Balwantrao Chavan College of Pharmacy, India
The present study was aimed at the development and evaluation of microballoons containing a crude drug for gastroretentive drug delivery. Microballoons are hollow, spherical multiple-unit dosage forms designed to prolong gastric residence time and enhance the bioavailability of drugs with absorption windows in the upper gastrointestinal tract. The crude drug was selected based on its therapeutic potential and was formulated into microballoons using the solvent evaporation technique with suitable polymers. The prepared microballoons were evaluated for micromeritic properties such as particle size, bulk density, tapped density, Hausner’s ratio, Carr’s index, and angle of repose to assess flow characteristics. Further evaluation parameters included drug entrapment efficiency, buoyancy studies, surface morphology, and in vitro drug release behavior. The microballoons exhibited good flow properties, high floating ability, and uniform particle size distribution. In vitro drug release studies demonstrated sustained release of the crude drug over an extended period, indicating effective gastroretentive behavior. The formulation of crude drug-loaded microballoons offers a promising approach to improve therapeutic efficacy, enhance bioavailability, reduce dosing frequency, and increase patient compliance. The study concludes that microballoon-based delivery systems are suitable carriers for herbal drugs requiring prolonged gastric retention.
Microballoons are an advanced form of gastroretentive drug delivery system (GRDDS) designed to prolong the residence time of drugs in the stomach. They are developed based on a non-effervescent floating approach, which does not rely on gas-generating agents. Microballoons are generally hollow, spherical structures without a solid core, making them lightweight and capable of floating on gastric fluids for an extended duration.
These systems are typically prepared as free-flowing powders composed of natural polymers (such as proteins and polysaccharides) or synthetic polymers. The particle size of microballoons generally ranges up to 200 µm, which facilitates easy administration and uniform drug distribution. Due to their low density and high buoyancy, microballoons remain afloat in gastric fluid for prolonged periods without causing irritation or damage to the gastrointestinal tract.
Various formulation techniques are employed for the preparation of microballoons, including simple solvent evaporation, double emulsion method, phase separation (coacervation), polymerization, spray drying, spray congealing, and hot-melt encapsulation methods. These techniques enable the formation of hollow structures capable of sustained and controlled drug release.
Microballoons represent an advanced and specialized category of gastroretentive drug delivery systems (GRDDS) that are specifically designed to prolong the gastric residence time of orally administered drugs. The primary objective of these systems is to retain the dosage form in the stomach for an extended duration, thereby improving drug bioavailability, especially for drugs that are preferentially absorbed in the stomach or upper part of the small intestine, are unstable in the intestinal environment, or exhibit a narrow absorption window.
Microballoons are developed using a non-effervescent floating approach, which distinguishes them from effervescent systems that depend on gas-generating agents such as sodium bicarbonate. In non-effervescent systems, buoyancy is achieved through the intrinsic low density of the dosage form, resulting from the presence of a hollow internal structure. These microballoons are generally spherical in shape and lack a solid core, which significantly reduces their density and enables them to float continuously over gastric contents for a prolonged period.
Structurally, microballoons are composed of a polymeric shell surrounding an internal hollow cavity. The polymers used may be of natural origin, such as proteins and polysaccharides (e.g., gelatin, alginate, chitosan), or synthetic polymers, such as ethyl cellulose, polyvinyl alcohol, or Eudragit polymers. These materials are selected based on their biocompatibility, biodegradability, swelling ability, and capacity to control drug release. The formulation is typically obtained in the form of free-flowing powder, which enhances ease of handling, uniform dosing, and formulation stability.
The particle size of microballoons generally does not exceed 200 µm, which plays a crucial role in their performance. Smaller particle size ensures better dispersion in gastric fluid, uniform drug distribution, and reduced risk of dose dumping. Additionally, the small and smooth spherical shape minimizes mechanical irritation to the gastric mucosa, thereby improving patient tolerability and safety.
One of the most significant features of microballoons is their low density and high buoyancy, which allows them to remain afloat on gastric fluid for several hours. When introduced into the stomach, microballoons do not sink or adhere to the gastric wall but rather float freely, ensuring prolonged gastric retention without causing obstruction or irritation. This floating behavior results in extended drug release at the desired site, improved therapeutic efficacy, and reduced dosing frequency.
A variety of formulation techniques are employed for the preparation of microballoons, each offering specific advantages depending on the nature of the drug and polymer used. These include simple solvent evaporation, double emulsion technique, phase separation (coacervation), polymerization, spray drying, spray congealing, and hot-melt encapsulation methods. These methods facilitate the formation of hollow microspheres by controlling solvent removal, polymer precipitation, or thermal solidification. The choice of technique directly influences particle size, entrapment efficiency, buoyancy, and drug release profile.
Overall, microballoons offer a versatile and efficient approach for sustained and controlled drug delivery in the stomach. Their ability to maintain buoyancy, protect the drug from premature degradation, and release the drug in a controlled manner makes them particularly suitable for chronic therapy and drugs requiring localized gastric action. As a result, microballoons have gained considerable attention in pharmaceutical research as a promising carrier system for improving oral drug delivery performance.
Microballoons are an advanced form of gastroretentive drug delivery system (GRDDS) designed to enhance the therapeutic efficacy of orally administered drugs by prolonging their residence time in the stomach. These systems are particularly beneficial for drugs that are preferentially absorbed in the stomach or upper part of the small intestine, exhibit poor stability in the intestinal environment, or possess a narrow absorption window. Microballoons are formulated based on a non-effervescent floating approach, which eliminates the need for gas-generating agents and instead relies on the intrinsic properties of the formulation to achieve buoyancy.
Structurally, microballoons are hollow, spherical microspheres without a solid core, consisting of a polymeric shell surrounding an internal cavity. This hollow structure significantly reduces the density of the system, making it lower than that of gastric fluid. As a result, microballoons are capable of floating freely on the gastric contents for an extended period. They are usually prepared as free-flowing powders using natural polymers such as proteins and polysaccharides or synthetic polymers selected for their biocompatibility, biodegradability, and controlled-release properties. The particle size generally remains below 200 µm, which ensures uniform distribution in gastric fluid and minimizes irritation to the gastric mucosa.
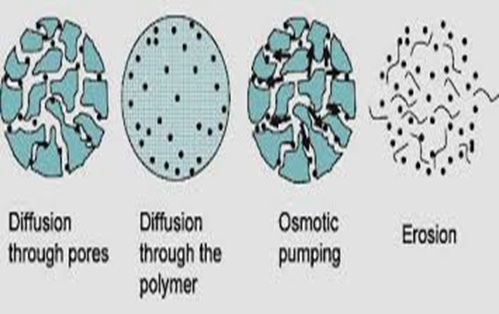
When microballoons come into contact with gastric fluid, the polymeric shell rapidly hydrates and swells, forming a gel-like barrier around the microsphere. This hydrated polymer layer acts as a diffusion-controlling membrane that regulates the penetration of gastric fluid into the microballoon and controls the outward diffusion of the drug. The drug present near the surface dissolves first, followed by gradual release from the inner layers, resulting in a controlled and sustained drug release profile.
Simultaneously, as the polymer swells, air becomes entrapped within the internal hollow cavity, further reducing the overall density of the system. This entrapped air provides sufficient buoyant force to keep the microballoons floating over the gastric contents for prolonged periods. The continuous floating behavior ensures that the drug delivery system remains in the stomach, allowing prolonged exposure of the drug to its absorption site and reducing fluctuations in plasma drug concentration.
Thus, the combined effect of low density, polymer hydration, gel barrier formation, and controlled diffusion governs both the floating behavior and drug release mechanism of microballoons. These characteristics make microballoons an efficient gastroretentive system capable of delivering drugs in a sustained, controlled, and site-specific manner, thereby improving bioavailability and therapeutic outcomes.
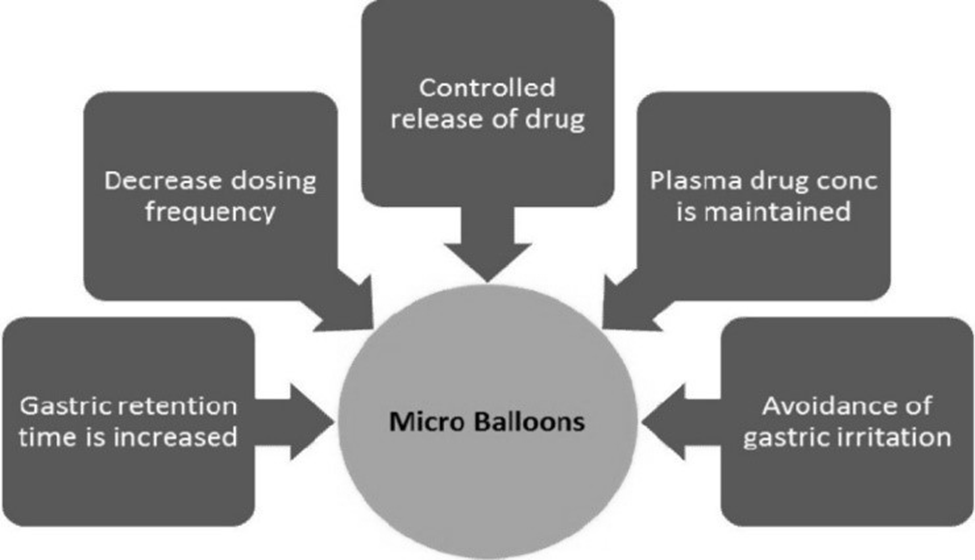
Advantages of Microballoons
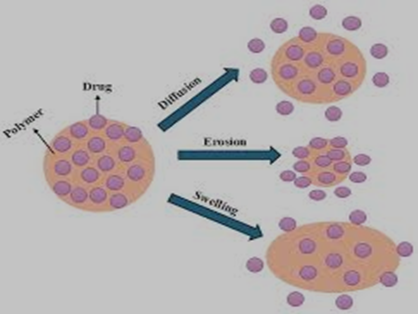
Mechanism of Drug Release from Microballoons
Upon contact with gastric fluid, the polymers and gel-forming agents present in microballoons hydrate and swell, forming a colloidal gel barrier around the surface. This gel layer regulates the penetration of gastric fluid into the microballoon and controls the diffusion of the drug.
As hydration continues, the outer layer dissolves gradually, allowing the drug to be released in a controlled and sustained manner. Simultaneously, air becomes entrapped within the swollen polymer matrix, resulting in a decrease in density. This entrapped air provides buoyancy, enabling the microballoons to float continuously over gastric contents.
Formulation Methods of Microballoons
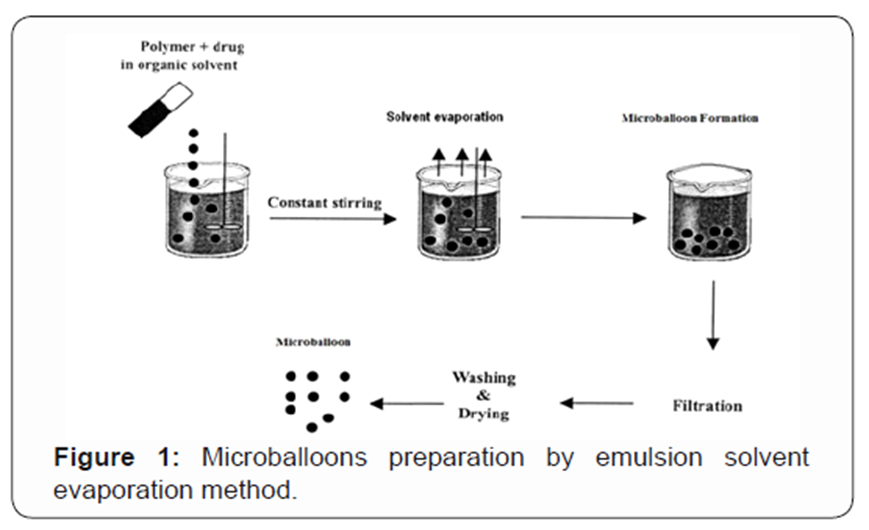
1. Emulsion Solvent Evaporation Method
This is one of the most widely used methods for the preparation of microballoons. In this technique, the drug is first dissolved or dispersed in an aqueous phase, while the polymer is dissolved in a volatile organic solvent such as chloroform or dichloromethane to form the organic phase. The aqueous drug solution is emulsified into the polymer-containing organic phase under continuous stirring, forming a water-in-oil (W/O) emulsion.
This emulsion is then added to a large volume of aqueous phase containing an emulsifying agent (such as polyvinyl alcohol), resulting in the formation of a multiple emulsion system. Continuous stirring facilitates the evaporation of the organic solvent, leading to precipitation of the polymer around the aqueous droplets. As the solvent evaporates, hollow microspheres (microballoons) are formed due to the removal of solvent from the internal phase. The formed microballoons are collected, washed to remove residual solvent and surfactant, and finally dried.
Hollow microballoons with good buoyancy and controlled drug release.
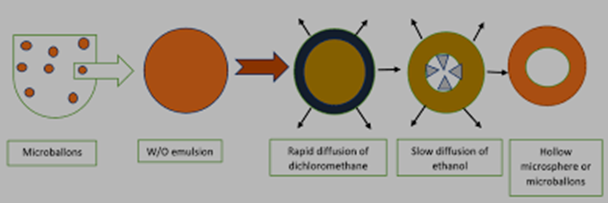
2. Emulsion Solvent Diffusion Method
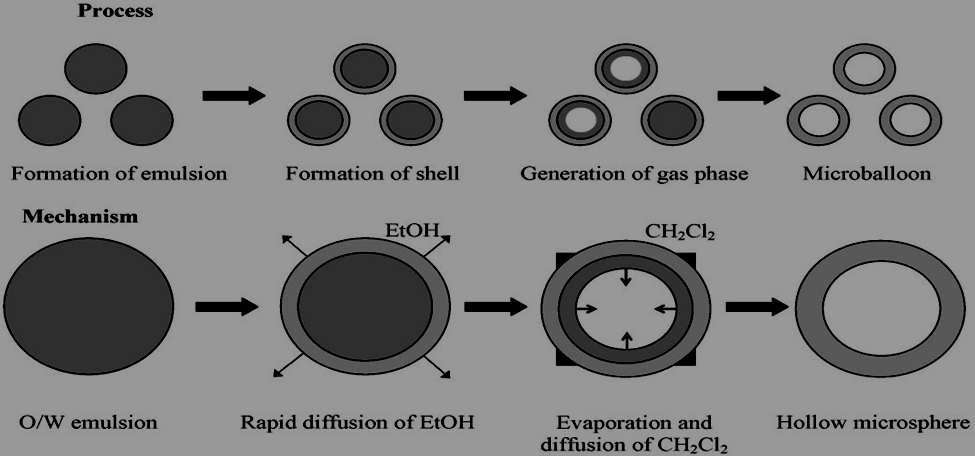
The emulsion solvent diffusion method is based on the mutual diffusion of solvents between the internal and external phases. In this method, the drug and polymer are dissolved in a mixture of partially water-miscible solvents, typically ethanol and methylene chloride. This solution is poured into an aqueous solution of polyvinyl alcohol (PVA) under constant agitation.
Ethanol rapidly diffuses into the external aqueous phase, leading to a reduction in polymer solubility and causing polymer precipitation around the methylene chloride droplets. Subsequently, the entrapped methylene chloride slowly evaporates, resulting in the formation of internal cavities within the microspheres. These cavities are responsible for the hollow structure and buoyancy of microballoons.

Uniform, spherical hollow microballoons with high floating ability.
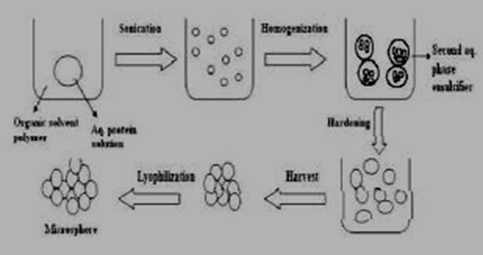
3. Single Emulsion Technique
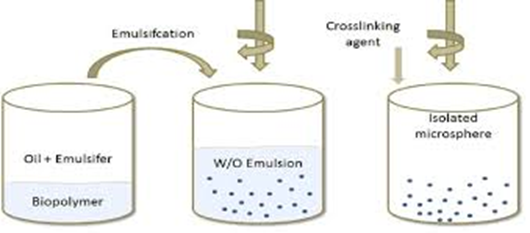
The single emulsion technique is mainly employed for hydrophilic polymers and drugs. In this method, an aqueous solution or suspension of the polymer and drug is prepared and then dispersed into an immiscible organic phase such as oil or chloroform under mechanical stirring or sonication, forming a water-in-oil (W/O) emulsion.
To stabilize the formed droplets, the emulsion is subjected to chemical cross-linking (using agents such as glutaraldehyde) or heat denaturation, which solidifies the polymer shell. The hardened microspheres are then separated by centrifugation, washed thoroughly to remove residual cross-linking agents, and dried to obtain hollow microballoons.
Stable microballoons with controlled size and enhanced structural integrity.
4. Double Emulsion Technique
The double emulsion technique, commonly known as the water-in-oil-in-water (W/O/W) method, is especially useful for hydrophilic drugs. Initially, the aqueous drug solution is emulsified into an oil phase containing the polymer to form a primary W/O emulsion using homogenization.
This primary emulsion is then added to an aqueous solution of PVA to form a secondary emulsion. The organic solvent is removed by evaporation or diffusion, causing the polymer to harden around the internal aqueous droplets. The resulting hollow microspheres are then separated, washed, and dried.
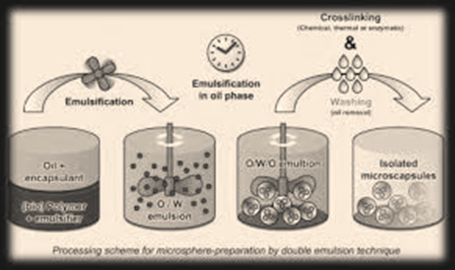
High drug entrapment efficiency and uniform hollow microballoons.
5. Coacervation Phase Separation Technique
In the coacervation phase separation technique, microballoons are formed by separating the polymer-rich phase from the polymer-poor phase. Phase separation is induced by altering temperature, pH, ionic strength, or by adding a non-solvent to the polymer solution.
During phase separation, the polymer-rich coacervate droplets deposit around the drug particles, forming a coating. The coated particles are then hardened by cross-linking or solvent removal. Finally, the microballoons are separated and dried.
Microballoons with high encapsulation efficiency and controlled release characteristics.
6. Spray Drying and Spray Congealing Methods

a) Spray Drying
In spray drying, a solution or suspension of drug and polymer is atomized into a chamber containing hot air. The solvent evaporates rapidly due to high temperature, leading to the formation of hollow microballoons. The rapid drying process results in spherical particles with a porous structure.
Fine, uniform microballoons suitable for large-scale production.
b) Spray Congealing
Spray congealing involves spraying a molten polymer containing the drug into a cooling chamber. Upon cooling, the droplets solidify to form microspheres. Unlike spray drying, no solvent is required; solidification occurs by thermal congealing.
Microballoons are prepared by various emulsion-based and spray techniques that create hollow structures through solvent evaporation, diffusion, phase separation, or thermal solidification.
Formulation Methods of Microballoons: Comparative Overview
Table: Comparison of Different Methods Used for Preparation of Microballoons
|
Sr. No. |
Method |
Principle |
Key Materials Used |
Advantages |
Limitations |
|
1 |
Emulsion Solvent Evaporation |
Evaporation of volatile organic solvent leads to polymer precipitation forming hollow microspheres |
Polymer, volatile solvent (chloroform), emulsifier (PVA) |
Simple method, good control over particle size, high buoyancy |
Use of organic solvents, longer processing time |
|
2 |
Emulsion Solvent Diffusion |
Diffusion of partially water-miscible solvent induces polymer precipitation |
Ethanol, methylene chloride, PVA |
Uniform particle size, good floating ability |
Solvent handling required |
|
3 |
Single Emulsion Technique |
Cross-linking or heat denaturation of polymer droplets |
Hydrophilic polymers, oil phase, cross-linking agents |
Good structural integrity, suitable for proteins |
Possible toxicity from cross-linkers |
|
4 |
Double Emulsion Technique (W/O/W) |
Formation of multiple emulsion for drug entrapment |
Aqueous drug solution, polymer, oil phase, PVA |
High entrapment of hydrophilic drugs |
Complex process, risk of drug leakage |
|
5 |
Coacervation Phase Separation |
Induced polymer-rich phase coats drug particles |
Polymer, non-solvent, cross-linker |
High encapsulation efficiency |
Difficult to control particle size |
|
6 |
Spray Drying |
Rapid solvent evaporation using hot air |
Polymer solution, hot air |
Scalable, rapid process |
Heat sensitive drugs may degrade |
|
7 |
Spray Congealing |
Thermal solidification of molten polymer |
Molten polymer, cooling air |
Solvent-free method, good stability |
Requires high temperature |
Crude Drug as an Approach in Microballoon Formulation
In addition to synthetic and semi-synthetic polymers, crude drugs of natural origin play an important role in the formulation of microballoons. The use of crude drugs aligns with the growing interest in herbal and natural drug delivery systems, offering improved safety, biocompatibility, and patient acceptability.
Crude drugs may be used either as active pharmaceutical ingredients (APIs) or as polymeric carriers in the preparation of microballoons. Natural polymers obtained from crude drugs, such as polysaccharides, gums, mucilages, and proteins, possess excellent swelling, gel-forming, and film-forming properties that are essential for gastroretentive systems.
Role of Crude Drugs in Microballoons
Advantages of Using Crude Drugs
Crude drugs / natural polymers used in microballoons
|
Crude drug (source) |
Main polymeric component |
Primary role in microballoons |
Advantages |
|
Sodium alginate (brown algae) |
Alginate (anionic polysaccharide) |
Forms gel network on contact with acidic medium; provides swelling, gel barrier and entraps air for buoyancy |
Biocompatible, easy to cross-link (Ca²?), good film-forming and mucoadhesive properties |
|
Chitosan (crustacean shells / fungal sources) |
Chitosan (cationic polysaccharide) |
Coating or matrix former; improves mucoadhesion and can modify release (pH sensitive) |
Biodegradable, mucoadhesive, can form polyelectrolyte complexes with alginate |
|
Gelatin / collagen (animal connective tissue) |
Gelatin (protein) |
Hydrogel-former; provides structural integrity, can produce hollow beads/microbeads |
Biodegradable, good film-forming, accepts ionic/enzymatic cross-linking |
|
Guar gum / locust bean gum (seed galactomannans) |
Galactomannan polysaccharides |
Swelling agents and viscosity enhancers; slow diffusion-controlled release |
Readily available, inexpensive, high swelling capacity |
|
Xanthan gum (microbial exopolysaccharide) |
Xanthan (anionic polysaccharide) |
Viscosity builder, gel layer formation to control diffusion and improve buoyancy |
High viscosity at low concentrations, stable over pH range |
|
Pectin / carrageenan (plant / seaweed polysaccharides) |
Pectin (anionic), Carrageenan (sulfated polysaccharide) |
Gel formation (ionic or acid-induced) used as matrix or coating |
GRAS-status (many), biodegradable, form strong gels under suitable conditions |
|
Starch / modified starch (e.g., maize, rice, potato) |
Polysaccharide (amylose/amylopectin) |
Matrix former; can be modified to adjust swelling & erosion |
Cheap, abundant, amenable to chemical modification |
|
Okra mucilage / Aloe vera mucilage (plant mucilages) |
Heteropolysaccharide mucilage |
Natural mucoadhesive and gel-forming excipient for buoyancy and release |
Natural, often gentle on mucosa, multifunctional (binders, gelling) |
Crude Drug as an Approach:
Crude drugs and natural polymers are increasingly used in the formulation of microballoons due to their biocompatibility, biodegradability, cost-effectiveness, and inherent functional properties such as swelling, gel formation, and mucoadhesion. These characteristics make them highly suitable for gastroretentive drug delivery systems, where prolonged gastric residence and controlled drug release are required. Natural polymers can function either as drug carriers (matrix or coating materials) or as active therapeutic agents in herbal microballoon formulations.
The practical workflow for using crude drugs in microballoon formulation begins with proper selection and authentication of the raw material to ensure identity, quality, and reproducibility. This is followed by extraction or isolation, commonly using aqueous or hot-water methods for gums and mucilages, or chemical/enzymatic treatments for specific polysaccharides. The extracted material is then purified and standardized to remove impurities and to maintain batch-to-batch consistency.
Further characterization of the natural polymer is performed to evaluate physicochemical properties such as functional groups, thermal behavior, crystallinity, viscosity, and molecular weight, along with functional properties like swelling index and mucoadhesive strength. Drug–polymer compatibility studies are essential to ensure formulation stability and predictable drug release behavior.
Based on polymer properties, an appropriate formulation method (emulsion techniques, coacervation, spray drying, etc.) is selected. The formulation process is then optimized by adjusting polymer concentration, drug ratio, emulsifier type, stirring speed, and cross-linking conditions to achieve maximum buoyancy, entrapment efficiency, and controlled drug release. Finally, the prepared microballoons are evaluated for particle size, floating behavior, micromeritic properties, surface morphology, and in-vitro drug release.
Although natural polymers offer many advantages, certain challenges such as high viscosity, batch variability, heat sensitivity, and regulatory quality requirements must be carefully managed. Proper standardization and controlled processing help overcome these limitations.
Overall, the use of crude drugs as an approach in microballoon formulation provides a safe, effective, and sustainable strategy for developing gastroretentive drug delivery systems with improved therapeutic outcomes.
Crude drugs are used in microballoon formulations as natural polymers or actives due to their swelling, gel-forming, and mucoadhesive properties, which enhance gastric retention and controlled drug release.
Applications
Microballoons formulated using crude drugs are especially useful in:
Applications of Microballoons
Microballoons enhance gastric pharmacotherapy by enabling localized and sustained drug release at the gastric mucosa. This makes them highly effective in the treatment of Helicobacter pylori infections, gastric and duodenal ulcers, gastritis, and gastroesophageal reflux disease.
Floating and bioadhesive microballoons containing acetohydroxamic acid and hollow microspheres of ranitidine hydrochloride have been successfully developed for gastric ulcer treatment. Microballoons are particularly advantageous for poorly soluble and weakly basic drugs, as prolonged gastric retention improves dissolution and absorption.
Drugs such as verapamil hydrochloride, tranilast, melatonin, metoclopramide, and glipizide show enhanced bioavailability when delivered via gastroretentive microballoon systems. Additionally, microballoons are effective carriers for drugs with narrow absorption windows, including antibiotics, antifungals, antivirals, and NSAIDs such as indomethacin, where sustained release also reduces gastric irritation.
Microballoons are evaluated for micromeritic properties, buoyancy, swelling, release kinetics, and in-vivo performance and are widely applied in gastroretentive, controlled drug delivery systems.
Limitations of Microballoons
Despite their advantages, microballoon formulations have certain limitations. Controlled-release systems generally contain higher drug loads, and any compromise in formulation integrity may result in dose dumping and potential toxicity. Drug release can be influenced by food intake and gastrointestinal transit time. These dosage forms should not be crushed or chewed, and batch-to-batch variations may cause differences in release profiles.
Evaluation of Microballoons
Microballoons are evaluated for various parameters including:
These evaluations ensure uniformity, stability, and performance of the formulation.
Evaluation of Microballoons
Micromeritic Evaluation
Micromeritic analysis is carried out to assess the physical characteristics, flow behavior, and packing properties of microballoons, which are critical for formulation handling and processing. Parameters such as particle size and shape, bulk density, tapped density, Hausner’s ratio, Carr’s index, porosity, and angle of repose are commonly evaluated.
The particle size distribution of microballoons is determined using optical microscopy by measuring approximately 200–300 particles with a calibrated ocular micrometer to calculate the mean particle diameter. True density is measured using a liquid displacement method or a helium densitometer. Bulk and tapped densities are determined using a bulk density apparatus by recording volume changes upon tapping.
The Carr’s compressibility index is calculated using the following equation:
I = Vb – Vt X 100
Vb
where (V_b) represents the bulk volume and (V_t) represents the tapped volume. A Carr’s index value below 15% indicates good flow properties, whereas values above 25% indicate poor flowability.
The porosity (e) of microballoons is calculated using the equation:
e = [1- (Tapped Density)] X 100
True Density
The angle of repose, which reflects the flow characteristics of the powder, is measured using the fixed funnel method. The hollow structure and surface morphology of microballoons are confirmed using scanning electron microscopy (SEM).
In-Vitro Buoyancy Study
In-vitro buoyancy studies are performed to evaluate the floating efficiency of microballoons in simulated gastric conditions. A known quantity of hollow microspheres is placed in 900 mL of 0.1 N hydrochloric acid and agitated at 100 rpm for 8–10 hours using a dissolution apparatus.
After the test duration, floating and settled microspheres are separated by filtration, dried until constant weight, and weighed individually. The percentage buoyancy is calculated using the following formula:
Buoyancy (%) = Wf X 100
(Wf + Ws)
where (W_f) is the weight of floating microspheres and (W_s) is the weight of settled microspheres.
Scanning Electron Microscopy
For SEM analysis, dried hollow microspheres are mounted on a brass stub and coated with a thin layer of gold using an ion sputter. The samples are examined under a scanning electron microscope at an accelerating voltage of 20 kV to study particle shape, surface texture, size, and internal hollowness.
In-Vitro Drug Release Studies
The drug release profile of microballoons is evaluated using a USP XXIII basket-type dissolution apparatus. A weighed quantity of microballoons equivalent to the required drug dose is filled into a hard gelatin capsule and placed in the dissolution basket containing an appropriate dissolution medium.
The dissolution medium is maintained at 37 ± 1 °C, and the apparatus is operated at a specified rotation speed under sink conditions. Samples (5 mL) are withdrawn at predetermined time intervals and analyzed using liquid chromatography or mass spectrometry techniques. The withdrawn volume is replaced with fresh dissolution medium. All experiments are conducted in triplicate.
Drug Release Kinetic Analysis
To elucidate the drug release mechanism, dissolution data are fitted to various kinetic models, including:
The most appropriate release model is selected based on correlation coefficients using PCP Disso v3 software.
Swelling Studies
Swelling studies are conducted to evaluate the hydration and expansion behavior of polymers used in microballoons, which significantly affects buoyancy and drug release. These studies are performed using a USP dissolution apparatus, optical microscopy, and advanced analytical techniques such as ¹H-NMR imaging, confocal laser scanning microscopy (CLSM), cryogenic SEM, and light scattering imaging.
The swelling ratio is calculated using the equation:
Swelling ratio = Weight of wet formulation
Weight of dry formulation
In-Vivo Evaluation
In-vivo studies are carried out using suitable animal models such as rats or beagle dogs to assess gastric retention and floating behavior. Radiographic imaging with barium sulphate-loaded microballoons is commonly employed to visualize the location and retention time of microballoons in the stomach.
Crude Drug–Based Microballoons with GRDDS
Gastroretentive drug delivery systems (GRDDS) are designed to prolong the residence time of dosage forms in the stomach in order to enhance drug bioavailability, reduce dosing frequency, and achieve site-specific drug delivery. Microballoons, as a non-effervescent floating system, are an important class of GRDDS, and the use of crude drugs or natural polymers further strengthens their gastroretentive performance.
Natural polymers obtained from crude drugs possess swelling, gel-forming, and mucoadhesive properties, which directly support the fundamental principles of GRDDS. When crude drug–based polymers such as alginate, chitosan, gums, or mucilages are used in microballoon formulations, they hydrate in gastric fluid to form a gel barrier that lowers the system density and promotes buoyancy, thereby enabling the dosage form to float on gastric contents for an extended period. This floating behavior is a key requirement of GRDDS for resisting gastric emptying.
In addition, the mucoadhesive nature of many crude drug polymers enhances contact with the gastric mucosa, further improving gastric retention time. The prolonged gastric residence ensures controlled and sustained drug release at the desired site, which is a major objective of GRDDS, particularly for drugs that are absorbed in the stomach or upper gastrointestinal tract.
Crude drugs also contribute to the controlled release mechanism of GRDDS by forming a hydrated polymeric matrix that regulates drug diffusion and polymer erosion. This results in minimized plasma drug level fluctuations and improved therapeutic efficacy. Moreover, the natural origin of crude drug polymers improves biocompatibility and safety, which is highly desirable for long-term gastroretentive therapy.
Thus, the integration of crude drugs into microballoon formulations provides a synergistic approach to GRDDS, where floating ability, gastric retention, controlled release, and patient safety are achieved simultaneously. This correlation highlights the potential of crude drug-based microballoons as an effective and sustainable gastroretentive drug delivery strategy.
Crude drug–based microballoons enhance GRDDS by improving buoyancy, mucoadhesion, gastric retention, and controlled drug release through natural polymer hydration and gel formation.
Clinical Relevance of Crude Drug–Based Microballoons in GRDDS
The clinical importance of gastroretentive drug delivery systems (GRDDS) lies in their ability to retain the dosage form in the stomach, thereby improving drug absorption, therapeutic efficacy, and patient compliance. Microballoons formulated using crude drugs or natural polymers show significant clinical advantages in the treatment of several chronic and site-specific conditions.
1. Anti-ulcer Therapy
Anti-ulcer drugs such as ranitidine, famotidine, omeprazole, and sucralfate require prolonged gastric residence to exert their therapeutic effect by reducing acid secretion or protecting the gastric mucosa. Crude drug–based microballoons float in gastric fluid and release the drug slowly, ensuring localized and sustained action in the stomach. Natural polymers with gastroprotective and mucoadhesive properties further enhance mucosal contact, leading to improved ulcer healing and reduced dosing frequency.
2. Antibiotics for Gastric Infections
Antibiotics used in the treatment of Helicobacter pylori–associated gastric infections, such as amoxicillin, clarithromycin, metronidazole, and tetracycline, benefit greatly from GRDDS. Microballoons prolong gastric residence time, maintaining high local drug concentration in the stomach, which enhances bacterial eradication and reduces the risk of antibiotic resistance. Crude drug polymers help control drug release and improve stability in acidic gastric conditions.
3. Antihypertensive Drugs
Certain antihypertensive drugs, including propranolol, verapamil, and nifedipine, are absorbed primarily in the upper gastrointestinal tract. Microballoon-based GRDDS enhance their bioavailability by prolonging gastric retention and providing sustained drug release, resulting in stable plasma drug levels. This reduces dosing frequency and minimizes fluctuations in blood pressure, improving patient compliance in long-term hypertension management.
Clinical Significance
By combining the floating capability of microballoons with the swelling, gel-forming, and mucoadhesive properties of crude drug–derived polymers, GRDDS achieves:
Thus, crude drug–based microballoons represent a clinically effective and patient-friendly gastroretentive delivery system for the management of gastric disorders, infections, and chronic cardiovascular conditions.
Crude drug–based microballoons enhance GRDDS effectiveness in anti-ulcer therapy, gastric antibiotics, and antihypertensives by prolonging gastric retention and providing controlled, site-specific drug release.
Marketed Formulations of Microballoons
Several drugs are commercially available in the form of floating microballoon systems, including formulations of Nizatidine, Propranolol hydrochloride, Domperidone, and Theophylline, marketed by reputed pharmaceutical companies. These products demonstrate the clinical relevance and commercial feasibility of microballoon-based drug delivery systems.
Table: Clinical Relevance of Microballoon-Based GRDDS
|
Therapeutic Category |
Drug Examples |
Clinical Problem |
Benefit of Microballoons (GRDDS) |
|
Anti-ulcer agents |
Ranitidine, Famotidine, Omeprazole, Sucralfate |
Short gastric residence and frequent dosing |
Prolonged gastric retention enables sustained local action, improved ulcer healing, reduced dosing frequency |
|
Antibiotics (H. pylori therapy) |
Amoxicillin, Clarithromycin, Metronidazole, Tetracycline |
Low gastric residence reduces eradication efficiency |
Maintains high local drug concentration in stomach, improves bacterial eradication, reduces resistance |
|
Antihypertensive drugs |
Propranolol, Verapamil, Nifedipine |
Narrow absorption window in upper GIT |
Enhanced bioavailability, sustained plasma levels, better blood pressure control |
|
Drugs unstable in intestine |
Erythromycin, Levodopa |
Degradation at intestinal pH |
Retention in acidic stomach improves stability and therapeutic effect |
|
Drugs for local gastric action |
Antacids, Cytoprotective agents |
Need site-specific delivery |
Floating microballoons ensure localized and prolonged gastric action |
Microballoon-based gastroretentive drug delivery systems are clinically beneficial for drugs that require prolonged gastric residence, localized stomach action, or absorption in the upper gastrointestinal tract. By floating on gastric fluid and releasing the drug in a controlled manner, microballoons improve therapeutic efficacy, bioavailability, and patient compliance in the treatment of gastric disorders, infections, and chronic cardiovascular diseases.
Microballoon-based GRDDS improve treatment of ulcers, gastric infections, and hypertension by prolonging gastric retention and providing controlled, site-specific drug release.
CONCLUSION
Microballoons represent a promising and innovative gastroretentive drug delivery system due to their low density, high buoyancy, and controlled drug release characteristics. They remain afloat over gastric contents for extended periods without causing gastrointestinal irritation, leading to reduced fluctuations in plasma drug concentration and enhanced therapeutic outcomes. Hollow microballoons offer significant potential in targeted drug delivery, diagnostics, gene and genetic material delivery, and safe in-vivo applications. Optimized microballoon formulations thus serve as an effective and reliable approach for prolonged gastric retention and improved drug bioavailability.
REFERENCES

Shaikh Nasima, Dr. Vishal Kshirsagar, Dr. Kshitija Deshmukh, A Comprehensive Overview of Gastric Approaches to MircoBalloon, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 2, 3145-3161. https://doi.org/10.5281/zenodo.18703534
 10.5281/zenodo.18703534
10.5281/zenodo.18703534
