Matoshri College of Pharmacy, Ekhlahare Nashik.
Rebelliousness with immunosuppressive meds, after renal transplantation is accepted to be a significant reason for allograft dismissal and unite misfortune, with the great expenses of these specialists, thought about a huge justification for resistance. Our motivation was to decide the consistency paces of renal transfer patients who accepted their immunosuppressant treatment for nothing and assess their examples of consistency.All patients who got a renal transfer and accepted their immunosuppressant drugs at our foundation for their most memorable year post-transplant were remembered for the review. The consistency rate was determined, and serum immunosuppressant focuses were used to approve consistency appraisals.Estimation of non-adherence risk factors: We investigated non-adherence risk factors from each of the five elements of the WHO characterization of non-adherence risk factors. The dependability of all multi-thing instruments was inspected by the leading head part investigation to decide variable gathering and by computing Cronbach's ? values on the subsequent subscales. (Sub-)scale scores were determined by averaging thing scores.Financial variables recovered from clinical documents were age (years), orientation and ethnicity; those evaluated by organized interview were living alone/together, work status, saw sufficiency of one's monetary circumstance to take care of drug costs (on a four-direct scale from all that could be needed toward insufficient cash), and instructive level (on a four-point scale mirroring the age until which patients went to class — until 11/12, 14/15, 18/19 years, or more established). Gotten social help with medicine taking was surveyed utilizing an 8-thing scale that scored how frequently in the previous month a patient got social help from others (for example somebody helped set up the medicine.
Transplantation is the last choice to treat the disappointment of the kidney—the kidney of a solid person who can match the patient. The human body tends to go against the outer specialist which enters the body. When the outer specialist recognizes the body's safe framework gets activated, it can cause serious outcomes in the body after the kidney relocates to stay away from these results Immunosuppressive medicine is recommended to the patient after the trasplantation. In this article, we will take note of the historical backdrop of kidney transplantation, the system it follows, a few hints that will help the patient, drugs that go about as immunosuppressants the complexities that are confronted, and toward the end a few inquiries which their responses which are found in the wake of cooperating with a patient went through kidney transplantation.The reason for the audit is to achieve earth-shattering quality kidney relocation and express adherence to immunosuppressive drugs.The principal effective kidney relocation was acted in 1954 by a group including Joseph Murray, the beneficiary's specialist, and Hartwell Harrison, the specialist for the contributor. Murray was granted a Nobel Prize in Physiology or Medication in 1990 for this and other work.Kidney disappointment, otherwise called end-stage kidney sickness, happens when the kidneys are not ready to eliminate squander from your blood and control the degree of liquid in your body enough. Kidney disappointment can happen unexpectedly or continuously. Individuals with kidney disappointment need dialysis or a kidney relocation to remain alive.Dialysis is a treatment for individuals whose kidneys are coming up short. When you have kidney disappointment, your kidneys don't channel blood how they ought to Subsequently, squanders and poisons develop in your circulation system. Dialysis is crafted by your kidneys, eliminating side effects and overabundance of liquid from the blood.
History
Fig (1): Dr. John P. Merrill (left) explains the workings of a then-new machine called an artificial kidney to Richard Herrick (middle) and his brother Ronald (right).
Perhaps the earliest notice about the chance of a kidney relocates was by American clinical scientist Simon Flexner, who pronounced in a perusing of his paper on "Propensities in Pathology" in the College of Chicago in 1907 that it would be conceivable in the then-future for sick human organs replacement for sound ones by a medical procedure, including conduits, stomach, kidneys, and heart(1).In1933, specialist Yuriy Vorony from Kherson in Ukraine endeavored to the primary human kidney relocation, utilizing a kidney eliminated six hours sooner from a departed contributor to be reimplanted into the thigh. He estimated kidney capability utilizing an association between the kidney and the skin. His most memorable patient kicked the bucket two days after the fact, as the joint was incongruent with the beneficiary's blood bunch and was rejected.It was only after 17 June 1950, that an effective transfer was performed on Ruth Exhaust, a 44-year-elderly person with a polycystic kidney infection, by Dr. Richard Lawler at Little Organization of Mary Clinic in Evergreen Park, Illinois. Albeit the given kidney was dismissed ten months after the fact because no immunosuppressive treatment was accessible at that point, the mediating time gave Exhaust's excess kidney time to recuperate and she experienced another five years(2). Dr. John P. Merrill (left) makes sense of the functions of a then-new machine called a fake kidney to Richard Herrick (center) and his sibling Ronald (right). The Herrick twin siblings were the subjects of the world's most memorable fruitful kidney relocation, Ronald being the contributor.A kidney relocation between living patients was embraced in 1952 at the Necker medical clinic in Paris by Jean Cheeseburger, albeit the kidney bombed after three weeks. The main effective transfer of this sort happened in 1954 in Boston. The Boston transplantation, performed on 23 December 1954 at Brigham Emergency Clinic, was performed by Joseph Murray, J. Hartwell Harrison, John P. Merrill, and others. The technique was finished between indistinguishable twins Ronald and Richard Herrick which diminished issues of a resistant response. For this and later work, Murray got the Nobel Prize for Medication in 1990. The beneficiary, Richard Herrick, kicked the bucket eight years after the transplantation because of inconveniences with the giver's kidney that were inconsequential to the transplant(3).In 1955, Charles Loot, and William James "Jim" Dempster (St Marys and Hammersmith, London) did the principal expired giver relocate to Joined Realm, which was unsuccessful.[citation needed] In July 1959, "Fred" Peter Raper (Leeds) played out the first fruitful (8 months) perished contributor relocate in the UK. After a year, in 1960, the principal fruitful living kidney relocation in the UK happened, when Michael Woodruff performed one between indistinguishable twins in Edinburgh(4).In November 1994, the Ruler Qaboos College Medical Clinic, in Oman, performed effectively the world's most youthful cadaveric kidney relocation. The work occurred from an infant of 33 weeks to a 17-month-old beneficiary who made due for a long time (because of the several organs relocated into him)(5).Until the standard utilization of medicine to forestall and treat intense dismissal, presented in 1964, perished giver transplantation was not performed. The kidney was the least demanding organ to relocate: tissue composing was straightforward; the organ was generally simple to eliminate and embed; live contributors could be utilized without trouble; and in case of disappointment, kidney dialysis was accessible from the 1940s. As made sense in Thomas Starzl's 1992 journal, these elements make sense why Starzl's group and others started with kidney transplantation as the primary sort of strong organ transplantation to mean clinical practice before endeavoring to continue toward liver transplantation, heart transplantation, and different kinds.The significant boundary to organ transplantation between hereditarily non-indistinguishable patients lay in the beneficiary's resistant framework, which would regard a relocated kidney as a 'non-self' and right away or constantly reject it. Hence, having a prescription to stifle the resistant framework was fundamental. Nonetheless, stifling a singular's safe framework puts that person at a more serious gamble of contamination and malignant growth (especially skin disease and lymphoma), notwithstanding the symptoms of the meds. Kidney disappointment, otherwise called end-stage renal illness (ESRD), is an ailment wherein the kidneys can never again channel side effects from the blood, working at under 15% of typical levels. Kidney disappointment is named either intense kidney disappointment, which grows quickly and may determine; and persistent kidney disappointment, which grows gradually and can frequently be irreversible.(6) Side effects might incorporate leg expansion, feeling tired, spewing, loss of hunger, and confusion. Complexities of intense and ongoing disappointment incorporate uremia, hyperkalemia, and volume overload. Difficulties of constant disappointment likewise incorporate coronary illness, hypertension, and anemia.Reasons for intense kidney disappointment include low circulatory strain, blockage of the urinary lot, certain drugs, muscle breakdown, and hemolytic uremic syndrome.[2] Reasons for constant kidney disappointment include diabetes, high pulse, nephrotic disorder, and polycystic kidney disease. Finding intense disappointment is much of the time in light of a mix of elements, for example, diminished pee creation or expanded serum creatinine. Determination of persistent disappointment depends on a glomerular filtration rate (GFR) of under 15 or the requirement for renal substitution therapy. It is likewise identical to arrange 5 constant kidney disease.Therapy of intense disappointment relies upon the basic cause. Therapy of constant disappointment might incorporate hemodialysis, peritoneal dialysis, or a kidney transplant. Hemodialysis utilizes a machine to channel the blood outside the body. In peritoneal dialysis, the explicit liquid is put into the stomach hole and afterward depleted, with this cycle being rehashed on various occasions per day. Kidney transplantation includes precisely setting a kidney from another person and afterward taking an immunosuppressant prescription to forestall rejection(7). Other suggested measures for persistent sickness incorporate remaining dynamic and explicit dietary changes. Misery is likewise normal among patients with kidney disappointment and is related to unfortunate results including a higher gamble of kidney capability decline, hospitalization, and demise. A new PCORI-financed investigation of patients with kidney disappointment getting short-term hemodialysis tracked down comparable viability among nonpharmacological and pharmacological medicines for depression. In the US, intense disappointment influences around 3 for every 1,000 individuals a year. Ongoing disappointment influences around 1 out of 1,000 individuals with 3 for every 10,000 individuals recently fostering the condition each year. Intense disappointment is much of the time reversible while constant disappointment frequently is not. With proper therapy numerous with persistent sickness can proceed working.The reason for most immunosuppressive regimens is prednisolone, a corticosteroid. Prednisolone smothers the invulnerable framework, however, its drawn-out use at high dosages causes a huge number of incidental effects, including glucose prejudice and diabetes, weight gain, osteoporosis, muscle shortcoming, hypercholesterolemia, and waterfall development. Only prednisolone is generally insufficient to forestall the dismissal of a relocated kidney. Consequently, other, non-steroid immunosuppressive specialists are required, which additionally permit lower portions of prednisolone. These include: azathioprine Kidney disappointment, otherwise called end-stage renal sickness (ESRD), is an ailment wherein the kidneys can never again enough channel side-effects from the blood, working at under 15% of typical levels. Kidney disappointment is named either intense kidney disappointment, which grows quickly and may determine; and persistent kidney disappointment, which grows gradually and can frequently be irreversible. Side effects might incorporate leg enlarging, feeling tired, spewing, loss of hunger, and confusion. Inconveniences of intense and constant disappointment incorporate uremia, hyperkalemia, and volume overload. Difficulties of ongoing disappointment likewise incorporate coronary illness, hypertension, and anemia. Reasons for intense kidney disappointment include low pulse, blockage of the urinary lot, certain meds, muscle breakdown, and hemolytic uremic syndrome. Reasons for persistent kidney disappointment include diabetes, highpulse, nephrotic condition, and polycystic kidney disease. Determination of intense disappointment is much of the time in light of a mix of elements, for example, diminished pee creation or expanded serum creatinine. The finding of persistent disappointment depends on a glomerular filtration rate (GFR) of under 15 or the requirement for renal substitution therapy. It is likewise comparable to arranging 5 constant kidney diseases(7).Therapy of intense disappointment relies upon the basic cause. Therapy of constant disappointment might incorporate hemodialysis, peritoneal dialysis, or a kidney transplant. Hemodialysis utilizes a machine to channel the blood outside the body. In peritoneal dialysis, the explicit liquid is set into the stomach cavity and afterward depleted, with this cycle being rehashed on various occasions per day. Kidney transplantation includes precisely putting a kidney from another person and afterward taking an immunosuppressant prescription to forestall rejection. Other suggested measures for persistent illness incorporate remaining dynamic and explicit dietary changes. Sorrow is likewise normal among patients with kidney disappointment, and is related to unfortunate results including a higher gamble of kidney capability decline, hospitalization, and demise. A new PCORI-subsidized investigation of patients with kidney disappointment getting short-term hemodialysis tracked down comparable viability among nonpharmacological and pharmacological medicines for depression.
In the US, intense disappointment influences around 3 for every 1,000 individuals a year.Constant disappointment influences around 1 out of 1,000 individuals with 3 for every 10,000 individuals recently fostering the condition each year. Intense disappointment is much of the time reversible while persistent disappointment frequently is not. With proper therapy, numerous with ongoing illnesses can proceed to work and mycophenolate, ciclosporin, and tacrolimus.(12)(13).
Kidney Failure
Kidney disappointment, otherwise called end-stage renal sickness (ESRD), is an ailment wherein the kidneys can never again channel side effects from the blood, working at under 15% of typical levels(16). Kidney disappointment is named either intense kidney disappointment, which grows quickly and may determine; and persistent kidney disappointment, which grows gradually and can frequently be irreversible. Side effects might incorporate leg enlarging, feeling tired, spewing, loss of hunger, and confusion. Inconveniences of intense and constant disappointment incorporate uremia, hyperkalemia, and volume overload. Difficulties of ongoing disappointment likewise incorporate coronary illness, hypertension, and anemia.Reasons for intense kidney disappointment include low pulse, blockage of the urinary lot, certain meds, muscle breakdown, and hemolytic uremic syndrome. Reasons for persistent kidney disappointment include diabetes, highpulse, nephrotic condition, and polycystic kidney disease. Determination of intense disappointment is much of the time in light of a mix of elements, for example, diminished pee creation or expanded serum creatinine. The finding of persistent disappointment depends on a glomerular filtration rate (GFR) of under 15 or the requirement for renal substitution therapy. It is likewise comparable to arranging 5 constant kidney diseases. Therapy of intense disappointment relies upon the basic cause. Therapy of constant disappointment might incorporate hemodialysis, peritoneal dialysis, or a kidney transplant(16). Hemodialysis utilizes a machine to channel the blood outside the body. In peritoneal dialysis, the explicit liquid is set into the stomach cavity and afterward depleted, with this cycle being rehashed on various occasions per day(16). Kidney transplantation includes precisely putting a kidney from another person and afterward taking an immunosuppressant prescription to forestall rejection. Other suggested measures for persistent illness incorporate remaining dynamic and explicit dietary changes.(16) Sorrow is likewise normal among patients with kidney disappointment, and is related to unfortunate results including a higher gamble of kidney capability decline, hospitalization, and demise(16). A new PCORI-subsidized investigation of patients with kidney disappointment getting short-term hemodialysis tracked down comparable viability among nonpharmacological and pharmacological medicines for depression.In the US, intense disappointment influences around 3 for every 1,000 individuals a year. Constant disappointment influences around 1 out of 1,000 individuals with 3 for every 10,000 individuals recently fostering the condition each year. Intense disappointment is much of the time reversible while persistent disappointment frequently is not. With proper therapy, numerous with ongoing illness can proceed to work.(18)
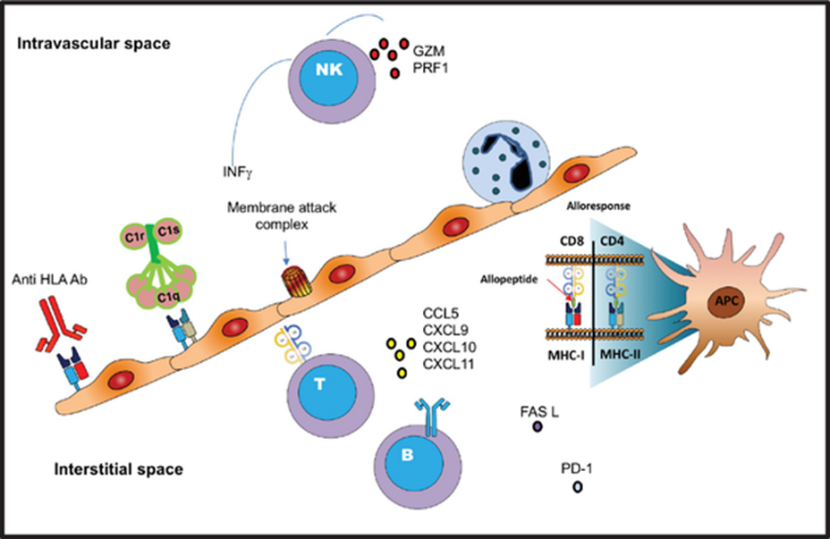
Fig (2): Mechanism Of Kidney Failure
Signs And Side Effects
Side effects can shift from one individual to another. Somebody in the beginning phase of kidney illness may not feel wiped out or see side effects as they happen. At the point when the kidneys neglect to channel appropriately, squander collects in the blood and the body, a condition called azotemia. Extremely low degrees of azotemia might deliver scarcely any, side effects. Assuming the illness advances, side effects become observable (if the disappointment is of adequate degree to cause side effects). Kidney disappointment joined by recognizable side effects is named uremia.
Side effects of kidney disappointment incorporate the following:
•Elevated degrees of urea in the blood, which can result in:
•Retching or looseness of the bowels (or both) that might prompt drying out
•Sickness
•Weight reduction
•Nighttime pee (nocturia)
•More regular pee, or in more noteworthy sums than expected, with pale pee
•Less continuous pee, or in more modest sums than expected, with dull-shaded pee
•Blood in the pee
•Strain or trouble peeing
•Surprising measures of pee, typically in huge amounts
•A development of phosphates in the blood that unhealthy kidneys can't sift through may cause:
•Tingling
•Bone harm
•Nonunion in broken bones
•Muscle cramps (brought about by low degrees of calcium which can be related to hyperphosphatemia)
•A development of potassium in the blood that sick kidneys can't sift through (called hyperkalemia) may cause:
•Unusual heart rhythms
•Muscle paralysis
•Disappointment of kidneys to eliminate abundance liquid might cause:
•Enlarging of the hands, legs, lower legs, feet, or face
•Windedness because of additional liquid on the lungs (may likewise be brought about by frailty)
•Polycystic kidney sickness, which causes enormous, liquid-filled growths on the kidneys and some of the time the liver, can cause:
•Torment toward the back or side
•Solid kidneys produce the chemical erythropoietin that animates the bone marrow to make oxygen-conveying red platelets. As the kidneys fall flat, they produce less erythropoietin, bringing about diminished creation of red platelets to supplant the normal breakdown of old red platelets. Thus, the blood conveys less hemoglobin, a condition known as paleness. This can result in:
•Feeling drained or frail
•Memory issues
•Trouble concentrating
•Discombobulation
•Low pulse
•Ordinarily proteins are too huge to even consider going through the kidneys. Anyway, they can go through when the glomeruli are harmed. This doesn't cause side effects until broad kidney harm has occurred, after which side effects include:
•Frothy or effervescent pee
•Expanding in the hands, feet, mid-region, and face
•Different side effects include:
•Hunger misfortune, which might remember a terrible preference for the mouth
•Trouble dozing
•Obscuring of the skin
•Overabundance of protein in the blood
•With high dosages of penicillin, individuals with kidney disappointment might encounter seizures
Kidney Dialysis
Kidney dialysis (from Greek δι?λυσις, dialysis, 'disintegration'; from δι?, dia, 'through', and λ?σις, lysis, 'releasing or parting') is the most common way of eliminating abundance water, solutes, and poisons from the blood in individuals whose kidneys can never again carry out these roles normally. This is alluded to as renal substitution treatment. The principal fruitful dialysis was acted in 1943. Dialysis might be started when there is an unexpected quick loss of kidney capability, known as intense kidney injury (recently called intense renal disappointment), or when a continuous decrease in kidney capability, constant kidney disappointment, arrives at stage 5. Stage 5 constant renal disappointment is reached when the glomerular filtration rate is under 15% of the ordinary, creatinine leeway is under 10 mL each moment, and uremia is present(10).Dialysis is utilized as a brief measure in either intense kidney injury or in those anticipating kidney relocation and as an extremely durable measure in those for whom a transfer isn't shown or not possible.(9) In Western European nations, Australia, Canada, the Assembled Realm, and the US, dialysis is paid for by the public authority for qualified people.(35)(36)
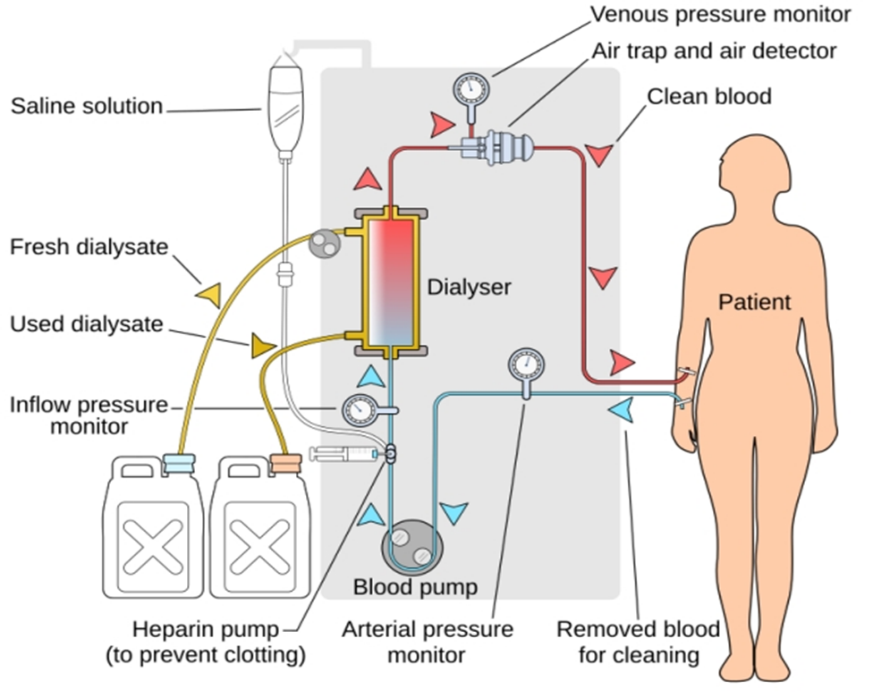
Fig( 3) : Dailysis
TIPS - To take care after transplantation
Prescription After Kidney Relocate(47)
The meds you will be taking after your transfer to hold your body back from dismissing your new kidney are called immunosuppressants. You should accept these medications consistently however long you have your transfer. At times even after a transfer quits working, we suggest staying on small dosages of these medications to forestall immune response development. This will make you bound to have another viable transfer later.
Various immunosuppressants can be utilized. You won't be taking these drugs however will be on a mix of them. Every one of them makes expected side impacts, yet recollect that not all patients experience the ill effects of the multitude of aftereffects recorded.
Prograf (FK506) - is required two times per day. The results of this medication incorporate cerebral pain, hand quakes, queasiness, loose bowels, hypertension, expanded glucose and potassium, and diminished magnesium. Prograf can likewise hurt your kidneys over the long run. The dosing of this medication depends on how much medication is in your blood. You should accept care to portion it 12 hours separately and have your blood tests done not long before your morning portion.
Cyclosporine - is required two times every day. The results of this medication incorporate hypertension, gentle handquakes, cerebral pain, and expanded development of hair. Cyclosporine can likewise hurt your kidneys over the long run. You should accept care to portion it 12 hours separately and have your blood tests done not long before your morning portion.
Rapamune (Sirolimus) - is required once a day toward the beginning of the day. The symptoms of this medication are lower leg enlarging, stomach torment, queasiness, runs or stoppage, joint hurts, fever, cerebral pain, hypertension, sickliness, and elevated cholesterol and fatty substance levels. Blood levels are additionally estimated for this medication so blood tests ought to be finished before your morning portion.
Cellcept - is required two to four times each day. The results of this medication are looseness of the bowels, queasiness, spewing, rash, and low white platelet count with an expanded risk for contamination.
Prednisone - is taken for a couple of days following your transfer. A few patients will experience the ill effects of trouble resting or may feel "hyper". These sentiments will pass in a couple of days. A few patients should be on prednisone long haul. The choice to utilize prednisone will be founded on the sort of kidney sickness you have and your gamble for dismissal. The significant results of long-haul prednisone are expanded hunger, stomach ulcers, osteoporosis, diabetes, waterfalls, state of mind swings, and Cushing's condition. Cushing's condition incorporates round cheeks, projecting mid-region, fat stores over the upper back, skin inflammation, and expanded development of facial and body hair. Most patients are not on sufficiently high dosages to experience the ill effects of these aftereffects, and these secondary effects will diminish or vanish as the portion is diminished. All the immunosuppressant drugs recorded above work to attempt to keep your insusceptible framework from dismissing your relocated organ. This additionally implies that they make it harder for your insusceptible framework to battle microorganisms, infections, and disease cells. This puts you at a higher gamble for contamination and disease. You should accept anti-toxins for the initial three to a half years after your transfer sto assist with forestalling disease. You should have customary physicals with your essential consideration specialist for disease screening including evaluating for skin malignant growth which is the most widely recognized post-relocate disease.Not with standing the immunosuppressants and anti-toxins, you may likewise have to take different medications to treat hypertension, diabetes, or different circumstances. It is entirely expected for patients to return home on ten to twelve distinct prescriptions after their transfer. You should be focused on taking your medications and following your physician's instructions for any changes.
Complexities Related to the Utilization of Immunosuppressive Medications
Immunosuppressive medications are fundamental for relocation capability, however as referenced above, they can prompt a wide assortment of multi-organ problems and illnesses that cause mortality, including cardiovascular issues. Important post-relocate diabetes, hypertension, and hyperlipidemia are among the huge confusions brought about by immunosuppressive medications. Consequently, it is fitting to restrict, if conceivable, the utilization of glucocorticoids. Furthermore, the avoidance and treatment of pallor are likewise significant. For this situation, vitamin D supplementation, treatment with folic corrosive, vitamin B6 and B12, and the utilization of calming and cell reinforcement medications can be remembered for the treatment of kidney relocation beneficiaries. What's more, a sound way of life, including smoking suspension, a solid eating regimen, and, in particular, active work are key elements in diminishing cardiovascular gambling.Malignant growth is the second most normal reason for death in kidney-related patients. These tumors primarily incorporate renal cell carcinoma and skin malignant growth. Contrasted with everybody, kidney relocation beneficiaries have a place with a gathering of patients with a higher gamble of creating renal cell carcinoma. Around the vast majority of renal cell carcinomas are accepted to foster solid kidneys. Nonetheless, the frequency of renal cell carcinoma in a relocated kidney is uncommon and is assessed to be around 0.1%. Skin malignant growth is the most well-known and forceful sort of disease in kidney relocation beneficiaries. The most often detailed skin diseases in the previously mentioned gathering of patients incorporate cutaneous squamous cell carcinoma, basal cell carcinoma, Kaposi's sarcoma, and harmful melanoma. Even though Kaposi's sarcoma is an uncommon disease, its occurrence in relocated beneficiaries is more than multiple times higher than in everybody. Significantly, kidney relocation beneficiaries treated with calcineurin inhibitors are at outstanding gamble for Kaposi's sarcoma. Concerning skin disease, melanoma is likewise a much of the time detailed malignant growth. If the previously mentioned malignant growth is analyzed, the transformation of a CsA or Tac-based immunosuppressive routine to a mTOR inhibitor is by all accounts the ideal arrangement with clear beneficial outcomes. As referenced in this audit, the decision of immunosuppressive treatment is essential and ought to be individualized for every patient given illness etiology and unit capability.One or more complexity related to the utilization of immunosuppressive medications is viral diseases. Epstein-Barr infection (EBV) is a human herpesvirus tainting roughly 90% of grown-ups. The previously mentioned infection can show asymptomatic viremia, irresistible mononucleosis condition, or inclusion of different organs, like hepatitis, myocarditis, and pancreatitis. The most suggestive diseases in kidney relocated beneficiaries are essential contaminations, Which are likely connected with the reactivation of the benefactor infection. The most ridiculously troubling appearance of EBV is post-relocate lymphoproliferative sickness.Furthermore, cytomegalovirus (CMV) is a typical infection in kidney-relocated beneficiaries. The gamble of CMV contamination relies fundamentally upon the CMV serological status of the benefactor and beneficiary. Concerning immunosuppressive medications, belatacept is related to an expanded gamble of essential CMV disease and a drawn-out course of viral replication in patients at a high gamble of CMV contamination. Additionally, BK polyomavirus and norovirus are likewise confusions that happen after organ transplantation. Essential contamination with BK polyomavirus happens in adolescence, and 80-90% of grown-ups are exposed to it. The infection stays dormant in the renal tubules and uroepithelium, while norovirus in immunocompromised patients can create ongoing norovirus diseases related to repetitive and repeating episodes of watery runs that can endure from months to years. Because of the properties of immunosuppression, which relocation beneficiaries should continually apply, the previously mentioned gathering of patients is very powerless against bacterial contaminations. Urinary plot diseases of different aetiologies are the most widely recognized contamination in kidney relocation beneficiaries. They happen most often in the main year after transplantation, and the rate goes from 7% to 8%. Gram-negative microorganisms cause up to 90% of cases, and Escherichia coli was the most regularly detailed. Disease with C. difficile is multiple times more probable in hospitalized strong organ relocate beneficiaries contrasted with everyone.Intrusive parasitic contaminations represent a danger to kidney-relocated beneficiaries. Contagious contaminations in emerging nations essentially affect patient and unite endurance. Kidney relocation beneficiaries are in danger of contagious diseases predominantly in the early period after medical procedures. The most widely recognized contagious contaminations are brought about by growths of the Candida class and can be supplanted by additional harmless diseases with endemic mycoses, for example, mucormycosis, histoplasmosis, blastomycosis, and coccidioidomycosis.
Concentrate on Populace
This cross-sectional review was completed at the Facility of Nephrology, Clinical Center Niš, Serbia. Every one of the 63 KTPs going to follow-up visits from January to April 2013 was drawn nearer for consideration in the review. Consideration measures were: no less than 18 years; (42) kidney transplantation no less than 1 year already; (21) immunosuppressant treatment (Tac, CsA, or Sir) for 1 back-to-back year, and being the beneficiary of only one renal transfer at the hour of study enlistment. The reasons for end-stage kidney sickness were: constant glomerulonephritis (n = 37), persistent pyelonephritis (n = 16), and diabetic nephropathy (n = 7). All patients were on immunosuppressive treatment. Notwithstanding immunosuppressants, they were taking mycophenolate mofetil and prednisone. The review was supported by the Morals Panel of the Staff of Medication, College of Niš. Informed assent was acquired from all members, support in the review was deliberate and the data was dealt with privately. Kidney transplantation is the ideal treatment for end-stage renal illness. The future of relocated patients is essentially worked on contrasted with that old enough paired stand-by recorded patients on dialysis. Even though kidney transplantation drags out life and works on personal satisfaction, it stays a constant sickness, in which patients are required to proceed with clinical development for the checking of joint capability and medicine until the end of their lives(22). The endurance of the relocated kidney is reliant upon the recommended immunosuppressive drugs(21).Notably, nonadherence to immunosuppressive treatment after organ transplantation is emphatically connected with negative clinical results. Kidney joins beneficiaries who don't stick to their endorsed drug regimens are at an expanded gamble of contamination, episodes of intense and persistent dismissal and, at last, unite misfortune. It has been accounted for that such nonadherence represents 16.3-36.4% of united misfortunes and 19.9% of late intense dismissals.(20) Unfortunately, adherence by kidney relocation patients (KTPs) isn't just a huge deterrent to allograft upkeep, but may likewise bring about the requirement for dialysis, diminished efficiency, and decreased personal satisfaction for the patient.
Assuming that inquiries were posed to the patient for more information
Questions
• Do you generally take your prescription at the fitting time?
• When you feel more regrettable, have you at any point ended up taking your medicine?
• Have you at any point neglected to take your medicine?
• Have you at any point neglected to take your prescription toward the end of the week?
• Somewhat recently, how often did you neglect to take your endorsed portion?
• Since your last visit, what number of entire days have gone by in which you didn't take your prescription?
The responses were recorded. Patients were grouped by their reactions to the survey. The initial four inquiries were addressed emphatically or adversely utilizing the Yes/No arrangement. The reaction design for the fifth thing was on a 5-point scale with the accompanying choices: never, 1-2 times, 3-5 times, 6-10 times, and >10 times. The last thing expected members to show the number of days. In light of their reactions to the SMAQ things, patients were delegated being either disciple or nonadherent. The adherence bunch comprised of patients who showed a palatable degree of adherence. Patients were viewed as disciples if they answered all inquiries with an adherence reply in every one of the six SMAQ things, for example 'Indeed' in the first, 'No' in the following three things, and not having missed multiple portions during the last week or having neglected to take the drug on not over 2 days during the most recent 3 months. The nonadherence bunch addressed patients who had a low degree of adherence. A patient was considered nonadherent if he/she answered any of the six things on the scale with a nonadherence reply, for example, 'No' in the first, 'Yes' in the accompanying three things, and concerning evaluation, assuming the patient has missed multiple dosages during the last week or had neglected to take the drug on over 2 days during the most recent 3 months.
REFRENCES




Mansi Bhandawne, Tanvi Jadhav*, Hitesh Mahajan, Omkar Labhade, Immunosuppressive Drug Adherence in Kidney Relocate Patients: A Comprehensive Review, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 1429-1442. https://doi.org/10.5281/zenodo.15031749
 10.5281/zenodo.15031749
10.5281/zenodo.15031749
