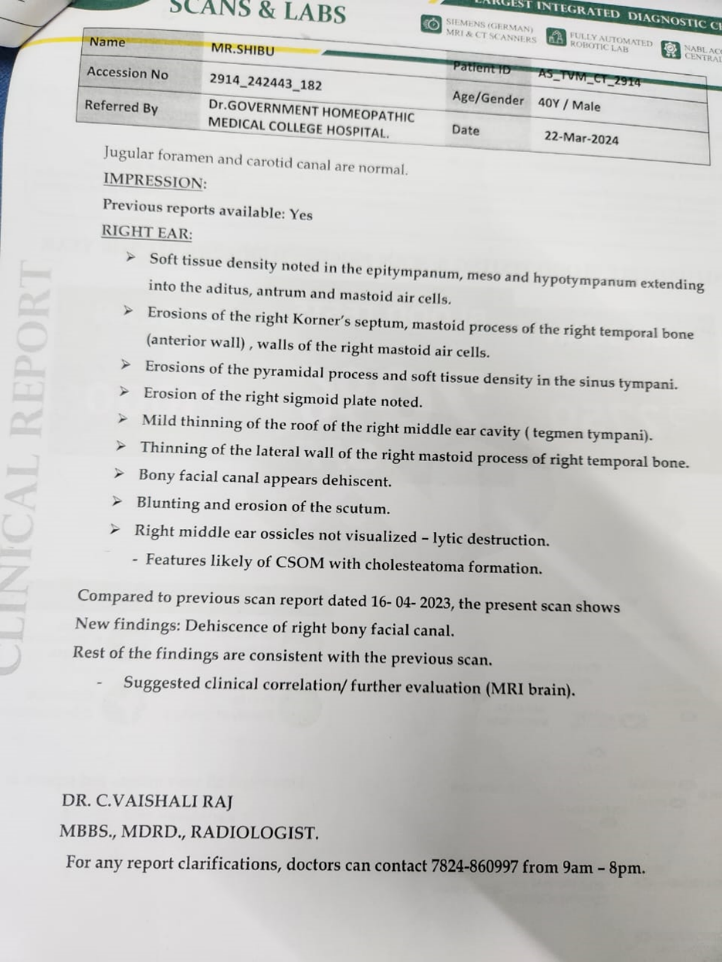
FIG 3 B
PATIENT PERSPECTIVE
The persistent discharge from my right ear was affecting my sleep and daily activities. After starting homoeopathic treatment, the discharge gradually reduced and eventually stopped. I feel healthier overall, and I am satisfied with the improvement without undergoing surgery. The follow-ups and attention given by the doctor made me feel reassured and involved in my care.
DISCUSSION
Cholesteatoma is a locally destructive lesion of the temporal bone characterized by the accumulation of keratinizing squamous epithelium, which promotes chronic infection, inflammation, and progressive bony erosion. The condition is conventionally managed surgically, with tympanomastoidectomy and ossicular reconstruction being the gold standard to prevent further destruction and restore auditory function. However, surgery may not be feasible for all patients due to personal preference, comorbidities, or other constraints.
In this case, a 40-year-old male with chronic, purulent, and offensive right-sided otorrhea associated with mild hearing loss was diagnosed with cholesteatoma through HRCT. Initial imaging revealed soft tissue thickening in the epitympanic space, mastoid air cells, and antrum, with erosions of the right temporal bone including the Koerner’s septum, pyramidal process, and scutum. The initial impression suggested active cholesteatomatous destruction with associated osteolytic changes.
The patient received individualized homoeopathic treatment with Tuberculinum 200/1D, selected based on constitutional features including a marked desire for traveling, an interest in exploring new foods, offensive purulent discharge, and a family history of tuberculosis. Follow-up over several months demonstrated significant symptomatic improvement, including reduced frequency and severity of otorrhea and subjective improvement in hearing.
The follow up HRCT scan revealed stability of the previously noted lytic changes, with no new areas of bone erosion and arrest of destructive progression. Mild dehiscence of the bony facial canal was noted, but the overall destructive process observed in the initial scan remained unchanged. These findings suggest that homoeopathic treatment helped stabilise the condition, prevented further progression of the cholesteatoma, and provided effective symptomatic relief.
This case highlights the potential role of individualized homoeopathic management in chronic cholesteatoma, particularly in providing symptomatic improvement and stabilizing disease progression. While surgical excision remains the definitive treatment, constitutional homoeopathy may offer a useful complementary or alternative option for patients seeking non-surgical approaches, especially in arresting disease advancement and enhancing quality of life.
Moreover, considering that very few published reports have documented the homoeopathic management of cholesteatoma, this case contributes valuable clinical insight to the existing literature. As a single-case report, findings cannot be generalized. Absence of histopathological confirmation and lack of audiometric quantification are limitations of this case.
Further controlled studies with larger patient populations are required to validate these findings and establish standardized protocols for homoeopathic intervention in cholesteatoma management.
CONCLUSION
This case demonstrates that individualized homoeopathic treatment may provide symptomatic relief and potentially stabilize disease progression in chronic cholesteatoma. While surgical intervention remains the definitive management to prevent further structural damage and restore hearing, homoeopathy can serve as a complementary or alternative option for patients unwilling or unable to undergo surgery. The observed arrest of destructive changes on HRCT and reduction in clinical symptoms suggest that personalized homoeopathic care could improve patient quality of life. Further controlled studies are warranted to substantiate these findings and to develop evidence-based protocols for homoeopathic management of cholesteatoma.
DECLARATION OF PATIENT CONSENT
We have obtained written consent from the patient. He has also agreed to the publication of his clinical information in the journal, with the assurance that his name and initials will not be disclosed.
FINANCIAL SUPPORT AND SPONSORSHIP: Nil.
CONFLICTS OF INTEREST: None declared.
REFERENCES


Dawood Nisha S, Anupama U, Nisha M, Management of Cholesteatoma with Constitutional Homoeopathic Treatment: A Detailed Case Report, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 647-656. https://doi.org/10.5281/zenodo.18173961
 10.5281/zenodo.18173961
10.5281/zenodo.18173961
