Sitabai Thite College of Pharmacy, Shirur
This research study presents the formulation, development, and comprehensive evaluation of a novel sustained-release polyherbal transdermal patch for gout therapy. A polyherbal extract blend of Haritaki, Punarnava, Guduchi, Nirgundi, and Cocoa was optimized and formulated into a transdermal patch designed to provide targeted and sustained delivery of the polyherbal extract blend, leveraging the synergistic anti-inflammatory properties of the herbs. The polyherbal extract blend was evaluated for its in vitro anti-inflammatory activity and in vitro dissolution study of Monosodium urate (MSU) crystal, demonstrating significant potential for gout therapy. The patch exhibited controlled drug release, optimal physical and pharmaceutical properties, and significant anti-inflammatory activity in vitro. In vitro drug permeability and ex vivo permeation studies revealed a steady and sustained release of the polyherbal extract blend, indicating potential for improved therapeutic efficacy and reduced side effects. This study provides a comprehensive understanding of the formulation, development, and evaluation of a novel sustained-release polyherbal transdermal patch for gout therapy. This innovative patch offers a promising, targeted, and sustained treatment approach for gout management, providing a potential alternative to conventional therapies. The findings of this research have significant implications for the development of herbal-based transdermal patches for various inflammatory diseases.
When urate crystals accumulate in the joints or soft tissues, a severe condition called gout results. A higher-than-normal blood uric acid content is necessary for the formation of uric acid crystals. Gout is an inflammatory disease that can sometimes be lethal and has negative effects on the body. A lower quality of life is associated with gout, the most prevalent type of inflammatory arthritis [1–3]. Elevated serum uric acid (SUA) levels, or hyperuricaemia, are a prerequisite for the development of gout. As SUA levels increase and physiological saturation thresholds for uric acid are exceeded in body fluids, monosodium urate (MSU) crystals form and accumulate in and around joints. Clinical manifestations of MSU crystal deposition include tophaceous deposits of MSU crystals in the skin and joints, chronic joint damage, and acute flare-ups of severe pain and inflammation affecting peripheral joints, most often the first metatarsophalangeal (MTP) joint. Thanks to current epidemiological studies, we now have a better understanding of the risk factors for the development of gout, the impact of co-morbid illness on mortality and cardiovascular morbidity, and trends in the incidence and frequency of gout [4]. Acute gout, also called podagra when it affects the first metatarsophalangeal joint, is caused by the inflammatory reaction of the joint tissues that results from the development of monosodium urate (MSU) crystals within the joint. The link between crystal deposition and joint inflammation was established by Garrod, who developed the thread-test assay of serum urate, who said that "the deposited urate of soda may be looked upon as the cause, and not the effect, of the gouty inflammation." Early clinical descriptions of acute gout, from Hippocrates to Charcot, highlighted how quickly and inflammatorily an episode might occur.[5] Attacks of gout are typified by sudden, intense symptoms that nearly always happen at night. The first MT joint of the big toe is often affected by the patient's sudden onset of discomfort, which rapidly becomes red and swollen. Veins on the leg may enlarge, turning purple, and sometimes bruising.[6] The biochemical hallmark of gout is extracellular fluid urate saturation, which is characterised by hyperuricemia in the blood with plasma or serum urate concentrations exceeding 6.8 mg/dL (about 400 µmol/L), the approximate limit of urate solubility.[7] Acute gout flares, which are recurring flare-ups of inflammatory arthritis, chronic gouty arthropathy, and accumulation of urate crystals in the form of tophaceous deposits are some of the clinical signs of gout. Chronic nephropathy and uric acid nephrolithiasis
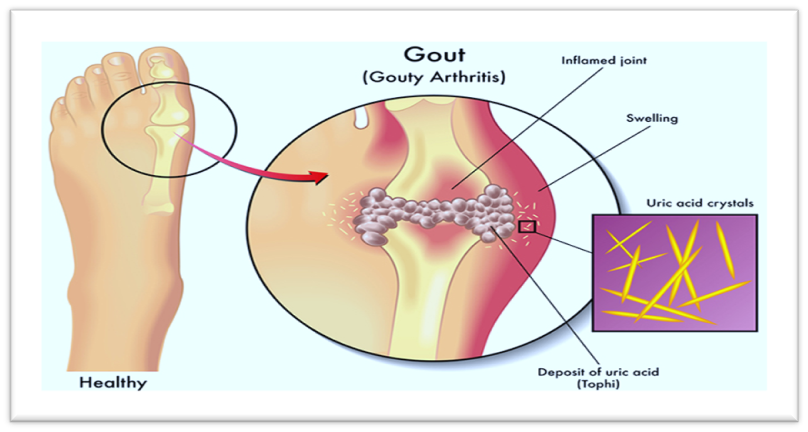
Figure 1. Gout (Gouty Arthritis)
Types of gouty arthritis: [8]
1. Acute Gouty Arthritis
2. Chronic Gouty Arthritis
Pathogenesis of acute gouty arthritis:
The buildup of uric acid crystals in the joints is the primary cause of gout. Consequently, uric acid buildup triggers the release of inflammatory mediators such as cytokines. This interface causes phagocytes to produce excessive amounts of IL-8, which in turn causes neutrophils to form. The initial development of mast cells and monocytes, followed by neutrophils, is also necessary for the pathologic phase of urarthritis. The UA crystals are flooded by macrophages before to the main gouty arthritis attack. Prominent macrophages possess the ability to retain these crystals without triggering an inflammatory reaction. In contrast, less-differentiated monocytes are produced in response to tumour necrosis factor levels, in addition to epithelial activation after the body's salt crystal process. Due to neutrophil chemotaxis and other inflammatory mediators, the affected areas experience vasodilatations, a rise in endothelial gaps, and an accumulation of macrophages and lymphocytes, all of which contribute to inflammation.
Chronic gouty arthritis's pathogenesis:
It can be described as an inflammatory disease. It may result in recurrent bouts of arthritis because of persistent inflammation. The formation of uric acid, cartilage degradation, gristle damage, and persistent inflammation are all signs of chronic inflammatory illness. The presence of salt crystals in animal tissue causes cartilage cells to expand, releasing gas, cytokines, and matrix metalloproteases, ultimately leading to cartilage damage.
The Disease Stages of Gout:
Understanding its four components and symptoms is crucial. The next reports could be helpful.
Stage 1. Asymptomatic Gout
The buildup of uric acid in the blood is the first step in the distinctive formation of uric acid crystals in the joint. The body breaks down purines to produce uric acid, a natural waste product. Purine is a substance that is found naturally in human tissue and in high concentrations in a variety of foods and beverages, such as alcohol, shellfish, and some meats, such as organ meats, bacon, turkey, and venison. Uric acid typically dissolves in the blood, passes through the kidneys for filtering, and is eliminated through urine. However, uric acid can accumulate in the blood to high levels, a condition known as hyperuricemia, if the body creates too much of it or the kidneys are ineffective at removing it. Some people have hyperuricemia with no symptoms at all. For some, it's the initial phase of gout. In this phase, the serum urate levels were deemed to be greater than 6.8 mg/dl.
Stage 2. Acute Gout
Excessive blood uric acid levels can cause severe discomfort and swelling by leaking out and crystallising in the areas surrounding the joints. The phrase "attack" refers to the abrupt and unexpected onset of pain, which can last anywhere from a few days to a few weeks.
It's likely that you may discover or suspect that you have gout for the first time during your first attack. By taking a sample of fluid from the afflicted joints and looking for uric acid crystals, your doctor can diagnose the condition. [9] The only method to determine if you have gout or another type of arthritis that would need a totally different course of treatment is to look for crystals. One of these is calcium pyrophosphate deposition disease (CPPD), which is sometimes referred to as "pseudogout" due to its gout-like characteristics. Similar to gout, crystals that accumulate in the joints cause pseudogout to flare up unexpectedly and violently. The crystals are made of calcium pyrophosphate dihydrate, which is the difference. The cause of these crystals forming in the joint is unknown. The goals of treatment for acute gout include reducing the pain and inflammation associated with attacks and controlling uric acid levels to minimise or stop future flare-ups. This frequently entails taking drugs that either raise the excretion of uric acid or decrease its formation,in addition to a diet low in purines. Mono Sodium Urate (MSU) precipitates out of the serum at higher serum uric acid levels and is deposited as crystals in the tendons or joints, producing irritation in the surrounding area.
Stage 3. Intercritical or Interval Gout
You will most likely go months or perhaps years without experiencing any symptoms after your initial gout episode or attacks. "Intercritical" or "interval" gout is the stage in which attacks occur at short or lengthy intervals. At this point, uric acid can still accumulate in the blood and joints even when attacks are not happening, so your doctor can still recommend uric acid-lowering drugs to lessen the likelihood or intensity of subsequent attacks. Losing weight aids in the management of gout if you are overweight. Drinking lots of water and eating a diet low in purines are also crucial during this phase. [10]
Stage 4. Chronic Tophaceous Gout
Chronic tophaceous gout, the last and most troublesome stage of gout, may develop if uric acid levels are not well managed during the interval stage. Tophi, which are buildups of urate crystals that might manifest as lumps or lumps beneath the skin, are a hallmark of chronic gout. A tophus can develop beneath the skin, in the bones or cartilage, in the bursa that cushions and shields the joint, or in a joint itself. Tophi that develop in the finger's tiny joints can limit movement and result in physical changes. Under the skin, tophi can be unattractive, infectious, and occasionally painful. In the cartilage and bone, tophi can potentially cause joint injury and deformity. Kidney stones, joint discomfort, and soreness are other issues that may arise during this chronic period. The majority of gout sufferers never go through this fourth stage because of efficient therapies. Continued use of uric acid-lowering medications is required for those who do, and it can lessen the risk of problems and, in certain situations, totally eradicate visible tophi.[11]
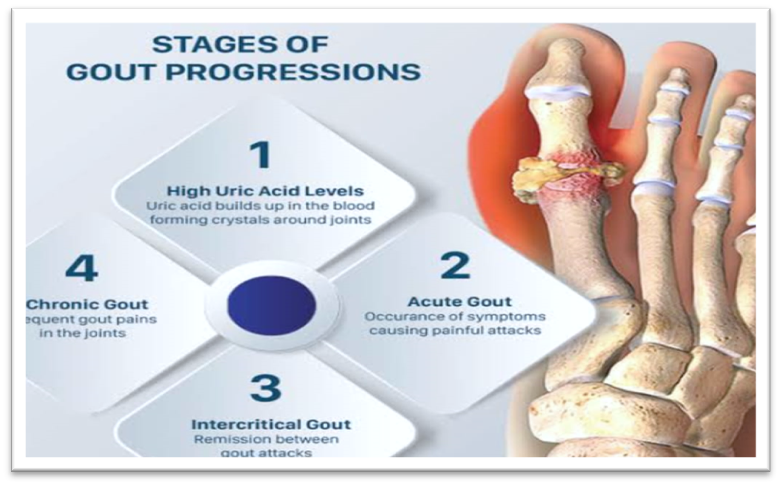
Figure 2. Stages of gout
Etiology
Gout often has a complex etiology that includes dietary variables, medical comorbidities, and genetic susceptibility. Rarely, gout which is typically linked to other health issues can be brought on by a single genetic flaw. The outcome is increased serum uric acid, which in some people might show up as clinical gout, regardless of the underlying cause. The root cause of gout is crystallisation of uric acid, which is frequently linked to elevated blood levels of the acid. Genetic predispositions and food may be the cause of this. under the excretion of urea, or uric acid salts. The main cause of hypeuracemia, or elevated blood uric acid levels in most cases, is under excretion of uric acid, whereas overproduction of uric acid is the secondary cause. The following describes important factors [12].
Lifestyle:
Consuming alcohol, fructose-sweetened beverages, meat, and seafood are dietary factors linked to gout. Additional triggers include surgery and physical trauma. Coffee, vitamin C, dairy products, and physical activity seem to reduce the risk.
Genetic:
There is a genetic component to gout. There is evidence linking the genes ABCG21, SLC2A9, and SLC22A12 to gout. Hereditary hyperuricemia is caused by a mutation in SLC22A12 that results in loss of function. Gout exacerbates certain rare genetic conditions by decreasing urate absorption and increasing urate release.
Medical condition
Gout frequently coexists with metabolic syndrome, a confluence of excessive cholesterol levels, insulin resistance, hypertension, and obesity. Lead poisoning, renal failure, haemolytic anaemia, solid organ transplant, and polycythaemia are other conditions that are exacerbated by gout. Gout risk is increased by a body mass index more than 35. Gout risk factors include prolonged exposure to lead and alcohol contaminated with lead.
Diet
Consuming foods high in red meat and seafood as well as beverages sweetened with fructose, a fruit sugar, raises uric acid levels, which raises the risk of developing gout. Drinking alcohol, particularly beer, raises your risk of developing gout.
Weight
Your body creates more uric acid and your kidneys have a harder difficulty getting rid of it if you are overweight.
Family history of gout
You have a higher chance of getting gout if other family members have had it.
Age and sex
Because women typically have lower levels of uric acid, gout is more common in men. However, women's uric acid levels start to resemble men's after menopause. In contrast to women, who typically have gout symptoms after menopause, men are more prone to acquire gout sooner, typically between the ages of 30 and 50.[13]
Medication
Diuretics are linked to gout, and other drugs that raise the risk of gout include ACE inhibitors, niacin, aspirin, beta blockers, Ritonavir, Pyrazinamide, and angiotensin receptor blockers, including Lostarin. Combining any of these medications with hydrochlorothiazide further increases the risk of gout.[14]
Sign and Symptoms
The most typical sign of gout is recurring acute inflammatory arthritis, which is characterised by a red, hot, and swollen joint. This is usually the metatarsal-phalangeal joint at the bases of the affected big toe. Other joints, such as the finger, wrist, knee, and heel, may also be impacted. Usually, joint discomfort starts between two and four hours later and at night. The primary cause of this is a decrease in body temperature. In addition to joint discomfort, other symptoms include fever and exhaustion. [15-16]
Complications
Following complications of gout can exist:
Diagnosis
Risk Factors
The conversion of hypoxanthine to xanthine and subsequently uric acid by xanthine oxidase, followed by the transformation of allantoin by uricase, is the last stage of purine metabolism. The solubility of allantoin is significantly higher than that of uric acid. There are gene mutations in humans, other primates, giraffes, and Dalmatians that prevent them from producing uricase. The uricase gene was inactivated approximately 25 million years ago due to a genetic mutation. URAT1 activity, which is in charge of excreting uric acid, increased concurrently. The antioxidant idea emerged when humans and other primates lost the capacity to synthesise vitamin C around 20 million years ago, with uric acid taking the place of ascorbic acid as the primary antioxidant. The emergence of hyperuricemia in humans, which makes them the only known mammals to acquire spontaneous gout, is one distinctive feature of this evolutionary process. The primary cause of gout, a disorder in which uric acid crystals build up in joints and cause pain and inflammation, is hyperuricemia. Higher serum urate levels have been linked to an increased risk of gout development and more frequent flare-ups over time, according to research. Over 2000 older persons with gout participated in the trial, and those whose serum urate levels were higher than 9 mg/dL had a threefold higher chance of having a flare-up during the following 12 months than those whose levels were lower than 6 mg/dL.[20-21]
Triggers
A flare-up of gout can be caused by any disease that alters the concentration of extracellular urate. Stress (primarily from medical conditions like cardiovascular diseases, recent surgeries, trauma, dehydration, or starvation), dietary choices (like eating high-purine foods like organ meats or seafood, as well as alcoholic beverages like beer, wine, and spirits), and medications (like aspirin, diuretics, or even allopurinol) are some of the factors that contribute to these conditions.
Pathophysiology
MSU crystals, the byproduct of human purine metabolism, are deposited in bones, soft tissues, and joints, causing gout, an inflammatory arthritis. Acute gout flare (acute arthritis), chronic gouty arthritis (chronic arthritis), tophaceous gout (production of tophi), renal functional impairment, and urolithiasis are just a few of the various manifestations of this illness. [21]
Uric Acid Physiology
In humans and higher primate species, uric acid is the end result of purine metabolism because of a mutation that inhibits the gene that codes for the uricase enzyme. It was once thought that uric acid was an essential natural antioxidant in the human body that was mostly in charge of removing reactive oxygen species. The regulation of oxidative stress is not significantly influenced by uric acid. Rather, it is believed to play a role in immunological surveillance as well as blood pressure and intravascular volume regulation. At pH 7.4, uric acid, a weak organic acid, is mostly found in its ionised form, MSU. Because of the high salt content, this form is less soluble. The non-ionized form of uric acid, which is even less soluble within the physiological range, is found in acidic environments such as urine. In contrast to MSU linked to gout, uric acid crystals and stones may develop in the urinary tract as a result. The liver produces the majority of the body's urate endogenously, with the small intestines contributing only a modest amount. Since the glomerulus filters almost all urate, renal excretion plays a crucial role in controlling the body's urate pool in steady-state settings. The urate pool enlarges when hyperuricemic. The typical range for urate levels in men is 800–1000 mg, whereas in women it is 500–1000 mg. The daily ureate turnover is between 500 and 1000 mg. Serum urate concentrations in males rise to the adult range during puberty, while in females of reproductive age, urate levels stay low. The reason for this discrepancy is that oestrogen affects renal urate transporters, which causes women to have higher clearance and less renal urate reabsorption. However, urate levels in postmenopausal and menopausal women are similar to those of adult males, and hormone replacement treatments may have an impact. Monosodium urate crystals (MSU) build up in tissues and cause gout, a systemic illness. Uric acid crystal production requires elevated serum uric acid (SUA) over a certain threshold. Many individuals with hyperuricemia do not develop gout or even create UA crystals, despite though hyperuricemia is the primary pathogenic defect in gout. In actuality, gout only occurs in 5% of patients with hyperuriceamia greater than 9 mg/dL. As a result, it is believed that gout is influenced by a number of additional factors, including hereditary predisposition. MSU crystals can create tophi in many tissues, but they are most commonly found in and surrounding joints. By identifying the pathognomonic MSU crystals through joint fluid aspiration or tophi aspirate, gout is primarily diagnosed. Acute joint inflammation, which is the initial manifestation of gout, is promptly alleviated by NSAIDs or colchicine. Tophi and renal stones are late appearances. The primary objective of gout care is to reduce serum uric acid levels below the deposition threshold, either by dietary changes or the use of medications that lower blood uric acid. As a result, MSU crystals dissolve, stopping additional attacks [22]
Pathogenesis of hyperuricemia
The body's ionised form of uric acid is called urea. With a pH of 5.8, uric acid is a weak acid. The deposition of uric acid crystals in tissues begins when the level of serum uric acid beyond the usual threshold. 6.8 mg/dL is the pathological threshold for hyperuricemia. The solubility of uric acid in the joint may be influenced by certain circumstances. These include the pH, water content, electrolyte level, and other synovial constituents including collagen and proteoglycans. The balance between SUA's creation—from purine intake in the diet or endogenous generation by cellular turnover—and its excretion by the kidneys and GIT determines the body's amount of SUA. Only 10% of gout cases are caused by increased UA production; the other 90% are brought on by renal under-excretion of UA [7].
Gender and age are two factors that influence SUA levels. SUA has few children. SUA levels begin to rise after puberty in order to return to normal. Levels are higher in men than in women. Nonetheless, postmenopausal women's SUA levels rise to match those of males. This explains why gout typically affects postmenopausal women and middle-aged and older men. In rare cases, it can occur in children and young adults due to inborn purine metabolism abnormalities. These enzymatic abnormalities lead to elevated SUA, which in turn causes the kidneys and joints to produce UA crystals
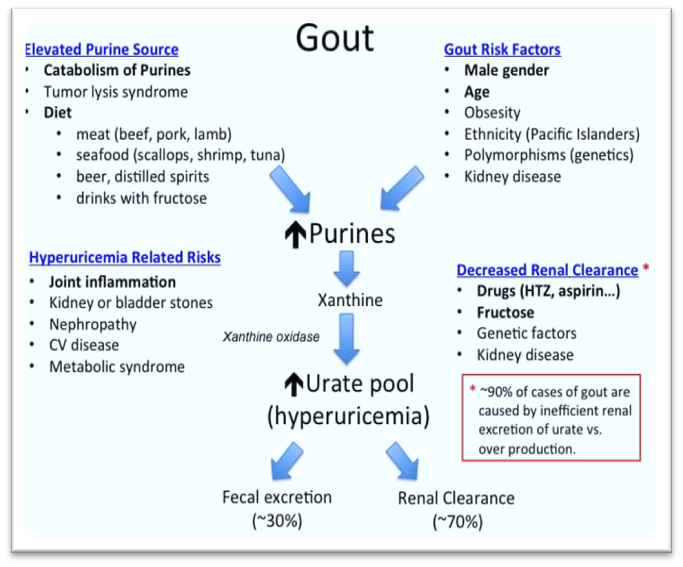
Figure 3. Pathogenesis of Hyperuricemia
Overproduction of uric acid
Deficiency of enzymes involved in purine metabolism leads to overproduction of UA. For example, Lesch-Nyhan syndrome is an inborn error of metabolism resulting from deficiency of an enzyme involved in UA metabolism named hypoxanthine–guanine phosphoribosyl transferase. It is a genetic X-linked recessive disorder with varying degrees of severity only 10% of gout cases are caused by increased UA production; the other 90% are brought on by renal under-excretion of UA. Gender and age are two factors that influence SUA levels. SUA has few children. SUA levels begin to rise after puberty in order to return to normal. Levels are higher in men than in women. Nonetheless, postmenopausal women's SUA levels rise to match those of males. This explains why gout typically affects postmenopausal women and middle-aged and older men. In rare cases, it can occur in children and young adults due to inborn purine metabolism abnormalities. These enzymatic abnormalities lead to elevated SUA, which in turn causes the kidneys and joints to produce UA crystals. based on the kind of mutation. In addition to renal stones, the disease's clinical picture includes neurological abnormalities such dystonia, chorea, cognitive impairment, obsessive harmful behaviour, self-mutilation, and articular symptoms (early onset gout). It can result in renal failure and tophi development if treatment is not received. Phosphoribosyl pyrophosphate synthetase's hyperactivity is another enzymatic anomaly that contributes to gout in young people. It is a hereditary illness that is X-linked dominant. There are two clinical versions of the syndrome: a moderate late juvenile or early adult-onset type and a severe early onset form in children. Neurological problems such as sensorineural hearing loss, hypotonia, and severe ataxia are included in the clinical picture. Arthritis and uric acid kidney stones are symptoms of the mild type. Nevertheless, less than 10% of cases of excessive urate production are caused by these enzymatic abnormalities.[23]
Diet
Consuming purine-rich foods, such as cooked or processed foods, particularly those derived from animals and seafood, is a major factor in raising the precursors of uric acid. Gout patients can consume foods high in purines of vegetable origin, such as beans, lentils, mushrooms, peas, legumes, and dairy products, since they do not pose a danger of hyperuricemia or gout. Additionally, a lower risk of hyperuricaemia and gout was linked to meals high in vitamin C, low-fat dairy products, and plant oils like olive, sunflower, and soy. Vitamin C can be used as a supplement to treat gout because it has been shown to improve renal excretion of uric acid. One well-known risk factor for gout is alcohol consumption. Research has indicated that the quantity of alcohol drank is correlated with its consumption. Additionally, the type of alcohol consumed affects the chance of developing hyperuriceamia and gout. For example, compared to spirits, beer has the highest risk of gout. However, wine was the alcoholic beverage with the lowest risk.[24]
Endogenous urate production
Increased endogenous uric acid production happens when cellular turnover is increased, as in inflammatory, haematological, and cancerous conditions. Additionally, tissue injury and chemotherapy may lead to an increase in purine synthesis. Additionally, obesity and excess body weight increase the formation of uric acid, which raises the risk of hyperuricaemia. It was discovered that leptin raised urate levels in the blood. Therefore, exercising and losing weight are excellent ways to lower SUA levels and the risk of developing gout.[25]
Decreased excretion of uric acid
The kidneys eliminate two-thirds of urate, with the gastrointestinal tract (GIT) handling the remaining portion. Decreased excretion of uric acid through the GIT due to reduced secretory activity of the transporter ABCG2 raises blood uric acid levels and increases renal excretion
Because uric acid crystals are insoluble, they need certain membrane transporters to pass through cell membranes. These transporters include the organic anion transporters (OAT1 and OAT3) and the urate transporter/channel (URAT), primarily URAT1. Four stages culminate in the excretion of uric acid by the kidneys. After UA passes through Bowman's capsule (glomerular filtration) in the first phase, practically all urates that pass through the proximal tubules are reabsorbed. Part of the reabsorbed UA is secreted during the third phase, which concludes with another reabsorption phase in the proximal tubules. Nearly 10% of the filtered urate passes through Bowman's capsule as expelled UA, with the remainder being reabsorbed by the organism.
Genes responsible for uric acid regulation
The transporter URAT1, which is found on the apical membrane of renal tubules, is encoded by the SLC22A12 gene. Another gene that controls the excretion of UA is SLC2A9. It codes for a transporter protein found in renal tubule membranes. When both genes are polymorphic, the fractional excretion of UA is reduced, which raises SUA levels. Both the GIT and the kidney's proximal tubular cells use ABCG2 as a gene transporter for UA. Important factors influencing SUA levels include the genes SLC17A1 and SLC17A3, which function as membrane transporters in the kidneys. SLC22A11, the glucokinase regulatory protein (GCKR), Carmil (LRRC16A), and the near PDZ domain containing 1 (PDZK1) genes are additional genes that are involved in determining SUA levels
Figure 4. Pathogenesis and different steps of progression of gout.
Impact of systemic diseases on uric acid
It appears that gout is more common in osteoarthritic joints, indicating that OA-induced cartilage damage leads to the formation of MSU crystals. It is interesting to note that UA crystals appear to affect the cartilage from its outer surface, while pseudogout crystals appear inside the cartilage. As a result of decreased vascularity and the synovial membrane's susceptibility to passing the crystals, UA crystals accumulate in the joint, causing gout to affect peripheral joints like the big toe. One risk factor for gout and hyperuricemia is hypertension. Reduced glomerular filtration rate from elevated systemic blood pressure causes a drop in glomerular blood flow and UA excretion Recent evidence, however, indicates that uric acid is a real modifiable risk factor for the development of essential hypertension and that hyperuricemia raises blood pressure Another important risk factor for gout and hyperuricaemia is diabetes mellitus (DM). When oxidative phosphorylation fails, adenosine levels rise, which raises uric acid synthesis and decreases renal excretion. By boosting its renal reabsorption from renal tubules, insulin therapy raises SUA. Gout and hyperuricaemia are also linked to metabolic syndrome.[26]
Treatments
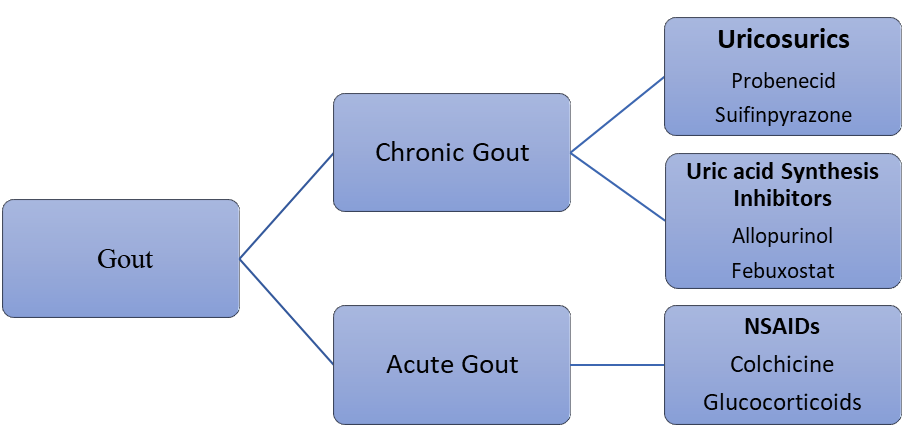
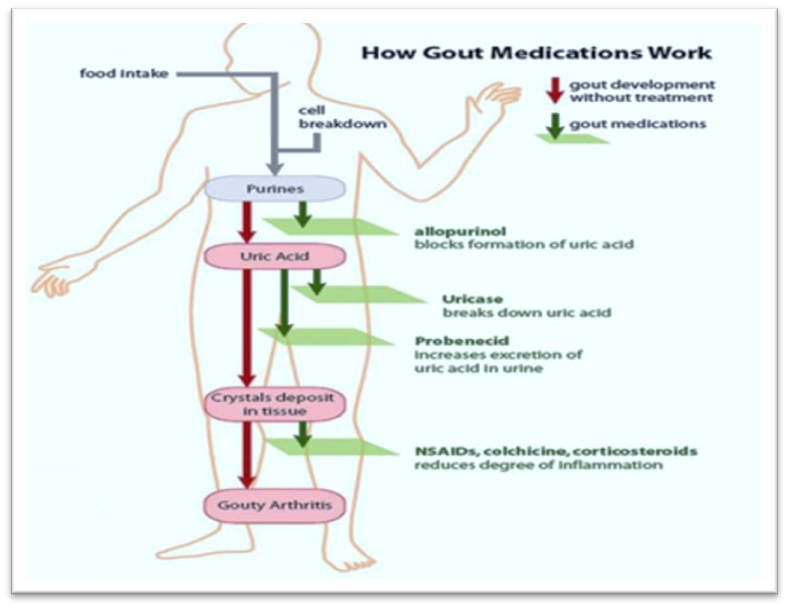
Figure 5. Gout Development and Treatment
The frequency and intensity of your gout symptoms, as well as your personal preferences, will determine the course of treatment that you and your doctor decide on.
Lifestyle changes
Some people may be able to avoid gout episodes by following a Mediterranean or DASH diet and losing weight if necessary. Doctors advised gout patients to avoid alcohol and red meat (beef, hog, lamb, and organ meats) for decades, but it is now known that a balanced diet is much more beneficial overall and has additional benefits for the heart, which is a typical concern for gout sufferers. According to a study involving over 45,000 men, gout was 42% more likely to strike those who consumed the traditional American diet, which includes red meat, French fries, sweets, and alcohol, than those who followed the DASH diet. Gout risk and uric acid levels were considerably decreased by following the low-sodium DASH diet, which places a strong emphasis on fruits, vegetables, nuts, whole grains, and other complete, unprocessed foods.
Anti-inflammatories
To halt an attack as quickly as possible. A short course of nonsteroidal anti-inflammatory medicines (NSAIDs), such naproxen (Aleve) and ibuprofen (Motrin, Advil), which come in stronger prescription and over-the-counter forms, is probably advised. Because NSAIDs can induce ulcers and intestinal bleeding, they are typically administered to those under 65 who do not use blood thinners or have a history of bleeding. Prescription anti-inflammatory colchicine reduces gout pain, but it can also cause unpleasant side effects like nausea, vomiting, or diarrhoea. Lower dosages have fewer adverse effects and are just as effective as higher dosages. Corticosteroids are also good at rapidly reducing inflammation, but they can have dangerous adverse effects. Gout treatment is guided by specific objectives. Reducing inflammation and discomfort is the main goal during acute flares. The long-term objective is to lower serum urate levels in order to prevent tophi flare-ups and regression. [27]
Introduction to Inflammation
Inflammation is a natural Defence mechanism that occurs in response to tissue injury. This complex process involves a series of biological changes, including enzyme activation, mediator release, and increased blood flow to the affected area. The primary goal of inflammation is to protect the body by removing harmful substances, repairing damaged tissue, and promoting healing. Inflammation can be acute or chronic. Acute inflammation is a short-term response that typically resolves on its own, although it may cause temporary discomfort. Chronic inflammation, on the other hand, is a long-term response that can lead to tissue damage and persistent health problems. While inflammation is a necessary response, it can sometimes be harmful. In cases where the inflammatory response is uncontrolled or misdirected, it can lead to tissue degradation, allergic reactions, or autoimmune disorders. Understanding the mechanisms of inflammation is crucial for developing effective treatments for inflammatory-related diseases.
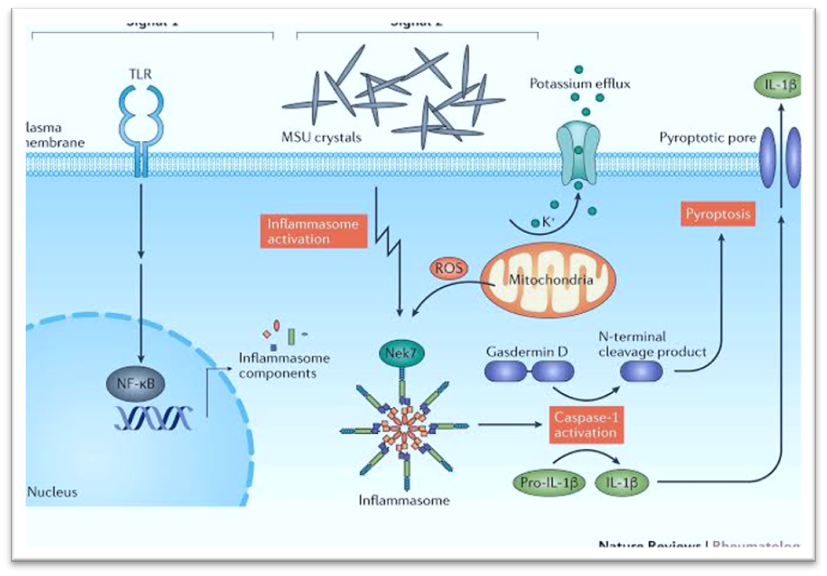
Figure 6. The inflammatory process in gout
Introduction to Anti-Inflammatory Agents
Inflammation is a natural response of the body's immune system, but chronic inflammation can lead to various diseases, including arthritis, diabetes, and cardiovascular disease. Anti-inflammatory agents are designed to reduce inflammation-induced pain, swelling, and tissue damage. These agents can be categorized into pharmaceutical medications, including non-steroidal anti-inflammatory drugs (NSAIDs) and steroidal medications, as well as natural anti-inflammatory agents found in foods, herbs, and supplements. Pharmaceutical anti-inflammatory agents, such as NSAIDs (e.g., aspirin, ibuprofen, and naproxen) and steroidal medications (e.g., corticosteroids), have been widely used to treat various inflammatory conditions. However, long-term use of these medications can lead to significant adverse effects.Natural anti-inflammatory agents, including omega-3 fatty acids, polyphenols, and curcumin, have gained attention for their potential health benefits. Certain herbs like Haritaki, Nirgundi, Punarnava, Guduchi, and Cocoa (theobromine) have anti-inflammatory, antioxidant, and immune-modulatory properties.These natural agents may provide a safer and more effective alternative for managing chronic inflammation-related issues.[28]
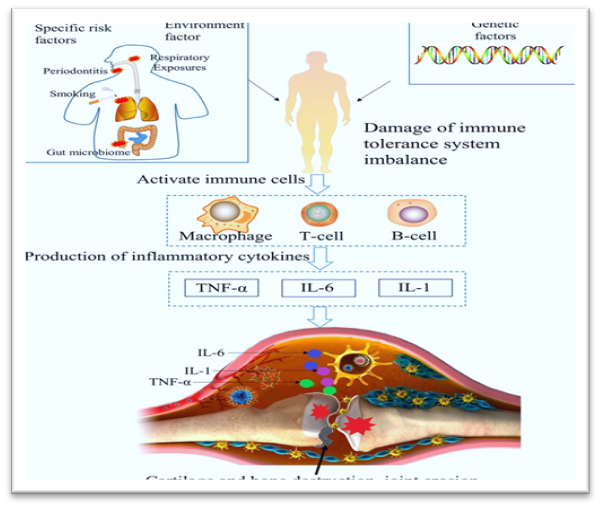
Figure 7. The mechanism diagram of inflammatory factors
Transdermal Patches
To get a certain amount of medication through the skin and into the bloodstream, a transdermal patch is utilised. The FDA first authorised transdermal patch products in 1981. There are currently transdermal delivery systems that contain nicotine to help people quit smoking, fentanyl for chronic pain, nitroglycerin and clonidine for cardiovascular illness, and scopolamine (hyoscine) for motion sickness. Transdermal delivery prevents pulsed entry into the systemic circulation, permits continuous input of medications with short biological half-lives, and offers controlled, continuous drug administration. Compared to traditional injection and oral techniques, TDDS has numerous benefits. It lessens the strain that the oral route often puts on the liver and digestive system. It improves patient adherence and reduces negative pharmacological adverse effects brought on by transient overdose. It is particularly useful for patches that only need to be applied once a week. Patient adherence to medication therapy is facilitated by such a straightforward dosage schedule.[29]
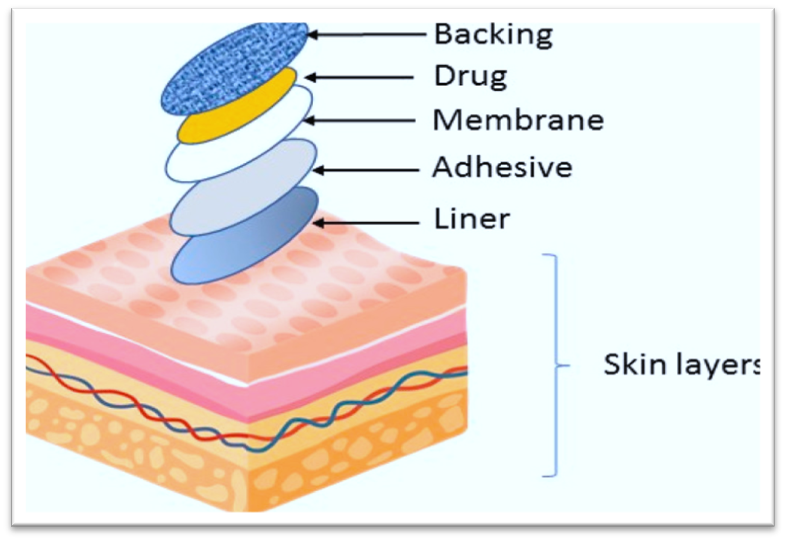
Figure 8. Components of Transdermal Patches
The main components to a transdermal patch are:
Drug Delivery Routes via Human Skin There are three methods that drug molecules can pass through human skin:
Large, flat, polyhedral, plate-like envelopes filled with keratin—a substance derived from dead cells that have moved up from the stratum granulosum—make up the stratum corneum, the outermost layer of the epidermis. Dead cells devoid of nuclei make up the majority of this skin layer. New cells from the stratum germinativum (basale) continuously replace these dead cells when they slough off on the surface in the thin, air-filled stratum disjunction. Ten to fifteen layers of corneocytes make up the stratum corneum, which ranges in thickness from roughly ten to fifteen μm when dry to forty μm when hydrated. It is primarily made up of keratin-rich corneocytes (bricks) arranged in a multi-layered "brick and mortar" structure within an intercellular matrix (mortar) that is made up of triglycerides, cholesterol, cholesterol sulphate, free fatty acids, long chain ceramides, and sterol/wax esters. Keratinocytes in the middle to upper stratum granulosum release their lamellar contents into the intercellular space, generating the intercellular lipid matrix. The stratum corneum's first layers reorganise to create wide, intercellular lipid lamellae, which subsequently unite to form lipid bilayers. The behaviour of the lipid phase differs from that of other biological membranes due to the lipid content of the stratum corneum. An key component of the stratum corneum, water serves as a plasticiser to keep it from cracking and contributes to the production of a natural moisturising factor that keeps it supple. [31] Determining the main route of drug permeation within the stratum corneum is crucial to comprehending the physicochemical characteristics of the diffusing drug and vehicle effect across the stratum corneum. In order to proceed to the next keratinocyte, a molecule that travels by the transcellular route must first partition into and diffuse across the estimated 4–20 lipid lamellae that separate each keratinocyte. For the majority of medicines, this sequence of partitioning into and diffusing across several hydrophilic and hydrophobic domains is not advantageous. As a result, it is presently thought that the intercellular route is the main mechanism that most medications pass through the stratum corneum.[32]
Transdermal Drug Delivery (TDD)
By applying a drug formulation to healthy, unbroken skin, TDD is a painless way to distribute medications systemically Without accumulating in the dermal layer, the medication first penetrates the stratum corneum before moving on to the deeper epidermis and dermis. Drugs can be absorbed systemically through the dermal microcirculation once they reach the dermal layer Compared to other traditional drug delivery methods, TDD has numerous benefits]. It can avoid problems like needle anxiety by offering a non-invasive substitute for parenteral methods. Numerous placement choices for transdermal absorption on the skin are made possible by the skin's enormous surface area and accessibility. Additionally, there are fewer peaks in the pharmacokinetic profiles of medications, which reduces the possibility of harmful side effects. In addition to being appropriate for patients who are vomiting or unconscious, or who depend on self-administration, it can increase patient compliance by lowering the frequency of doses. TDD improves bioavailability by avoiding pre-systemic metabolism. Regarding the application of the skin as a novel site for vaccination strategies, TDD is a desirable vaccination route for therapeutic proteins and peptides because the skin is known to be rich in dendritic cells in both the epidermal and dermal layers, which are essential for immune responses. [33-34]
Introduction To Skin
The skin, which covers the body's whole exterior, is the biggest organ. The epidermis, dermis, and hypodermis are the three layers of the skin, each of which has unique physical features and purposes (see Image. Cross Section, Layers of the Skin). The body's first line of defence against infections, UV rays, toxins, and mechanical harm is the complex network that makes up the skin. The amount of water released into the environment and temperature are also controlled by this organ.[35] The thickness of the epidermal and dermal layers affects skin thickness, which varies by body region. Because of the stratum lucidum, an additional layer in the epidermis, the hairless skin in the palms of the hands and soles of the feet is the thickest. Thin skin refers to areas that lack this additional layer. Because of its thick epidermis, the back has the thickest skin among these areas. Because of its barrier function, the skin is vulnerable to a number of infectious and inflammatory diseases. Furthermore, cosmesis, sensory alterations, and wound healing are important surgical issues. In many areas of medicine, addressing disorders requires an understanding of the anatomy and function of the skin. [36-37]
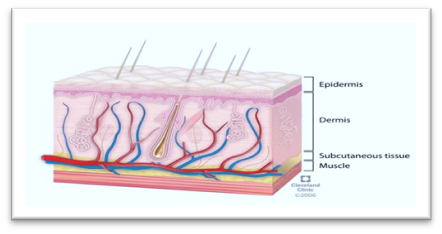
Figure 9. Schematic representation of the skin layers
Epidermis
The skin's outermost layer, the epidermis, is made up of multiple layers and different kinds of cells that are essential to its operation. The epidermis' layers: The stratum basale, stratum spinosum, stratum granulosum, stratum lucidum, and stratum corneum are the layers of the epidermis, arranged from deepest to shallowest. The basement membrane (basal lamina) separates the stratum basale, also called the stratum germinativum, from the dermis, and hemidesmosomes affix to it. Cuboidal to columnar, mitotically active stem cells that continuously generate keratinocytes make up this layer's cells. Melanocytes are also seen in this stratum. The stratum spinosum, commonly known as the prickle cell layer, is made up of eight to ten cell layers. Uneven, polyhedral cells with cytoplasmic processes—also referred to as spines—that protrude outward and make contact with nearby cells via desmosomes are seen in this layer. This layer contains dendritic cells. Diamond-shaped cells with keratohyalin and lamellar granules are found in the three to five cell layers that make up the stratum granulosum. Keratin precursors found in keratohyalin granules agglomerate, cross-link, and form bundles. The glycolipids released to the cell surfaces are found in the lamellar granules, which serve as an adhesive to preserve cellular cohesiveness. The thicker skin on the palms and soles contains the stratum lucidum, which is made up of two to three cell layers. Eleidin, a byproduct of keratohyalin transformation, makes up this thin, transparent layer. The topmost layer of the epidermis is occupied by the stratum corneum, which has 20 to 30 cell layers. Keratin and dead keratinocytes, which are anucleate squamous cells that produce horny scales, make up the stratum corneum. The thickness of this layer varies the most, particularly in callused skin. Defensins, which are a component of our first line of immune defence systems, are released by dead keratinocytes within this layer.The epidermal cells: Keratinocytes, melanocytes, Langerhans cells, and Merkel cells are examples of epidermal cells (see Image. Cells of the Epidermis). The majority of the epidermis' cells are keratinocytes, which come from the basal layer. The lipids and keratin produced by these cells are necessary for the formation of the epidermal water barrier. By permitting the skin to absorb UVB light, which is essential for vitamin D activation, keratinocytes also aid in the management of calcium. The primary component of skin colour, melanin, is synthesised by melanocytes, which are derived from neural crest cells. Between stratum basale cells are these cells. Melanin secretion is stimulated by UVB light, which serves as an internal sunscreen and protects against additional UV radiation exposure. Tyrosinase is an enzyme that converts tyrosine to dihydroxyphenylalanine, which is how melanin is formed. The lengthy processes that link the melanocytes to the nearby epidermal cells are subsequently responsible for the movement of melanin from cell to cell. Melanocytes send melanin granules to the cytoplasm of basal keratinocytes via the long processes. Through cytocrine secretion, keratinocytes phagocytose the tips of melanocyte processes, facilitating this transfer. Dendritic cells called Langerhans cells are essential for antigen presentation and serve as the skin's first line of defence against cellular immune responses. These cells in the stratum spinosum can be seen using special dyes. The mononuclear phagocytic system includes Langerhans cells, which are mesenchymal in origin and produced from bone marrow stem cells that are CD34-positive. Tennis racket-shaped cytoplasmic organelles and Birbeck granules are found in these cells. Major Histocompatibility Complex (MHC) I and MHC II molecules are expressed by Langerhans cells, which also take up and deliver antigens from the skin to the lymph nodes. Merkel cells are modified epidermal cells with an oval form that are located just above the basement membrane in the stratum basale. The fingertips have the highest concentration of these cells, which are mechanoreceptors for light touch and are present in the palms, soles, and oral and genital mucosa. Merkel cells have intermediate keratin filaments and use desmosomes to attach to nearby keratinocytes. Merkel cell membranes interact with the skin's free nerve terminals. [38-39]
Dermis
The basement membrane connects the dermis to the epidermis. The papillary and reticular connective tissue layers that make up the dermis blend together without obvious separation. The thinner top dermal layer, known as the papillary layer, is made up of loose connective tissue that comes into touch with the epidermis. The deeper, thicker, and less cellular layer is called the reticular layer. Collagen fibre bundles make up the dense connective tissue that makes up this layer. Sweat glands, hair, follicles, muscles, sensory neurones, and blood vessels are all found in the dermis.[40]
Hypodermis
Beneath the dermis is the hypodermis, sometimes referred to as the subcutaneous fascia. Adipose lobules, sensory neurones, blood arteries, and sparse skin appendages like hair follicles are all found in this layer, which is the deepest layer of the skin.
Functions
The skin's many functions demonstrate how intricate and crucial it is to preserving general health and wellbeing. Below is a discussion of these responsibilities. [41]
Drug Penetration Routes
Figure 09 diagrammatically illustrates the two potential channels for medication penetration through intact skin: the transepidermal and transappendegeal pathways. Molecules traverse the stratum corneum, a multicellular, multilayered barrier with a variety of architectural features, as part of the trans epidermal pathway. The terms intra- or inter-cellular can be used to describe trans epidermal penetration. Hydrophilic or polar solutes can be transported via the intracellular pathway via corneocytes, which are terminally developed keratinocytes. Diffusion of lipophilic or non-polar solutes through the continuous lipid matrix is made possible via transport via intercellular gaps. Molecules go through sweat glands and across hair follicles via the transappendegeal pathway. [42-43]
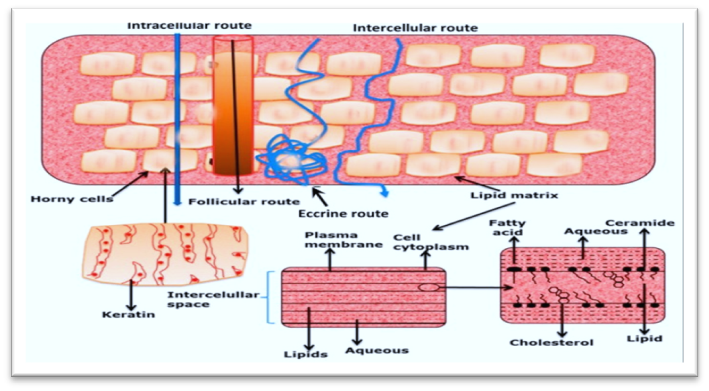
Figure 10. Possible drug penetration routes across human skin
AIM AND OBJECTIVES
Aim:-
Formulation and Evaluation of Polyherbal Transdermal Patch for Gout Therapy. A novel sustained-release polyherbal transdermal patch that effectively dissolves Monosodium Urate (MSU) crystals, reduces inflammation, and provides prolonged relief from gout symptoms, while minimizing the risk of adverse effects and improving patient compliance.
Objectives:-
Expected Outcomes
DRUG PROFILE
1] Punarnava [53]

Synonym: Spreding Hogweed, Red spiderling, Tar vine
Biological source: Boerhavia diffusa is a perennial herb with many medicinal uses. It's used in Ayurvedic, Unani, and Siddha medicine.
Family: Nyctaginaceae
Chemical constituents: Punarnavine, an alkaloid, Traces of nitrate and chlorates, Beta-sitosterol, Alpha-2-sitosterol, Palmitic acid, Archidic acid, Hentriacontance, Ursolic acid
Bioactive Compounds
Mechanisms of Action
Therapeutic uses
2]Guduchi [54]

Synonym: Giloy
Biological source: climbing shrub of tinospora cordifolia
Family: Menispermaceae
Chemical constituents: alkaloids, flavonoids, steroids, glycosides, terpenes and polysaccharides
Bioactive Compounds
Mechanisms of Action
Therapeutic uses:
3] Nirgundi [55]

Synonym: Vitex negundo, Aslak
Biological source: Shrub vitex negundo
Family: Verbenaceae
Chemical constituents: Flavanoids, volatile oil, triterpenes and lignans
Nirgundi (Vitex negundo) is a traditional Ayurvedic herb used for various health benefits, including antigout treatment. The herb contains several chemical compounds that contribute to its antigout properties:
Bioactive Compounds
Mechanisms of Action
Therapeutic uses:
4] Haritaki [56]

Synonym: Terminalia chebula, Black myrobalan
Biological source: Terminalia chebula tree
Family: Combretaceae
Chemical constituents: Tannins, gallic acid, saponin,sorbitol, chebulinic acid and other phytochemicals
Bioactive Compounds
Mechanisms of Action
Therapeutic uses: anti-inflammatory , To manage diabetes ,Promote digestion, improve oral hygiene
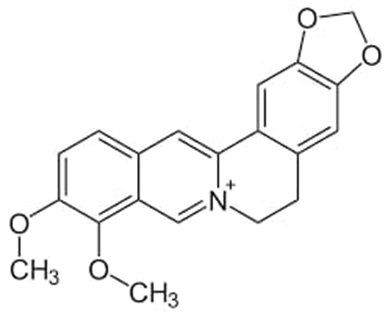
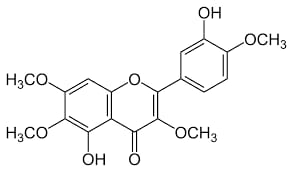
5]Cocoa plant: [57]

Synonyms: - "cocoa plant" include cacao tree, chocolate tree, and Theobroma cacao.
Biological Source: - Theobroma cacao, commonly known as the cocoa or cacao tree, is the seeds (cocoa beans) found within the fruits (pods) of this tropical evergreen tree
Family: Malvaceae family.
Chemical Constituent: - The chemical constituents of Theobroma cacao (cocoa) include bioactive compounds like flavonoids (catechins, epicatechins), methylxanthines (theobromine, caffeine), and polyphenols, along with lipids, proteins, and carbohydrates.
Bioactive Compounds
Mechanisms of Action
Primarily acts by inhibiting adenosine receptors and, to a lesser extent, by inhibiting phosphodiesterase enzymes, leading to various physiological effects like increased alertness, heart stimulation, and mild diuresis.
Therapeutic uses:
MATERIALS AND METHODS
Materials used:
|
Sr. No. |
Materials |
Source |
|
1. |
Punarnava |
STCOP, Shirur |
|
2. |
Haritaki |
STCOP, Shirur |
|
3. |
Guduchi |
STCOP, Shirur |
|
4. |
Nirgundi |
STCOP, Shirur |
|
5. |
Cocoa |
STCOP, Shirur |
|
6. |
Polyvinyl alcohol |
STCOP, Shirur |
|
7. |
HPMC |
STCOP, Shirur |
|
8. |
Eudragit RS-100 |
STCOP, Shirur |
|
9. |
Dibutyl phthalate |
STCOP, Shirur |
|
10. |
Polyethylene glycol 200 |
STCOP, Shirur |
|
11. |
Oleic acid |
STCOP, Shirur |
|
12. |
Methanol |
STCOP, Shirur |
|
13. |
Chloroform |
STCOP, Shirur |
|
14. |
Uric acid |
STCOP, Shirur |
|
15. |
NaOH |
STCOP, Shirur |
|
16. |
Sodium chloride |
STCOP, Shirur |
|
17. |
Sodium dihydrogen phosphate |
STCOP, Shirur |
|
18. |
Disodium phosphate |
STCOP, Shirur |
|
19. |
Bovine albumin |
STCOP, Shirur |
|
20. |
Allopurinol tablet |
STCOP, Shirur |
|
21. |
Diclofenac Sodium tablet |
STCOP, Shirur |
Equipment Used:
|
Sr. No. |
Equipment’s |
Source |
|
1. |
Magnetic stirrer with Hot plate |
STCOP/B.PH/-155/03/2022-2024 GI-1109 |
|
2. |
UV-Spectrophotometer |
STCOP/ B.PH/127/2019-20 (Jasco V 730) |
|
3. |
Incubator |
STCOP/B.PH. /1/123/2004-05 |
|
4. |
Electron Microscope |
STCOP/B.PH/D-3-18/01/22-23 GI-1109 |
|
5. |
Centrifuge |
STCOP/B.PH/1/114/1/2022-23 |
|
6. |
Diffusion cell apparatus |
STCOP/B.PH/1/117/2022-23 |
|
7. |
Colorimeter |
STCOP/B.PH/1-16/02/2022.23 |
|
8. |
Hot air oven |
STCOP/B.PH/105/2022-23 |
METHODOLOGY
The leaves of Nirgundi and Punarnava, the seed of Haritaki, and the stem of Guduchi/Giloy were obtained from Shirur,Pune.
These materials were identified by comparing them with an authenticated sample by a Prof.N.M.Ghangaonkar from Head of Department of Botany at C.T.Bora College,Shirur. The dried leaves, seeds, and stems were cut into small pieces and ground into a moderate to coarse powder and then kept in a dry place until extraction.
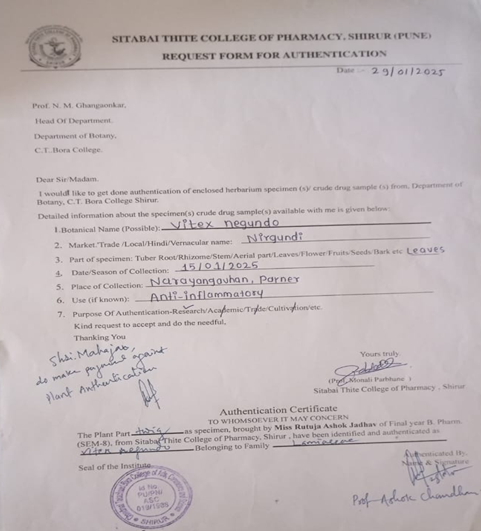
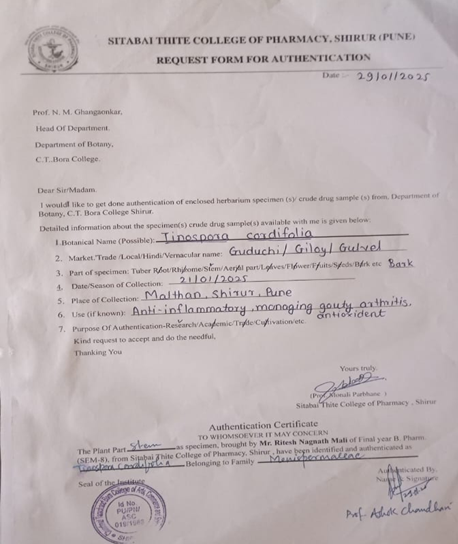
Figure 11. Authentication letter
1] Punarnava:[58]
2] Guduchi:[59]
3]Nirgundi:[60]
4]Haritaki:[61]
4] Theobromine from cocoa powder:[62]
Percentage yield:
|
Extract |
Predicted Yield (%) |
Experimental Yield (%) |
|
Punarnava |
35 .5 |
6.5 |
|
Guduchi |
4.26 |
1.2 |
|
Nirgundi |
1.5 |
0.35 |
|
Haritaki |
4.5 |
2.58 |
|
Cocoa |
2.57 |
1.8 |
Test for Alkaloids
• Dragendroff”s test
Dissolve a few mg of hydro-alcoholic until an acid reaction occurs, then add 1 ml of Dragendroff’s reagent, an orange or orange-red precipitate is produced immediately.
• Hager's test
1 ml of Hydroalcoholic extract of the drug was taken in a test tube, adding a few drops of Hager's reagent. Formation of yellow precipitate confirms the presence of alkaloids.
• Wagner's test
Acidifying 1 ml of hydro-alcoholic extract of the drug with 1.5% w/v of hydrochloric acid and adding a few drops of Wagner's reagent. A yellow or brown precipitate is formed.
• Mayer's test
Adding a few drops of Mayer's reagent to 1 ml of hydro-alcoholic extract of the drug. White or pale-yellow precipitate is formed.
Carbohydrates
• Anthrone test
Take 2 ml of Anthrone test solution, adding 0.5 ml of hydro-alcoholic extract of the drug. A green or blue colour indicate the presence of Carbohydrates.
• Benedict's test
Take 0.5 ml of hydro-alcoholic extract of the drug adding 5 ml of Benedict's solution and boiling for 5 minutes. Formation of a brick red coloured precipitate is due to the presence of carbohydrates.
• Fehling's test
Take 2 ml of hydro-alcoholic extract of the drug adding 1 ml of a mixture of equal parts of Fehling's solution 'A' and Fehling's solution 'B' and boiling the contents of the test tube for few minutes. A red or brick red precipitate is formed.
Molisch's test
In a test tube containing 2 ml of hydro-alcoholic extract of the drug adding 2 drops of a freshly prepared 20% alcoholic solution of ß- naphthol and mix, pouring 2 ml conc. sulphuric acid so as to from a layer below the mixture. Carbohydrates, if present, produce a red-violet ring, which disappears on the addition of an excess of alkali solution.
Flavonoids
• Shinoda's test
In a test tube containing 0.5 ml of hydro-alcoholic extract of the drug, adding 5-10 drops of dil. hydrochloric acid followed by a small piece of magnesium. In the presence of flavonoids a pink, reddish pink or brown colour is produced.
Proteins
• Biuret's test
To 1 ml of hot hydro-alcoholic of the drug adding 5-8 drops of 10% w/v sodium hydroxide solution followed by 1 or 2 drops of 3% w/v copper sulphate solution. A red or violet colour is obtained.
• Millon's test
Dissolving a small quantity of hydro-alcoholic of the drug in 1 ml of distilled water and adding 5-6 drops of Millon's reagent. A white precipitate is formed which turns red on heating.
Saponins
In a test tube containing about 5 ml of a hydro-alcoholic of the drug adding a drop of sodium bicarbonate solution, shaking the mixture vigorously and leave for 3 minutes. Honeycomb like froth is formed.
Steroids
• Liebermann-Burchard's test
Adding 2 ml of acetic anhydride solution to 1 ml of hydro-alcoholic extract of the drug in chloroform followed by 1 ml of conc. sulphuric acid. A greenish colour is developed which turns to blue.
• Salkowski Reaction
Adding 1 ml of conc. sulphuric acid to 2 ml of hydro-alcoholic of the drug carefully, from the side of the test tube. A red colour is produced in the chloroform layer.
Tannins
To 1-2 ml of plant hydro-alcoholic extract, adding a few drops of 5% FeCla solution was added. A green colour indicates the presence of gallotannins while brown colour tannins.
Glycosides
Detection of glycoside on paper spray solution No. 1 (0.5 % aqueous sol. of Sodium metaperiodate) & waiting for 10 minutes after then spraying solution No. 2 [0.5% Benzidine (w/v) in solution of Ethanol-acetic Acid (4:1)], white spot with blue background shows presence of glycoside.
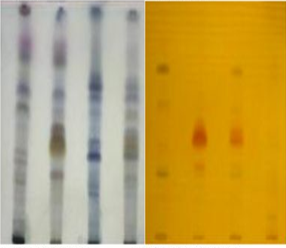
To isolate an extract using Thin Layer Chromatography (TLC) and Rf values, you can identify specific compounds based on their Rf values (the ratio of the distance a compound travels to the distance the solvent travels), and then use this information to isolate the desired compound(s) using preparative TLC or other chromatography techniques
Use UV light: Examine the plate under UV light (254 nm or 366 nm) to visualize compounds that absorb UV light.
Use other visualization methods: Other methods include spraying with specific reagents (e.g., iodine chamber, vanillin-sulfuric acid) to visualize specific types of compounds.
5. Calculate Rf (Retention Factor):
The RF value is a measure of how far a compound travels on a TLC plate compared to the solvent front. It's calculated as: Rf = (Distance travelled by the compound) / (Distance travelled by the solvent front).
Accurately 100mg of drug was weight and was dissolved in 100ml of pH 7.4 phosphate buffer to give a 1 mg/ml, which gave the 1st stock solution. From the 1st stock solution 2ml was pippetted and transferred to 100 ml volumetric flask and volume was make up with pH 7.4 phosphate buffer upto 100ml to give 20µg/ml, 2nd stock solution and so on . The sample solution were then scanned at UV Spectrophotometer at 264nm, 290nm, 302nm, 315nm, 285 nm and 294 nm for punanrnava extract, guduchi extract, Haritaki extract, Nirgundi extract ,cocoa extract and uric acid respectively ; absorbance were recorded, and graph was plotted between absorbance and concentration to obtain a calibration curved.
The functional groups present in the preparation were identified through FT-IR scanning microscopy. As IR rays passed through the sample, the absorbed radiations were transformed into vibrations or stretching, revealing spectrum signals ranging from 4000 cm-1 to 400 cm-1. These signals provided insights into the functional groups and the types of bonds present, forming a molecular fingerprint of the sample.
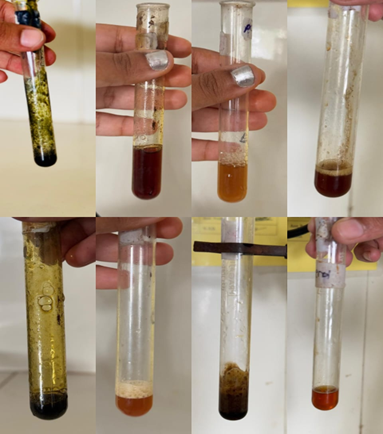
Preparing monosodium urate (MSU) crystals is a procedure commonly used in research to study gout or to investigate the immune response to crystalline substances. MSU crystals are known to trigger inflammation, making them useful for experiments related to inflammation and gout.
Dissolve Uric Acid:
Dissolve uric acid sodium salt in distilled water at a concentration of 10 mg/ml. The solubility of uric acid in water is quite low, so you will need to adjust the pH to fully dissolve it.
Adjust pH:
Heat the solution gently on a magnetic stirrer and hot plate to increase solubility. Add NaOH dropwise to the solution while stirring until the pH reaches 7.2-7.4, where uric acid is more soluble. This step is crucial for completely dissolving uric acid without forming unwanted salts.
Sterilization and Filtration:
After the uric acid is fully dissolved, and the desired pH is reached, cool the solution to room temperature. Filter the solution through a sterile 0.22 µm filter to remove any undissolved particles and to ensure sterility.
Crystallization:
Allow the filtered solution to cool to room temperature and then place it in a refrigerator (4°C) for at least 24 hours. This encourages the formation of MSU crystals. For larger crystals, you can leave the solution to crystallize for several days.
Drying:
After the final wash, spread the MSU crystals on a sterile petri dish or glass tray and let them dry in an oven set to a low temperature (below 60°C) or in a desiccator to avoid degradation. The drying process can take a few hours to overnight, depending on the method used.
Storage:
Store the dried MSU crystals in a sterile, airtight container at room temperature until needed.
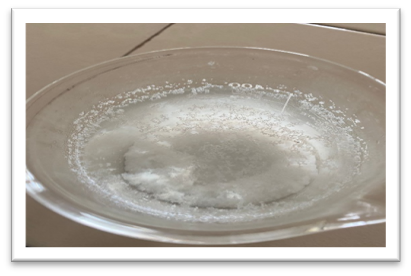
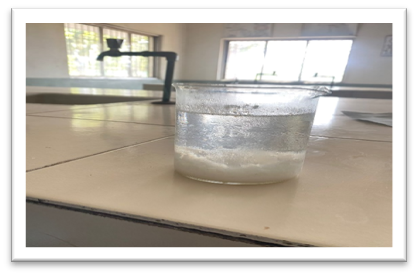
Figure 12. Preparation of Uric acid crystals
MSU crystal can be identified under a microscope using polarised light.
Step 1: Preparation of MSUA Crystals
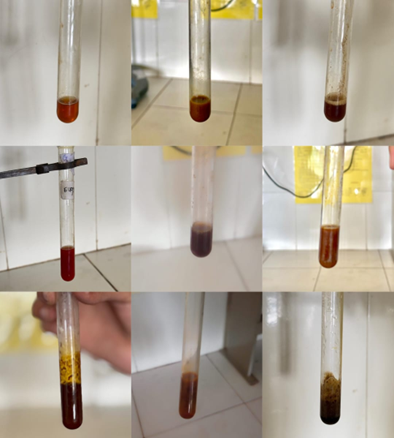
Step 2: Preparation of Polyherbal Extract
Step 3: Preparation of Dissolution Medium
Step 4: Dissolution Assay
Step 5: Sampling and Analysis
Step 6: Data Analysis
Step 7: Calculation of Parameters
Dissolution rate = (Concentration of dissolved uric acid at time t) / (Time t)
Dissolution efficiency = (Concentration of dissolved uric acid at time t) / (Initial concentration of MSUA crystals)
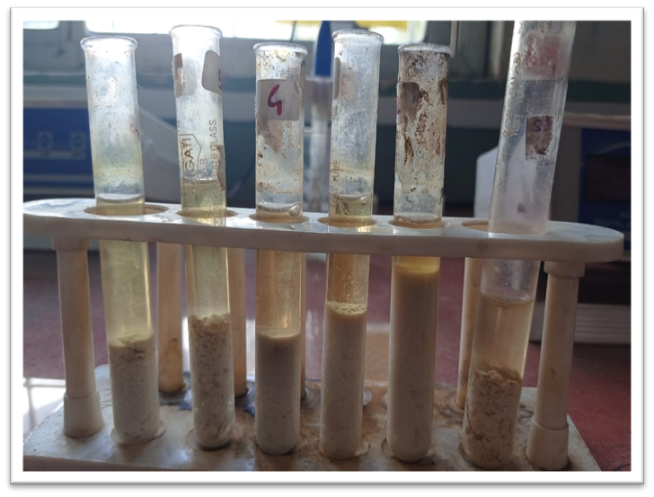
Figure 13. In vitro dissolution study of MSU crystal
Preparation of Backing layer: -

Figure 14. Preparation of backing layer
Preparation of Polymeric Drug Solution and Patch: -

Figure 15. Preparation of Polymeric Drug Solution and Patch
|
|
F1 |
F2 |
F3 |
|
Polyvinyl alcohol |
3 gm |
3 gm |
3 gm |
|
HPMC |
0.073 gm |
0.083 gm |
0.093 gm |
|
Eudragit RS-100 |
0.43 gm |
0.40 gm |
0.37 gm |
|
Dibutyl phthalate |
0.35 ml |
0.25 ml |
0.15 ml |
|
Polyethylene glycol 200 |
0.35 ml |
0.25 ml |
0.15 ml |
|
Oleic acid |
0.1 ml |
0.1 ml |
0.1 ml |
|
Methanol |
2 ml |
3 ml |
4ml |
|
Chloroform |
2 ml |
3 ml |
4ml |
|
Water |
5 ml |
5ml |
5ml |
|
Punarnava extract |
0.4 ml |
0.4 ml |
0.4 ml |
|
Haritaki extract |
0.4 ml |
0.4 ml |
0.4 ml |
|
Guduchi extract |
0.4 ml |
0.4 ml |
0.4 ml |
|
Nirgundi extract |
0.4 ml |
0.4 ml |
0.4 ml |
|
Cocoa extract |
0.4 ml |
0.4 ml |
0.4 ml |



Figure 16. Formulation of transdermal patch
1. Thickness of the patch: The thickness of the drug loaded patch is measured in different points by using a digital micrometer and the average thickness and standard deviation is determined to ensure the thickness of the prepared patch. The thickness of transdermal film is determined by travelling microscope dial gauge, screw gauge or micrometer at different points of the film.
2. Weight uniformity: The prepared patches are dried at 60°c for 4hrs before testing. A specified area of patch is to be cut in different parts of the patch and weigh in digital balance. The average weight and standard deviation values are to be calculated from the individual weights.
3. Folding endurance: A strip of specific area is to be cut evenly and repeatedly folded at the same place till it breaks. The number of times the film could be folded at the same place without breaking gives the value of the folding enoulence
4. Percentage Moisture content: The prepared films are to be weighed individually and to be kept in a desiccator containing fused calcium chloride at room temperature for 24 hrs. After 24 hrs the films are to be reweighed and determine the percentage moisture content from the below mentioned formula.
5. Content uniformity test: 10 patches are selected, and content is determined for individual patches. If 9 out of 10 patches have content between 85% to 115% of the specified value and one has content not less than 75% to 125% of the specified value, then transdermal patches pass the test of content uniformity. But if 3 patches have content in the range of 75% to 125%, then additional 20 patches are tested for drug content.If these 20 patches have range from 85% to 115%, then the transdermal patches pass the test.
6. Moisture Uptake: Weighed films are kept in desiccators at room temperature for 24 h. These are then taken out and exposed to 84% relative humidity using saturated solution of Potassium chloride in desiccators until a constant weight is achieved. % moisture uptake is calculated as given below.
7. Drug content: A specified area of patch is to be dissolved in a suitable solvent in specific volume. Then the solution is to be filtered through a filter medium and analyze the drug contain with the suitable method (UV or HPLC technique).
8. Stability studies: Stability studies are to be conducted according to the ICH guidelines by storing the TDDS samples at 40$0.5°c and 75+5% RH for 6 months. The samples are withdrawn at 0 30, 60, 90 and 180 days and analyze suitably for the drug content.
In vitro Drug Permeation study:
Diffusion cell apparatus was used to study the diffusion of the drug from the buccal mucosa of goat. The goat buccal mucosa was cut in appropriate size to fit into the cell. Freshly cut buccal mucosa was used. The dissolution medium consisted of 6 ml of phosphate buffer (pH 6.8). The diffusion was performed at 37oC ± 0.50C, with rotation speed of 50 rpm. Samples (1 ml) were withdrawn at predetermined time intervals (2,4 and 6... 60 min) and volume was replaced with fresh medium. The samples were filtered through Whatman filter paper and analyzed after appropriate dilution by UV spectrophotometry at 262nm, 290nm, 302nm, 315nm and 258nm of Punarnava, Guduchi, Haritaki, Nirgundi and Cocoa extract respectively.
|
Apparatus |
Diffusion Cell |
|
Dissolution Medium |
Phosphate Buffer Ph (6.8) |
|
Temperature |
37+0.5oC |
|
Volume |
6ml |
|
Speed |
50 rpm |
|
Sample Withdrawn |
1 ml |
|
Running Time |
20 min |
The objective of the study was to in vitro analyse anti-inflammatory activity using albumin denantation activity.
Preparation of egg albumin:
Anti-inflammatory activity by egg albumin by denaturation method:
Preparation of erythrocytes suspension:
Heat induces Haemolysis:
RESULT AND DISCUSSION
Identification test:
Table 1. Observation of Identification test
|
Sr. No |
Plant constituent |
Punarnava |
Guduchi |
Nirgudi |
Haritaki |
Cocoa |
|
1 |
Alkaloids |
+ |
+ |
+ |
+ |
+ |
|
2 |
Flavonoids |
+ |
+ |
- |
+ |
+ |
|
3 |
Saponins |
+ |
+ |
+ |
- |
+ |
|
4 |
Proteins |
+ |
- |
- |
+ |
+ |
|
5 |
Phenols |
+ |
|
+ |
+ |
+ |
|
6 |
Steroids |
+ |
+ |
- |
- |
- |
|
7 |
Tannins |
+ |
+ |
+ |
+ |
+ |
Isolation of extract by using TLC
Table 2. Observation of Isolation of extract by using TLC
|
Sample |
Solvent System |
Rf values |
|
Punarnava
|
Chloroform: Methanol (7.5:0.5) |
0.23, 0.33, 0.68, 0.78, 0.75 |
|
Guduchi |
Toluene: Ethyl acetate (5:1.5) |
0.19 |
|
Nirgundi
|
Toluene: Methanol: Formic acid (7.8:2.2:0.75ml) |
0.19, 0.20, 0.45, 0.5, 0.58, 0.66 |
|
Haritaki |
Toluene: Ethyl acetate: Formic acid (6:4:0.3) |
0.17 |
|
Cocoa |
Ethyl acetate: Ethanol (8:2) |
0.29 |
Stationary phase: Silica gel G
Punarnava, Guduchi

Nirgundi
Haritaki

Cocoa
Calibration Curve: -
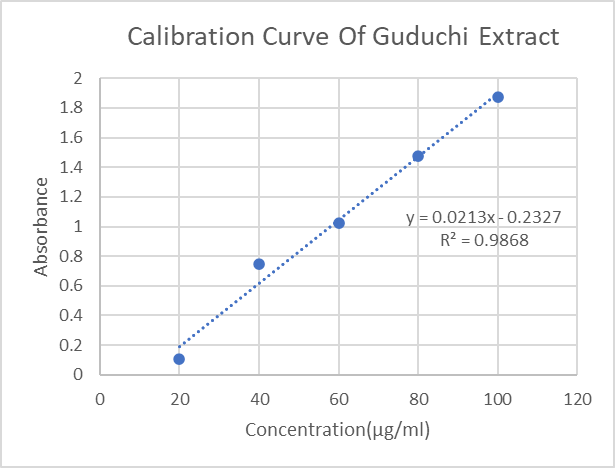
Figure 17. Calibration Curve of Guduchi Extract
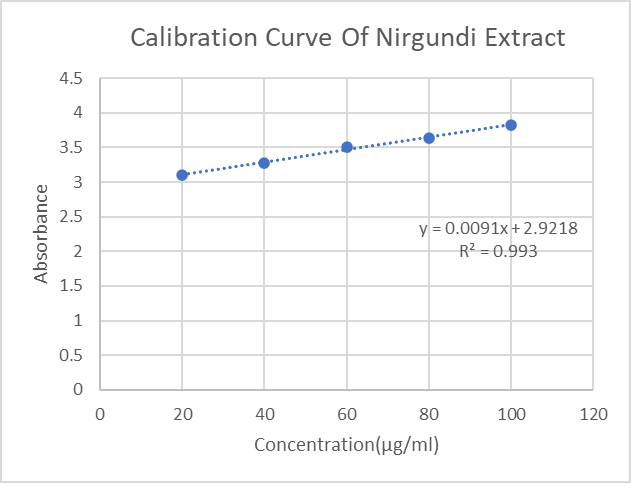
Figure 18. Calibration Curve of Nirgundi Extract
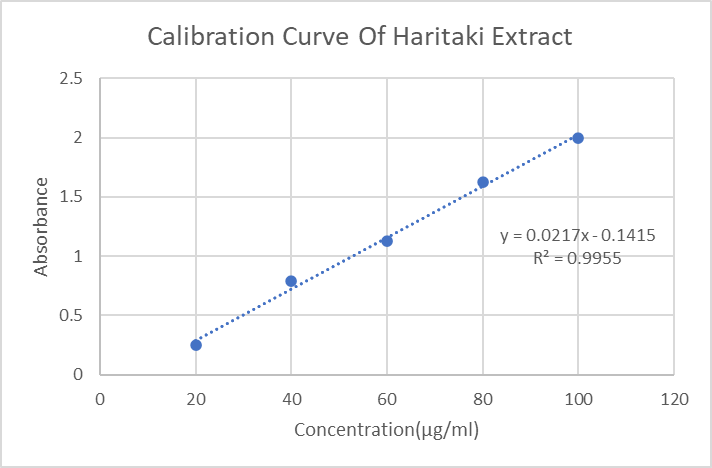
Figure 19. Calibration Curve of Haritaki Extract
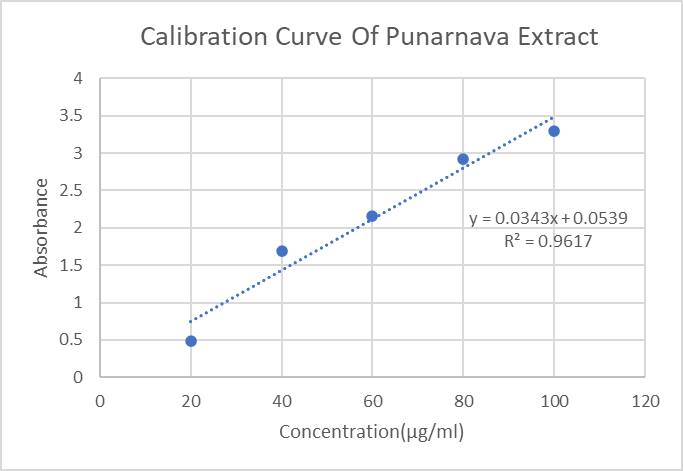
Figure 20. Calibration Curve of Punarnava Extract
5) Cocoa extract
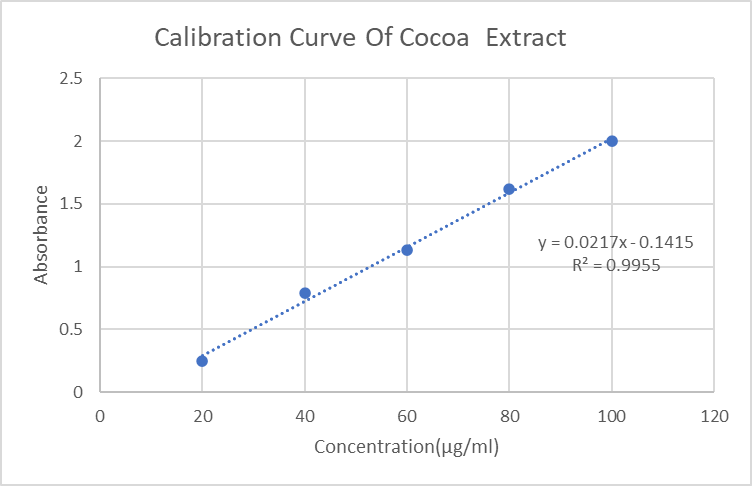
Figure 21. Calibration Curve of Cocoa Extract
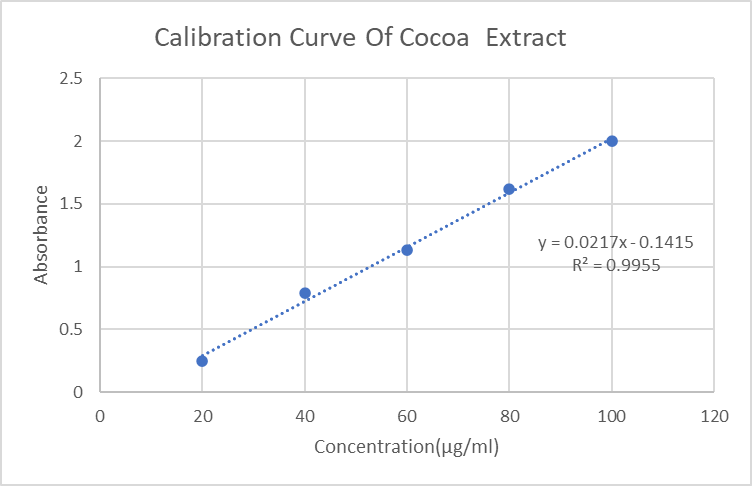
Figure 22. Calibration curve of Uric acid
FT-IR: -
Berberine
Table 3. Observation of IR Spectra of Guduchi extract
|
Sr.No |
Functional Character |
Vibrational Frequency (cm-1) |
|
1 |
C=O (Carbonyl) |
1710 |
|
2 |
C-H (Alkyl Halides) |
1122 |
|
3 |
N-H (Secondary Amines/Amides) |
2484 stretching vibrations |
|
4 |
Aromatic C-H |
3025-2916 |
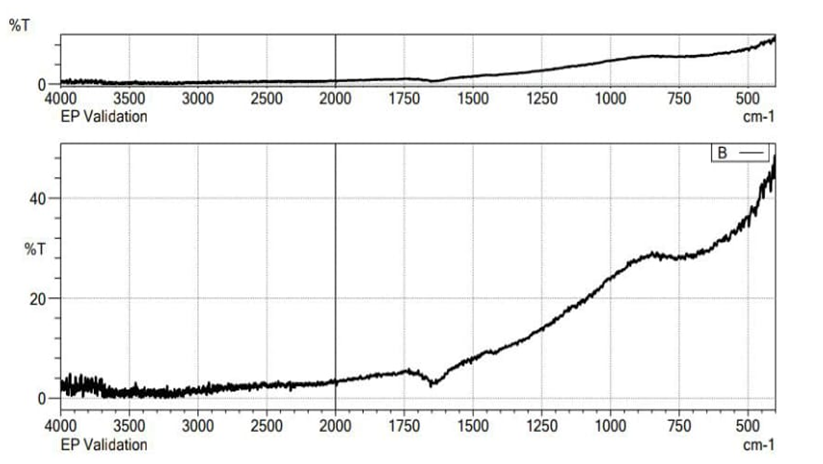
Figure 23. IR Spectra for Guduchi extract
Casticin
Table 4. Observation of IR Spectra of Nirgundi extract
|
Sr. No |
Functional Character |
Vibrational Frequency(cm-1) |
|
1 |
O–H stretching |
3200–3600 |
|
2 |
C=O stretching (from esters, ketones, or carboxylic acids |
1700–1730 |
|
3 |
C=C stretching (aromatic rings or alkenes) |
1600–1620 |
|
4 |
C–H bending and C–O stretching (especially in flavonoids and phenolics) |
1500–1300
|
|
5 |
C–O stretching (ethers or secondary alcohols) |
1100–1000 |
|
6 |
Aromatic C–H out-of-plane bending |
800-700 |
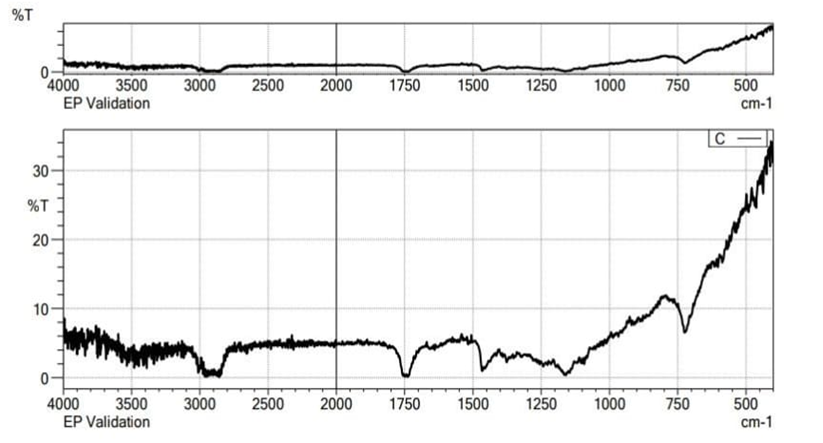
Figure 24. IR Spectra for Nirgundi extract
chebulagic acid
Table 5. Observation of IR Spectra of Haritaki extract
|
Sr.No |
Functional Character |
Vibrational Frequency (cm-1) |
|
1 |
Broad, strong peak indicating O-H stretching (alcohols, phenols, carboxylic acids). |
3600-3200 cm-1 |
|
2 |
C-H stretching (alkanes, alkenes, aromatics) |
3000-2850 cm-1 |
|
3 |
C=O stretching (aldehydes, ketones, esters, carboxylic acids) |
1700-1650 cm-1 |
|
4 |
C=C stretching (aromatic rings, alkenes).
|
1600-1450 cm-1: C=C stretching (aromatic rings, alkenes). |
|
5 |
C-O stretching (alcohols, ethers, esters). |
1100-1000 cm-1 |
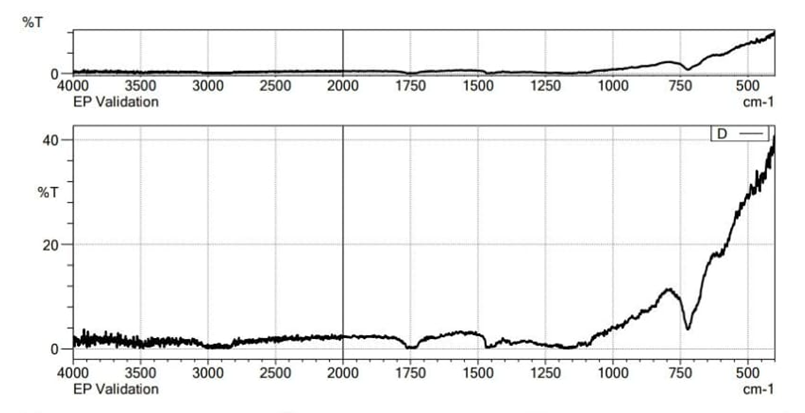
Figure 25. IR Spectra for Haritaki extract
Punarnavoside
Table 6. Observation of IR Spectra of Punarnava extract
|
Sr.No |
Functional Character |
Vibrational Frequency 1) |
|
1 |
O–H stretching (broad; from phenols, alcohols, and possibly carboxylic acids) |
3200–3600 |
|
2 |
C=O stretching (from esters, carboxylic acids, or ketones) |
1700–1725 |
|
3 |
C=C stretching (aromatic or conjugated systems, common in flavonoids) |
1600–1625 |
|
4 |
C–H bending and possible N–H bending (if alkaloids are present) |
1500–1300 |
|
5 |
C–O stretching (from alcohols, glycosides, and esters) |
1200–1000 |
|
6 |
Aromatic C–H out-of-plane bending |
800–700 |
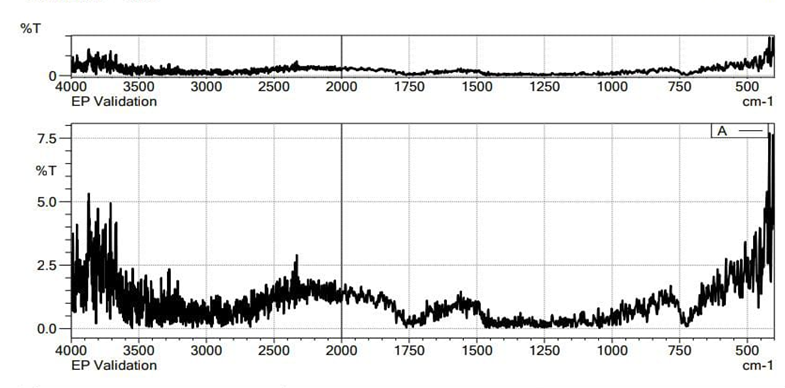
Figure 26. IR Spectra for Punarnava extract
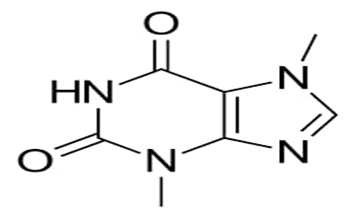
Theobromine
Table 7. Observation of IR Spectra of Cocoa extract
|
Sr. No |
Functional Character |
Vibrational Frequency(cm-1) |
|
1 |
N–H stretching (broad but moderate, may appear as two bands) |
3150–3400 |
|
2 |
C=O stretching (carbonyl groups in conjugated amide/urea-like system) |
1700–1720 |
|
3 |
C=C or ring stretching (aromatic-like vibrations) |
1600 |
|
4 |
C–N stretching |
1500–1300 |
|
5 |
Aromatic ring out-of-plane C–H bending |
800–700 |
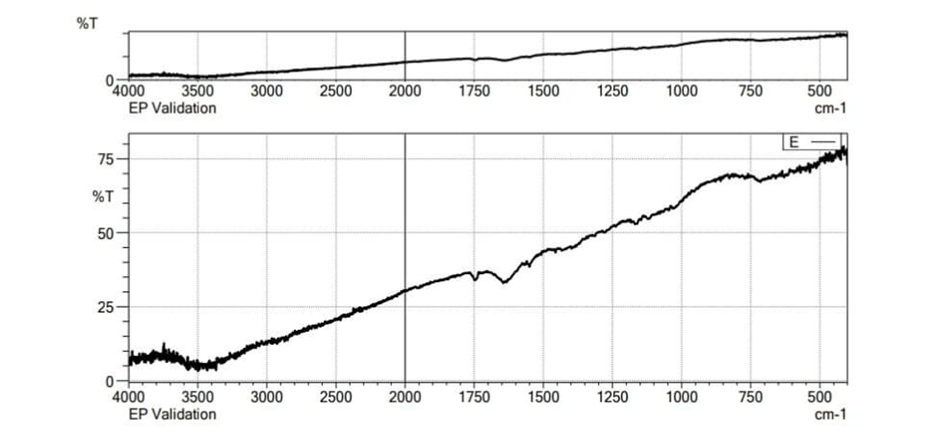
Figure 27. IR Spectra for Cocoa extract
The IR spectra showed similar characteristic peaks at their respective wavelengths with minor differences. The similarity in the peaks indicated the compatibility of drug with formulation excipients.
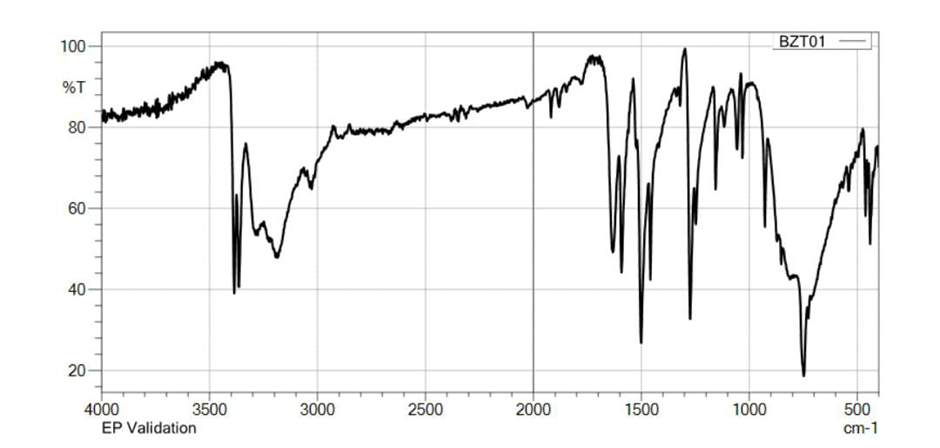
Figure 28. IR Spectra for Interaction of Polymer with extract mixture
Microscopic Evaluation of Mono Sodium Urate Crystals [MSU]:
Monosodium urate, a salt formed by uric acid ion, consists of one sodium ion, one water molecule. and one urate molecule bonded together. Under polarized light MSU crystals exhibit strong negative birefringence and appear as needle-shaped crystals with lengths ranging from 5 to 25 micrometers.
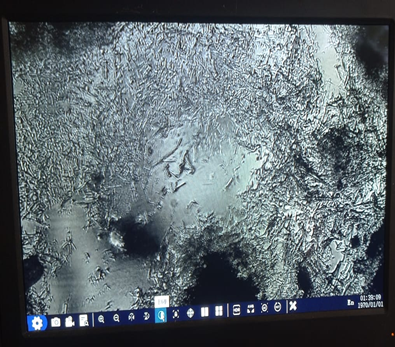
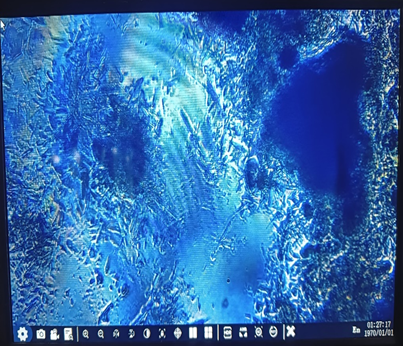
Figure 29. Microscopic Evaluation of Mono Sodium Urate Crystals [MSU]
In vitro dissolution study of MSU crystal
Table 8. Observation of In vitro dissolution study of MSU crystal at different concentration and time interval
|
Concentration Of Extract (mg) |
Time Intervals |
Absorbance by UV Spectrophoto- meter |
Absorbance by Calorimetry |
Weight of Crystal after drying (mg) |
|
0.5 |
0 min |
1.815 |
0.29 |
100 |
|
12 hr |
1.965 |
0.33 |
90 |
|
|
24 hr |
2.087 |
0.39 |
80 |
|
|
48 hr |
2.098 |
0.46 |
70 |
|
|
1 |
0 min |
1.193 |
0.31 |
100 |
|
12 hr |
1.278 |
0.37 |
90 |
|
|
24 hr |
1.429 |
0.38 |
70 |
|
|
48 hr |
1.593 |
0.45 |
60 |
|
|
1.5 |
0 min |
1.634 |
0.28 |
100 |
|
12 hr |
1.765 |
0.30 |
90 |
|
|
24 hr |
1.856 |
0.36 |
70 |
|
|
48 hr |
1.983 |
0.45 |
60 |
|
|
2 |
0 min |
1.748 |
0.30 |
100 |
|
12 hr |
1.923 |
0.42 |
80 |
|
|
24 hr |
2.197 |
0.48 |
60 |
|
|
48 hr |
2.439 |
0.53 |
40 |
|
|
2.5 |
0 min |
1.442 |
0.31 |
100 |
|
12 hr |
1.597 |
0.37 |
90 |
|
|
24 hr |
1.891 |
0.43 |
70 |
|
|
48 hr |
2.027 |
0.48 |
60 |
|
|
Standard (Allopurinol) |
0 min |
1.893 |
0.35 |
100 |
|
12 hr |
2.016 |
0.45 |
70 |
|
|
24 hr |
2.836 |
0.52 |
50 |
|
|
48 hr |
2.987 |
0.57 |
30 |
Table 9. Observation of In vitro dissolution study of MSU crystal dissolution rate and efficac
|
Concentration Of Extract (mg) |
Time Interval |
Concentration of dissolved MSU [mg] |
Dissolution Rate [mg/hr] |
Dissolution efficiency [%] |
|
0.5 |
0 min |
0 |
|
|
|
12 hr |
10 |
0.83 |
0.1 |
|
|
24 hr |
20 |
0.83 |
0.2 |
|
|
48 hr |
30 |
0.62 |
0.3 |
|
|
1 |
0 min |
0 |
|
|
|
12 hr |
10 |
0.83 |
0.1 |
|
|
24 hr |
30 |
1.25 |
0.3 |
|
|
48 hr |
40 |
0.83 |
0.4 |
|
|
1.5 |
0 min |
0 |
|
|
|
12 hr |
10 |
0.83 |
0.1 |
|
|
24 hr |
30 |
1.25 |
0.3 |
|
|
48 hr |
40 |
0.83 |
0.4 |
|
|
2 |
0 min |
0 |
|
|
|
12 hr |
20 |
1.66 |
0.2 |
|
|
24 hr |
40 |
1.66 |
0.4 |
|
|
48 hr |
60 |
1.25 |
0.6 |
|
|
2.5 |
0 min |
0 |
|
|
|
12 hr |
10 |
0.83 |
0.1 |
|
|
24 hr |
30 |
1.26 |
0.3 |
|
|
48 hr |
40 |
0.83 |
0.4 |
|
|
Standard (Allopurinol) |
0 min |
0 |
|
|
|
12 hr |
30 |
2.5 |
0.3 |
|
|
24 hr |
50 |
2.08 |
0.5 |
|
|
48 hr |
70 |
1.45 |
0.7 |
Dissolution profile: -
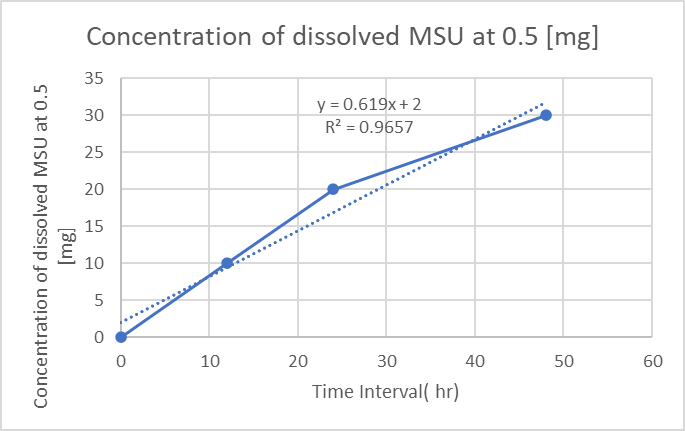
Figure 30. Concentration of dissolved MSU at 0.5 [mg]
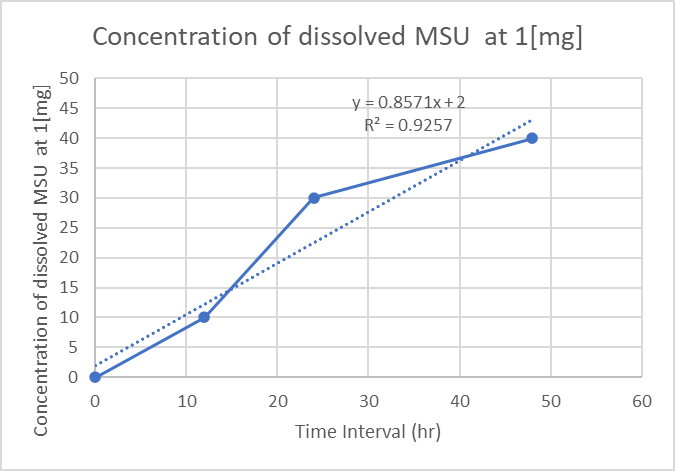
Figure 31. Concentration of dissolved MSU at 1 [mg]
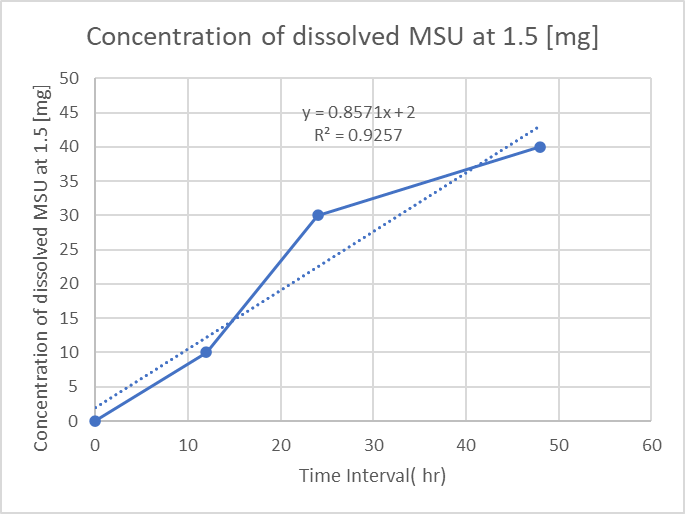
Figure 32. Concentration of dissolved MSU at 1.5 [mg]
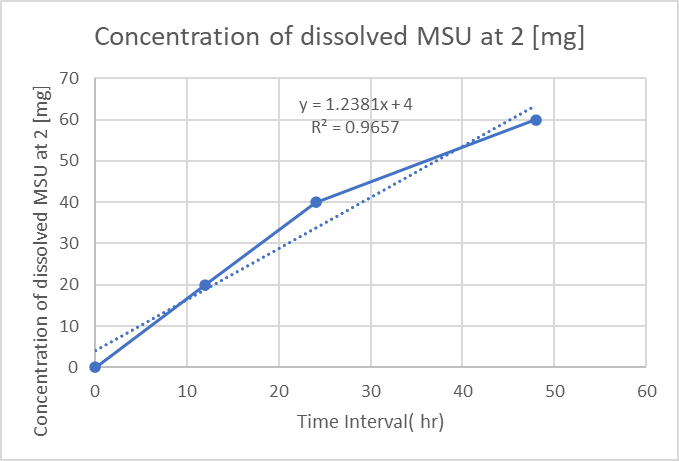
Figure 33. Concentration of dissolved MSU at 2 [mg]
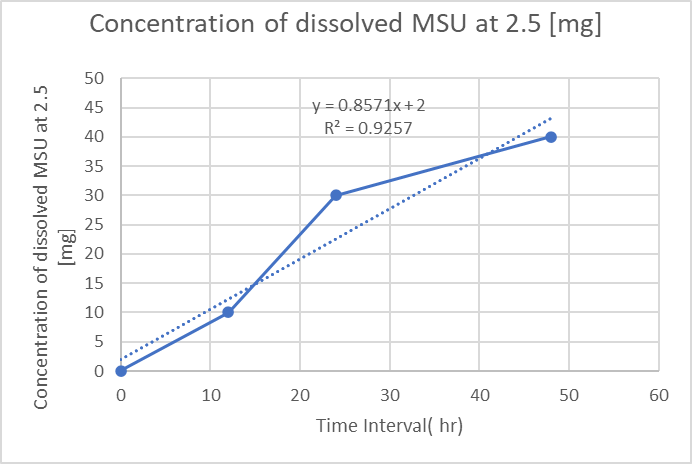
Figure 34. Concentration of dissolved MSU at 2.5 [mg]
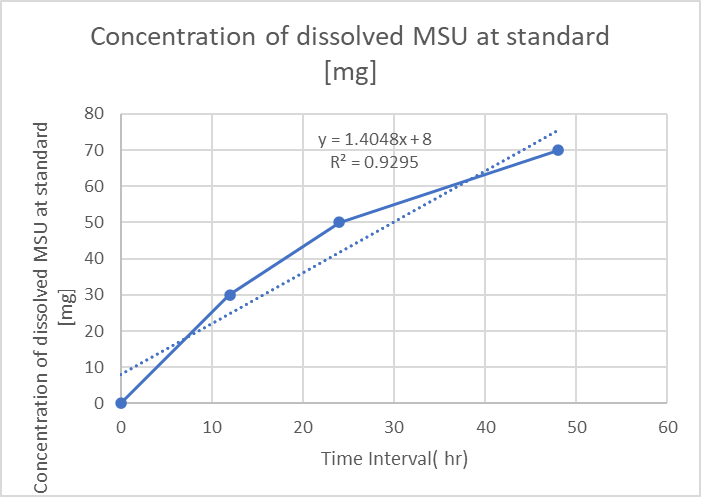
Figure 35. Concentration of dissolved MSU at standard [mg]
Evaluation Transdermal Patches:
Table 10. Observation of Evaluation Transdermal Patches
|
Sr. No. |
Evaluation parameters |
F1 |
F2 |
F3 |
|
A.
|
Organoleptic Evaluation |
|||
|
Rectangular Shape |
Rectangular Shape |
Rectangular Shape |
|
|
Brownish |
Brownish |
Brownish |
||
|
Transparent |
Transparent |
Transparent |
||
|
Yes |
Yes |
Yes |
||
|
Yes |
Yes |
Yes |
||
|
B. |
Weight |
0.35gm |
0.39gm |
0.46gm |
|
C. |
Thickness(mm) |
0.098 |
0.104 |
0.142 |
|
D. |
pH |
6.77 |
6.81 |
6.5 |
|
E. |
% Moisture content |
3.24 |
3.86 |
4.13 |
|
F. |
% Moisture Uptake |
5.27 |
5.35 |
6.01 |
|
G. |
Folding Endurance |
113 |
106 |
110 |
|
H. |
% Drug Content |
84.79 |
88.24 |
90.12 |

Figure 36. Appearance of transdermal patch
In vitro drug release study:
In vitro drug release studies of polyherbal patch formulation (F3) through Frans diffusion cell showed slow and sustained release of drug up to 9 hrs.
% Cumulative drug release of transdermal patch:
Table 11. Observation of % Cumulative drug release of transdermal patch (F3)
|
Time (hr) |
Punarnava |
Haritaki |
Guduchi |
Nirgundi |
Cocoa |
|
1 |
13.1 |
11.21 |
10.78 |
12.40 |
13.96 |
|
2 |
17.6 |
15.96 |
18.21 |
17.60 |
23.79 |
|
3 |
25.12 |
18.54 |
22.35 |
23.40 |
40.28 |
|
4 |
33.30 |
22.34 |
28.35 |
34.90 |
54.27 |
|
5 |
39.1 |
27.45 |
34.26 |
49.37 |
62.19 |
|
6 |
53.41 |
43.58 |
41.21 |
59.21 |
69.13 |
|
7 |
68.7 |
55.25 |
51.23 |
75.78 |
70.16 |
|
8 |
75.02 |
65.46 |
58.52 |
81.36 |
84.59 |
|
9 |
89.76 |
77.04 |
74.89 |
83.70 |
88.56 |
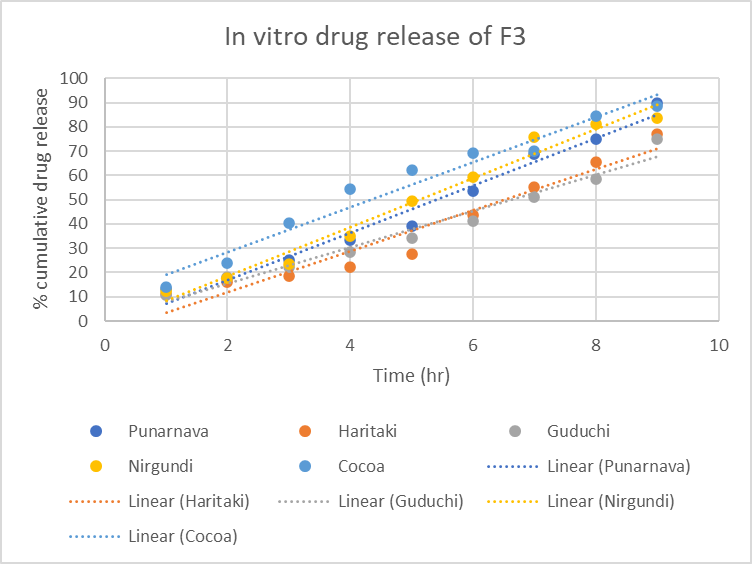
Figure 37. In vitro drug release study of F3 formulation
Stability study:
The stability studies were conducted on the most satisfactory formulation, F3, at two different conditions: (30 ± 2°C / 65 ± 5% RH) and (40 ± 2°C / 75 ± 5% RH) for two months, in accordance with ICH guidelines, to assess its long-term stability. The formulation was evaluated for physicochemical properties at 30-day and 60-day intervals, and no significant differences were observed, indicating that the formulated patches met all standard requirements for stability.
Table 12. Observation of Stability study of F3 formulation
|
Parameters |
0th day |
30th day |
60th day |
||
|
Organoleptic Evaluation |
|
|
|
|
|
|
Rectangular shape |
Rectangular Shape |
Rectangular Shape |
Rectangular Shape |
Rectangular Shape |
|
Brownish |
Brownish |
Brownish |
Brownish |
Brownish |
|
Transparent |
Transparent |
Transparent |
Transparent |
Transparent |
|
Yes |
Yes |
Yes |
Yes |
Yes |
|
Yes |
Yes |
Yes |
Yes |
Yes |
|
Weight |
0.46 gm |
0.45 |
0.44 |
0.44 |
0.43 |
|
Thickness [mm] |
0.142 |
0.141 |
0.140 |
0.149 |
0.138 |
|
pH |
6.5 |
6.5 |
6.5 |
6.5 |
6.5 |
|
%Moisture content |
4.13 |
4.11 |
4.10 |
4.08 |
4.08 |
|
%Moisture uptakes |
6.01 |
5.99 |
5.98 |
5.96 |
5.95 |
|
Folding endurance |
110 |
109 |
107 |
106 |
105 |
|
%Drug content |
90.12 |
90.10 |
90.08 |
90.05 |
90.01 |
In Vitro Anti-inflammatory activity
Inhibition of Protein Denaturation
Table 13. Observation of Inhibition of Protein Denaturation Test Sample and Standard vs. Conc
|
Sr.No. |
Concentration |
% Inhibition Sample |
% Inhibition Standard (Diclofenac Sodium) |
|
1. |
100 |
9.09 |
8 |
|
2. |
200 |
18.1 |
13.8 |
|
3. |
300 |
36.3 |
24.3 |
|
4. |
400 |
45.4 |
30.3 |
|
5. |
500 |
58.8 |
44 |
Graphical representation of % inhibition sample vs conc
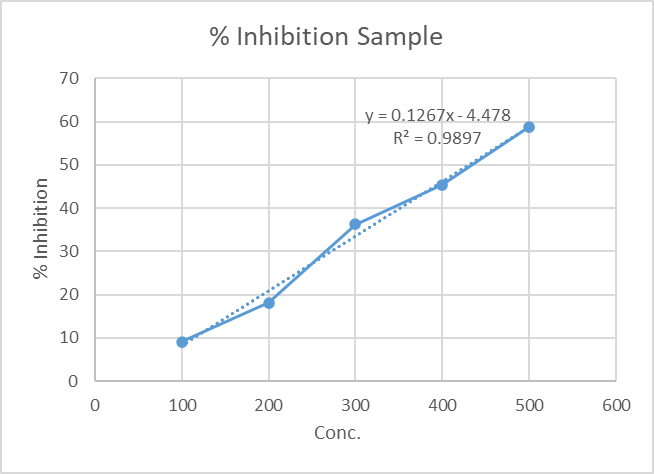
Figure 38. % inhibition vs. conc.of sample of Inhibition of Protein Denaturation
Graphical representation of % inhibition standard vs conc.
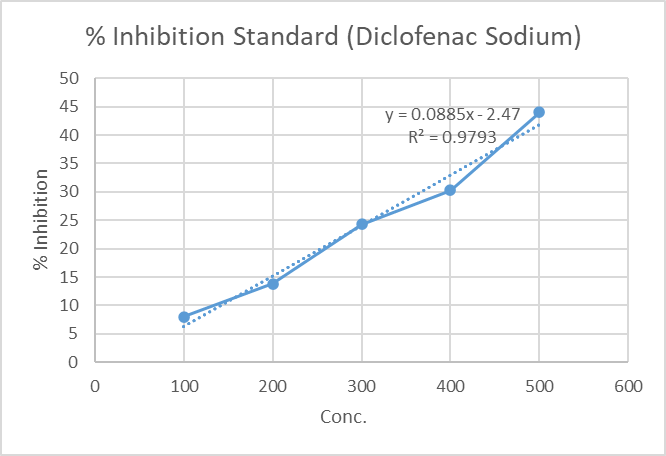
Figure 39. % inhibition vs. conc.of standard Inhibition of Protein Denaturation
Graphical comparison of sample and standard vs conc.
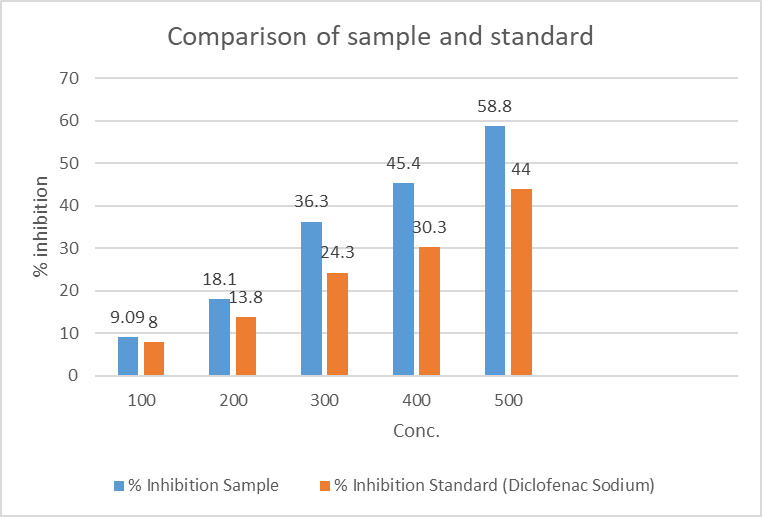
Figure 40. Comparison of Sample and Standard vs. Conc. of Inhibition of Protein Denaturation
Heat Induced Haemolysis:
Table 14. Observation of Heat Induced Haemolysis Test Sample and Standard vs. Conc
|
Sr. No. |
Concentration |
Sample (%) |
Standard (%) |
|
1. |
100 |
16.52 |
15.3 |
|
2. |
200 |
18.26 |
21 |
|
3. |
300 |
27.54 |
29 |
|
4. |
400 |
39.4 |
45.8 |
|
5. |
500 |
45.72 |
51.2 |
.Graphical representation of % inhibition vs conc.
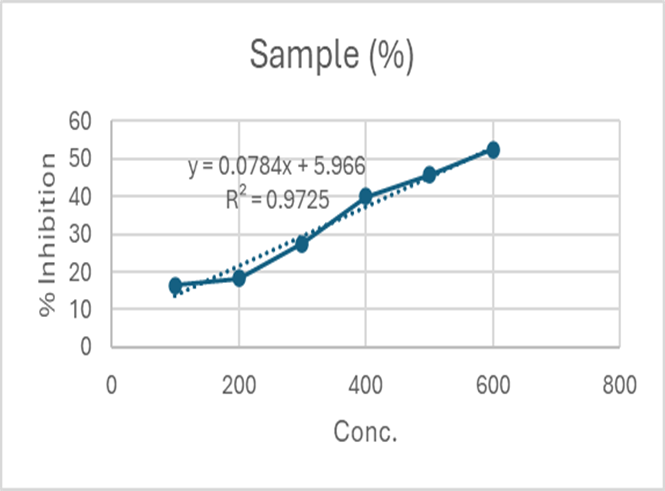
.Figure 41 . % inhibition vs. conc.of sample
Graphical representation of % inhibition vs conc.
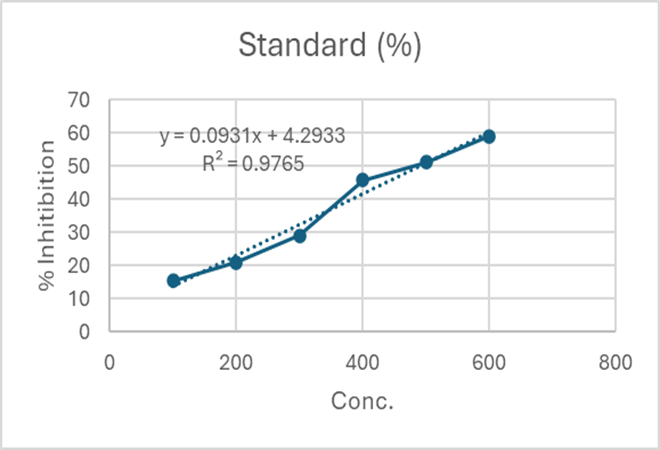
Figure 42 . % inhibition vs. conc.of standard
Graphical comparison of sample and standard vs. Conc.
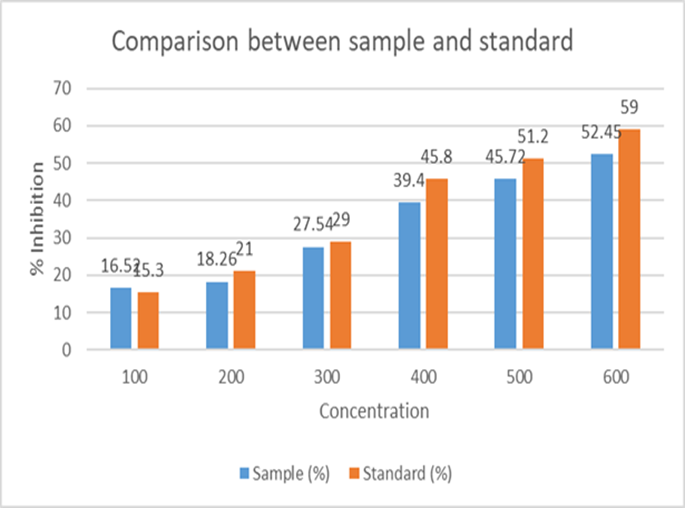
Figure 43. Comparison of Sample and Standard vs. Conc. of Heat Induced Haemolysis
CONCLUSION
In order to manage gout, the current study effectively investigated the creation and assessment of a transdermal patch as a unique sustained release drug delivery system. The study showed that transdermal patches can efficiently distribute anti-gout medication over an extended length of time through meticulous formulation and testing, providing a number of benefits over traditional oral medications. These benefits include decreased dose frequency, stable medication plasma levels, better patient compliance, and fewer gastrointestinal side effects that are frequently linked to oral delivery. The homogeneity, stability, and suitable mechanical strength of the prepared patches were validated by the physicochemical analysis. The development of a novel sustained-release polyherbal transdermal patch for gout therapy aims to provide effective symptom relief by dissolving Monosodium Urate crystals, enhancing bioavailability, and minimizing side effects, ultimately improving patient compliance and safety. This innovative approach promises significant advancements in gout management through controlled release and reduced adverse reactions. Formulation F3 shows the best results, with enhanced anti-inflammatory activity based on the organoleptic characteristics and physicochemical characteristics. Overall, the transdermal patch represents a promising alternative drug delivery system for gout treatment, potentially enhancing therapeutic outcomes and quality of life for patients. Future studies involving in vivo testing and clinical trials are recommended to further establish its efficacy and safety in human subjects.
REFERENCES








Monali Parbhane, Ritesh Mali, Sakshi Kachare, Rutuja Jadhav, Madhuja Walunj, Akanksha Rohakale, Shivdhan Shinde, Shravani Zende, Formulation and Evaluation of Polyherbal Transdermal Patch for Gout Therapy, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 5203-5253. https://doi.org/10.5281/zenodo.15754233
 10.5281/zenodo.15754233
10.5281/zenodo.15754233
