Pydah College of Pharmacy, Patavala, Kakinada-Yanam Road, Kakinada, E.GT, Andhra Pradesh.
The skin is the largest organ of the human body and plays an important role in protection, thermoregulation, and maintaining homeostasis. Hair follicles present in the skin are responsible for hair growth and sebum secretion. When these follicles become infected or inflamed, a common skin condition known as folliculitis occurs. Folliculitis is mainly caused by microorganisms such as Staphylococcus aureus and is characterized by redness, itching, and pus-filled lesions around hair follicles. Conventional treatments such as antibiotics and antiseptic creams are commonly used but may cause side effects like skin irritation, dryness, and antimicrobial resistance after prolonged use. Therefore, there is increasing interest in herbal formulations for the treatment of skin disorders due to their safety, effectiveness, and minimal side effects. The present study focuses on the formulation and evaluation of a polyherbal gel containing Phyllanthus emblica (Amla), Eclipta alba (Bhringraj), Melaleuca alternifolia (Tea Tree Oil), and Simmondsia chinensis (Jojoba Oil) for the management of folliculitis. These herbal ingredients possess antibacterial, anti-inflammatory, antioxidant, and wound-healing properties. The herbal gel formulation is expected to enhance topical drug delivery, reduce microbial infection, relieve inflammation, and promote healing of affected follicles. Herbal gels are preferred due to their non-greasy nature, good spreadability, cooling effect, and better skin absorption. This study aims to develop a safe, effective, and natural alternative treatment for folliculitis while supporting the use of traditional herbal medicine in modern pharmaceutical formulations.
The skin is the largest organ of the human body and serves as a vital barrier that protects internal tissues from physical damage, harmful microorganisms, ultraviolet radiation, and chemical substances. It plays an essential role in thermoregulation, sensation, and the maintenance of homeostasis. Structurally, the skin is composed of three primary layers — the epidermis, dermis, and hypodermis each performing specialized functions that ensure overall skin health and protection.
Embedded within the dermis are numerous appendages such as hair follicles, sebaceous glands, and sweat glands, which work together to maintain the physiological integrity of the skin. Among these, hair follicles are highly specialized structures responsible for the growth of hair shafts. They are also involved in sebum secretion and serve as minor excretory and thermoregulatory organs. Each hair follicle consists of a hair bulb, root, and shaft, and is nourished by a rich supply of blood vessels and nerves. The normal functioning of these follicles is crucial for maintaining healthy skin and hair, antiseptic washes, and corticosteroid creams. Although effective, prolonged use of such chemical-based treatments can cause antimicrobial resistance, skin irritation, dryness, and allergic reactions. Furthermore, synthetic formulations often disrupt the natural skin microbiome and barrier function, leading to further complications.
In recent years, there has been a growing global shift toward herbal and natural remedies for managing skin disorders. Herbal medicines, However, when these follicles become infected, inflamed, or blocked, they give rise to various dermatological conditions, one of the most common being folliculitis. Folliculitis is defined as the inflammation of one or more hair follicles, resulting in the formation of small, red, or pus-filled lesions. The condition may be superficial, affecting only the upper part of the follicle, or deep, involving the entire follicular structure and surrounding tissue.
The most frequent causative organism associated with folliculitis is Staphylococcus aureus, a Gram-positive bacterium that naturally inhabits the skin surface but can penetrate hair follicles through micro-abrasions or damaged skin. Other microbial agents such as Pseudomonas aeruginosa, Malassezia furfur (yeast), and even viruses like herpes simplex can also contribute to folliculitis. In addition to infectious causes, mechanical irritation, occlusion by cosmetics or tight clothing, excessive sweating, and poor hygiene are also important predisposing factors.
Clinically, folliculitis is characterized by itching, tenderness, erythema (redness), and pustule formation around hair follicles. In severe cases, lesions can coalesce to form painful boils or abscesses. Repeated or chronic infections may lead to scarring alopecia, post-inflammatory pigmentation, and a significant impact on the patient’s self-esteem and comfort.
Conventional treatment options for folliculitis typically include topical or systemic antibiotics, antifungal agents derived from plant sources, offer a holistic approach to healing by addressing not just the symptoms but also the underlying causes of inflammation and infection. They are generally biocompatible, cost-effective, and free from major side effects, making them an attractive alternative to modern synthetic drugs.
Plants are rich in phytochemicals such as flavonoids, tannins, alkaloids, terpenoids, and phenolic acids, which exhibit a broad spectrum of biological activities including antibacterial, antifungal, antioxidant, anti-inflammatory, and wound-healing properties. These properties make them highly effective for the management of inflammatory and infectious skin diseases like folliculitis.
Formulating these herbal extracts into a gel base enhances their topical delivery and therapeutic efficiency. Herbal gels are preferred over creams or ointments due to their non-greasy texture, excellent spreadability, cooling effect, and fast absorption through the skin. They also help maintain skin hydration and provide prolonged contact time of the active ingredients on the affected area.
The present study aims to formulate and evaluate a polyherbal gel composed of Phyllanthus emblica (Amla), Eclipta alba (Bhringraj), Melaleuca alternifolia (Tea Tree Oil), and Simmondsia chinensis (Jojoba Oil) for the effective healing of folliculitis. Each of these herbs contributes distinct but complementary therapeutic actions that, when combined, exhibit a synergistic healing effect:
The synergistic combination of these herbal ingredients aims to control microbial infection, reduce inflammation, promote wound healing, and restore follicular health, offering a safe and effective alternative to conventional therapies.
By developing and evaluating this herbal gel, the study not only addresses the growing need for natural dermatological formulations but also supports the integration of traditional medicinal knowledge with modern pharmaceutical techniques. Such herbal innovations represent a sustainable and patient-friendly approach toward the management of folliculitis and other inflammatory skin conditions.
HISTORY OF FOLLICULITIS
The term “folliculitis” originates from the Latin word “folliculus,” meaning small bag or sac, referring to the hair follicle, the tiny structure within the skin responsible for hair growth. The suffix “-itis” denotes inflammation. Hence, folliculitis literally means inflammation of the hair follicle.
The history of folliculitis dates back to the early stages of medical science when skin infections and pustular eruptions were first described in ancient civilizations. Although the condition was not specifically termed folliculitis at that time, ancient medical practitioners across different cultures had observed and documented inflammatory eruptions associated with hair-bearing regions of the body.
1. Early Descriptions in Ancient Medicine
In Ayurvedic texts such as the Sushruta Samhita and Charaka Samhita (circa 600–400 BCE), conditions resembling folliculitis were described under the category of “Pidaka” or “Kustha” localized inflammatory lesions characterized by redness, pus formation, and pain. These conditions were believed to arise from vitiation of the doshas (Vata, Pitta, and Kapha) and the accumulation of toxins (ama) in the body. Herbal remedies, detoxifying therapies, and lifestyle modifications were recommended to balance these elements and purify the blood.
Similarly, in Traditional Chinese Medicine (TCM), skin pustules resembling folliculitis were recorded under the term “Furuncle” or “Yang Du,” believed to result from heat toxins and damp stagnation. Treatment methods included the use of cooling herbs, acupuncture, and topical plant-based pastes to drain pus and restore skin balance.
Ancient Greek and Roman physicians, including Hippocrates (460–370 BCE) and Galen (129–200 CE), also described inflammatory skin lesions in their medical writings. Hippocrates emphasized that the obstruction of pores and infection of sweat glands or hair roots could lead to pustular eruptions — an early recognition of folliculitis-like infections.
2. Development in Medieval and Early Modern Periods
During the Middle Ages (5th–15th centuries), follicular infections were poorly understood and often grouped with other pustular skin diseases such as boils, carbuncles, and abscesses. Physicians at that time attributed these conditions to “impurities of the blood” or imbalances in bodily humors, consistent with the humoral theory that dominated pre-modern medicine.
With the advent of the microscope in the 17th century, scientists began to observe the microscopic structure of skin and hair follicles. This discovery laid the foundation for recognizing the anatomical basis of follicular infections. Early anatomists like Marcello Malpighi (1628–1694) contributed significantly to the understanding of skin histology, identifying the structure of follicles and sebaceous glands.
In the 19th century, as bacteriology emerged as a scientific field, the true cause of folliculitis began to be elucidated. Pioneers such as Louis Pasteur and Robert Koch established the germ theory of disease, proving that infections were caused by microorganisms rather than imbalances in body fluids. Around this time, Staphylococcus aureus was identified as a major pathogen responsible for follicular infections, marking a turning point in the medical understanding of folliculitis.
3. Modern Medical Understanding
By the early 20th century, folliculitis had become a well-recognized dermatological condition, distinguished from other pustular disorders such as acne vulgaris and furunculosis. Dermatologists classified folliculitis into several types based on depth, causative organism, and clinical presentation, such as:
Non-infectious folliculitis caused by chemical irritants or physical trauma
Microscopic and culture-based diagnostic methods were developed to identify the specific pathogens responsible. With advances in antibiotic therapy in the mid-1900s, particularly the discovery of penicillin, folliculitis could be effectively treated, significantly reducing severe infections and scarring.
However, the widespread and sometimes inappropriate use of antibiotics led to the emergence of antibiotic-resistant strains of Staphylococcus aureus, such as MRSA (Methicillin-Resistant Staphylococcus aureus). This development renewed medical interest in alternative and complementary treatments, including herbal and natural therapies with antimicrobial potential.
4. Evolution of Herbal and Natural Remedies
While modern dermatology focused on antibiotics and antiseptics, traditional systems of medicine continued to rely on plant-based formulations to manage folliculitis and other skin infections.
In Ayurveda, herbs like Amla (Phyllanthus emblica), Bhringraj (Eclipta alba), Neem (Azadirachta indica), and Turmeric (Curcuma longa) were used for their antibacterial, antioxidant, and anti-inflammatory properties. Similarly, in Unani and Siddha medicine, herbal pastes and oils were applied to soothe inflamed follicles and prevent recurrence.
In the 21st century, with increasing awareness about the side effects of synthetic drugs and the rise of antimicrobial resistance, research has refocused on herbal extracts, essential oils, and polyherbal gels for treating folliculitis. Modern analytical techniques such as HPLC, GC-MS, and UV spectroscopy have enabled the identification and standardization of active phytoconstituents, bridging traditional knowledge and scientific validation.
5. Current Perspective
Today, folliculitis is recognized not just as a simple infection but as a multifactorial disorder influenced by microbial invasion, inflammation, oxidative stress, and skin barrier dysfunction. Treatment strategies emphasize antimicrobial, anti-inflammatory, and antioxidant approaches all of which can be effectively achieved through herbal therapy.
Herbal formulations are now being studied extensively for their potential to heal follicular inflammation naturally, providing safe, non-toxic, and sustainable alternatives to conventional chemical treatments. This revival of traditional wisdom through modern research represents a significant step forward in the holistic management of skin and hair follicle disorders.
EARLY SYMPTOMS OF FOLLICULITIS
Folliculitis is an inflammatory disorder of the hair follicles that can occur on any part of the body where hair grows. The early symptoms of folliculitis often begin subtly and may resemble mild skin irritation, but gradually progress into visible lesions if left untreated. Identifying these symptoms in the initial stages is crucial for preventing the spread of infection, reducing discomfort, and avoiding complications such as abscess formation or scarring.
1. Initial Stage: Mild Irritation and Redness
2. Formation of Small Red or White Bumps
3. Itching and Discomfort
4. Tenderness and Localized Pain
5. Swelling and Localized Warmth
6. Development of Crusts and Scaling
7. Commonly Affected Areas
8. Differences Between Mild and Deep Folliculitis
9. Systemic Symptoms (in Severe or Widespread Cases)
Although rare in the early stage, if the infection spreads or becomes severe, individuals may experience:
10. Importance of Early Detection
Causes of Folliculitis
Folliculitis is the inflammation or infection of hair follicles, which can occur due to multiple factors. Understanding the causes is essential for prevention, treatment, and formulation of herbal therapies.
1. Microbial Infection
Bacterial: The most common cause is Staphylococcus aureus, which infects hair follicles and leads to red, pus-filled bumps.
Fungal: Candida species or dermatophytes can cause fungal folliculitis, especially in moist areas.
Viral: Rarely, viruses such as herpes simplex may lead to follicular inflammation.
2. Physical and Mechanical Factors
Shaving or Waxing: Damages hair follicles, making them prone to infection.
Friction from tight Clothing: Continuous rubbing irritates follicles, causing pseudofolliculitis barbae.
Excessive Sweating: Creates a warm, moist environment favorable for microbial growth.
3. Environmental and Lifestyle Factors
Hot Tubs and Pools: Improperly treated water can cause Pseudomonas folliculitis (hot tub rash).
Humidity and Heat: Promote bacterial and fungal growth on the skin.
Poor Hygiene: Accumulation of sweat, dirt, and oils can block follicles and trigger infection.
4. Immune and Medical Conditions
Immunocompromised Individuals: People with HIV, diabetes, or undergoing chemotherapy are more susceptible.
Use of Corticosteroids or Antibiotics: Can disturb skin microbiota, increasing infection risk.
5. Cosmetic and Topical Products
Oily or Comedogenic Lotions and Creams: Can clog follicles, leading to inflammation.
Hair Care Products: Excessive use of gels, waxes, or conditioners may irritate follicles.
Types of Folliculitis
Folliculitis is the inflammation or infection of hair follicles. It can be classified based on cause (infectious or non-infectious) and depth (superficial or deep).
1. Superficial Folliculitis
Affects only the upper part of the hair follicle. Common and mild.

Cause: Staphylococcus aureus (most common).
Symptoms: Small, itchy pustules or red bumps with pus at the center.
Common sites: Scalp, face, arms, legs.

Cause: Pseudomonas aeruginosa (from contaminated water in hot tubs/pools).
Symptoms: Red, itchy bumps or pustules, especially on areas covered by swimwear.

Cause: Yeast (Malassezia furfur).
Symptoms: Itchy, acne-like eruptions on back, chest, shoulders.
Common in: Hot, humid climates or oily skin.


Cause: Shaving or friction that irritates follicles.
Symptoms: Small, inflamed bumps or ingrown hairs, mostly on beard area or legs.
2. Deep Folliculitis
Involves the whole hair follicle and surrounding tissue; more painful and severe.

Cause: Staphylococcus aureus infection in beard area.
Symptoms: Deep pustules, crusts, and scarring in bearded men.
Cause: Deep Staphylococcus infection.
Furuncle: Single painful nodule with pus.
Carbuncle: Cluster of interconnected boils.

Cause: Gram-negative bacteria (e.g., Klebsiella, Enterobacter).
Occurs in: People with long-term antibiotic or acne treatment.
Symptoms: Sudden acne flare-ups around nose and mouth.
Eosinophilic Folliculitis

Cause: Immune response (often in HIV patients or immunocompromised people).
Symptoms: Itchy, red papules or pustules, especially on face and upper body.

Causes:
Occlusion (tight clothing, heavy creams)
Heat and sweat (occlusive folliculitis)
Chemicals (contact dermatitis)
Symptoms: Red bumps or pustules without infection.
DIAGNOSIS OF FOLLICULITIS
Accurate diagnosis of folliculitis is essential to distinguish it from other skin conditions such as acne, boils (furuncles), carbuncles, eczema, or contact dermatitis, and to ensure the appropriate management and treatment. Folliculitis can range from mild, self-limiting superficial infections to deep, recurrent, or chronic infections. Therefore, proper evaluation involves a combination of clinical examination, laboratory tests, and sometimes imaging studies.
The first and most important step in diagnosing folliculitis is a thorough physical examination of the affected skin area. Dermatologists assess:
Small, red or white bumps (papules or pustules) centered around hair follicles.
Lesions may be dome-shaped, slightly raised, or filled with pus.
Folliculitis commonly affects hair-bearing areas such as the scalp, beard, neck, chest, back, thighs, buttocks, and armpits.
Patterns may indicate the type of folliculitis — for example, hot tub folliculitis is often distributed on areas exposed to contaminated water.
Redness (erythema), tenderness, warmth, swelling, or crust formation.
Early diagnosis can detect minimal crusting, scaling, or post-inflammatory pigmentation before chronic scarring develops.
Dermatologists also gather a history of recent shaving, waxing, tight clothing, sweating, or exposure to hot tubs or contaminated water, which may trigger folliculitis.
2. Laboratory Investigations
When clinical examination is insufficient to determine the causative organism, laboratory tests are used to confirm the diagnosis and guide treatment. Common investigations include:
a. Microscopy
Gram Staining: Detects bacterial organisms such as Staphylococcus aureus in pus or exudate from the pustules.
KOH (Potassium Hydroxide) Test: Used to identify fungal folliculitis caused by dermatophytes or Malassezia species.
b. Culture Tests
Bacterial Culture: Swabs from pustules are cultured on appropriate media to identify the bacterial species and determine antibiotic susceptibility.
Fungal Culture: Samples can be grown on Sabouraud Dextrose Agar to detect fungal pathogens.
c. Sensitivity Testing
Determines which antibiotics or antiseptics will be effective, especially in cases of recurrent or resistant infections
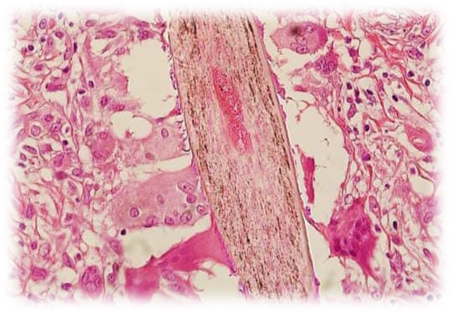
3. Histopathological Examination
In rare or severe cases, a biopsy of the affected follicle may be performed for histopathology. This helps distinguish folliculitis from other follicular disorders, such as:
Microscopic examination may reveal neutrophilic infiltration, abscess formation within the follicle, and perivascular inflammation, which confirms folliculitis.
4. Imaging Studies
Imaging is not commonly required but may be useful in deep or recurrent infections, especially when abscesses or sinus tracts are suspected:
Ultrasound: Detects abscess formation or deep follicular involvement.
MRI or C T Scan: Reserved for extensive infections affecting deeper tissues in rare cases.
5. Differential Diagnosis
Diagnosing folliculitis requires distinguishing it from conditions with similar presentations, including:
Condition Distinguishing Features
6. Role of Early Diagnosis
7. Integration with Herbal Treatment
Treatment of Folliculitis
The management of folliculitis depends on its cause, severity, and recurrence. Treatment strategies can be conventional, supportive, or herbal-based.
1. Conventional Treatment
Topical Antibiotics: Creams or ointments containing mupirocin, fusidic acid, or clindamycin for mild bacterial infections.
Oral Antibiotics: Prescribed for widespread or recurrent infections, especially those caused by Staphylococcus aureus.
Antifungal Agents: Used for fungal folliculitis (e.g., ketoconazole, clotrimazole).
Cleansing and Hygiene: Regular washing with antiseptic solutions to reduce microbial load.
Avoidance of Triggers: Avoid tight clothing, excessive shaving, and exposure to contaminated water.
2. Supportive Measures
Topical antiseptics such as chlorhexidine or benzoyl peroxide.
Soothing agents to relieve itching and inflammation.
Warm compresses to promote drainage of pustules.
3. Herbal / Natural Treatment
Herbal Gels and Pastes: Contain antimicrobial and anti-inflammatory plant extracts.
Benefits: Reduce redness, control microbial infection, promote healing, and prevent recurrence.
Common Herbs Used: Amla, Bhringraj, Neem, Turmeric, Tea Tree Oil, Jojoba Oil.
4. Integrated Approach
Mild cases: May respond to herbal gels alone.
Moderate to severe cases: Can combine herbal therapy with topical antibiotics to enhance healing and reduce side effects.
Herbal Gel Formulation
While understanding the history, symptoms, and diagnosis of folliculitis provides a foundation for managing the condition, modern approaches increasingly focus on natural and safe alternatives to conventional treatments. Medicinal herbs, known for their antimicrobial, anti-inflammatory, and healing properties, offer an effective solution for follicular inflammation.
This study emphasizes the use of a polyherbal gel combining Amla, Bhringraj, Tea Tree Oil, and Jojoba Oil, which work synergistically to control infection, reduce inflammation, and promote skin and follicle health. The following sections describe the properties of these herbs, the method of gel preparation, and its evaluation for treating folliculitis.
Phyllanthus emblica (Amla)

1. Botanical Overview
Common Names: Amla, Indian Gooseberry
Scientific Name: Phyllanthus emblica .
Family: Phyllanthaceae
Species: Phyllanthus emblica
Amla is a small to medium-sized deciduous tree native to India and Southeast Asia. It produces round, greenish-yellow fruits known for their high vitamin C content and potent medicinal properties. The plant is widely used in Ayurvedic, Unani, and Siddha medicine for its therapeutic effects on hair, skin, and overall health.
2. Main Active Components
The therapeutic properties of Amla are attributed to its rich phytochemical composition, including:
Vitamin C (Ascorbic Acid): Powerful antioxidant that supports collagen synthesis and tissue repair.
Tannins: Contribute to antimicrobial and astringent activity.
Flavonoids (Quercetin, Kaempferol): Anti-inflammatory and antioxidant effects.
Phenolic compounds: Aid in reducing oxidative stress and promote skin and follicle health.
Minerals (Calcium, Phosphorus, Iron): Support cellular metabolism and repair.
3. Traditional Uses
4. Modern Uses and Research
Recent studies have validated many traditional claims and revealed additional benefits:
Antioxidant Activity: Protects skin cells from oxidative stress and aging.
Anti-inflammatory Effects: Reduces inflammation in skin conditions including folliculitis.
Antibacterial Properties: Effective against Staphylococcus aureus and other skin pathogens.
Wound Healing: Promotes tissue regeneration and repair of minor skin lesions.
Cosmetic Applications: Incorporated in lotions, creams, and gels for skin rejuvenation and hair care.
5. Mechanism of Action in Folliculitis
Amla contributes to the healing of folliculitis through multiple mechanisms:
1. Antimicrobial Action: Reduces bacterial growth in inflamed hair follicles.
2. Anti-inflammatory Action: Calms redness, swelling, and irritation.
3. Antioxidant Activity: Neutralizes free radicals, supporting faster skin and follicle recovery.
4. Collagen Stimulation: Improves skin structure and resilience, promoting healing of micro-lesions around hair follicles.
6. Application in Herbal Gel
Extracted using water or ethanol to retain active compounds.
Incorporated into the gel base to deliver antioxidant and anti-inflammatory effects directly to affected follicles.
Synergizes with Bhringraj, Tea Tree Oil, and Jojoba Oil for enhanced antimicrobial and healing action.
Eclipta alba (Bhringraj)

1. Botanical Overview
Common Names: Bhringraj, False Daisy, Bh??garaj
Scientific Name: Eclipta alba
Family: Asteraceae
Species: Eclipta alba
Bhringraj is an annual or perennial herb native to India, commonly found in moist areas and riverbanks. It is highly valued in Ayurvedic medicine for its therapeutic effects on hair, skin, and liver health. The plant has small, oblong leaves, white flowers, and a strong aromatic smell, making it easily recognizable in traditional herbal practices.
2. Main Active Components
Bhringraj’s medicinal properties are due to its rich phytochemical profile, which includes:
Wedelolactone: Antimicrobial, anti-inflammatory, and hepatoprotective activity.
Flavonoids: Antioxidant and anti-inflammatory effects.
Alkaloids and Coumestans: Provide antimicrobial and healing properties.
Saponins and Triterpenoids: Promote wound healing and protect skin and hair follicles.
Essential oils: Contribute to antimicrobial and soothing effects.
3. Traditional Uses
4. Modern Uses and Research
Recent studies have validated its traditional applications and discovered new benefits:
Antimicrobial Activity: Effective against Staphylococcus aureus, E. coli, and other skin pathogens.
Anti-inflammatory Effects: Reduces inflammation in skin disorders, including folliculitis.
Antioxidant Properties: Protects hair follicles and skin cells from oxidative stress.
Wound Healing: Promotes faster tissue regeneration and repair in skin injuries.
Cosmetic Applications: Incorporated into hair oils, shampoos, and herbal gels to maintain scalp and follicle health.
5. Mechanism of Action in Folliculitis
Bhringraj aids in folliculitis management through multiple mechanisms:
1. Antimicrobial Action: Inhibits growth of bacteria around inflamed follicles.
2. Anti-inflammatory Effect: Reduces redness, swelling, and discomfort.
3. Antioxidant Protection: Shields follicles and surrounding skin from oxidative damage.
4. Hair Follicle Nourishment: Strengthens follicles and prevents hair loss due to infection or inflammation.
6. Application in Herbal Gel
Leaf extracts are obtained via aqueous or ethanol extraction, retaining active compounds.
Incorporated into the gel to deliver antibacterial, anti-inflammatory, and healing effects directly to affected areas.
Works synergistically with Amla, Tea Tree Oil, and Jojoba Oil, enhancing the overall therapeutic efficacy of the gel.
Melaleuca alternifolia (Tea Tree Oil)

1. Botanical Overview
Common Names: Tea Tree Oil, Melaleuca Oil
Scientific Name: Melaleuca alternifolia
Family: Myrtaceae
Species: Melaleuca alternifoli
Tea Tree Oil is an essential oil extracted from the leaves of the Melaleuca alternifolia tree, native to Australia. The oil is aromatic, pale yellow, and known for its potent antimicrobial properties, making it widely used in traditional medicine, dermatology, and modern natural skincare products.
2. Main Active Components
The therapeutic efficacy of Tea Tree Oil comes from its rich blend of terpenes and alcohols, including:
Terpinen-4-ol: Primary active component responsible for antimicrobial and anti-inflammatory activity.
α-Terpinene, γ-Terpinene: Contribute to antioxidant and antibacterial effects.
1,8-Cineole: Provides mild antimicrobial and soothing properties.
Other monoterpenes and sesquiterpenes: Enhance broad-spectrum antimicrobial activity.
3. Traditional Uses
4. Modern Uses and Research
Scientific studies have confirmed many traditional uses:
Antimicrobial Activity: Effective against Gram-positive and Gram-negative bacteria, including Staphylococcus aureus, a major cause of folliculitis.
Anti-inflammatory Properties: Reduces inflammation and irritation in skin conditions.
Antifungal Effects: Useful in treating fungal folliculitis and other dermal fungal infections.
Cosmetic Applications: Incorporated into shampoos, creams, and gels for skin and hair care.
5. Mechanism of Action in Folliculitis
Tea Tree Oil helps manage folliculitis by:
1. Killing pathogenic bacteria: Penetrates the hair follicle to reduce bacterial load.
2. Reducing inflammation: Calms redness, swelling, and irritation around follicles.
3. Promoting healing: Supports recovery of damaged follicular and skin tissue.
6. Application in Herbal Gel
Added in small concentrations to prevent skin irritation while maintaining antimicrobial potency.
Works in synergy with Amla and Bhringraj to enhance antimicrobial, antioxidant, and anti-inflammatory effects.
Contributes to long-lasting therapeutic action in folliculitis treatment.
Simmondsia chinensis (Jojoba Oil)

1. Botanical Overview
Common Names: Jojoba Oil, Goat Nut Oil
Scientific Name: Simmondsia chinensis
Family: Simmondsiaceae
Species: Simmondsia chinensis
Jojoba Oil is a liquid wax extracted from the seeds of the Jojoba plant, native to Northwestern Mexico and Southern United States. Unlike most plant oils, it is a wax ester, which closely resembles the natural sebum of human skin, making it highly compatible for topical application and cosmetic formulations.
2. Main Active Components
The therapeutic properties of Jojoba Oil are due to its unique chemical composition:
Wax esters (~97%): Mimic natural skin sebum and enhance skin barrier function.
Fatty acids: Oleic acid, gadoleic acid — support moisturization and skin repair.
Vitamins and minerals: Vitamin E, zinc, copper — provide antioxidant protection.
Phenolic compounds: Contribute to anti-inflammatory and antibacterial activity.
3. Traditional Uses
Moisturizer: Hydrates and softens skin, preventing dryness.
Hair care: Strengthens hair shafts, reduces breakage, and promotes scalp health
Wound healing: Applied to minor cuts, burns, and skin irritations.
Anti-inflammatory: Reduces redness and swelling in inflamed skin areas.
4. Modern Uses and Research
Skin Barrier Restoration: Protects and restores the skin’s natural barrier, preventing moisture loss.
Anti-inflammatory and Soothing: Reduces irritation, itching, and inflammation in conditions like folliculitis.
Antioxidant Properties: Protects skin cells from free radical damage.
Cosmetic Applications: Widely used in creams, gels, lotions, and hair serums due to its non-greasy texture and high compatibility with skin.
5. Mechanism of Action in Folliculitis
Jojoba Oil enhances folliculitis treatment by:
1. Maintaining skin hydration: Prevents dryness and cracking around follicles.
2. Anti-inflammatory action: Soothes irritation, redness, and itching.
3. Supporting healing: Promotes recovery of damaged skin and follicle tissues.
4. Synergistic effect: Works with Amla, Bhringraj, and Tea Tree Oil to enhance overall antimicrobial and therapeutic activity.
6. Application in Herbal Gel
Added to the gel to improve spreadability, moisture retention, and skin compatibility.
Ensures the gel is non-greasy, easy to apply, and soothing, making it ideal for sensitive or inflamed skin.
Complements the antimicrobial and healing properties of other herbal ingredients in the gel.
Detailed Methodology — From Raw Materials to Final Gel (100 g batch)
1. Summary of final formulation (target per 100 g)
2. Materials, equipment & safety
Equipment
3. Raw material handling & authentication
3.1 Procurement
Procure P. emblica fruits and E. alba leaves from certified suppliers or authenticated botanical vendors. Request batch certificates if available.
3.2 Botanical authentication
Perform gross botanical checks: morphology, colour, odour. If available, confirm identity via voucher specimen or herbarium reference.
3.3 Cleaning & pre-processing
Remove foreign matter: Manually separate stones, stems, visible dirt.
Wash: Rinse plant material in potable water to remove dust and soil. For leaves, use gentle immersion and draining. For fruits, cut away spoiled portions.
Surface drying: Pat dry with clean cloth to remove excess water.
3.4 Drying
Objective: Reduce moisture to ~8–10% (dry weight) to prevent microbial growth and promote efficient extraction.
Method options:
Shade drying: Spread material in thin layer under shade with good ventilation until crisp (may take several days).
Tray drying: Use hot-air oven at 40–45°C until constant weight (faster, preserve phytoconstituents).
Notes: Avoid temperatures > 45°C to preserve heat-sensitive constituents (vitamin C in Amla is heat labile).
3.5 Size reduction & sieving
Mill the dried material in a grinder to coarse powder. Sieve through 60 mesh to obtain uniform particle size to improve extraction kinetics. Record weight after milling (for yield calculations).
4. Extraction of active constituents
You will prepare hydroalcoholic extracts (70:30 ethanol:water) for both herbs. This solvent system balances polarity to extract a wide range of phytochemicals (phenolics, tannins, flavonoids, etc.).
4.1 Solvent selection & ratio
Solvent: Ethanol : Distilled water = 70 : 30 (v/v). Use analytical grade ethanol.
4.2 Cold maceration (recommended for small labs / preserving heat-sensitive compounds)
Procedure (per herb; scale-up accordingly):
Weigh herb powder: for practical yield, start with 100 g dry powder (adjust per batch). Use a plant:solvent ratio of 1:10 w/v (100 g powder : 1000 mL solvent).
4.3 Alternative: Reflux / Soxhlet extraction (if equipment available)
Soxhlet with ethanol (70%) yields exhaustive extraction but uses heat—use only if heat-stable constituents are targeted and lab has reflux setup.
4.4 Concentration of extract
Concentrate combined filtrates under reduced pressure using a rotary evaporator at bath temperature 40–45°C to remove the bulk of ethanol and reduce volume to a semi-solid mass.
Final drying: remove residual solvent by drying in vacuum oven (40–45°C) until thick, sticky extract (viscous semi-solid) or a concentrated syrup results. Record extract weight to calculate extraction yield:
Yield (%) = (Weight of dry extract / Weight of starting dry powder) × 100.
4.5 Solvent removal & safety
Ensure residual ethanol content is minimized (below safety limits). If possible, analyze residual solvent or allow evaporative drying in fume hood.
4.6 Storage of extracts
Transfer extracts into sterile, amber glass bottles, label (plant name, batch, date, solvent, yield), and store at 4–8°C until use. Use within recommended timeframe to avoid degradation.
5. Preparation of oil components
5.1 Tea tree essential oil handling
Use cosmetic grade tea tree oil. Record batch/lot. Because essential oils are volatile, store in amber glass, tightly capped, at cool temperature. Handle in low-light, ventilated area.
5.2 Jojoba oil
Use cold-pressed, cosmetic-grade jojoba oil. Store similarly.
5.3 Optional: Oil infusion (if using herb-infused oil)
Some formulations prefer oil-extracts (oleoresins). To make a gentle infusion: macerate dried herb in jojoba oil at 40–50°C in water bath for 4–6 hours, filter, and use. (Not necessary here since we use separate extracts + oils.)
6. Preparation of gel base (Carbopol system)
6.1 Principles
Carbopol 940 forms transparent gels when neutralized (with TEA). Hydration and deaeration are critical for smooth texture.
6.2 Procedure — preparing hydrated carbopol (for 100 g final gel)
In a clean beaker, add ~70 mL distilled water (cooled or room temp). Begin stirring with a magnetic stirrer at low speed.
Sprinkle Carbopol 940 — 1.0 g slowly over the vortex to avoid lumps. Continue slow stirring to disperse uniformly.
Allow Carbopol to hydrate and swell for 2–3 hours (or until no dry particles). Keep covered to avoid contamination. Gentle stirring intermittently reduces air entrapment.
Add Glycerin — 5 mL to the hydrated Carbopol and mix to obtain a smooth viscous gel base.
7. Incorporation of extracts, oils, preservative & emulsifier
7.1 Dissolving extracts for addition
If extracts are viscous, pre-dissolve or suspend them in a small volume of distilled water (or a minimal amount of ethanol if not fully water soluble). For instance, dissolve 10 g Amla extract in ~8–10 mL of warm distilled water with gentle stirring until homogeneous. Do the same for 10 g Bhringraj extract.
Note: If extracts contain residual ethanol, ensure compatibility with the gel base and adjust volumes accordingly.
7.2 Emulsifier (if needed)
Since tea tree oil and jojoba oil are hydrophobic, Tween 80 (polysorbate 80) can be used as a solubilizer/emulsifier. Use 2–3 drops (or 0.1–0.3 g) for 100 g batch if separation observed. Alternatively, incorporate oils as fine droplets with high-shear mixing.
7.3 Stepwise incorporation
Place hydrated Carbopol + glycerin on the homogenizer at low speed.
Slowly add the aqueous extracts (Amla and Bhringraj solutions) dropwise to the gel base while stirring gently to avoid aeration. Ensure uniform dispersion.
In a separate small beaker, mix Tea Tree Oil (5 mL) and Jojoba Oil (5 mL) with the chosen emulsifier (few drops of Tween 80) and gently mix to pre-emulsify.
Add the oil mixture slowly to the gel base under moderate stirring or high-shear homogenizer for 2–3 minutes to obtain a fine dispersion.
Add Methylparaben (0.1 g) dissolved in a little warm distilled water to the bulk and mix thoroughly.
8. pH neutralization & final volume adjustment
8.1 pH adjustment
8.2 Final volume / weight
After pH adjustment, add distilled water to bring final weight to 100 g. Mix gently but thoroughly to ensure homogeneity and avoid air bubbles.
9. Deaeration and finishing touches
10. Packaging, labeling & storage
11. Good Manufacturing Practices (GMP) & documentation
12. Waste management & safety disposal
Collect solvent wastes (ethanol) in designated containers and hand over to authorized hazardous waste disposal. Solid plant residues can be composted if free from chemical contamination. Follow institutional biosafety and chemical disposal rules.
13. Troubleshooting & practical tips
14. Scale-up considerations
Maintain herb:solvent and Carbopol:water proportions when scaling. Extraction efficiency and mixing dynamics change with volume—use proportionate mixing times and appropriate homogenizer scale. Record pilot batch date
Mechanism of Action of Herbal Gel in Folliculitis
The formulated polyherbal gel contains Amla, Bhringraj, Tea Tree Oil, and Jojoba Oil, which work synergistically to treat folliculitis. Its action can be described at multiple levels:
antimicrobial, anti-inflammatory, antioxidant, and healing effects.
1. Antimicrobial Action
Tea Tree Oil and Bhringraj provide broad-spectrum antibacterial activity.
When applied, the gel penetrates hair follicles and reduces bacterial growth, particularly against Staphylococcus aureus, the main causative agent of folliculitis.
This helps in preventing infection spread and reducing pus formation.
2. Anti-inflammatory Action
Amla, Bhringraj, and Jojoba Oil have anti-inflammatory properties.
The gel soothes redness, swelling, and itching around affected follicles.
Reduces local irritation and discomfort, improving patient comfort.
3. Antioxidant Effect
Amla and Bhringraj are rich in vitamins, flavonoids, and phenolic compounds.
They neutralize free radicals in inflamed skin, reducing oxidative stress.
Supports faster healing of follicular tissue and prevents damage to surrounding skin.
4. Skin Barrier Protection & Moisturization
Jojoba Oil mimics natural sebum and restores the skin’s barrier function.
Keeps the skin moisturized and flexible, preventing cracking and secondary infections.
Provides a soothing, non-greasy layer over inflamed follicles.
5. Promotion of Healing
The combined effect of antimicrobial, anti-inflammatory, and antioxidant action accelerates healing of damaged hair follicles.
Enhances collagen synthesis and tissue regeneration (primarily from Amla extract).
Prevents recurrence of folliculitis by maintaining healthy follicle and skin environment.
Evaluation:
1. Organoleptic Evaluation (Appearance, Colour, Odour, Texture)
Purpose: Quick sensory check to describe the gel.
Materials: Clean white tile/plate, spatula.
Procedure :Place ~1 g gel on a white tile.
Observe and note: color, clarity/translucency, presence of lumps, phase separation.
Smell gently and note odor intensity (mild/moderate/strong).
Rub a small amount between fingers — note tackiness, greasiness, spread feel.
2. pH Determination
Purpose: Ensure skin-friendly pH (target 5.5–6.5; you earlier targeted 6.0–6.5).
Materials: Digital pH meter (calibrated), distilled water, beaker, magnetic stirrer.
Procedure:
Calibrate pH meter (pH 4.0 & 7.0 buffers).
Prepare 1% w/w gel dispersion: dissolve 1 g gel in 100 mL distilled water (stir until uniform).
Immerse pH electrode and record pH after stabilization (3 min). Repeat in triplicate.
Report: Mean ± SD (n=3).
Acceptance: pH 5.5–6.8 acceptable for topical use; earlier formulation aim 6.0–6.5.
3. Viscosity / Rheology (Brookfield Viscometer / Viscometer alternative)
Purpose: Assess gel flow — affects application and stability.
Materials: Brookfield viscometer (or hand-held viscometer), spindle set, sample beaker, temperature control (room temp).
Procedure (Brookfield):
Allow gel to equilibrate to 25°C ±1°C.
Pour gel into beaker to appropriate level for spindle.
Select spindle (e.g., SC4-18 or as per instrument guidance).
Measure viscosity at 10, 20, 50 rpm (or standard rpm). Record readings after stabilization. Repeat twice.
Report: Viscosity (cP) at specified rpm, include shear dependence (non-Newtonian behavior).
Interpretation: Compare between batches; higher viscosity = firmer gel. No single numeric acceptance — report reproducibility.
4. Spreadability Test (Slip and Spread method)
Purpose: Measure ease of spreading on skin.
Materials: Two glass slides (20 × 20 cm), 100 g weight, stopwatch, scale, sample applicator.
Procedure:
Place 0.5 g gel centrally on lower glass slide.
Place upper slide on top and apply 100 g weight for 1 minute to squeeze gel into uniform film.
Remove weight and attach rope to upper slide; apply a pull with constant force and measure time taken for upper slide to move 7.5 cm. (Alternative: measure diameter of spread after set time).
Calculate Spreadability (S) = (m × l) / t, where m = weight tied to upper slide (g), l = distance (cm), t = time (s).
Report: Spreadability value (higher = better spread).
5. Homogeneity & Visual Microscopic Examination
Purpose: Confirm uniform distribution of ingredients and absence of large particles.
Materials: Light microscope (10–40×), glass slides, coverslips, pipette.
Procedure:
Place a thin film of gel on microscope slide, cover with coverslip.
Examine at 10× and 40× for lumps, undispersed oil globules, crystals or foreign particles.
Note presence/absence and take photomicrographs if possible.
Interpretation: Homogeneous gel shows uniform texture and no large particulate matter.
6. Particle / Oil Globule Size (simple microscope method)
Purpose: Check oil droplet size when emulsified — large droplets may indicate poor stability.
Materials: Light microscope, stage micrometer (if available).
Procedure:
Prepare slide as above.
At 40×, visually estimate largest droplet diameter or capture image and measure using software or compare to micrometer scale.
Report range and mean droplet size (µm) if measurable.
Interpretation: Smaller droplet size → better stability. Qualitative is acceptable for lab scale.
CONCLUSION
The present study entitled “Synergizing Science and Care for Folliculitis Healing by Using Phyllanthus emblica” was designed to formulate, develop, and evaluate a polyherbal gel aimed at the effective treatment of folliculitis. The main goal of this project was to integrate traditional herbal wisdom with modern pharmaceutical formulation techniques to offer a safe, natural, and efficient therapeutic alternative to conventional synthetic drugs.
Folliculitis, being a common yet often recurrent skin disorder, requires treatments that not only target the microbial infection but also soothe inflammation, promote healing, and restore the natural barrier of the skin. Synthetic medications such as antibiotics and corticosteroids, though effective, often lead to side effects such as irritation, dryness, resistance, and disturbance of the skin microbiome. Therefore, the shift toward herbal formulations represents a major advancement in dermatological therapy.
In this study, four herbal ingredients — Phyllanthus emblica (Amla), Eclipta alba (Bhringraj), Melaleuca alternifolia (Tea Tree Oil), and Simmondsia chinensis (Jojoba Oil) — were carefully selected based on their well-documented pharmacological properties. Each herb contributes distinct actions — antioxidant, antimicrobial, anti-inflammatory, emollient, and wound healing — which together exhibit a synergistic therapeutic effect when combined in a gel form.
REFERENCES




P. Lakshmi Suma, B. Mounika, B. Tarakeshwari, B. Samatha, Synergizing Science and Care for Folliculitis Healing by using Phyllanthus emblica, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 3237-3262. https://doi.org/10.5281/zenodo.19229138
 10.5281/zenodo.19229138
10.5281/zenodo.19229138
