1,3,7,8,10 Rungta Institute of Pharmaceutical Sciences
2,4,5,6,9 Rungta Institute of Pharmaceutical Sciences and Research
Famotidine is a histamine H2 receptor antagonist that is widely used in the treatment of acid related gastrointestinal disorders such as peptic ulcer disease, gastroesophageal reflux disease (GERD), and Zollinger Ellison syndrome. However, the drug has certain pharmacokinetic limitation including relatively low oral bioavailability and a short biological half-life, which require frequent dosing to maintain therapeutic drugs levels in the body. These limitations may reduce patient compliance and therapeutic effectiveness. To overcome these problems, the development of sustained release drug delivery systems has gained considerable attention in pharmaceutical research. The present study focuses on the formulation and evaluation of sustained release matrix tablets of famotidine using hydroxypropyl methyl cellulose (HPMC) as a rate controlling polymers. Sustained release matrix tablets are designed to release the drug gradually over an extended period, thereby maintaining a constant therapeutic concentration in the bloodstream and reducing the need for frequent administration. HPMC is widely used in matrix tablet formulations due to its excellent swelling gel forming and drug release controlling properties.In this formulation approach, the matrix tablets are generally prepared using suitable methods such as direct compression or wet granulation, where famotidine is uniformly dispersed within the polymer matrix. Various concentration of HPMC is incorporated in the formulation to regulate the drug release rate. When the tablet comes into contact with gastrointestinal fluids, the polymer swells and forms a gel layer around the tablet. This gel barrier controls the diffusion of the drug from the matrix system, resulting in a prolonged and controlled drug release. The prepared matrix tablets are evaluated using several pre-compression and post-compression parameters to ensure their quality and performance. Pre-compression study includes parameters such as Bulk density, tapped density, Carr’s index, Hausner’s ratio, and angle of repose to assess the flow propertiesof the powder blend. Post -compression evaluation involves testing parameters such as hardness, friability, weight variation, thickness, drug content uniformity, and in-vitro dissolution studies. The dissolution studies help to determine the rate and pattern of drug release from the matrix tablet and confirm the sustained release behavior of the formulation. The development of sustained release matrix tablet of famotidine using HPMC offers several advantages, including prolonged drug release, improved therapeutic efficacy, reducing dosing frequency, and better patient compliance. Therefore, such formulations can be considered an effective approach for the controlled delivery of famotidine in the management of acid related gastrointestinal disorders
Oral drug delivery systems remain in the most widely used and preferred route of drug administration due to their convenience, safety and patient compliance. Among the various oral dosage forms, tablets are the most commonly used because they are easy to manufacture, stable, and allow accurate dosing. However, many conventional tablets release the drug rapidly after administration, which can lead to fluctuations in drug concentration in the body. These fluctuations may cause reduced therapeutic effectiveness and sometimes unwanted side effects. To overcome these limitations, modified or controlled drug delivery systems have been developed1. Sustained release drug delivery systems are designed to release the drug slowly over an extended period of time, thereby maintaining a relatively constant drug concentration in the bloodstream. Such systems help in reducing the frequency of drug administrations, improving patient compliance, and minimizing side effects associated with sudden peaks in drug levels. Sustained release formulations are especially beneficial for drugs that have a short biological half-life and require frequent dosing to maintain their therapeutic effect. Matrix tablets are one of the most commonly used approaches for developing sustained release formulations. In these systems, the drug is uniformly dispersed within a polymer matrix that controls the rate of drug release. The release of the drug from the matrix occurs through mechanisms such as diffusion, dissolution, and erosion of the polymer. Matrix systems are widely preferred because they are simple to formulate, cost-effective, and suitable for large-scale manufacturing1,2. Among the various polymers used in sustained release formulations, hydrophilic polymers have gained significant attention due to their safety, biocompatibility, and ability to control drug release effectively. One such polymer is Hydroxypropyl Methylcellulose (HPMC), which is widely used in pharmaceutical formulations. HPMC is a semi-synthetic, ono-ionic cellulose ether that forms a gel layer when it comes into contact with aqueous fluids. This gel layer acts as a barrier that controls the penetration of water into the tablet and the diffusion of the drug from the matrix. As the outer layer of the tablet hydrates and swells, the drug gradually diffuses out, providing a sustained release effect over a n extended period. Famotidine is a histamine H2 receptor antagonist that is commonly used in the treatment of various acid related gastrointestinal disorders such as peptic ulcers, gastroesophageal reflux disease (GERD), and Zollinger Ellison syndrome. It works by inhibiting the action of histamine on H2 receptors located on gastric parietal cells, thereby reducing the secretion of gastric acid. Although famotidine is effective in managing these conditions, it has a relatively short elimination half-life, frequent dosing is often required to maintain effective therapeutic levels in the body2.
Drug Profile- Famotidine
Famotidine is a histamine H2 receptor antagonist that is widely used for the treatment of acid -related gastrointestinal disorders. It is commonly prescribed for conditions such as gastric ulcers, duodenal ulcers, Zollinger-Ellison syndrome, and gastroesophageal reflux disease (GERD). The drug reduces gastric acid secretion and helps in healing ulcers and relieving symptoms caused by excess stomach acid.In the treatment of benign gastric and duodenal ulcers, famotidine is generally administered orally at a dose of 40 mg once daily at bedtime for about 4-8 weeks. For the management of GERD, the usual recommended dose is 20 mg taken orally twice daily for 6-12 weeks.Famotidine shows incomplete absorption from the gastrointestinal tract, resulting in a relatively low oral bioavailability of about 40-45%. Additionally, the drug has a short biological half-life pf approximately2.5-3.5 hours. Due to these pharmacokinetic limitations, famotidine often requires multiple daily dosing. Therefore, developing a sustained- release formulation can help maintain therapeutic drug levels for a longer period and improve patient compliance3.Pharmacologically, famotidine acts as a competitive antagonist of histamine H2 receptors located on gastric parietal cells. By blocking these receptors, it inhibits the stimulation of acid secretion in the stomach. This property makes famotidine effective in treating disorders associated with excessive gastric acid production.Compared with other H2 receptor antagonists, famotidine shows high selectivity and potency for the H2 receptor. Studies involving healthy volunteers and patients with acid-hypersecretory conditions have shown that famotidine is 20-50 times more potent than cimetidine and approximately eight times more potent than ranitidine in reducing gastric acid secretion3.Famotidine is widely available and used both as a prescription medicine and as an over-the-counter drug. While oral formulations are most commonly used, intravenous preparations are also available for use in hospital settings when oral administrations are not possible.The drug belongs to a class of medications known as H2- blockers, which work by reducing the amount of acid produced by the stomach. This helps in relieving symptoms such as heartburn, acid reflux, and ulcer pain4.
Figure 1.1: Structure of Famotidine
Famotidine is available in several dosage forms, including3,4:
Tablets:
Powder for oral suspension
These formulations allow flexibility in dosing and make the medication suitable for both adult and pediatric patients.
Generic Name: Famotidine
Brand Name:
Duexis, Duo Fusion, Fluxid, Good Sense Acid Reducer, Pepcid, Pepcid Complete, Zantac Reformulated Aug 2022
Chemical Formula: C8H15N7O2S3
IUPAC Name: [{(2- [(diamino methylidene) amino]-1,3-thiazol-4-yl} methyl) sulfanyl]-N-sulfamoylpropanimidamide
Molecular Weight: 337.5 g/mol
Density: Famotidine Powder Density: 1.838 g/cm
Melting Point: 163.5
Boiling Point: 662.383 at 760mmHg
Colour: White to Pale Yellow Crystals
Taste: Bitter Taste
Odour: Odorless
State: Solid Crystals
Solubility: 1000mg/L
Freely soluble in glacial acetic acid, slightly soluble in methanol, very slightly soluble in water, and practically insoluble in ethanol.
Solubility in water: 0.1% (w/v) at 293k
Mechanism of Action:
Famotidine works by inhibiting histamine-2 (H2) receptors present on the gastric parietal cells in the stomach. Normally, histamine stimulates these cells to produce gastric acid. By competitively blocking these receptors, famotidine reduces the secretion of gastric acid.As a result, the drug decreases both actually both the acidity and the total volume of gastric secretions. It is effective in reducing basal and nighttime acid secretion and also lowers acid production stimulated by food, caffeine, insulin and pentagastrin4,5,6.
Pharmacokinetics
Absorption:
After oral administration, famotidine has a bioavailability of about 40-45%. The drug usually begins to act within 1 hour, and its maximum effect is seen in 1-3 hours. When given intravenously, the peak effect occurs in about 30 minutes. The acid-suppressing effect generally lasts 10-12hours.
Distribution:
Famotidine shows low plasma protein binding (15-20%) and has a small volume of distribution (about 1.0-1.3 L/kg)7.
Metabolism:
Only a small amount of famotidine undergoes metabolism in the liver. It is mainly metabolized by the cytochrome P450 enzyme system, particularly CYP1A28.
Elimination:
The elimination half-life of famotidine is about 2.5-3.5 hours. Around 65-70% of the drug is excreted unchanged in urine. In patients with severe kidney problems, the half-life can increase to more than 20 hours, so the dose must be adjusted. Children with chronic kidney disease may also show changes in famotidine pharmacokinetics9.
Administration:
Dosage Forms and Strengths
Famotidine is available in several dosage forms such as tablets, oral suspensions and intravenous solution. Tablets are commonly available in 10 mg, 20 mg, and 40mg strengths.
The IV formulation can be given either as a slow injection over at least 2 minutes or as an infusion for 15-30 minutes. The oral suspension should be shaken well before use, while tablets can be taken with or without food10.Over-the-counter (OTC) famotidine is available as tablets, chewable tablets, and gel capsules in 10 mg or 20 mg strengths. These tablets should be taken 10-60 minutes before foods or drinks that may cause heartburn, and they should not be used for more than two weeks unless advised by a doctor.A combination product containing famotidine, calcium carbonate, and magnesium hydroxide is also available11.
Adult Dosage:
Duodenal ulcer (active):
40 mg orally at bedtime for upto 8 weeks, or 20 mg twice daily.
Maintenance therapy for duodenal ulcer:
20 mg once daily at bedtime.
Gastric ulcer:
40 mg once daily at bedtime for up to 8 weeks.
Non-erosive GERD:
20 mg twice daily for up to 6 weeks.
GERD with erosive esophagitis:
20-40 mg twice daily for up to 12 weeks.
Hypersecretory conditions:
20-60 mg every 6 hours, starting with 20 mg every 6 hours.
Special Populations
Renal impairment:
Dose reduction is required because the drug is mainly eliminated through the kidneys13.
Pregnancy:
Famotidine can cross the placenta. It may be used during pregnancy if the benefits outweigh the risks, especially when lifestyle changes and antacids do not control symptoms13,14.
Breastfeeding:
Small amount of famotidine can pass into breast milk, but available evidence suggests it is unlikely to cause harm to the infant15.
Older adults:
Lower doses are recommended if kidney function is reduced16.
Pediatric patients:
The usual dose is 1 mg/kg per day divided into two doses17,18.
Adverse Effects:
Famotidine is generally well tolerated. Some common side effects include:
Headache, Dizziness, Diarrhea, Constipation
Agitation (more common in infants)
Intravenous administration may sometimes cause local irritation at the injection site. Rarely, famotidine may cause thrombocytopenia (low platelet count), which requires discontinuation of the drug19,20,21,22.
Drug Interactions:
Famotidine has minimal effects on liver enzymes, so it usually causes few drug interactions. However, it can reduce the absorption of some medications that require stomach acid for proper absorption. It should not be used with drugs such as cefuroxime, dasatinib, delavirdine, neratinib, pazopanib, and risedronate.
It may also increase the levels of tizanidine, so these two drugs should generally not be used together23,24.
Contraindications:
Famotidine should not be used in patients who have allergy or hypersensitivity to famotidine or other H2 receptor antagonists such as cimetidine25.
OTC famotidine should also not be used by patients who have26,27:
Monitoring:
Since famotidine is mainly eliminated through the kidneys, renal function should be monitored, especially in older patients. In cases of gastrointestinal bleeding, healthcare providers may also monitor complete blood count and gastric ph.
Toxicity:
Famotidine is mainly eliminated from the body through the kidneys. Therefore, patients with impaired renal function may have a higher risk of drug accumulation and toxicity. For this reason, dose adjustment is necessary in individuals with moderate to severe renal impairment to prevent excessive drug levels in the body.Clinical information from the famotidine package insert indicates that oral doses as high as 640 mg per day, which are significantly higher than the approved therapeutic doses, have been administered to patients with severe acid-hypersecretory conditions. Interestingly, these high doses did not produce any serios adverse effects. In most reported cases, symptoms of drug overdose were similar to the usual side effects observed during normal therapeutic use7,28.Management of famotidine overdose generally involves removing any unabsorbed drug from the gastrointestinal tract, closely monitoring the patient, and providing supportive treatment when required.Famotidine is classified as a pregnancy category B drug, which means that studies have not shown significant risk to the fetus, but the medication should still be used during pregnancy only when the expected benefits outweigh potential risks.The drug can also be excreted in breast milk. Therefore, when prescribing famotidine to breastfeeding mothers, healthcare providers should carefully consider the benefits to the mother and the possible effects on the infant. Compared with other H2 receptor antagonists, famotidine is found in lower concentrations in breast milk, which may make it a relatively safer option for use during breastfeeding14,29.
Effervescent Floating Drug Delivery System (FDDS):
Effervescent floating drug delivery systems are designed to remain floating in the stomach for a prolonged period, which helps in controlled drug release. These systems contain a floating chamber filled with air, water, vacuum, or inert gas, which reduces the density of the dosage form and allows it to float on gastric fluid.In this system, carbon dioxide (CO2) gas is produced through an effervescent reaction between organic acids such as citric acid and carbonate or bicarbonate salts. The generated gas becomes trapped within the structure of the dosage form, which helps the tablet float in the stomach31. Effervescent FDDS are usually prepared using swellable polymers such as methylcellulose, chitosan, or similar hydrocolloid polymers. These polymers swells when they come in contact with gastric fluid and form a gel-like matrix. Along with these polymers, effervescent agents such as sodium bicarbonate, citric acid, and tartaric acid are incorporated into the formulation. When the dosage form reaches the acidic environment of the stomach, the effervescent components react and release carbon dioxide gas. The gas becomes trapped within the swollen hydrocolloid matrix, decreasing the density of the system. As a result, the dosage form remains buoyant in the gastric fluids, allowing the drug to be released slowly over an extended period for use during breastfeeding32.
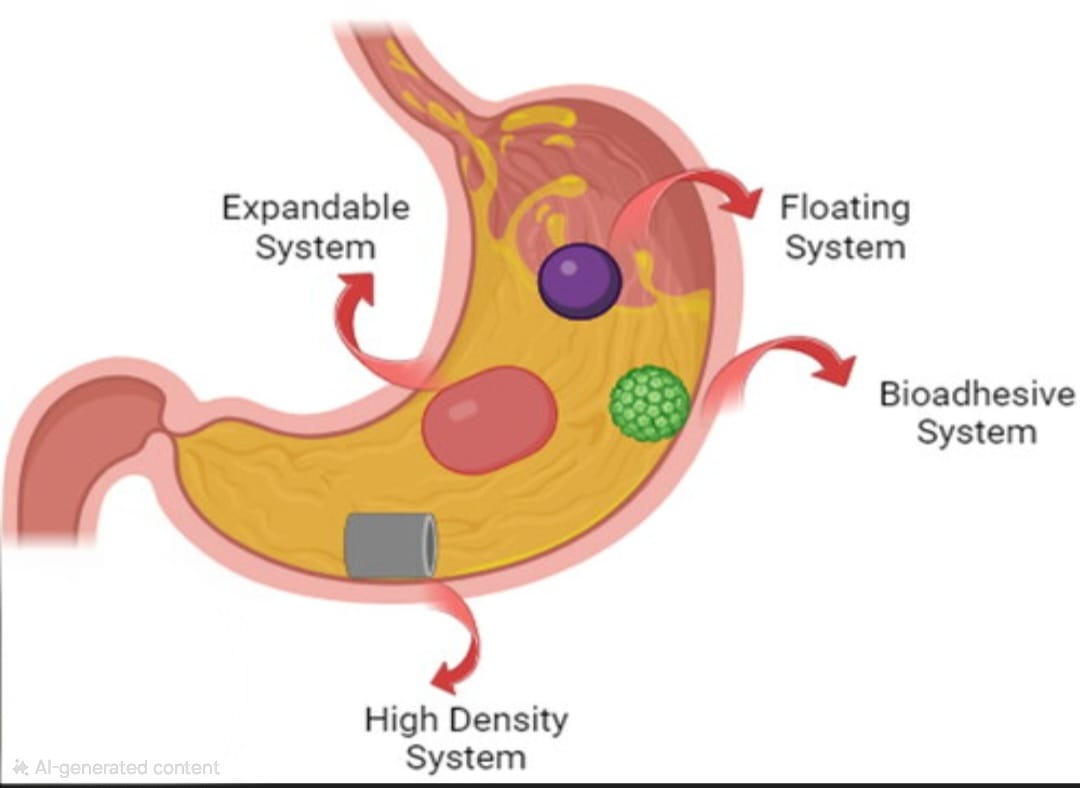
Figure 1.2: GRDDS based on effervescence
Gas Generating System:
This buoyant delivery system uses effervescence reaction between citric acid/ tartaric acid and carbonate/bicarbonate salts to release CO2 which further reduces its specific gravity and makes it float over chime.Low density FDDS is based on the release of CO2 upon contact with gastric fluids after oral administration. The materials are formulated in such a way that after entering in the stomach, CO2 is liberated due to reaction with acidic gastric content and which get entrapped in the gel-based hydrocolloid. It produces an upward motion of the dosage forms and maintains its buoyancy. Ultimately it causes a decrease in specific gravity of dosage form and hence resulting into a float on the chime. The CO2 generating components are mixed within the tablet matrix in a single layer or multi-layered form to produce gas generating mechanism in hydrocolloid layer, and the drug in the other layer results into a sustained release effect33.
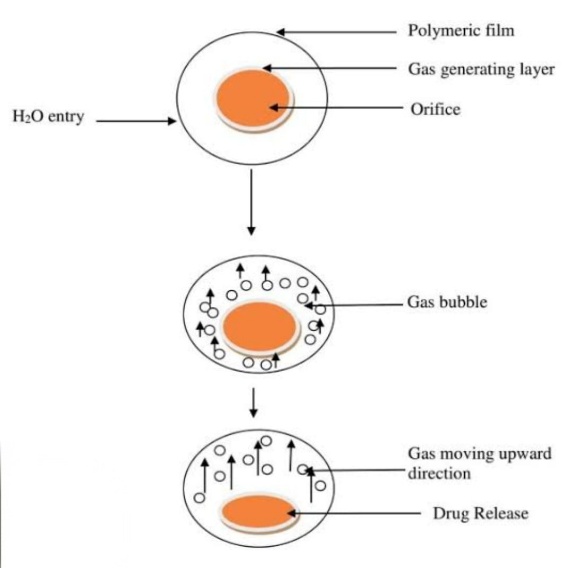
Figure 1.3: Mechanism of floatation via CO2 liberation
CONCLUSION
The formulation of sustained release matrix tablets of famotidine using hydroxypropyl methylcellulose (HPMC) represents an effective strategy for improving the drug’s therapeutic performance. Since famotidine has a relatively short half-life and moderate bioavailability, conventional dosage forms may require frequent dosing. Incorporating the drug into a polymetric matrix system helps to slow down the drug release rate, allowing the medication to be delivered gradually over an extended period. HPMC acts as a suitable release-controlling polymer because of its swelling and gel-forming properties, which regulate the diffusion of the drug from the matrix. Based on various studies and evaluation, HPMC-based matrix tablets can successfully provide controlled and prolonged drug release while maintaining acceptable tablet quality parameters. This type of sustained release formulation helps reduce dosing frequency, improve patient convenience, and enhance overall treatment effectiveness. Therefore, sustained release matrix tablets of famotidine prepared with HPMC offer a promising approach for the effective management of acid-related gastrointestinal disorders.
REFERENCES

Tannu Sahu, Rohit Singh, Sushmita Pradhan, Khemchand Sahu, Santosh Singh, Razi Ahmed, Nutan Sahu, Suchita Wamankar, Dr. Gyanesh Kumar Sahu, Dr. Chanchal Deep Kaur, Development and Evaluation of Gastroretentive sustained release system of Famotidine using HPMC, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 3368-3377, https://doi.org/10.5281/zenodo.19234909
 10.5281/zenodo.19234909
10.5281/zenodo.19234909
