Dr. K. V. Subba Reddy Institute of Pharmacy, Dupadu, Kurnool.
Iontophoresis is a fascinating technique that utilizes a low electric current to facilitate the transdermal delivery of ions and charged molecules. This method has garnered significant interest in recent years as an alternative to traditional drug delivery systems, especially for targeting localized conditions and minimizing systemic side effects. This review provides an in depth examination of the principles underlying iontophoresis, including its mechanisms, equipment, and factors affecting drug transport. Key applications in dermatology, pain management and treatment of hyperhidrosis are highlighted, showcasing the therapeutic potential of iontophoresis across diverse medical fields. Additionally, we address recent advancements, such as the development of novel drug formulations and enhanced device technologies, which have improved the efficacy and broadened the applications of iontophoretic drug delivery. Challenges, including skin irritation and variability in individual responses, are discussed alongside potential strategies for overcoming these limitations. This article aims to present a comprehensive overview of iontophoresis and its growing role in modern medicine, while also identifying future research directions for optimizing its clinical use..
Transdermal medication delivery is becoming more and more significant in contemporary pharmacological therapy. When non-ionized medications are needed in modest dosages, it is utilised. It is possible to administer transdermally passively or with assistance. The non-ionized medication enters the skin through the stratum corneum during passive delivery. Due to its semi-permeable nature, the skin only permits a minimal quantity of medication molecules to infiltrate the skin [1]. Ionised medications are difficult to pass through this barrier, hence routine transdermal distribution is not recommended unless an outside energy source is available to push the medication through the skin. Facilitated diffusion is assisted by electrical energy through iontophoresis, electroosmosis and convective water flow [2]. Iontophoresis, also called ionophoresis, electrophoresis or cataphoresis is a technique for increasing the therapeutic absorption of ionic medications into the body by applying an electrical current [3]. Iontophoresis works by making opposite charges attract and like charges repel, which significantly enhances ion penetration. Positive lidocaine ions, for instance, are drawn to the cathode and repelled from the anode. Comparably, negative iodothuridine ions are drawn to the anode and repelled from the cathode [4]

The following are the features of iontophoresis process for local therapy:
Many medications with low penetration qualities such as high molecular weight electrolytes like proteins, peptides, and oligonucleotides, which are often difficult to supply other than the parenteral route, have utilized in this method’s potential for transdermal administration. Iontophoresis has demonstrated a significant penetration of bigger peptides such as insulin for which there have been a number of iontophoretic studies with hardly any report demonstrating that iontophoresis can even reach human insulin’s baseline levels in vivo [7].
Historical Background of Iontophoretic Process:
The term "iontophoresis," which comes from the Greek words "ionto," which means "ion," and "phoresis," which means "to bear," refers to a technique that uses a small amount of electricity to enhance the number of ionized molecules that can enter or flow through tissue. The use of electricity in clinical settings dates back to the Greek civilization’s golden age and was most likely by Varatti in 1747 [8]. Important contributions were made by the French physician Bernard Raymond Fabre Palaprat (1773-1833) [9]. Using his own arm, Samuel George Morton (1799-1851) performed an experiment in which he applied electric current after connecting graphite powder to a positively charged electrode [10]. Benjamin Ward Richardson, acknowledged as the "father of dental iontophoresis" (1828–1896), found the "voltaic narcotism," a method for oral anaesthetic delivery. In the 1870s, the German Hermann Munk (1839-1912) performed experiments with primitive equipment laid the ground work for the subsequent discoveries of proteins and processes of active transport in biological membranes in the 20th century. The mid-18th century saw the first suggestion for the use of electric current in medicine administration. In the 19th century, significant advancements were made, most notably by William James Morton (1846–1920). During the time of Stephen Leduc (1853–1939) and Fritz Frankenhausener (1868), attempts were made to administer metal ions in addition to alkaloids. Before 1908, Frankenhausener is credited with coining the word “iontophoresis” [11]. Today, the treatment of hyperhidrosis is the most successful and popular applications of iontophoresis in dermatological medication (Sloan JB et al., 1986). The first commercial devices are available in the market (Kalia et al., 2004) [12]. Behar-Cohen et al. assessed the use of iontophoresis in rats receiving parenteral delivery of dexamethasone in combination with ocular application of the medication [13]. On rabbit corneas, gentamicin sulfate and iontophoresis were evaluated by Frucht-Pery et al [14]. In place of analyzing endogenous chemicals to diagnose renal failure, Wascotte et al. employed reverse iontophoresis, which collects material via the skin, and correlated this with blood sample [15].
Basic Principles of Iontophoresis:
Basic principles:
Iontophoresis is a fascinating procedure that facilitates the transfer of charged and uncharged molecules over the skin by means of a small, specified electric current. Three fundamental components make up an iontophoretic system:

Figure 1. Schematic representation of iontophoretic process
The reservoirs may only contain saline or buffer when using reverse iontophoresis for clinical monitoring. The current source drives electronic current to the active reservoir, where it is converted into ionic current, when the active and indifferent reservoir systems are applied to the skin. Ionic current travels via the active reservoir, the skin, the indifferent reservoir underneath the skin, and back through the skin into the indifferent reservoir. It is converted back into electronic current at the indifferent reservoir, finishing the circuit at the current source's opposite pole. An electrode with a defined charge repels a substance that is attracted to an oppositely charged electrode that is positioned elsewhere on the body. Therefore, a positively charged medication or ion in solution, an electronic device to control the current, an anode reservoir system (with the anode electrode), and a cathode reservoir system (with the cathode electrode) make up an anodal iontophoretic device. The cathode is applied to a different area of the skin than the positively charged medication, which is placed in the anode reservoir system at the intended application site. All cations, including the positively charged medication, migrate into the skin and away from the anode when an electric current is applied. In parallel, the body's negatively charged ions flow from the body into the donor reservoir [17]. An anodal iontophoretic system is shown in Fig 2
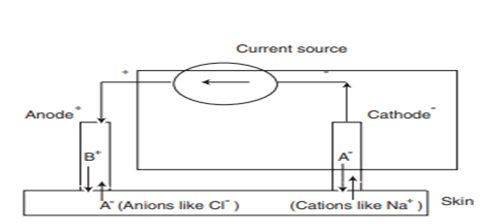
Figure 2. An anodal iontophoretic process
Electrode system in iontophoresis:
The form and shape of the electrodes that are selected should conform nicely to the skin's surface and cause the least amount of pH changes in the skin. Silver/Silver chloride (Ag/AgCl) electrodes have been commonly used in iontophoretic systems. The silver present at the anode oxidizes and reacts with chloride ions to form insoluble AgCl. As of right now, the AgCl at the cathode gets reduced to Ag+ and releases the Cl- .The reactions do not involve the electrolysis of water [18].
Types of electrodes:
Electrodes have a small chamber covered by a semipermeable membrane into which ionised solution may be injected [19]
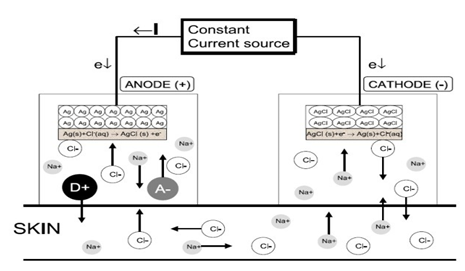
Figure 3. Iontophoresis and Drug Delivery
Transport Mechanisms:
Abramson and Gorin derived an equation to compare the iontophoresis flux due to electric mobility, electroosmosis and simple diffusion. The increased flux during iontophoresis would include:
Jionto = Jelectric + Jpassive + Jconvective
Jelectric –The flux due to electric current application;
Jpassive – The flux due to passive delivery through the skin; and
Jconvective - The flux due to convective transport due to electro osmosis. The total flux of a solute (JI) across the skin during iontophoresis is the sum of electro-migration (JEM), electro-osmotic (JEO), and passive diffusion (JP) contributions [20].
JI = JEM + JEO + JP
According to Faraday’s law, the electro-migration flux of each ion in the iontophoretic circuit at steady state is given by
JEM=ti * IF * Zi

Where, ti is the transport number, and zi is the valence of ith ion, F the Faraday’s constant and I is the total current. The transport number depends on the ion’s relative mobility (µi) and charge, and upon its concentration (ci) relative to those of the other ions present:
ti=ci*zi*uii=1n(cj*zj*uj)
Since the saline is the primary extracellular electrolyte that the body contains in large quantities, Na+ and Cl- ions always carry the majority of the current during in vivo iontophoresis. High molecular weight cations and uncharged compounds are mostly transported by electroosmosis. Because of its negative charge at physiological pH, the skin functions as a cation- selective membrane [21]. Neutral molecules are carried in the anode to cathode direction by an electro osmotic solvent flow caused by the preferred passage of counterions. The potential gradient created by the electric field is proportional to the volume flow v (volume * time −1 * area −1).
v=Lve*-d∅dx
Where Lve


JEO=v*cj

At pH 7, electroosmosis slows the transit of anions while facilitating the transport of high molecular weight cations. It can be changed by adjusting the membrane's permselectivity and adjusting the formulation in the electrode chambers. For small ions such as Na+ or Cl-, electromigration dominates; on the other hand, neutral solutes are transported only by electro-osmosis and passive diffusion [23

Figure 4.Transport mechanisms of iontophoresis
Pathways Of Molecular Transport In Iontophoresis:
The application of current can also create changes in the permeability and create new pathways for drug permeation. Although there are three routes for a drug to permeate through the skin:

Figure 5. Pathways of Molecular Transport in iontophoresis
Types Of Iontophoretic System:
The system of drug delivery via iontophoresis can be classified in accordance to the modification and improvement done in this system which allows the uniform and predictive drug release in an effective manner. The types are:
Factors Affecting Iontophoretic Delivery System:
ADVANTAGES:
DISADVANTAGES:
Applications:
Table 1: Drugs used in iontophoresis treatment
|
S. No |
Name of the drug |
Class of the drug |
Trade name |
Use/ Indication |
|
1. |
Lignocaine along with epinephrine |
Local anaesthetic |
Akten, Lignospan forte, Oraqix, Zingo |
To reduce pain |
|
2. |
Dexamethasone phosphate |
Steroid |
Dalalone, Dexasone, Dexacen, Dexamethasone solurex |
For the treatment of uveitis and other inflammatory eye conditions |
|
3. |
Fentanyl HCl |
Opioid |
Ionsys |
Ensures patient controlled analgesia in acute and moderate to severe postoperative pain |
|
4. |
Ketoprofen |
Non-steroidal anti-inflammatory drugs (NSAIDs) |
Orudis, Orudis KT, Oruvail, Alrhumat and Kefenid |
Increased drug retention in skin and has potential in topical therapy of musculoskeletal diseases |
|
5. |
Celecoxib |
NSAIDs |
Celebrex |
Used to treat osteoarthritis, acute pain, joint inflammation and joint injuries |
|
6. |
Ciprofloxacin |
Fluoroquinolones |
Ciloxan, Ciproxin, Cetraxal, Cipro, Proquin |
Delivery into the aqueous humour for the treatment of intraocular infections |
|
7. |
Terbinafine |
Anti-fungal agent |
Lamisil and Terbinex |
Provides fungicidal activity against dermatophytes, moulds and dimorphic fungi |
|
8. |
Acyclovir |
Anti-viral agent |
Zovirax |
Used in the treatment of herpes simplex and Varicella zoster virus infections |
|
9. |
Cisplatin |
Anti- cancer agent |
Cisplatinum, Platamin, Neoplatin, Cismaplat |
Used to treat skin basal cell and squamous cell carcinoma |
Various Synergistic Approaches with Iontophoresis:
Patents For Iontophoresis:
India has seen a range of patents filled for iontophoresis applications, particularly in therapeutic and medical contexts.
Table 2: Patents for iontophoresis
|
Title |
United states patent |
Issued |
Inventors |
Assignee |
Application number |
Filed |
|
Iontophoretic electrode device, method and gel insert |
4,383,529 |
May 17, 1983 |
Henry L. Webster, Providence, Utah |
Wescor, Inc.,Logan, Utah |
202,889 |
Nov 3, 1980 |
|
Wireless iontophoresis pad and controller |
0266005 |
August 25 ,2022 |
Anton Sabiev, Forest Hills, NY (US), William Bauman, New Rochelle NY (US), Mark Korsten, Hastings- on-Hudson NY (US) |
William Bauman |
17/36,602 |
May 4, 2022 |
|
Iontophoretic delivery device with integrating hydrating means |
6,223,075 |
April 24, 2001 |
Jon E.Beck, Lindsay B. Lloyd, Tomasz J. Petelenz |
Iomed, Inc., |
08/762,051 |
Dec 9, 1996 |
|
Device and method for corneal delivery of riboflavin by iontophoresis for the treatment of keratoconus |
9,700,456 B2 |
Jul.11,2017 |
Fulvio Foschini, Pierre Roy, Edoardo Stagni, Giovanni Cavallo, Giulio Luciani |
Sooft Italia spa |
13/824,850 |
Jan.12, 2011 |
|
Stabilized interface for iontophoresis |
5,837,281 |
Nov 17, 1998 |
Katsumi Iga, Masafumi Misaki Keiichiro Okabe, Emi Kyo |
Takeda chemicals industries, Ltd., Advance Co., Ltd., Teikoku Hormone Mfg. Co., Ltd., |
614,375 |
March 12, 1996 |
|
Iontophoresis patch equipped with donor gel and reference gel |
20120310143A1 |
June 12, 2012 |
Yaegashi, Mitsutoshi, Hasui, Akihiro, Kubo, Hiroyuki |
Yaegashi, Mitsutoshi |
13/578,168 |
Feb. 09, 2012 |
CONCLUSION:
Iontophoresis is a word which is derived from the Greek “ionto” represents “ions” and “phoresis” represents “to bear”. Iontophoresis refers to a non-invasive technique that uses a small amount of electricity to enhance the number of ionized molecules that can enter or flow through tissue. It is a technique which represents for delivering drugs through the skin, offering a range of clinical applications from treating hyperhidrosis to enhancing the delivery of analgesics and anti-inflammatory agents. This method is utilized to deliver the high molecular weight substances like peptides, oligonucleotides etc. Its advantages include controlled, localized drug administration and reduced systemic side effects compared to traditional methods. It also by passes the first pass metabolism and gastric tract effects. It also offers patients compliance. However challenges such as skin irritation, variability in patient response, and limitations in drug types suitable for iontophoretic delivery remain areas for further research. Further advancements in electrode design, drug formulations, and personalized protocols could improve efficacy, safety, and patient outcomes, potentially broadening the utility of iontophoresis
REFRENCES

Dr. B. V. Ramana*, Yakkanti Anjani, Shaik Farooq, Bandi Likhitha, Iontophoresis: Principle and Its Applications, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 477-488. https://doi.org/10.5281/zenodo.14992676
 10.5281/zenodo.14992676
10.5281/zenodo.14992676
