1PharmD, St. James College of Pharmaceutical Sciences, Chalakudy
2Assistant Professor, St. James College of Pharmaceutical Sciences, Chalakudy
3HOD, Department of Pharmacy Practice, St. James College of Pharmaceutical Sciences, Chalakudy
Anaemia is a common consequence of chronic renal disease, which affects 10% of the global population. The primary cause of it is the kidneys' diminished capacity to produce enough EPO in response to hypoxia or anemia. The management of anemia and quality of life have improved with the use of ESAs and iron therapy in current treatment. This treatment raises safety concerns as it attempts to bring the hemoglobin level close to normal. HIF-PHIs, or hypoxia-inducible factor (HIF) prolyl hydroxylase domain (PHD) inhibitors, were created as a substitute method and oral treatment for anemia in chronic kidney disease in order to address these issues. Clinical trial data demonstrated no inferiority in correcting anemia when compared to ESAs or a placebo. Improved iron mobilization and utilization, a reduction in LDL cholesterol, and a reduction in major cardiovascular events were among the other benefits for inflammatory patients.
Anaemia is a common side effect of chronic renal disease. The main cause of the condition's increasing prevalence and severity is the sick kidney's inability to produce more EPO in response to hypoxia and/or anaemia. According to the World Health Organisation, anaemia is defined as having fewer red blood cells or a lower than normal concentration of haemoglobin (Hb). As a result, Hb <12 g/dl for females and <13 g/dl for males have been identified. Erythropoiesis-stimulating medications (ESA) and iron supplements were the conventional cornerstones of anaemia treatment. Even though ESAs have decreased the need for blood transfusions, cardiovascular morbidity and mortality, and symptoms associated with severe anaemia of CKD with haemoglobin target levels of 10 to 11 g/dl, higher haemoglobin target levels (i.e., > 13 g/dl) increase the risk of cardiovascular and cerebrovascular events, vascular access thrombosis, progression to end-stage renal disease, and overall mortality. Oral hypoxia-inducible factor (HIF) prolyl hydroxylase inhibitors have become a viable alternative treatment option for anaemia in patients with chronic kidney disease since the role of the HIF pathway in the physiological response to hypoxia was discovered. As a treatment for anaemia, HIF-PHI primarily improves erythropoiesis by altering iron metabolism and increasing endogenous EPO synthesis. This review outlines the mechanism of action, focusing on safety and efficacy, potential advantages when compared with the current anaemia treatment.
MECHANISM OF ACTION OF HIF-PHI
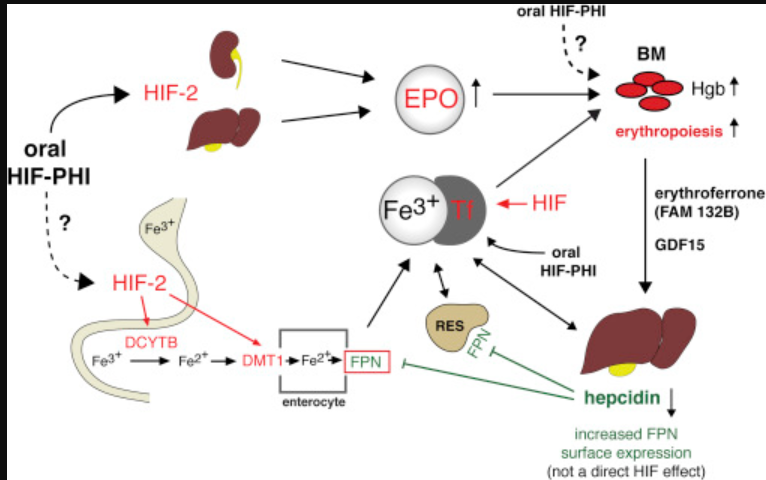
Hypoxia-inducible factor domain inhibitors are exquisite transcription factors that help the body adapt to different oxygen levels by controlling the transcription of over 1000 hypoxia-responsive genes. The HIF pathway is largely responsible for controlling cell-specific responses to hypoxia, including erythropoiesis, iron regulation, angiogenesis, lipid and glucose metabolism, glycolysis, mitochondrial function, cell growth and survival, inflammation, and immunological response. The constitutively expressed β and α subunits make up the heterodimer of hypoxia-inducible factor. HIFα comes in three varieties: HIF1α, HIF2α, and HIF3α. The HIFβ subunit is a nuclear protein that is not oxygenase responsive and has other roles in transcription, even though the HIFα component is highly inducible by hypoxia. The HIF-2α subunit has been shown to be the primary mediator of erythropoiesis. HIF is regulated by the prolyl hydroxylase domain (PHD) enzyme family, which has three isoforms (PHD1, PHD2, and PHD3). O2-oxoglutarate (2-OG) and Fe+ mediate the activity of these enzymes, which serve as cellular oxygen sensors. When iron and/or oxygen are present, PHD enzymes hydroxylate prolines in HIF-α at its C- and N-terminal oxygen-dependent degradation domains (CODD and NODD). This interacts with the von Hippel-Lindau (pVHL) protein-E3 ligase complex to target the protein for proteasomal degradation. Although the hypoxia-inducible factor-α subunit is continuously synthesised, it is immediately degraded in normoxic environments. PHD enzyme activity is inhibited and HIF-α avoids proteasomal breakdown and accumulates in hypoxic or iron-deficient environments. After moving to the nucleus, it joins HIF-β to form the HIF-α/β heterodimer, which binds to target genes' hypoxia response elements and causes erythropoiesis and other reactions. As fibrosis increases in chronic kidney disease, EPO-producing cells become fewer in number and less sensitive to changes in O2 concentration. HIF-2 is the main mediator of the hypoxic activation of erythropoiesis; it also increases the transcription of EPO and activates the expression of genes linked to iron metabolism. Because they boost the liver's production of EPO, which only occurs in a foetus, they are also effective for anephric patients. Although the mechanism of action of all HIF-PHIs is the same, their molecular structures, potencies, time-dependent cell inhibition, and binding to NODD and CODD vary. Roxadustat is an example of a pan inhibitor of PHD isoforms. Daprodustat inhibits all three PHDs, but it preferentially inhibits PHD1 and PHD3. Vadadustat inhibits all three PHDs, but it preferentially inhibits PHD3. Molidustat suppresses PHD2 mainly. PHD dioxygenase has become a major pharmacologic target for the development of HIF-activating compounds through structure-based drug discovery efforts because of their biochemical properties and role in HIF regulation.
THERAPEUTIC USES OF HIF-PHI
HIF-PHI helps patients with CKD anaemia by promoting a robust Hb response. In addition to promoting endogenous EPO, HIF-PHI is expected to have therapeutic effects because HIF transcription factors regulate a variety of hypoxic reactions.
Haemoglobin correction and maintaenance
When administered intravenously, ESA treatment may produce supraphysiological plasma EPO concentrations, which are associated with an increased risk of cardiovascular disease and death in patients with chronic kidney disease. In the placebo comparison trials of non-dialysis dependent patients, Roxadustat increased haemoglobin more, had a higher haemoglobin response, and required less rescue medication during the first 52 weeks of treatment than the placebo. HIF-PHis have consistently shown that they are equally effective at increasing and maintaining haemoglobin levels when compared to ESAs. The ASCEND-ND (NCT02876835) global study, which included 3872 patients and compared daprodustat with darbepoetin alfa, demonstrated a non-inferior change in haemoglobin over a 52-week period, with a between-group difference of 0.08 g/dl (95% CI 0.03–0.13). Daprodustat and roxadustat decreased the need for resuscitation red blood cell transfusions and ESA medication, and they were more effective at achieving and maintaining target haemoglobin levels for up to four years in the placebo-comparator trials. The phase 3 trials demonstrated that all six HIF-PHis (Roxadustat, Daprodustat, Vadadustat, Molidustat, Desidustat, and Enorodustat) were just as successful as ESAs in restoring and preserving haemoglobin levels in dialysis patients with incident and prevalent DD-CKD. The ROCKIES trial (NCT02174731), which involved 2133 dialysis patients, showed that the percentage of time spent with haemoglobin > 10 g/dl was comparable and that roxadustat was not worse than epo-etin alfa (mean increase in haemoglobin of 0.77 versus 0.68 g/dl). In the ASCEND-D trial (NCT02879305), which included 2964 dialysis patients, daprodustat was not less effective than ESA medication in terms of correcting haemoglobin (mean haemoglobin increase of 0.28 versus 0.10 g/dl). ESA rescue was utilised more frequently by the Roxadustat group in the ROCKIES (3.7% versus 0.2%). In the incident INNO2VATE trial, more patients in the Vadadustat group (20.4% versus 16%) required ESA rescue, whereas in the prevalent trial, more patients in the ESA group (27.6% versus 30.2%) required ESA rescue.
Iron Metabolism and hepcidin
In clinical trials, the administration of HIF-Phi was consistently associated with lower serum hepcidin levels, higher serum TF and/or total iron binding capacity, and/or both. Most Phase 3 studies in ND-CKD demonstrated a significant reduction in hepcidin in patients randomly assigned to HIF-PHI by increasing erythropoiesis through inhibition of erythroferrone on bone morphogenetic proteins. Reduced hepcidin is linked to better use of iron stores and increased intestinal iron absorption because HIF activation also regulates the expression of genes encoding for proteins controlling intestinal iron absorption and transportation. Ferritin, a measure of iron metabolism by reticuloendothelial system macrophages, falls in patients on HIF-PHI. Clinically, ferritin levels decreased in the majority of studies that used Roxadustat in a placebo-comparator experiment. While serum and TSAT either stayed the same or increased, total iron binding capacity (TIBC) increased in the Roxadustat group. Taken together, these demonstrate that roxadustat promotes iron mobilisation and erythropoiesis. In incident dialysis patients, roxadustat treatment without iron supplements raised haemoglobin levels early on. However, after seven weeks of the 12-week study period, haemoglobin levels started to plateau at lower levels than in the groups receiving iron treatment. Hb levels were similarly raised and maintained by intravenous (50–62.5 mg/week elemental) and oral (50–195 mg/d elemental) iron supplements. Consequently, HIF-PHI was found to increase TIBC and decrease hepcidin, ferritin, and TSAT without affecting serum iron; these findings lend credence to the hypothesis that HIF-PHI may promote the utilisation of iron from iron storage sites. These effects are consistently displayed by all individual HIF-PHI, suggesting that HIF-PHI has a class influence on iron metabolism.
Elevated inflammatory state
Erythropoiesis is inhibited by inflammation through cytokine-mediated effects on bone marrow, iron metabolism, EPO responsiveness and production, and other mechanisms. The capacity of HIF-PHI to initiate and maintain a Hb response was unaffected by elevated C-reactive protein (CRP) levels. A pooled analysis of three RCTs showed that the Hb change was 2 g/dl in the Roxadustat group and 0.3 g/dl in the placebo group when comparing Roxadustat and placebo in patients with CRP above the upper limit of normal. In addition to its pro-erythropoietic effects, HIF-Phi has been shown to have anti-inflammatory qualities in a variety of disease models, such as sepsis and acute ischaemic injury. The underlying mechanism is complex, highly context-dependent, and most likely involves the HIF pathway interacting with cytokine production, proinflammatory nuclear factor-κB signalling, and modulation of both innate and adaptive immune responses. The safety, efficacy, and dosage requirements of HIF-PHI in patients with underlying inflammation across a wider range of C-reactive protein levels and ESA hyporesponsiveness require further investigation.
Effect on cholesterol
Cholesterol biosynthesis is a high-energy, high-oxygen process. Since increased HIF-1α directly stimulates the transcription of the insulin-induced gene-2 by breaking down the 3-hydroxy-3-methylglutaryl coenzyme. In hypoxic environments, the production of a reductase and cholesterol is inhibited. The synthesis of cholesterol will consequently drastically decrease. An ESA-comparator experiment has shown this ancillary effect; a Japanese study found that the ESA group did not change in LDL and HDL cholesterol levels, but the Daprodustat group did (14). While the LDL cholesterol intergroup differences in DD-CKD patients ranged from -9.7 to -18.3 mg/dl but were consistently significant, those in ND-CKD patients ranged from -9.4 to -27.1 mg/dl and were found to be independent of statin. Other HIF-Phis have not been shown to significantly lower LDL, with the exception of Desidustat. This implies that the pharmacological effect—possibly due to the inhibition of multiple PHD isoforms—may be the cause rather than the class impact.
Health related Quality of Life
Anaemia and lower HRQoL have been strongly linked in numerous studies, and raising Hb levels after taking ESA medication has been shown to significantly improve HRQoL in younger and ND-CKD patients. However, the improvement in HRQoL for Hb > 12g/dl after ESA is greatly reduced, suggesting that the full correction of anaemia by ESA only provides modest advantages over some HRQoL categories. In phase 3 trials comparing Roxadustat with a placebo, ND-CKD patients' HRQoL and functional health scores did not change significantly. In the DOLOMITES study, roxadustat and darbepoetin alfa had identical effects on patient-reported HRQoL measures. The DREAM-D trial revealed that patients taking Desidustat had higher HRQoL scores, but this was not different from the ESA arm. In common dialysis patients with DD-CKD, the PYRENEES trial comparing Roxadusat and ESA therapy showed that the Roxadustat group outperformed the ESA group in terms of improving the patient-reported HRQoL questionnaire.
Another advantage of HIF-Phi is that, unlike ESA therapy, it is taken orally, which eliminates injection site pain and response. Second, erythropoietin will be released as a result of iron mobilisation and absorption, which may lessen the need for iron. Third, the arm veins may be saved for possible future access to haemodialysis, at least in ND-CKD patients.
Safety of Hif-Phi
Systemic inhibition of HIF-PHD may have unfavourable on-target effects because HIF-1 and HIF-2 regulate several biologic processes; these effects will likely depend on the dosage and pharmacokinetics of the HIF-PHI medication. Because the HIF pathway performs a variety of metabolic functions, safety concerns have been raised regarding its continuous activation from HIF-PHIs.The Japanese pharmaceutical and medical devices agency's prescribing guidelines include a safety warning regarding the potential risk of pulmonary embolism, cerebral and myocardial infarction, thromboembolism, and deep vein and vascular access thrombosis with HIF-PHIs. Adverse event rates were comparatively similar in the placebo and HIF-Phi groups, and participants in the placebo-comparator trials for Roxadustat and Daprudostat in NDD-CKD patients were more likely to stop their treatment due to adverse events. Phase 3 active comparator trials for DD-CKD and NDD generally reported adverse effects similar to those of ESA therapy, although participants were more likely to stop because of adverse events in the HIF-Phi arms. In the safety analysis of pooled phase 3 trials in haemodialysis patients, Roxadustat was linked to a higher incidence of thromboembolic events (11.3 vs. 3.9%) than Darbepoetin alfa.
Cardiovascular safety
Patients with chronic kidney disease (CKD) have an increased risk of cardiovascular events, including myocardial infarction and stroke. Even so, preclinical data suggests that systemic HIF activation for a brief period of time provides protection against ischemia injury. When compared to an active comparator (Epoetin or Darbepoetin alfa), cardiovascular risk in HD patients was found to be similar to control. In the ND-CKD cohort, the pooled analysis of three trials comparing Roxadustat with a placebo also revealed a neutral cardiovascular risk. Furthermore, the on-treatment analyses showed a 22% lower risk of MACE+, or MACE plus hospitalization for heart failure, when Roxadustat was compared to ESA (HR 0.78, 95% CI 0.62-0.98). Specifically, in pooled ND-CKD trials, the risk of major adverse cardiovascular events (MACE) was higher than that of a placebo (HR 1.26, 95% CI 1.02-1.55). In comparison to Epoetin alfa, Roxadustat significantly reduced the risk of MACE and MACE+ in incident dialysis patients (MACE HR, 0.70 [95% CI, 0.51-0.97] and MACE+ HR, 0.66 [95% CI, 0.50-0.89]), suggesting an improvement in cardiovascular safety over the current standard of care. A pooled analysis of the ANDES, OLYMPUS, and ALPS trials comparing Roxadustat to placebo in patients with non-alcoholic CKD showed that Roxadustat was less effective for major adverse cardiovascular events (MACE; composite of mortality, non-fatal MI, and/or stroke) [HR 1.10 (95% CI 0.96-1.27)]. [HR 1.07 (95% CI 0.96-1.21)] and expanded MACE (hospitalization for either a heart attack or HF plus unstable angina or MACE plus hospitalization for either HF or angina). A pooled analysis of four Roxudustat ESA-comparator clinical trials (HIMALAYAS, ROCKIES, SIERRAS, and PYRENEES) in the dialysis population revealed no differences in the risk of heart failure, MI, unstable angina, and stroke.
In the PRO2TECT trial, the US population exhibited no cardiovascular risk, while the non-US population had a higher risk in the Vadadustat arm. Non-erythropoietic effects that could influence cardiovascular outcomes have been consistently found in clinical studies involving Roxadustat and Daprodustat. Triglycerides, total serum cholesterol, and low-density and high-density lipoprotein cholesterol are all decreased as a result of these activities. HIF-PHIs do not appear to alter echocardiographic parameters or lengthen the QT interval, even at supratherapeutic doses.
Renal safety
According to preliminary results from the erythropoietin (MIYABI) haemodialysis-correction (HD-C) and haemodialysis-maintenance (HD-M) trials (n=325), worsening of CKD occurred more frequently with Molidustat (13.4% and 12.2% respectively) than with Darbepoetin alfa (6.3% and 7.3% respectively) in NDD-CKD patients with anemia who had either not received treatment or had received ESA safety. Roxadustat therapy was shown to reduce kidney scarring by improving vascular regeneration following unilateral ischaemia-perfusion; this effect is most likely mediated by the VEGF A/VEGF (vascular endothelial growth factor) receptor 1 signaling pathway. However, a preliminary pooled safety study of patients with NDD-CKD treated with Roxadustat showed that the medication improved glomerular filtration rate (1-year drop in estimated glomerular filtration rate of -2.8 vs. -4.4 ml/min and placebo). According to a pooled analysis of three RCTs, the mean eGFR was 20±12 mL/min, and patients with stage ? CKD were more likely to experience renal failure in the Roxadustat group than in the placebo group. Hyperkalemia was more prevalent in patients with both NDD CKD and DD CKD in Chinese phase 3 trials; 12% of patients with NDD CKD treated with Roxadustat had metabolic acidosis; and a phase 2 trial found hyperkalemia in patients treated with other HIF-PHI
Malignancy
HIF-Phis and ESAs were found to have similar cancer risks in a recent meta-analysis of patients with NDD and DD-CKD. A post hoc analysis of three phase 3 Japanese studies in patients with NDD-CKD and DD-CKD revealed similar cancer-related side events in the Daprodustat and ESA groups (1.28 vs. 1.53 per 100 patient-years, respectively). Hypoxia, a common feature of the cancer microenvironment, is caused by uncontrolled and disordered cellular proliferation in the absence of adequate vascular supply. Moreover, hypoxia increases the expression of HIF-1α and HIF-2α inside tumor masses and reduces tumoral immunogenicity because it dysregulates cell metabolism and duplication. In the ASCEND-ND trial, Daprodustat was associated with a higher incidence of cancer-related outcomes (death or tumor progression or recurrence) compared to ESAs [3.7% vs. 2.5%; RR1.47 (95% CI 1.03-2.10)]. Roxadustat did not increase the risk of malignancy in patients with NDD-CKD, according to a pooled analysis of studies comparing it to a placebo. Belzutifan has FDA approval to treat renal cell carcinoma and other tumors in patients with von Hippel-Lindau syndrome by selectively blocking HIF-2α from dimerizing with HIF-1β. Anemia correction may be beneficial within the cancer microenvironment because it can reduce the effects of ischaemia, restore cell metabolism, and improve responsiveness to radiation therapy and chemotherapy, the latter of which is probably mediated by the restoration of appropriate vascularization of the tumor mass. Regarding this, it has been shown that in mice with Lewis lung cancer, four HIF-Phis—Roxadusat, Daprodustat, Molidustat, and Vadadustat—normalize tumor blood vessels and reduce hypoxic areas.
Other safety consideration
When compared to a placebo, roxadustat was associated with an increased risk of pulmonary embolism, deep vein thrombosis, and arteriovenous access thrombosis, according to a pooled analysis of trials conducted in patients with NDD-CKD. AV dialysis access thrombosis was more common in dialysis patients treated with HIF-Phis than in those treated with ESAs, according to a phase 3 trial. Hypertension: HIF-Phis was less likely than ESAs to induce hypertension in one meta-analysis of NDD-CKD patients [RR 0.89 (95% CI 0.81-0.98)], whereas another analysis of NDD-CKD trials revealed that the incidence of hypertension was higher in the Roxadustat group than in the placebo group [RR 1.37 (95% CI 1.13-1.65)].In the comparative analysis of DD-CKD patients, there was no discernible difference in the development of hypertension between the HIF-Phis and ESA groups. Retinopathy: Enarodustat caused more retinal adverse events and higher VEGF levels than ESAs (3.7% vs. 0.9%), according to the SYMPHONY-ND study. Despite having lower VEGF levels than the Darbepoetin group, Vadadustat was found to increase the risk of adverse events in the SYMPHONY-HD trial. Because roxadustat selectively binds to the thyroid hormone receptor-β (THRβ), it has also been known to cause reversible central hypothyroidism. By stopping the cell cycle's progression and preventing cell death, HIF-1α may act as a protective agent by directly triggering the transcription of THRβ.
FUTURE PERSPECTIVE
It is widely acknowledged that HIF-PHI are effective drugs for treating anemia in patients with chronic kidney disease. They function completely differently from the current ESAs and provide a viable alternative to current therapies. Since these medications are approved for use in clinical settings, the vast amounts of data produced by HIF-Phis's phase 3 programs—one of the biggest global research initiatives ever conducted in CKD—need to be carefully analyzed and monitored. Despite the availability of several large phase 3 trials, they evaluate adverse events over a relatively shorter period of time. It is surprising that non-dialysis patients expressed the greatest concern regarding cardiovascular safety, considering that they typically have fewer comorbidities, less severe anemia, and require lower dosages of HIF-Phi or ESAs to treat them. Because non-dialysis patients had a much lower occurrence, the experiment's statistical power was lower, which leads one hypothesis to suggest a statistical fluctuation. It is impossible to rule out the possibility of a unique safety profile for ESAs, depending on dosage usage. Preliminary research suggests that HIF-Phi may improve iron mobilization and absorption in inflammatory patients; this should be validated in clinical practice. In practice, it can be difficult to treat anemia in patients who are not responding well. Further research is necessary to determine whether this effect is specific to Roxadustat or a class effect. Based on the information that is currently available, that is one of the unique characteristics of the medication. The way that HIF-Phi medication reduces HDL and LDL cholesterol is another significant clinical event that requires explanation. Based on this consideration, a more comprehensive analysis should be carried out by looking at each patient who is also taking cholesterol-lowering drugs separately. The enrolled patients' CKD stages are too advanced for studies to be conducted, and their follow-up time is extremely brief. Future studies should investigate HIF-PHI's ancillary effects, which include angiogenesis, mitochondrial function, immunity, cell growth and survival, vasodilation, and cell migration, in order to validate its safety concerns and advantageous ancillary effects. Results are inconclusive when comparing CKD progression data to placebos or ESAs. The patient's preferences (orally administered), current medication load, and possible ESRD treatment (home dialysis, hemodialysis, and peritoneal dialysis) all influence how HIF-PHI works in clinical practice.
REFERENCES



Sona Toji*, Anu Benedict, Ashna Saju, Maria George, Lincy George, HIF-PHI for Management of Anaemia of Chronic Kidney Disease: An Overview, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 5, 3588-3597. https://doi.org/10.5281/zenodo.15479991
 10.5281/zenodo.15479991
10.5281/zenodo.15479991
