Department of Pharmacy, LCIT School of Pharmacy, Bilaspur
Myocardial infarction (MI) is one of the most common and serious heart conditions, caused mainly by a sudden fallor blockage in the blood flow to the heart muscle. This interruption leads to a lack of oxygen, which triggers inflammation, oxidative stress, and gradual damage or death of cardiac cells. Even though modern medicines such as antiplatelet drugs, beta-blockers, statins, and ACE inhibitors are widely used, many patients continue to face side effects, high costs, or limited improvement in long-term heart recovery. These challenges have encouraged interest in natural remedies, especially medicinal plants, which have been used for generations in traditional healing systems. Several medicinal plants-such as Terminalia arjuna, Withania somnifera, Moringa oleifera, Magnolia officinalis, Allium sativum, Panax ginseng, and Ocimum sanctum—contain beneficial compounds that help protect the heart. These plants are rich in antioxidants and other natural chemicals that reduce inflammation, lower cholesterol, improve blood circulation, and protect the heart muscle from further injury. Many experimental studies have shown that these herbs can reduce the size of the affected area after an infarction, support stronger heart function, and prevent oxidative damage. Although most evidence currently comes from laboratory or animal studies, the results are encouraging and point toward real therapeutic potential. Overall, medicinal plants offer a promising and safer approach to supporting heart health,especially in the prevention and management of myocardial infarction. Their natural origin, affordability, and broad biological actions make them valuable alternatives or supplements to standard treatments. However, more well-designed human studies are needed to confirm their effectiveness, determine proper dosages, and ensure safety.
MI happens when coronary blood supply to a part of the myocardium is suddenly reduced or stopped, resulting in ischaemia and eventual cardiac tissue destruction. Although additional etiologies such coronary spasm, embolism, or dissection may also be implicated, the most frequent underlying mechanism is the rupture or erosion of an atherosclerotic plaque followed by thrombus development[1]. Insufficient blood flow to the coronary arteries causes myocardial infarction (MI), which is typically brought on by coronary artery stenosis or blockage . 10.636.5 million cases of MI brought on by ischaemic heart disease occurred worldwide in 2017[2]. According to the World Health Organization, MI significantly affects people's lives and is currently the world's leading cause of mortality. As a result, prevention and treatment of MI have gained significant attention[3].
The burden of MI is still rising globally due to ageing populations and rising rates of risk factors as smoking, obesity, diabetes mellitus, dyslipidaemia, and hypertension. According to contemporary epidemiological data, MI makes up a sizable component of cardiovascular diseases, which cause almost one-third of all deaths[4]. Prompt diagnosis and timely reperfusion therapy, either mechanically or pharmacologically, are crucial for reducing myocardial damage and enhancing therapeutic results. Medication, such as aspirin, nitroglycerin, beta-blockers, diuretics, statins, angiotensin-converting enzyme inhibitors.
(ACEI)/ angiotensin receptor blockers (ARB), and aspirin, is one of the most basic methods of treating MI [5]. The most effective and popular treatments for MI at the moment are percutaneous coronary intervention (PCI) and coronary artery bypass graft (CABG), which aim to increase the blood supply to the ischaemic myocardium[6].
The hallmark of MI is the death of heart cells due to a reduced oxygen supply caused by a blocked coronary artery. Variations in intracellular O2 levels have a major effect on oxidative metabolism, which is the main source of cardiac energy generation. Because coronary artery blockage reduces oxygen levels and increases anaerobic-dependent ATP synthesis, it results in energy starvation and cardiac cell necrosis[7].
Pharmacological therapies for MI have actually advanced from basic diuretics and vasodilators to combinations of diuretics, blockers and angiotensin-converting enzyme inhibitors[8]. These medications are crucial for reducing symptoms, boosting myocardial oxygen consumption, and improving haemodynamic parameters, but they don't deal with the underlying causes of MI or its after effects[9]. Traditional medicine has a long history and widespread use in this field globally, and plants offer a multitude of resources for anti-MI medications. Notably, natural product therapies are widely acknowledged as additional or alternative treatments for MI[10]. The use of botanical metabolites in these treatments has gained a lot of attention since they are typically kinder and safer than chemically produced anti-MI metabolites [11]. Medicinal plants have been utilised for ages to prevent, treat, or cure illnesses because they contain chemical compounds with therapeutic qualities[12]. They still have a big impact on both conventional and contemporary healthcare systems, and they serve as the foundation for many contemporary drugs. The goal of this article is to provide a thorough analysis of natural remedies and medicinal herbs used in the last five years to prevent and cure MI[13]. Based on MI's pathogenesis and treatment strategies. Apart from providing an innovative perspective to enhance research and discover new herbs for MI treatment, this study aims to establish a knowledge base for future studies on natural products and medicinal plants in MI treatment[14].
Important medicinal plants and their phytochemistry:
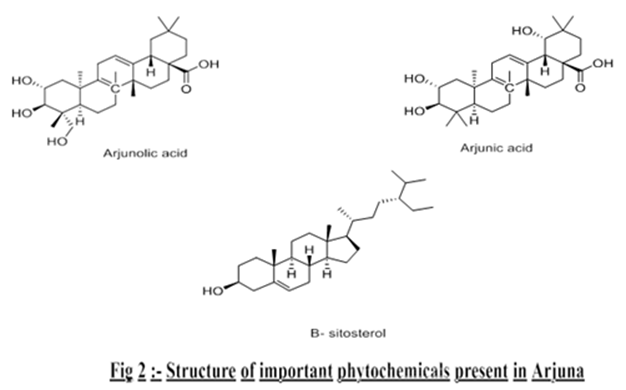
T. arjuna is an important Ayurvedic medicinal plant. It belongs to the Combretaceae family, which hasover 200 species worldwide, and is frequently referred to as Arjuna, Indradru, Partha, and Veeravriksha[15]. Almost 24 species of Terminalia have been identified from various regions of India, including Terminalia bellirica, Terminalia bialata, Terminalia catappa, Terminalia elliptica, Terminalia porphyrocarpa, Terminalia mantaly, and T. arjuna[16]. India, Burma, Mauritius, and Sri Lanka are home to arjuna. It features drooping branches, acrown that spreads horizontally, and a buttressed trunk. Its height ranges from 60 to 80 feet[17]. In the sub-Indo-Himalayan areas of Uttar Pradesh, Punjab, Deccan, South Bihar, Orissa, West Bengal, and Madhya Pradesh, T. arjuna is primarily found around rivers, rivulets, and ponds[18].

Fig1:-Terminalia arjuna
Phytochemistry:- The therapeutic tree Terminalia arjuna (Family: Combretaceae) is well-known for its cardioprotective qualities. The plant's pharmacological effects are influenced by a variety of bioactive substances found in its bark, leaves, fruits, and seeds, including triterpenoids, flavonoids, glycosides, tannins, and minerals[19].
Table1:- Summary of phytochemicals present in Terminalia arjuna by plant parts
|
Sr. No. |
Plant parts |
Major phytochemicals |
Pharmacological significance |
|
1. |
Bark |
Arjunic acid, Arjunolic acid, Arjunosides, Tannins, Flavonoids |
Cardioprotective, Antioxidants, Anti- inflammatory. |
|
2. |
Leaves |
Flavonoids, Tannins, Saponins |
Antioxidants, Antimicrobial. |
|
3. |
Fruits |
Gallic acid, Ellagic acid, β-sitosterol |
Lipid–lowering, Hepatoprotective. |
|
4. |
Seeds |
Phytosterols, polyphenols |
Cholesterol-lowering, Antioxidants. |
|
5. |
Roots |
Triterpenoids, Glycosides |
Suppourtive Cardioprotective role. |
Withania somnifera Dunal, which is a member of the Solanaceae family. This shrub grows throughout the Mediterranean, the Canaries, the Cape of Good Hope, and the drier sections of India, Sri Lanka, Afghanistan, Baluchistan, Sind, and portions of Africa. In the Himalayas, it can be found at elevations of up to 5,500 feet[20]. It grows widely all over India, especially in hotter regions, on waste sites, and at the sides of roads. In India, it is also grown for medical purposes. It is extensively grown in the Garhwal Hills, Rajasthan village, and Mandsaur, Madhya Pradesh. The tomentose shrub Withania somnifera is upright, branching, and evergreen (green all year round). Simple, petiolate leaves range in size from 4 to 10 cm in length and 2 to 7 cm in width. The leaf blades are whole along the edges, acute to obtuse at the apex, oblique at the base, and covered with a persistent greyish tomentum on the sides[21].

Fig 3 :-Withania somnifera
Phytochemistry :- Withania somnifera, which is also referred to as Indian ginseng or ashwagandha, is a well-known adaptogenic and cardioprotective medicinal herb. Myocardial infarction (MI) can be prevented and treated with the help of its bioactive compounds, which have anti-inflammatory, anti-apoptotic, antioxidant, and hypolipidemic qualities[22].
Table2:-Summary of phytochemicals present in withania somnifera by plant parts
|
Sr. No. |
Plant parts |
Major phytoconstituents |
Pharmacological significance |
|
1. |
Bark |
Phenolics, Withanolides |
Mild antioxidants. |
|
2. |
Leaves |
Withaferin-A, Flavonoids |
Antioxidants, Anti– apoptotic. |
|
3. |
Fruits |
Withanolides, Fatty acids |
Lipid metabolism regulation. |
|
4. |
Seeds |
Amino acids, Alkaloids |
Nutritional support. |
|
5. |
Roots |
Withanolides , Alkaloids, Sitoindosides |
Antioxidants, Anti-inflammatory, Hypolipidemic. |
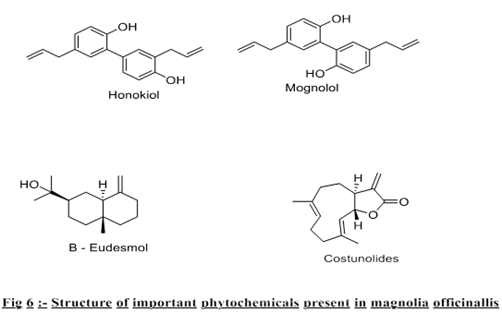
The deciduous medicinal tree Magnolia officinalis is indigenous to China's mountain forests and a member of the Magnoliaceae family. Its large, dark green leaves and fragrant white flowers bloom in the summer, and it can reach a height of 20 to 30 feet[23]. The primary portion used for medicinal purposes is the thick, fragrant bark. It has long been used in Chinese medicine under the name Houpu to treat circulation issues, anxiety, and digestive issues. The bark's pharmacological qualities, which include cardioprotective, anti-inflammatory, and antioxidant actions, are attributed to bioactive compounds including honokiol and magnolol[24]. Recent studies have shown that honokiol activates the PI3K/AKT signalling pathway, which has cardioprotective effects in myocardial ischaemia and reperfusion injury, while reducing oxidative stress, inflammation, and cardiomyocyte apoptosis. Both heart function and the size of infarcts are improved by these actions[25].

Fig 5:-Magnolia officinalis
Phytochemistry:- The plant's bioactive lignans, alkaloids, terpenoids, and phenolic compounds are mostly found in the bark of Magnolia officinalis, while they can also be found in the leaves, roots, and seeds. Its numerous pharmacological properties, such as antimicrobial, anti-inflammatory, antioxidant, and cardioprotective effects, are attributed to these phytochemicals[26].
Table3:- Summary of phytochemicals present in Magnolia officinalis by plant parts
|
Sr. no. |
Plant parts |
Major phytoconstituents |
Pharmacological significance |
|
1. |
Bark |
Honokiol, Magnolol, Obovatol, Magnoflorine, Costunolide, β-Eudesmol |
Antioxidants, Anti-inflammatory, Anti-anxiety, Cardioprotective. |
|
2. |
Leaves |
Magnolignan, Eudesmol, Linalool, α Pinene, β-Caryophyllene |
Antibacterial, Anti-inflammatory, Calming and relaxing effects. |
|
3. |
Roots |
Magnoflorine, Honokiol, Magnolol |
Sedative, Anti–inflammatory, Antioxidants. |
|
4. |
Seeds |
Honokiol, Magnolol, Fatty acid, phenolic compounds |
Antioxidants, Antimicrobial. |
|
5. |
Flowers |
Linalool, Eudesmol, Magnolol (trace) |
Fragrance, Antioxidants, Mild antimicrobial. |
One of the most extensively grown species of the Moringaceae family is the significant medical plant Moringa oleifera. Since ancient times, it has been highly prized due to its numerous therapeutic benefits. The wild tree grows in the Sub-Himalayan areas between Chenab and Oudh. It can grow as high as 1400 meters above the sea level[27]. People often grow it near their homes in Assam, Bengal and the Indian peninsula. It's an excellent coppicer. Additionally, it is grown in the northeastern regions of Bangladesh, Pakistan, Sri Lanka, West Asia, the Arabian Peninsula, East and West Africa, the West Indies, southern Florida, and Central and South America, ranging from Mexico to Peru, Brazil, and Paraguay[28]. Moringa oleifera is a small, fast-growing evergreen or deciduous tree that usually reaches a height of nine meters. It has soft, white wood and corky, sticky bark. Horse radish is the flavor of the roots.The leaves have glabrous, entire leaflets, jointed branches that are glandular at the joints, longitudinal fissures, and a main axis that is 30 to 75 cm long. The leaflets have a small tip at the base, a rounded or blunt-pointed apex, entire (not toothed) borders, and red-tinged mid-veins[29].

Fig 7:-Moringa oliefera
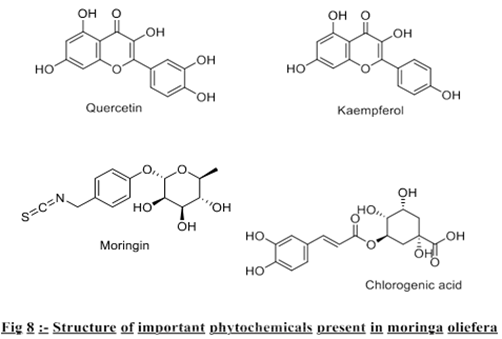
Phytochemistry:- Moringa oleifera, also known as the drumstick tree or horse radish tree, is a very important medicinal plant that is full of bioactive compounds that are good for the heart. Flavonoids, phenolic acids, alkaloids, glucosinolates, and terpenoids.
The phytochemicals that can be found in the leaves, seeds, pods, flowers, and roots of the plant[30].
Table4:- Summary of phytochemicals present in moringa oliefera by plant parts
|
Sr. no. |
Plant parts |
Major phytoconstituents |
Pharmacological significance |
|
1. |
Leaves |
Quercetin, Kaempferol, Chlorogenic acid, β-sitosterol, Ascorbic acid |
Potent antioxidants and anti – inflammatory, reduce lipid peroxidation and myocardial Oxidative stress. |
|
2. |
Seeds |
Oleic acid, Palmitic acid, Sterols, Flavonoids |
Hypolipidemic and membrane stabilizing effects, protect cardiac cells from injury. |
|
3. |
Pods |
Vitamin–C, Carotenoids, Polyphenols |
Enhance antioxidants defense and protect cardiac tissues from oxidative stress. |
|
4. |
Flowers |
Phenolic acid, Flavonoids, Alkaloids |
Anti–inflammatory and free radical scavenging properties, improve endothelial functions. |
|
5. |
Roots |
Moringine (benzylamine alkaloids), Tannins, Saponins |
Vasodilatory and cardioprotective effects, improve coronary circulation and reduce cardiac load. |
Garlic, or Allium sativum, was one of the first plants to be grown. It has been used as a spice, food, and traditional medicine for over 4,000 years. It is the medicinal plant that has been researched the most (Milner 1996)[31]. In 22 therapeutic formulations found in the Egyptian medical papyrus Codex Ebers, which dates to around 1550 B.C., garlic is mentioned as a helpful treatment for a number of diseases, including tumours, worms, headaches, heart tissues, and bites [32]. Bulbs are rounded and made up of up to fifteen tiny clove-like bulblets. A white or pinkish tunic (papery garment) covers the cloves and bulbs. An subterranean stem is connected to four to twelve long, sword-shaped leaves. Spherical cluster up to 25 cm long on a spike (flower stalk). The six perianth segments (petals and sepals) of greenish white or pinkish flowers are roughly 3 mm long[33].

Fig9:-Allium sativum
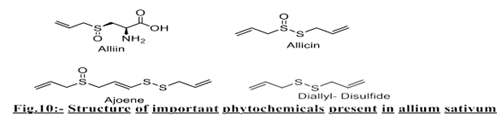
Phytochemistry:- Allium sativum, is dominated by organo sulfur compounds, which are primarily found in the bulb (clove) and include alliin, allicin, ajoene, diallyl disulphide (DADS), diallyl trisulfide (DATS), and S-allyl-L-cysteine (SAC). While garlic oil is abundant in volatile sulphides (DADS, DATS), aged garlic extract contains stable water-soluble compounds like SAC. All of which support its cardioprotective and antioxidant properties. By lowering oxidative stress, inflammation, platelet aggregation, and myocardial cell damage, these components work together to protect against myocardial infarction (MI)[34].
Table 5:- Summary of phytochemicals present in allium sativum by plant parts
|
Sr. No. |
Plant parts |
Major phytoconstituents |
Pharmacological significance |
|
1. |
Bulb (fresh) |
Alliin, Allicin, DADS, DATS, Ajoene |
Antioxidants, Vasodilatory, Antithrombotic. |
|
2. |
Aged garlic extract |
S-allyl-L-cysteine, S–allyl mercaptocysteine |
Anti-apoptotic, Antioxidants, Cardioprotective. |
|
3. |
Garlic oil |
DADS, DATS, Ajoene |
Prevents platelets aggregation, enhances NO release. |
|
4. |
Leaves and peel |
Flavonoids, Phenolics, Saponins |
Antioxidants, Anti– inflammatory. |
Panax ginseng was first grown in 11 BC and has been used medicinally for over 5,000 years. The genus name "Panax," which comes from the Greek words "pan," which means all, and "axos," which means medicine, was given to Panax ginseng by the Russian scientist C.A. Meyer[35]. The commercially available ginseng roots are divided into two categories based on how they are processed: red ginseng (RG) and white ginseng (WG). One possible explanation for the variations in the biological activity of WG and RG is that their industrial processing alters their chemical composition[36]. The common names for the genus Panax and the family Araliaceae are "Ginseng" and "Ginseng Family," respectively, according to Gray's Manual of Botany. In this instance, the common names of a genus and a family of plants that bloom[37].

Fig 11:-Panax ginseng
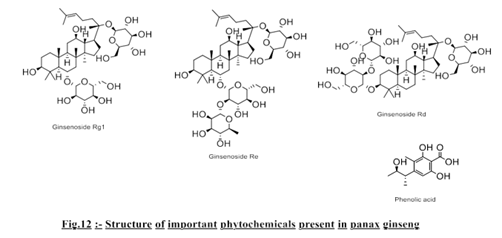
Phytochemistry:- The popular medicinal plant Panax ginseng, also known as Korean ginseng, is prized for its adaptogenic and cardioprotective qualities. Its high concentration of bioactive ginsenosides, polysaccharides, polyacetylenes, peptides, and phenolic compounds are largely responsible for its therapeutic action against myocardial infarction (MI)[38].
Table6:- Summary of phytochemicals present in panax ginseng by plant parts
|
Sr. no. |
Plant parts |
Major phytoconstituents |
Pharmacological significance |
|
1. |
Roots |
Ginsenosides (Rb1, Rg1, Rg3, Rd, Re, Rh1, Rh2), polysaccharide |
Antioxidants, Anti– inflammatory, Anti-apoptotic, improve Cardiac function and reduce infract size. |
|
2. |
Leaves and stems |
Ginsenosides (Rg1, Rd, Re), Polyecetylenes, Flavonoids |
Enhance coronary blood flow, reduce oxidative stress, protect cardiomyocytes. |
|
3. |
Barriers (fruits) |
Ginsenoside Re, Polysaccharides, phenolic acids |
Reduce lipid peroxidation, improve cardiac metabolism and antioxidant defense |
Ocimum sanctum has been acknowledged as one of the most versatile therapeutic herbs with a wide range of biological activity for more than 2000 years. On the Indian subcontinent, this widely utilised religious herb is called holy basil or tulsi. Basils, which most likely originated in India, are found across tropical Asia[39]. Usually cultivated from seeds, it is an annual plant. It is extensively distributed in tropical climates and may be found at an elevation of 1800 meters in the Himalayan region. In many parts of Asia and Africa, certain tulsi variants grow well in the wild[40]. Leaves are dark brown on the outside and on the inside it is a delicated shade of violet with hairy and subgrandular flowers that are dark purple to black on the outside and cream on the outside. The flower's pedicels are longer than the calyx, which is ovoid or campanulate and 3–4 mm bilipped; the lower lips, which are 170 times longer than the upper, have four mucronate teeth, the two largest in the centre; the upper lips are broadly rectangular or suborbicular[41].

Fig 13 :-Ocimum sanctum
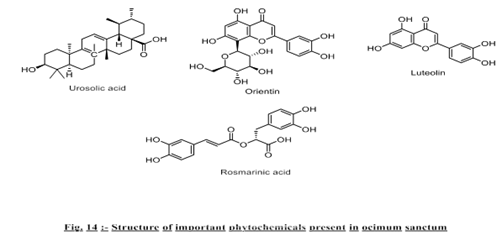
Phytochemsitry :- Ocimum sanctum, sometimes referred to as holy basil or tulsi, has strong antioxidant and cardioprotective qualities that are helpful in the treatment of myocardial infarction (MI). Its rich phytochemical composition, which improves endogenous antioxidant defences and lowers oxidative stress, lipid peroxidation, and myocardial necrosis, is largely responsible for its therapeutic potential. Numerous bioactive components, including flavonoids, phenolic acids, terpenoids, and essential oils, are found in various parts of Ocimum sanctum and are essential for cardio-protection[42].
Table7:-Summary of phytochemicals present in Ocimum sanctum by plant parts
|
Sr. no. |
Plant parts |
Major phytoconstituents |
Pharmacological significance |
|
1. |
Leaves |
Eugenol, Ursolic acid, Apigenin, Luteolin, Rosmarinic acid, Orientin, Vicenin, Carvacol |
Antioxidants, Anti – inflammatory, Anti – apoptotic effects and reduce lipid peroxidation and protect cardiac tissue from ischemic injury. |
|
2. |
Seeds |
Linoleic acid, Oleic acid and fixed oils |
Regulate lipid metabolism, improve membrane stability and exhibit hypolipidemic effects. |
|
3. |
Roots |
Triterpenoids, Saponins and phenolic compounds |
Improve myocardial Antioxidants defence and reduce infract size. |
|
4. |
Stem |
Phenolic acid, Flavonoids and Tannins |
Contribute to vascular protection and inhibition of inflammatory mediators. |
|
5. |
Essential oil (whole plant ) |
Eugenol, Methyl eugenol, Caryophyllene and Linalool |
Vasodilatory, Antiplatelet and free-radical scavenging effects and improving coronary bloodflow. |
Mechanism of Medicinal Plants in Treatment of MI
Medicinal plants play an important supportive role in the management of myocardial infarction by protecting heart muscle cells, improving blood flow, and reducing damage caused by oxidative stress and inflammation.
Table8 :-Mechanism of various medicinal plants in treatment of MI
|
Sr. No. |
Medicinal Plant |
Major Active Constituents |
Key Mechanism in Myocardial Infarction |
|
1 |
Terminalia arjuna |
Arjunic acid, Arjunolic acid, Arjunosides, Tannins, Flavonoids |
Enhances myocardial contractility, reduces oxidative stress, stabilizes cardiac cell membrane, improves coronary blood flow, prevents lipid accumulation in coronary arteries |
|
2 |
Withania somnifera |
Phenolics, Withanolides, Withaferin-A, Flavonoids |
Protects cardiomyocytes by reducing oxidative stress and inflammation, regulates stress hormones, limits ischemia-induced cell death, supports myocardial recovery |
|
3 |
Magnolia officinalis |
Honokiol, Magnolol, Obovatol, Magnoflorine, Costunolide, β-Eudesmol |
Suppresses inflammatory signaling, reduces oxidative damage, prevents calcium overload in cardiac cells, protects myocardial tissue during ischemic injury |
|
4 |
Moringa oleifera |
Quercetin, Kaempferol, Chlorogenic acid, β-sitosterol, Flavonoids |
Scavenges free radicals, reduces lipid peroxidation, protects heart tissue from ischemia-related oxidative injury |
|
5 |
Allium sativum |
Alliin, Allicin, DADS, DATS, Ajoene, S-allyl-L-cysteine |
Inhibits platelet aggregation, lowers cholesterol, improves endothelial function, enhances nitric oxide (NO) availability |
|
6 |
Panax ginseng |
Ginsenosides (Rb1, Rg1, Rg3, Rd, Re, Rh1, Rh2), Polysaccharides, Phenolic acids |
Improves mitochondrial energy metabolism, reduces oxidative stress, modulates inflammatory pathways, enhances survival of cardiac cells after infarction |
|
7 |
Ocimum sanctum |
Eugenol, Ursolic acid, Apigenin, Luteolin, Rosmarinic acid, Orientin, Vicenin, Carvacrol |
Reduces oxidative stress, suppresses inflammatory mediators, enhances endogenous antioxidant enzymes, limits myocardial cell injury during infarction |
CONCLUSION
Myocardial infarction (MI) is still the number one cause of death around the world. It happens because of oxidative stress, inflammation, and damage to cells. The drawbacks of existing synthetic drugs, including adverse effects and exorbitant costs, underscore the necessity for safer and more efficacious alternatives. Medicinal plants present a promising a venue owing to their extensive variety of bioactive phytoconstituents possessing antioxidant, anti-inflammatory, anti-apoptotic, and cardioprotective attributes. Plants including Terminalia arjuna, Withania somnifera, Allium sativum, Moringa oleifera, Panax ginseng, Magnolia officinalis, and Ocimum sanctum have shown substantial potential in preventing and controlling MI by altering critical molecular pathways involved in heart damage. Novel plant-based cardioprotective treatments may be made possible by fusing traditional herbal knowledge with contemporary pharmacological and clinical research. Medicinal plants have the potential to improve cardiovascular health worldwide by acting as safe, economical, and sustainable substitutes or supplements to traditional MI treatments with more scientific validation, standardization, and clinical studies.
The advancement of translational research and scientific validation will determine the future of treating myocardial infarction (MI) with medicinal plants. Using contemporary pharmacological, genomic, and bioinformatics tools to standardize herbal extracts, identify bioactive phytoconstituents, and determine their specific molecular processes is becoming increasingly important. Carefully considered clinical trials should come after preclinical research to verify safety, effectiveness, and dosage optimization in humans. Additionally, the development of sophisticated formulations such as liposomes, phyto-complexes, and nanoparticles can greatly enhance the stability, bioavailability, and targeted transport of compounds obtained from plants to cardiac tissues. Finding novel cardioprotective medications with fewer side effects will be made simpler by fusing traditional medical knowledge with contemporary drug development technologies.
REFERENCES


Takeshwar, Md Akib Quraishi, Herbal Approaches in the Treatment of Myocardial Infarction : A Phytochemical Perspective, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 3677-3690. https://doi.org/10.5281/zenodo.19257045
 10.5281/zenodo.19257045
10.5281/zenodo.19257045
