Valmik Naik College of Pharmacy, Telwadi, Kannad Chh. Sambhaji Nagar.
Scabies is a contagious parasitic skin illness caused by Sarcoptes scabiei var. hominis, which affects people of all ages around the world. The infestation develops predominantly by prolonged skin-to-skin contact, and symptoms include strong nocturnal itching, erythematous papulovesicular sores, and distinctive burrows. The disease burden is higher in overcrowded, resource-limited environments, as well as in immunocompromised people, who are more likely to develop severe forms such crusted scabies. The diagnosis is primarily clinical, supported by dermoscopy or microscopic examination of mites, eggs, or fecal pellets. Understanding the mite’s life cycle, transmission patterns, epidemiology, and host immune response is critical for timely discovery and management. Topical medications such as permethrin and lindane are used in treatment, as well as systemic therapy with oral ivermectin. To prevent reinfestation, all close contacts must be treated concurrently. Environmental Decontamination and public health awareness are critical for controlling outbreaks. This study highlights the causal agent, clinical symptoms, diagnostic techniques, and current preventive and treatment strategies for successful scabies care.
Aristotle and the Old Testament were the first to describe scabies.Sarcoptes scabiei gets its name from the Latin word “scabere,” which means to scratch, and the Greek words “sarx,” which means flesh, and “koptein,” which means to cut. The mite that causes scabies is an ectoparasite infection; it was isolated from human skin and identified by Bonomo in 1687. Renucci in Paris in 1814 demonstrated the disease in vivo and using light microscopy that same year (1–3).
Grouping The mite S. scabiei var hominis is the cause of the illness (2). S. scabiei is a 300–400 mm arthropod that is an obli-gate human parasite (4). It belongs to the order Astigmata, family Sarcoptidae, class Arachnids, and subclass Acari. These are ovoid creatures with a little anterior head and a caudal thoraco-abdominal section. The primitive legs have hair-like projections on them.
The presence of a unique head with mouthparts known as gnatosoma and the absence of a separation between the abdomen and cephalothorax allow them to be clearly identified from other arachnids (2,5). The male mite is half the size of the female, which is 0.3–0.4 mm in size (FIG. 2) (6). The mating of an adult male mite with a female mite initiates the life cycle of S. scabiei. The adult male dies after mating, and the female mite spends four to six weeks in the skin burrow laying her eggs. The female may live for 24 to 36 hours at room temperature (8) and crawls at a speed of 2.5 cm/minute on warm skin, not going beyond the stratum granulosum (7).

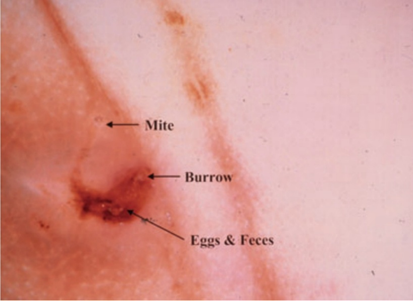
[FIG.1] Scabie Mites, Ova Feces.
The female lays one to three eggs every day, which hatch after three to four days to generate adult larvae. Before molting into either males or females, the larvae go through two more developmental stages: protonymphs and tritonymphs. Eventually, these larvae pierce the burrow’s roof and emerge at the skin’s surface. The life cycle lasts anywhere from 30 to 60 days (8). All phases of life can enter through the intact epidermis by secreting enzymes that break down the skin, which is then consumed. In less than half an hour, the mites can penetrate the skin. The mite population can reach up to 500 mites after 50 days and up to 25 adult females during the first month of infection.100 days (9). Nonetheless, 10–12 mites are often present on a typical host (7). In general, mite populations drop down quickly after three months. The human immunological response and mechanical elimination of the mites by scratching are likely answers. One month following the first infestation, for instance, sensitivity to mite antigens can be seen (9).
The human-specific mite Sarcoptes scabiei var. hominis is the cause of scabies, a parasitic skin ailment. Since adult mites are only about 0.4 mm in size, imaging tools are needed to see them [10,11]. When a pregnant female mite burrows on the human epidermis and produces two to three eggs per day, the life cycle of a scabies infection begins. After 48 to 72 hours, the majority of eggs laid in the burrows develop into larvae. In 10–14 days, larvae dig more burrows and mature into adults. The life cycle is’then repeated by adult mites through reproduction. After the first infection, the incubation period is thought to last four to six weeks. Mostly by direct skin-to-skin contact [11-13], but infrequently through indirect contaminated fomites, especially in individuals with crusted scabies [5,6,8]. Not living.

[FIG.2] Sarcoptes Scabiei.
Scabies mites can survive in thehuman host for 24 to 36 hours at room temperature, which allows for additional infection [12,13]
The study of epidemiology Scabies ”reverence fluctuates. Prevalence among the general population has been found to range from 4 to 27% in certain underdeveloped nations. [14] While the frequency of scabies is similar across all age groups in industrialized countries, it tends to be higher in preschoolers and adolescents in undeveloped countries. [15, 16] The idea that scabies outbreaks happen in 30-year cycles because of shifts in the host population’s immunological status is no longer recognized. [17, 18] Andrews [19] has charted the available data and found that the two World Wars were accompanied by two pandemics. As observed in New Zealand and Germany in the 1930s, isolated and unconnected epidemics do occasionally occur in addition to these two pandemics. There is no discernible regular cycle in the incidence.
The human scabies mite, Sarcoptes scabiei varietas hominis, is the pathogen responsible for causing scabies. The female adult measures approx. About twice as large as the male mite, measuring 0.3×0.4 mm. On the heated surface of the body, these parasites can travel at a speed of about 2.5 cm per minute. In the stratum corneum, pregnant females excavate superficial passages known as burrows (about 0.5–5 mm every day) and typically remain there for the next four to six weeks of their lives, depositing two to three eggs every day (20,21). Non-ovicidal antiscabies medications must therefore stay in the epidermis for at least this long since the larvae that hatch from them two to three days later swarm out onto the cutaneous surface and mature into in hair follicles and skin folds into nymphs, which develop into sexually mature mites within 9–17 days and copulate (22,23) The cycle restarts when the pregnant female mites burrow back into the skin and the male mites die soon after.
Only around 11 adult female mites are identified on the skin surface after the Immune response starts, as opposed to the otherwise anticipated exponential rise, which is explained by the fact that many defensive systems kill scabies mites by mechanical and immunological ways( 22):
leukemia, lymphoma, HIV or HTLV-1 infection, graft-versus-host disease, congenital immune deficiencies, drug-induced (systemic and topical corticosteroids, immunosuppressants, cytostatic agents, biological agents), and Down syndrome.
Extreme autoimmune disease, diabetes, liver disease, end-stage renal failure, drug and alcohol abuse, and undernutrition and malnourishment.
Leprosy, syringomyelia, spinal cord damage, sensory neuropathy, tabes dorsalis, and senile dementia.
Outside of the human body, the mites can live for 24 to 36 hours at room temperature. (21° C) and in relatively humid (40–80%) air (25,26). Higher humidity and lower temperatures allow them to live much longer (e 4). It only takes one pregnant mite or multiple larvae to infect another human host. This necessitates intense skin-to-skin contact lasting at least five to ten minutes in cases of common scabies, such as when nursing or snuggling a baby, engaging in sexual activity, or tending to nursing-dependent individuals (22, 25, 27).
All stages of mites can be wiped or washed away until they successfully penetrate the skin, which takes a little less than half an hour (26). Although there aren’t many scientific investigations on the quantity of mites or how they spread (22, 25, 26), the following hypotheses are tenable:
The number of mites—and, consequently, the transmissibility of infestation—is quite high until the specific immune response manifests and for a while following, after which the number of female mites significantly decreases (22). Medical examinations, handshakes, and hugs are insufficiently intensive types of contact to spread common scabies. Members of the same family or communal living group, as well as nursing-dependent individuals and those who care for them, are typically the contacts of individuals with common scabies who become infected (25). In common scabies, indirect transmission of the infection through clothing, furniture, or everyday use is uncommon but not completely insignificant (22). Even brief physical contact with the patient, exposure to the patient’s items, or dandruff can result in infestation in forms of scabies with numerous mites, especially crusted scabies (21, 29). In conclusion, the quantity of mites on the skin and the length and frequency of direct physical contact determine the likelihood of infestation transmission (21, 22, 28, 29).
After penetrating the skin, S. scabiei releases chemicals in reaction to kerati-nocytes and Langerhans cells (30), starting an immunological inflammatory response involving several cell types (31).
Both type I and type IV hypersensitivity reactions are present in the reaction. The type I reaction occurs when an antigen on the mite comes into contact with certain immunoglobulin-E (IgE) on mast cells in the epidermis. This causes the mast cells to degranulate, which results in wheal-and-flare reactions. The fact that IgE antibody levels are elevated in scabies patients and then fall following effective treatment lends credence to this (32).Furthermore, it has been reported that the scabies mite and the home dust mite are cross-reactive (33). Patients who have not come into touch with the mite will experience the rash in the type IV hypersensitivity reaction 10 to 30 days before it becomes apparent (32). A hypersensitivity reaction may appear within a day of a patient contracting the infection for the second time.
Scabies will eventually have increased antibody titers specific for parasite antigens and show significant superficial and deep dermal and perivascular inflammatory infiltrates made up of lymphocytes, histiocytes, and eosinophils. Interleukin-6 (IL-6) and vascular endothelial growth factor (VEGF) secretion are significantly elevated, while granulocyte colony stimulating factor (G-CSF) secretion is slightly elevated from normal human epidermal keratinocytes. While IL-8 and G-CSF encourage monocytes to develop into dendritic cells and neutrophils to proliferate, IL-6 is known to enhance the proliferation of kerati-nocytes (34). Additionally, IL-6 is known to stimulate Th1 CD4+ cells to release IL-2, which promotes their growth and differentiation, and to stimulate Th2 CD4+ cells to release IL-4, which stimulates the production of antibodies known to raise vascular permeability and start inflammation, which accounts for the edema seen in scabies lesions (31).
The hyperkeratosis observed in chronic and crusted scabies is clinically correlated with earlier research that demonstrated enhanced mitosis in keratinocytes in the basal layer of the epidermis (30, 35)
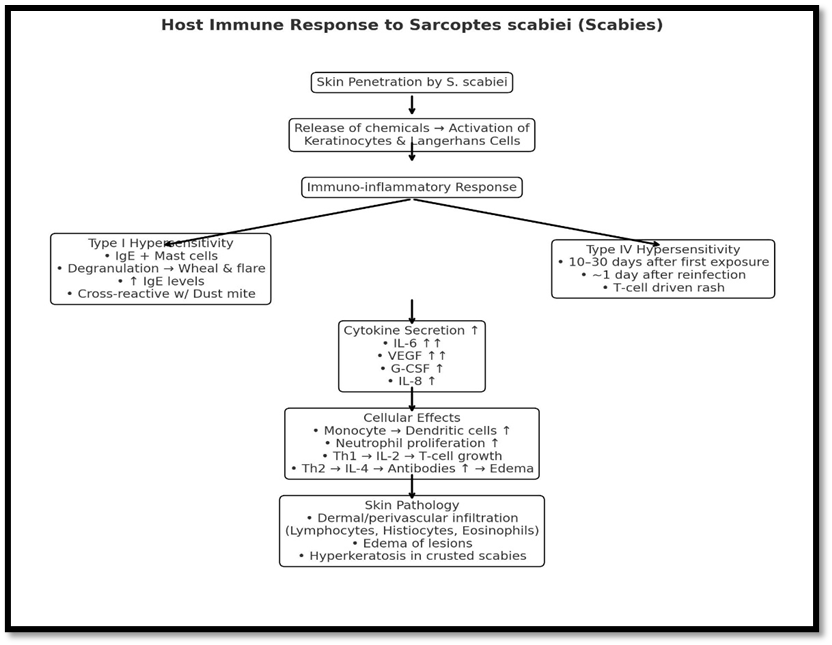
[FIG 3- Hot Immune Response
Types of scabies
The host immunological response to borrowed mites and their byproducts causes the most prevalent symptoms. The usual description of classic scabies is a severe, uncontrollable, widespread pruritus that is worse at night, while some patients may not have any symptoms at all (36).
The clinical manifestation is a small, erythematous papulovesicular rash that is usually symmetrical and preferentially affects the anterior axillary folds, the female nipple area, the periumbilical skin, the elbows, the volar surface of the wrists, the interdigital web spaces, the belt line, thighs, buttocks, penis, scrotum, and ankles. In adults, it typically spares the head, face, and neck, but it can also affect newborns and people with compromised immune systems.

[FIG.4] Burrows and excoriations in an infant with scabies.
Scabietic nodules and skin burrows are the pathognomonic lesions. The female mite’s tunnel is represented by the burrow, a narrow, serpiginous gray line that measures 1 to 10 mm (37). It is located on the hands and feet, namely on the finger web gaps, thenar, and hypothenar eminences. Distinct on the wrists (FIG. 4) Figure 2. Excoriations and burrows in a scabies infant. Scabies Lesions are frequently written off as excoriated or impetiginized skin, and burrows are rarely apparent to the unaided eye (38).

[FIG.5] Acral pustules in scabies.
A high index of suspicion is required in order to make the diagnosis. In addition, the clinical distribution and history of itching in other family members are almost pathognomonic.
Scabies in newborns and young children affects the neck, face, and scalp; however, infantile scabies is specific to the palms and ssoles (39). Very young infants may appear unhappy, feed poorly, and not scratch. Clinically, vesicles and brownish to pinkish nodules are frequently observed with plaques, pustules, or nodules. Common are acral pustules (FIG. 5). The use of topical steroids or a bacterial superinfection frequently results in changes to the rash’s appearance. Genital or groin nodules may be more common in adulthood (FIG. 4 and 5).
The Most patients will report having a severe itching sensation, particularly at night and after taking a hot shower. A hypersensitivity reaction to the excreta that the mite deposits inside the burrow has been linked to this (40).
2 Nodular scabies:
The glans, scrotum, thighs, and axilla are the most common locations for these violaceous, itchy nodules, which can last for several months and from which mites cannot be extracted (41). This is thought to be a type of hypersensitivity reaction to mite antigens that results in nodules. It can be misdiagnosed as urticaria pigmen-tosa (43), B-cell lymphoma or lymphomatoid papulosis (42), or chronic lymphocytic leukemia. Intralesional corticosteroids (44) or topical pimecrolimus twice daily (45), are two possible treatments.
3 Vesicular – bullous scabies:
t is an uncommon clinical manifestation that typically occurs in the elderly. Clinically, histologically, and in immunofluorescent results, it resembles bullous pemphigoid (46–47). According to theories, superinfection with Staphylococcus aureus could explain the mechanism, which would resemble how blisters form in bullous impetigo (48). Additionally, some believe that the mite’s penetration of the dermo-epidermal junction, cross-reaction with bullous pemphigoid antigen, or lytic secretions generated at the dermoepidermal connection may promote the synthesis of autoantibodies, which in turn trigger complement activation (49). Pemphigoid, pemphigus, bullous impetigo, epidermolysis bullosa, arthropod bite reaction, and acute contact dermatitis are among the differential diagnoses (46).
4 Special forms of scabies:
Due to their unusual presentation, these varieties are frequently misdiagnosed.
Incognito. This alters the clinical aspect of lesions and is caused by the administration of topical corticosteroids (44). There exists a correlation between mildly reduced immunity and hypereosophilia (50).
Infants and young children. Frequently, they are misdiagnosed. Lesions in clinical practice are primarily found on the hands, feet, and body folds and consist of more vesicles, pustules, and nodules. Patients may exhibit poor feeding and irritability (51). Histologically, there may be a thick infiltrate of Langerhans cells, which could lead to a misdiagnosis as Langerhans cell histocytosis.
Elderly. Often misdiagnosed as senile pruritus, they are treated with strong corticosteroid medications for extended periods of time, which might result in crusted scabies. Bullous scabies is another clinical manifestation that might resemble bullous pemphigoid (42,52).
Scabies of the scalp. Dermatomyositis and seborrheic dermatitis may be related or similar. More prevalent in patients with crusted scabies, children, newborns, the elderly, and immunocompromised people (41).
Crusted. Previously referred to as Norwegian scabies, it was initially identified in leprosy patients in Norway in 1848. Immunosuppression (topical or systemic glucocorticoid medication, HIV, human T lymphotropic virus 1 (HTLV-1) infection, organ transplant recipients), psychologically retarded, physically disabled, and indigenous Australians without a recognized immune deficiency are the causes of this (42,53,54).
Clinically, the hands, feet, knees, elbows, trunk, scalp, nail beds, and occasionally the entire body are affected by thick, gray, scaly, hyperkeratotic, or crusted plaques (55). Patients with crusted scabies frequently have mites under their nails, which can lead to thickenednails with dystrophies. Larger mite populations in crusted scabies may result in longitudinal nail splitting and subungual hyperkeratosis, although in normal scabies, the distal ends of nails may house scabies mites, where they are shielded from topical treatment (56). Untreated nails may serve as an infection reservoir, leading to treatment failure and symptom recurrence months later (57).
In certain instances, there is eosinophilia and generalized adenopathy (51). These patients have a high mite infestation and exhibit physical limitations, lack of control, or ignorance of the defensive scratching movements, such as in neuropsychiatric disorders, osteoarticular deformities, muscular atrophy, or other neuromuscular problems occasionally associated with loss of sensation, hypoesthesia, or anesthesia. Additionally, due to altered immune response in immunocompromised subjects, itching is less severe or absent in thesedisorders of patients(58).
Mites are abundant in the crusts, which flake off and contaminate clothes, linens, curtains, walls, floors, furniture, and the surrounding area. The mites stay infectious for two to three days after this. High fatality rates from secondary sepsis are associated with crusted scabmites( 59). After receiving inflix-imab treatment for juvenile rheumatoid arthritis, a case of crusted scabies was recorded. This was believed to be secondary to the patient’s susceptibility to a severe infection due to its immunomodulatory effects on cellular immunity (60). Psoriasis is a differential diagnosis (61).
Subungual scabies. Despite being well-known, this condition is frequently misdiagnosed. Even after effective treatment, it still shows up as nail plate dystrophy (62). Numerous fingernails and/or toe nails may be affected; they appear thicker and whiter, with or without subungual horny debris and/or nail plate deformity. This can possibly be the first sign of scabies (63).
Because scabies causes continual itching, the scratching may capture live mites that can live beneath the nails and subsequently spread across the skin, beginning proximally around the nail. When patients are treated, this will aid in reinfestation. For this reason, in addition to the usual therapy, it is advised to cut the nails extremely short and then brush the tips of the fingers with scabicidal for a few days in a row (64).
Canine. The prevalence of canine scabies infection in humans is unknown, and it is frequently misdiagnosed as papular urticaria or insect bites. Additionally, it is a severe rash that appears on parts of the body that come into contact with the pet, such as the chest, belly, thighs, and forearms. It appears 24 to 96 hours after the encounter and lasts for 5 to 13 weeks on average. Patients may exhibit fever, lymphadenopathy, and a subsequent bacterial infection in more complex cases. Patches of hair loss and/or scratching make it easy to identify the pet. According to some reports, var hominis may develop some protective immunity as a result of repeated exposure to S. scabiei var canis. All that has to be done is treat the dog (65).
dermatitis are examples of differential diagnosis. Scabies infestation can be mistaken for immunobullous illness, Langerhans cell histiocytosis, and severe medication reactions (66, 67–68). All individuals experiencing widespread impetigo in hot, humid climates should have their scabies status checked.
The Scabies is mostly diagnosed based on the patient’s medical history, physical examination, and family and close contact history. Scabies’ classic symptoms include acute, widespread itching that typically spares the head and face. At night, pruritus is more severe. The majority of the lesions are found in the finger webs , the flexor surfaces of the wrists, the elbows, the axillae, the buttocks and genitaliafingel, and the female breasts . Most sites have inflammatory, itchy papules. Scabies-specific nodules (usually in the axillae and vaginal areas) and burrows may be absent. Excoriations, eczematization and impetiginization are examples of nonspecific secondary lesions that can appear anywhere.
According to a report from a sub-Saharan area with a high (13%) prevalence of Scabies, the diagnosis had 100% sensitivity and 97% specificity when diffuse itching and visible lesions were linked to either at least two typical scabies locations or a household member who was itching. (69) There is a dearth of such data from regions where scabies is less common. Scabies
Occasionally, scabies manifests in atypical forms (70) that are more challenging to detect than the classic forms, perhaps increasing the likelihood of outbreaks. The face, scalp, palms, and soles are frequently affected by atypical presentations in babies. Elderly people have atypical papular scabies, immunocompromised individuals have localized or generalized crusted scabies, and patients with superinfected scabies have impetigo
Diagnostic Test:
The detection of mites, eggs, eggshell pieces, or mite pellets is necessary for a definitive diagnosis. In order to collect multiple superficial skin samples from distinctive lesions, such as burrows or papules and vesicles in the burrow site, a blade should be scraped laterally across the skin, being careful not to cause bleeding. A light microscope operating at low power can be used to examine the specimens Since potassium hydroxide dissolves mite pellets, it should not be utilized. This method is very operator dependant becausee there are few mites in cases of typical scabies. Scabies is not always ruled out when mites are not found.
A skin biopsy may be used to confirm the diagnosis In unusual circumstances or when direct examination is impossible. However, mites or other diagnostic findings are frequently absent, and histologic examination typically reveals a nonspecific, delayed hypersensitivity reaction.(71) Despite the relatively low sensitivity of diagnostic testing, empirical treatment is not recommended for patients with generalized itching and should be reserved for patients with a history of exposure, a typical eruption, or both.
(FIG.6) Dermoscopic image of a scabies burrow
Regardless of the presence of symptoms, infected individuals and their close physical contacts should receive treatment concurrently. Although there aren’t many thorough trials to support their use, topical or oral medications may be employed. The dosages and adverse effects of typical scabies treatments are compiled
Topical
The two topical scabies therapies that have been explored the most are lindane and permethrin. Permethrin, administered as a single nighttime application, was shown to be more successful than lindane in a Cochrane meta-analysis of four randomized trials comparing these treatments (odds ratio for clinical failure, 0.66; 95 percent confidence interval, 0.46 to 0.95).(72, 73 )Nonetheless, the meta-analysis revealed significant variation in the results across the trials. Clinical cure rates did not differ in the largest experiment; at an average of 28 days following therapy, 181 out of 199 patients treated with permethrin (91 percent) and 176 out of 205 patients treated with lindane (86 percent) had achieved complete resolution.(74)
However, lindane’s use has been restricted because to its potential neurotoxicity, particularly with repeated applications (75); the product is no longer available in Australia or the United Kingdom. The likelihood of negative effects from using 5 percent permethrin cream was shown to be at least 40 times lower than that of using 1 percent lindane lotion in an in vitro model evaluating systemic exposure under overuse setpatient (76) In a 1996 study, doctors noted a modest rate of central nervous system side effects in patients (1 per 500,000 U of disseminated permethrin), with no significant events. (77) The Centers for Disease Control and Prevention (CDC) recommend 5 percent permethrin as a first-line topical treatment for scabies, even though it is more expensive than litreatme (78) In areas where scabies is endemic, mass treatment with permethrin has also been successful in reducing the disease.
Crotamiton and benzyl benzoate, which are not accessible in the US, are further topical therapies. The cure rate at three weeks was 51% (19 of 37 patients) with 10% benzyl benzoate in a randomized trial conducted in Vanuatu, in the South Pacific, where scabies is a significant public health issue. This is comparable to the cure rate of 56% with a single oral dose of ivermectin of 200 µg per kilogram of body weight.(79) However, compared to 7% of patients treated with oral ivermectin, a third of patients treated with benzyl benzoate felt burning or stinging. Based mostly on professional experience, benzyl benzoate is regardedas the first-line local treatment in France, where permethrin is unavailable. The Cochrane Review came to the conclusion that there was not enough information to compare the efficacy of lindane or permethrin with either benzyl benzoate or crotamiton.(8) Crotamiton appears to be substantially less effective than permethrin at four weeks, according to scant data from a randomized trial (61 percent vs. 89 percent).(80)
Scabies has also been treated with pyrethrin as an aerosol spray, such as allethrin. However, two asthmatic girls with head lice experienced acute bronchospasm as a result of this treatment, and one of them died. People with a history of asthma should never be provided such a formulation of pyrethrin.(81) There is insufficient evidence to support the use of sulfur, topical ivermectin, and tea tree oil (82) as therapies.
Oral
Some individuals may not tolerate topical treatments well (e.g., they are messy, may be difficult to apply, and may cause burning or stinging, especially when the skin is excoriated or eczematous, and potential percutaneous absorption may offer a concern). Oral ivermectin (83) is a different strategy that has been widely utilized to treat a number of parasitic illnesses, such as lymphatic filariasis, onchocerciasis, and other nematode-related infestations. It is believed that ivermectin paralyzes and kills parasites by blocking glutamate-induced and {gamma}-aminobutyric acid-induced neurotransmission.Twenty Ivermectin does not pass across the intact blood-brain barrier (84) in humans, but it has been shown to cause central nervous system toxicity and abrupt death in collies.(85)
The effectiveness of a single dose of Ivermectin (200 µg per kilogram) for the treatment of scabies has been evaluated in a number of controlled trials. 37 out of 50 patients treated with ivermectin (74%) were cured in one placebo-controlled experiment, compared to 4 out of 26 patients in the placebo group (15%).(86) Ivermectin and 10% benzyl benzoate (15) or ivermectin and lindane did not significantly differ in clinical cure rates in short investigations.(87) A single ivermectin dose cured 70% of patients in a randomized trial comparing oral ivermectin with an overnight application of 5% perivermect (88), compared to a 98% cure rate with permethrin (P<0.003). However, a second ivermectin dose administered two weeks later increased the cure rate to 95%. Ivermectin’s lack of ovicidal activity may be the cause of its reduced efficacy when taken in a single dose.
Clinical experience and randomized trials have indicated that ivermectin is safe. Patients treated with this medication who had onchocerciasis and a high Loa loa microfilariae infection have been documented to experience encephalopathy. (89) A widespread ivermectin treatment program for children with scabies in the Solomon Islands showed no significant side effects. (90) Elderly patients who got ivermectin for scabies (91) were shown to have an increased risk of death in one study, but selection bias and confounding factors could be the cause. Other investigations, particularly those including nursing home residents, have not supported this finding.(92)
Although ivermectin may be used as first-line treatment, topical treatments may be a better option due to its greater cost in some nations. Ivermectin should be the first line of treatment for patients who do not respond to topical scabicides. It may also be the best option for older patients, those with generalized eczema, and other patients who might not be able to tolerate or adhere to topical medication.
Assessing the response
Patients should be informed that following the conclusion of properly administered scabicide medication, itching may continue for up to four weeks. The reason for the itching should then be looked into again.
Control of Infectivity
The most typical way that classic scabies is spread is through prolonged skin-to-skin contact with an infected individual. Treatment should be given to people who have this kind of contact but not to those who have more casual touch. All members of the home and any sexual encounters should have prescriptions, even if they don’t exhibit any symptoms. There is considerable worry that patients treated with ivermectin may stay contagious longer than those treated with topical treatments, however the time course for the eradication of parasites following therapy for classic scabies has not been thoroughly investigated.
Crusted scabies is very contagious, and treatment of anyone who has been even slightly exposed is advised. Patient care professionals and support staff (e.g., cleaning and laundry employees) in institutional settings should be regarded to have been exposed to infected individuals.
Classic scabies seldom spreads without direct person-to-person contact. However, the recovery of live mites from chairs and couches in scabies patients’ homes supports the adoption of environmental measures,(93 )despite a lack of data to prove their usefulness in preventing transmission. Ideally, garments and bed linens should be machine washed at 60°C and machine dried the day after the initial treatment (94); insecticide powder or aerosolized insecticide is typically kept for things that cannot be laundered. Items can also be kept in a sealed plastic bag for at least 48-72 hours. Only clothes and linens that came into contact with the patient during the last 48 to 72 hours should be cleaned, based on mite survival rate
Aloe barbadensis mill
Barbadensis Mill, a member of the Liliaceae family, is native to Eastern and Southern Africa but has spread to China, North Africa, the Mediterranean, the West Indies, and the Middle East. Hamdard Laboratories Waqf Pakistan manufactures Aloe barbadensis Mill under the brand name Baarasil. The chemical ingredient is Aloe barbadensis mill. Aloe vera gel can treat a variety of medical issues, including insect stings, eczema, bites, wound healing, acne, skin care, bruising, pruritus, and allergies. The drug is provided in syrup form, with a recommended dosage of 5 tsp thrice daily (Mantle, Gok, & Lennard, 2001).(95)
Rosmarinus officinalis
R. officinalis is utilized as a therapeutic herb around the world. This plant includes active compounds including 8-cineole and camphor. It possesses anti-inflammatory, antibacterial, and astringent properties that aid in treating scabies condition. Rosemary oil kills mites and quickly heals wounds and bruises. However, it is not recommended for internal usage (Chen et al., 2006; Issabeagloo et al., 2012).(96)
Cinnamomum camphor
This tree has been used for years to treat scabies effectively. C. camphor is a fragrant shrub that also has analgesic properties. This tree has insecticidal properties, which may have therapeutic benefits. It is beneficial in the treatment of muscle discomfort. Using the oil of this tree for 10 days will completely cure scabies illness.(97)
CONCLUSION:
Scabies remains a major global health concern, especially among overcrowded, resource-limited, and immunocompromised communities. Understanding the biology, transmission, and clinical variants of Sarcoptes scabiei is critical for accurate diagnosis and treatment. Although classic scabies is distinguished by distinctive itching and burrows, various atypical variants can delay diagnosis and raise the risk of outbreaks.
Accurate diagnosis is based on a thorough clinical examination accompanied by dermoscopy or microscopic identification of mites. Effective care necessitates the simultaneous treatment of infected persons and close contacts with both topical treatments such as 5% permethrin and systemic therapy such as oral ivermectin in appropriate instances. Prevention techniques, such as maintaining good personal hygiene, decreasing overcrowding, and properly cleaning linens and clothing, are essential for interrupting the transmission cycle. Early detection, adequate treatment, and community-level control strategies remain the cornerstones of decreasing morbidity and preventing recurrent or crusted scabies, which pose a significant risk of consequences. Continued awareness and education are critical to limiting the spread of this extremely contagious but totally treatable disease.
REFERENCES



Sneha Chavan*, Shital Rathod, Sabafarin Shaikh, Diagnosis, Prevention and Treatment of Scabies, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 1317-1334 https://doi.org/10.5281/zenodo.17852458
 10.5281/zenodo.17852458
10.5281/zenodo.17852458
