Shri Sambhaji College of pharmacy khadkut Nanded, Swami Ramanand Tirth Marathwada University
In order to improve the absorption of insulin through biological barriers, Labra sol ALF and Labra fil M 2125 CS were chosen as permeation-enhancing excipients. The development of oral insulin drug delivery systems remains a challenge for pharmaceutical technology researchers, as the formulation process must overcome a number of obstacles due to the adverse characteristics of peptides. The goal of this study was to formulate different sodium-alginate microparticles as a potential method for oral insulin administration. In our previous studies, the method has been successfully optimized using a small model peptide. To improve oral bioavailability, they were applied at a concentration of 0.10% (v/v %), along with different combinations of the two. Encapsulation efficiency demonstrated adequate drug incorporation, as it produced over 80% in each composition. The results of the enzymatic stability and in vitro dissolution tests demonstrated that, as a pH-responsive polymer, alginate bead swelling and drug release occur at higher pH, protecting insulin against the harsh environment of the gastrointestinal tract. After 120 minutes, SIF degradation caused 66% of the remaining insulin content. Permeability experiments demonstrated the effects of permeation enhancers and natural polymers on drug absorption, as they significantly improved drug transport through Caco-2 cells in the case of alginate microparticle formulations, compared to the placebo insulin solution. These results imply that these formulations are able to increase the oral bioavailability of insulin.Keywords: microbead; oral bioavailability; absorption enhancement; Labra sol ALF; Labra fil M 2125 CS; Caco-2 cells. An efficient oral insulin product is even more important for the management of patients with diabetes because of the increasing evidence that earlier initiation of intensive insulin therapy produces sustained tight glycaemic control, which results in a significant delay in complications. Oral insulin is one of the most exciting areas of development in the treatment of diabetes because of its potential benefits for patient convenience, rapid insulinization of the liver, and adequate insulin delivery avoiding peripheral hyper insulinaemia while potentially avoiding adverse effects of weight gain and hypoglycaemia. The development status of oral insulins that are publicly reported to be undergoing clinical studies is summarized in this review. Two oral insulin products are currently in an advanced stage of clinical development, and the first data from long-term therapy are anticipated to be available in the second half of 2010. Despite awareness of this unmet medical need, oral delivery of insulin has failed due to a number of obstacles. Researchers have attempted to develop oral insulin using various technologies for several decades with little clinical or commercial experience
Some milestones in the history of insulin therapy include the following: In 1921, young physician Frederick Banting (1881-1941) and fourth-year medical student Charles Best (1899-1978), who worked in the lab of Professor McLeod at Toronto University, discovered the last piece in a series of studies that had been started in 1916 by other researchers who hypothesized that the pancreas secreted a substance already named "insulin" that could lower blood glucose levels. The young researchers isolated this extract from the pancreas that "cured" hyperglycemia in diabetic dogs1-2, and in 1922 they successfully gave it to a 14-year- old diabetic patient, Leonard Thompson. [5] In 1923, the company Lilly started selling animal insulin. The hormone was discovered to be a protein in 1928, and since Banting and Best's insulin could not act for more than six hours, a lot of research was done to find ways to prolong its action. In 1936, Hagedorn observed that adding a basic protein, like protamine, to the insulin preparation kept the hormone suspended at the injection site, delaying absorption and prolonging its action. [6] The first insulin, known as "Isophane NPH" (Neutral Protamine Hagedorn), was marketed in 1946. In 1952, the first Lente insulin was produced in Denmark that was retarded with zinc and without protamine. [6] The precise formula for bovine insulin was determined by Sanger in 1955. A radio immunoassay for insulin was developed in the 1960s. Production of mono-component insulins, obtained by ion exchange chromatography, and mono-peak ones, separated by Sephadex G50 column, started in the 1970s. High performance chromatography allowed for the isolation of an insulin that was 99% pure from proinsulin and other islet hormones 2009.
Human Insulin
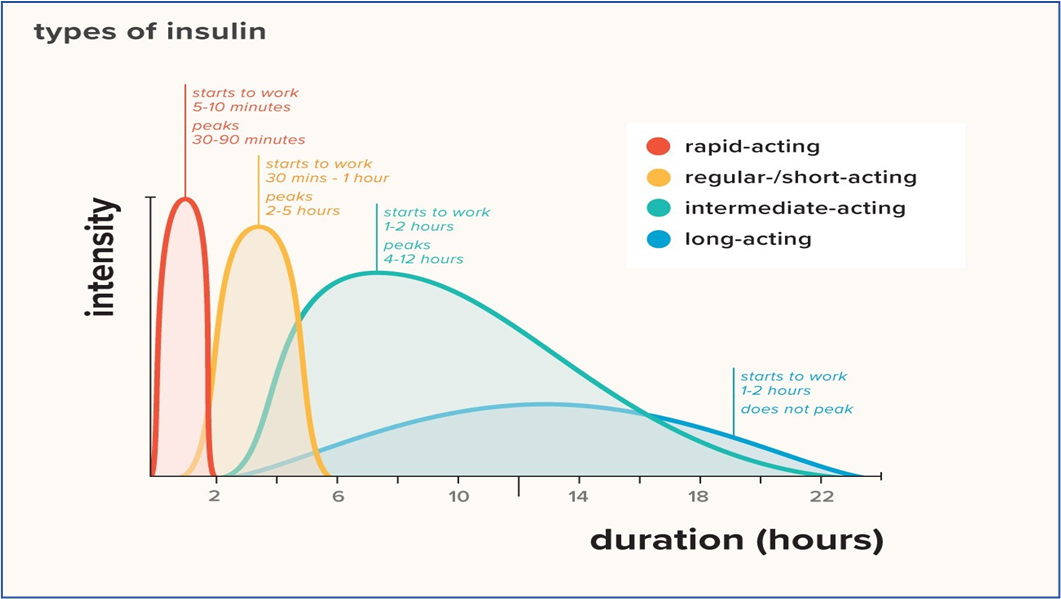
Complete synthesis of the human insulin molecule was accomplished in 1966 10. Human insulin is a globular protein with a molecular weight of approximately 5,800 kd, composed of 51 amino acid residues arranged in two polypeptide chains (A and B), connected by two disulfide bonds. Chain A comprises 21 residues with an additional disulfide bond between A6 and A11, while chain B comprises 30 amino acids. [8] Insulin only exists as a monomer at low concentrations; at higher concentrations, it exhibits a tendency to aggregate into stable dimers in aqueous solution at pH 2–8, and in the presence of zinc ions, it forms hexamers, which are nearly spherical in shape, with a diameter of 5 nm and a height of 3.5 nm. The hormone's polymerization has significant pharmacological ramifications. Prior to the 1980s, the pancreas of cows or pigs was used to extract insulin. Human insulin was first produced commercially in 1982.The scientific significance of this turning point in the history of diabetes is comparable to that of the discovery of insulin. The methods for synthesizing insulin were developed after it became evident that cadavers could not provide enough human insulin to meet global needs. Using an enzymatic process, trypsin catalyzes the substitution of threonine for alanine in position B30 of pig insulin to produce semisynthetic insulin. The resulting insulin was entirely devoid of other pancreatic and gastrointestinal hormones and shared the same amino acid sequence as the human insulin. Through the use of recombinant DNA, genetic engineering has made it possible to synthesize human insulin on an industrial scale. [7] DNA fragments encoding chains A and B are inserted separately into plasmids, and the resulting insulin chains are harvested (along with other bacterial proteins) and reassembled with the proper disulfide bonds. [9] To prevent contamination, plasmids containing genetic material coding for the proinsulin molecule were created, which is isolated from the culture medium and stripped of its connecting peptide. [10] Another method for producing biosynthetic insulin uses the yeast Saccharomyces cerevisiae as a living laboratory, inserting purified DNA that directs the synthesis of a single chain precursor that differs from proinsulin in one of the yeast's plasmids. The protein, which is continuously produced by the yeast during fermentation, is extracted from the culture medium, separated by centrifugation and crystallization, transformed into insulin ester by trypsin transpeptidation, and then hydrolyzed. This process ensures high purity. [7] [11] The three types of human insulins that are currently available on the market are: rapid-acting (Regular), intermediate-acting (NPH and Lente), and long-acting (Ultralente). The former is a clear, colorless, aqueous solution buffered at neutral pH (7–7.8). The main quaternary structure of pharmacological insulin is hexamers, which are made stable by zinc ions; other structures include dimers and tetramers. [12] The molecule tends to aggregate in the vial and in the tissue where it is injected; the hexamers must be split in order for the insulin to be absorbed from the subcutaneous injection site. As a result, Regular insulin enters the general circulation after a lag phase approximately 30 minutes after injection, reaching the plasmatic peak at 2–4 hours, and lasting for 6 hours. Protamine, a protein that is extracted from the nucleus of fish sperm and used to stabilize DNA, delays the absorption of NPH. The commercial form of NPH is Isophane-NPH insulin, a white suspension of orthorhombic crystals that contain 0.9 molecules of protamine and two zinc atoms per hexamer 5. Protamine in the crystal controls interactions between dimers and hexamers. The vehicle is water buffered at pH 6.9- 7.5. NPH is longer-acting; in fact, its blood absorption begins 1.5 hours after subcutaneous injection; it reaches a peak plasma concentration at 4 to 12 hours and disappears within 24 hours. The "tail," however, is relatively ineffective. Although NPH has the most regular absorption of all intermediate- and long-acting insulins, inter- and intra-individual variability is high. Preservatives such as phenol or meta-cresol are added
21. Insulin crystals are insoluble in water and have a tendency to precipitate to the bottom of the vial, which must be tilted a few times to resuspend them before use. [13] When the molar ratio of zinc to insulin is greater than one, the zinc ion decreases the solubility of insulin in neutral solvent 6. When an acid solution of insulin is brought to pH 7.4 with an excess of zinc ions, the resulting precipitate is amorphous and has moderately delayed absorption after subcutaneous injection. This type of insulin formulation is called Semilente and was manufactured until a few years ago. If insulin is allowed to crystallize at pH 5.5 before zinc is added and pH adjusted, the resulting formulation, called Ultralente, is made up of crystals that are insoluble in water and are absorbed very slowly. In commercial preparations, methyl-Para hydroxybenzoate is used as a preservative, and the suspension is buffered at pH 7–7.821. It enters the circulation 2.5 hours after injection, reaches its peak plasma concentration at 7–15 hours, and goes away by 20 hours. Both NPH and Lente insulins can be mixed with Regular in the syringe; however, while Regular and NPH maintain their pharmaco-kinetic properties, the Lente/Regular mixture changes over time because the excess of zinc ions binds part of the rapid-acting insulin, changing its form into one that is similar to Semilente. Long-acting insulin (Ultralente) is a milky-looking aqueous suspension of zinc-insulin crystals at neutral pH, which acts after 4 hours, reaches a slight but undesirable peak plasma concentration at 7 hours, and maintains blood insulin levels for about 8 to 20 hours. It also sporadically mimics endogenous basal secretion, its absorption is wildly irregular, and it cannot be combined with regular insulin in the syringe because the latter's action would be too delayed. [2] Because of its potential to improve patient convenience, oral insulin is one of the most interesting areas of development in the treatment of diabetes. Fast hepatic insulinization and sufficient insulin administration prevent peripheral hyperinsulinemia and may also prevent weight-related side effects. Gain and hypoglycemia. Growing evidence that early commencement of intense insulin treatment causes prolonged tight glycemic control resulting.
LITERATURE REVIEW:
AIM AND OBJECTIVES
Aim: - To formulate dosage form of Insulin
Objectives: -
The objective of this review is to:
Plan of Work: -
Insulin Preparations:
Human insulin therapy began in 1921 when insulin was first given to a diabetic dog. [14] All insulin preparations are currently made using recombinant DNA technology, and the dosages and concentration levels of insulin preparations used in clinics are indicated in international units; in fact, one international unit of insulin is the bioequivalent of 34.7 μg of crystalline insulin. Insulin preparations are made up of the amino acid sequence of human insulin or variations of it (insulin analogues). Although Novo Nordisk uses Saccharomyces cerevisiae, or baker's yeast, to synthesize insulin, Eli Lilly and Sanofi use a non-pathogenic strain of Escherichia coli. [15] The pharmacokinetic properties of various insulin preparations are summarized in Table 1. Individuals and even repeated doses of the same person can vary greatly in the time of onset of action, peak effect, and duration of action of insulin, depending on the injection site, dose size, exercise, and the presence of circulating anti-insulin antibodies (Table 1).
When two zinc ions are present in the formulation, the insulin molecules typically exist as dimers that can join to form hexamers; the formed hexamers generally exhibit further stability in the presence of phenolic compounds such as phenol and meta-cresol.5 Regular human insulin and rapidly acting insulin analogues are usually clear solutions at neutral pH with minor amounts of zinc (for greater stability and shelf life). [16] Pharmacokinetic properties of various types of short-acting insulins are summarized in Table 1. The optimal time for pre-prandial administration of regular human insulin and rapid-acting insulin is 45 and 15, respectively, according to a number of clinical studies.
The main drawbacks of regular insulin are postprandial hypoglycemia and late postprandial hypoglycemia. Regular insulin's onset time, peak effect, and duration are dose dependent.8 Unlike other insulin analogues, regular insulin can be administered intravenously to treat diabetic ketoacidosis. Regular insulin is a zinc-insulin crystalline product with a strength of 100 or 500 USP insulin units/ml. The product's packets are color coded orange for the 100 unit/mL and brown for the 500 unit/mL with diagonal white strips to prevent accidental use of the inappropriate strength. Insulin vials should be stored in their cartons, away from direct light and heat, and regular insulin is absorbed more quickly when injected in the abdomen or deltoid than in other areas, such as the thighs and buttocks. [17]
Technosphere human insulin and three insulin analogues lispro, as-part, and glulisine are examples of rapid-acting insulins. Subcutaneous injection of these analogues results in their rapid dissociation into monomers and rapid absorption because of their low propensity for self-aggregation. These rapid-acting insulins reach peak serum values within one hour and have a shorter duration of action than regular human insulin. As a result, when used to treat glycemia after meals, the pharmacokinetic properties of various rapid-acting insulins are compiled in Table 1. [18]
Insulin lispro is an insulin analog in which the lysine is at position B29 and the proline is at position B28. It is administered as a continuous subcutaneous infusion using specific external controlled infusion devices or as a subcutaneous bolus by pen or conventional syringe.10 For better dosing accuracy in pediatric patients, it should be diluted to a ratio of 1:1 or 1:2 with the sterile vehicle provided by the manufacturer. [19]
A fixed dose combination of insulin as-part protamine and insulin as-part (70/30) is intended only for subcutaneous administration and should not be administered intravenously. Insulin as- part is a single substitution of proline by as-partic acid at position B28. Usually, it is administered concurrently with certain long-acting insulin (e.g., NPH) to meet basal insulin needs in diabetic patients. To suspend the mixture in a vial immediately before use, gently roll the vial between your palms ten times or so until the suspension looks evenly opaque and cloudy. Additionally, when combining insulin as-part with NPH, remove the insulin as-part first, then mix it with NPH and inject it right away. The compatibility data suggests that insulin as-part should not be combined with crystalline zinc insulin preparations, and that a fixed dose combination of insulin as-part should not mix with other analogues. [20]
Insulin glulisine differs from human insulin because the amino acid asparagine at location B3 is replaced by lysine, and the lysine at location B29 is replaced by glutamic acid. This biosynthetic product is designed for parenteral administration and has all the necessary properties. [21] When administered subcutaneously 15 minutes before meals at a dose rate of 0.5-1 unit/kg/day, it shows a faster onset and shorter duration of action.15 It can also be administered alone via intravenous route at a dose of 0.05-1 unit/mL in normal saline for glycemic control under medical supervision in a hospital setting. It is usually used in conjunction with long-acting basal insulin or occasionally as a continuous administration by subcutaneous injection pump. Insulin glulisine formulation is stable in infusion sets up to 48 hours. [22]
A very small whistle-like device, Technosphere insulin is a dry-powder formulation of recombinant human regular insulin that can be inhaled and absorbed through pulmonary tissue. It is a rapid-acting powder insulin that is inhaled at mealtimes to improve blood glucose control in the type 1 and type 2 diabetic population. Patients should not use Technosphere as a substitute for long- acting insulin and in diabetic ketoacidosis; instead, it must be used in conjunction with long-acting insulin in type 1 diabetes. [23]
Insulin Preparation NPH is an equivalent mixture of protamine and native insulin in water for injection that has been adjusted to pH 7.1-7.4 with phosphate buffer. [24] It is an opaque suspension of rod-shaped insulin crystals with a particle size of less than 30μm. The preparation should be free of large aggregates after moderate shaking for consistent absorption. The formulation should not be used for more than 24 to 36 months after the date of manufacturing. NPH is packaged in 10 mL multiple dose containers or vials with a strength of in general, the absorption of NPH insulin is quick from abdominal fat, relatively slow from posterior upper arms and lateral thigh area, and slowest from superior buttocks area. [25] Patients should be careful for initial signs of frosting or clumping of this insulin, as it shows a noticeable loss of potency. This form of insulin must not be administered through intravenous route. Since the active ingredient is in the precipitate, the vial should be gently agitated to assure a uniform mixture for accurate measurement of each dose. The pharmacokinetic properties of long-acting insulins are summarized in Table 1
The threonine at position B30 has been detached in this insulin analogue, and myristic acid (a 14-C fatty acid chain) has been attached to the lysine at position 29. [26] Insulin detemir is administered subcutaneously once or twice daily using a conventional insulin syringe or injection pen. The properties of protein binding and self-association are responsible for the long duration and slow absorption. The basal insulin's onset of action is between 3 and 4 hours, with a peak observed between 6 and 8 hours. [27] The duration of action of insulin detemir is dose dependent; at low doses (0.1-0.2 unit/kg), the duration ranges between 5 and 12 hours; at moderate doses (0.6 unit/kg), it is approximately 20 hours; and at high doses (>0.6 unit/kg), it is between 22 and 24 hours.
Insulin glargine differs from regular insulin because it contains two arginine residues at the carboxyl terminal of the B chain and glycine at amino acid 21 of the insulin A chain, which neutralizes the asparagine when it is injected into subcutaneous tissue, forming micro-precipitates at the injection site. Generally, this insulin analogue is not mixed with other insulins, and it is preferable to use an additional syringe to prevent the possibility of contamination, which could result in a loss of efficacy. Because it only contributes to basal secretion, it is frequently used in conjunction with other insulins or occasionally with oral antidiabetic medications. The US Food and Drug Administration (FDA) has approved a higher strength preparation (300 units/mL). [28]
The product is a combination of insulin degludec and insulin as-part (70/30) for subcutaneous injection; another insulin degludec product is a fixed ratio combination of insulin degludec and glucagon-like peptide 1 agonist, liraglutide; it is available as degludec-100 unit/mL in combination with 3.6 mg/mL of liraglutide solution for injection. It is an ultra-long-acting (42 h) insulin analogue, with B-30 threonine deleted and B-29 conjugated to hexa-decanedioic acid. The prolonged duration of action is caused by the multihexamers depot formed at the injection site and the slow release of monomers. [29]
Table 1: Pharmaceutical properties of insulin preparations
|
Insulin preparations |
Onset of action (h) |
Peak effect (h) |
Duration of action (h) |
|
Short – acting (clear) |
|||
|
Regular insulin |
0.5-1 |
1-3 |
6-10 |
|
Insulin lispro |
0.25-0.5 |
0.5-1.0 |
3-5 |
|
Insulin as-part |
0.17-0.33 |
0.5-1.0 |
4-5.3 |
|
Insulin glulisine |
0.25-0.41 |
0.5-1.0 |
4-6.3 |
|
Technosphere insulin |
<0.25 |
0.5-1.5 |
2-3 |
|
Long acting (clear) |
|||
|
NPH |
1-2 |
6-14 |
16-24 |
|
Insulin detemir |
3-4 |
6-8 |
6-24 |
|
Insulin glargine |
1-2 |
Flat |
24 |
|
Insulin degludec |
1-2 |
Flat |
42 |
|
Mixture (cloudy) |
|||
|
Isophane / Regular insulin 70/30,50/50 |
0.5-1 |
2-12 |
18-24 |
|
NPL / Lispro mix 75/50 |
5 min |
7-12 |
1-24 |
NPH: neutral protamine Hagedorn, NPL protamine lispro [4]
Summarizes the pharmacokinetic characteristics of different insulin mixtures.
The mixture exhibits a rapid onset and an intermediate duration of action (~1 day). Patients with diabetes who have trouble mixing insulins can access stable premixed insulins (70% NPH and 30% regular), and they are advised not to change this combination ratio by mixing NPH or regular insulin in addition. The fixed combinations are typically administered twice a day, with the morning and evening meal Premixed combinations of neutral protamine lispro (NPL) and insulin lispro (75/25 and 50/50) have a prompter onset of glucose-lowering effect than 70% NPH/30% regular human insulin mixture. The fixed combination exhibits two phases of absorption: the first phase represents insulin lispro and its rapid onset of action. [30]
A conventional technique for subcutaneous insulin injection. Compared to other techniques, syringes are less costly and need less training, but they are less discrete.
A pen-like instrument for subcutaneous insulin injection. Compared to needles, insulin pens are more comfortable and handier, but they cost more and might not be reimbursed by insurance.
An apparatus that uses a tiny tube inserted beneath the skin to inject insulin. Insulin pumps can provide bolus insulin and lower A1C, however they can also lead to infection and weight gain.
An apparatus that delivers a thin stream of insulin into the skin. Although they can cause skin harm and are somewhat costly, jet injectors are an alternative for individuals who are unable to use syringes or who are afraid of needles.
A gadget that fits in your mouth is used to inhale rapid-acting insulin. People who smoke or have lung issues should not use inhaled insulin, which is administered at the beginning of each meal. You can learn how to use insulin pumps, how to securely store insulin, and when, when, and how to inject insulin from a doctor or diabetic nurse educator.
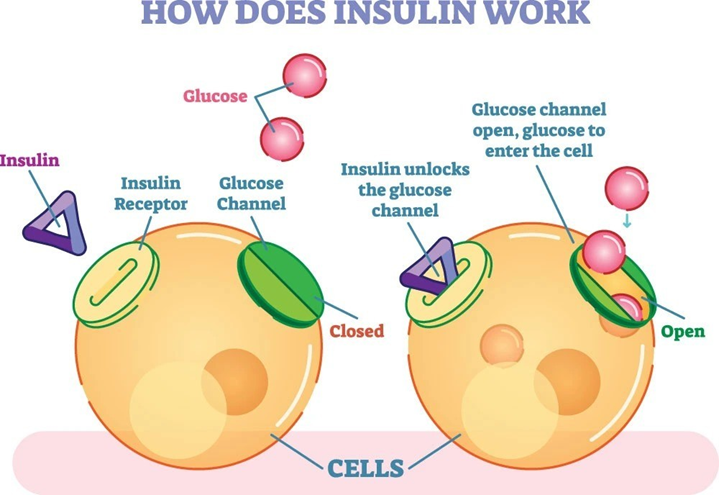
Insulin is a hormone secreted from the pancreas which works as a key which helps by unlocking the utilization of glucose (sugars) from blood. When a diabetes patient follows a strict diet, it decreases the glucose production in blood so the lesser challenge is given. When a diabetic patient exercises daily it helps in more affective utilization of sugars and ultimately better diabetes control When despite these efforts sugar rises then doctors help through medication to increase secretion of insulin or give direct insulin injections to control the abnormal rise of sugars in blood.

Types of Insulin Device
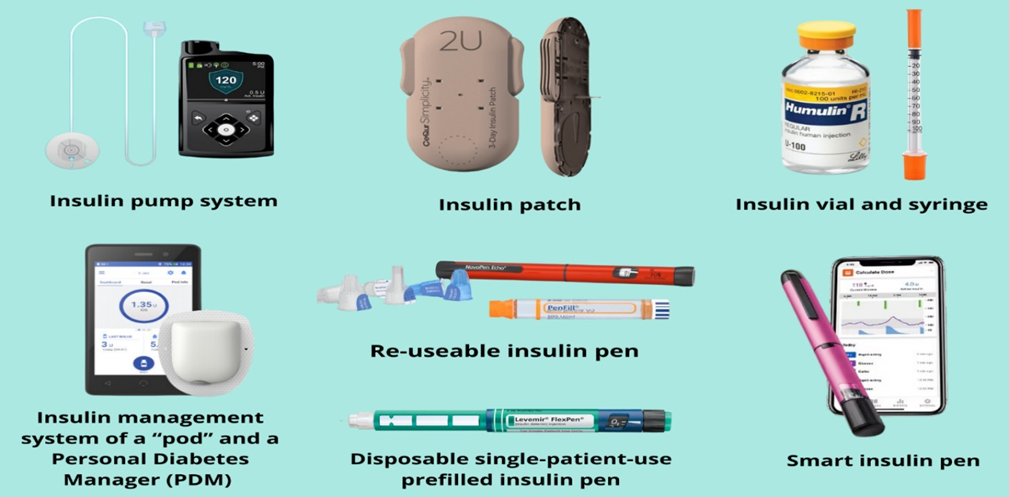
Insulin pumps deliver insulin continuously through a catheter, which is a small plastic tube that ends in a needle. The needle is inserted under the skin, and the tube leaves a flexible cannula behind. The cannula needs to be changed every few days.
A smart insulin patch, also known as a glucose-responsive insulin patch, is a type of wearable medical device for diabetes treatment. It is a transdermal patch comprising glucose-sensitive microneedle-array loaded with insulin for blood glucose regulation. Once applied on the skin, the microneedles penetrate under the skin and can sense blood sugar levels. If glucose levels go up, it can promote the release of insulin, which is transported through the regional lymph and capillary vessels for glucose regulation.
Unlike insulin pens or insulin pumps, insulin syringes require drawing insulin from a separate insulin vial before an injection can be given. Although some people with diabetes find this inconvenient, the advantages of insulin syringes are that they are cost effective and widely available.
Reusable insulin pens are a type of insulin delivery device that can be used for several years with the replacement of cartridges and needles. sustainable option than disposable pens, as they can: Reduce plastic waste by 80–90% Reduce carbon footprint by 40% Take up less space in the fridge Be cost-neutral or cheaper than disposable pens They are used only with rapid-acting insulin preparations.
Disposable insulin pens are prefilled with insulin and thrown away after the insulin cartridge is empty or the pen has been used for 28–32 days. The exact length of time depends on the type of insulin used.
Smart insulin pens are reusable or attachable devices that can help people with diabetes manage their insulin by automatically recording and sharing information about their insulin injections.
An insulin management system with a pad and a personal diabetes manager (PDM) typically includes the following features:
Pod: A tubeless, wearable pump that holds and delivers insulin. The pod is usually waterproof and can be worn under clothing.
PDM: A handheld device that controls the pod. The PDM allows the user to program the pod, check its status, and adjust insulin delivery.
CONCLUSION:
Due to the rise in obesity rates and the prevalence of sedentary lifestyles, there is a great need for anti- diabetic medications, which has caused companies to invest more in research and development to produce targeted formulations. Nanotechnology has the potential to revolutionize therapeutic approaches in our everyday lives Significant progress has been made in nanoparticulate drug delivery systems for anti-diabetic medications as a result of extensive research into nano-formulations; however, to improve their efficacy and safety, it is necessary to address ethical concerns and ensure long-term safety, as well as to comply with the most recent FDA regulations. Active targeting strategies, such as functionalizing appropriate ligands or using combinational drug therapy involving multiple anti-diabetic drugs, present promising avenues for regulating glucose levels over prolonged periods of time. These ongoing technological advancements in nanotechnology offer compelling prospects for the development of effective glucose-lowering therapeutic modalities in the near future.
REFERENCES






Shaikh Shirin Fatema Maulana*, Waghmare Vyanktesh, Wangawar Pallavi, Shinde Devanand, Suryawanshi Yogita, Swami Bhujayya, Formulation of Different Dosage Forms of Insulin. Sci., 2025, Vol 3, Issue 4, 152-165. https://doi.org/10.5281/zenodo.15120628
 10.5281/zenodo.15120628
10.5281/zenodo.15120628
