Krishnarao Bhegade Institute of Pharmaceutical Education and Research, Talegaon Dabhade, Pune, Maharashtra, India.
Acne vulgaris is a common, chronic inflammatory disorder of the pilosebaceous unit, primarily affecting the face, upper arms, trunk, and back. While predominantly observed in adolescents, it is not restricted to this age group and can persist into adulthood. The condition ranges in severity from mild comedones to severe, disfiguring inflammatory lesions that may cause scarring and psychological distress. The text distinguishes acne vulgaris from Acne Rosacea, a chronic condition usually affecting adults (ages 30-50) characterized by facial redness and the absence of comedones. The therapeutic role of herbal and natural ingredients in acne management. It details a wide array of botanicals-such as Neem, Turmeric, and Aloe Vera-along with natural oils and excipients that possess critical antibacterial, anti-inflammatory, and antioxidant properties, offering a natural pharmacological approach to treatment.
Acne vulgaris is a com is mon cutaneous inflammatory disorder of the pilosebaceous unit, which runs a chronic course. The condition commonly manifests with papules, pustules, or nodules primarily on the face, although it can also affect the upper arms, trunk, and back. The pathogenesis of acne vulgaris involves the interaction of multiple factors that ultimately lead to the formation of its primary lesion, which is known as “comedo” Although acne vulgaris is commonly observed among adolescents, it is not restricted to this age group and can affect individuals of various ages. The severity of this condition can vary, ranging from a mild presentation with only a few comedones to more severe forms characterized by disfiguring inflammatory manifestations, which can lead to hyperpigmentation, scarring, and adverse psychological effects. [1,2]
Types of acne vulgaris
It is a skin disease of adults often affected by women in which blood vessels of the face enlarge indicating a flushed appearance. Rosacea is a common, chronic, incurable, adult acne-like skin condition that is easily controllable and curable medically. Rosacea usually acts upon the central third of the face, especially the nose with periodic aggravation and relief. The symptoms may come and go and the skin may be clear for weeks, months, or years and then may emerge time and again. Rosacea inclind to develop in certain stages and causes to create inflammation of the skin of the face, especially the forehead, cheeks, nose, as well as chin. Symptoms and signs of rosacea are: Redness of the face, tiny red pimples and fine red lines on the facial skin . An enlarged, bulbous red nose. Eye problems, like swollen, Red eyelids and conjunctivitis.[3]
The most common form of acne; usually affects people from puberty to young adult. Acne vulgaris is a general skin condition characterized by the development of seborrhea, comedones, nodules, papules, pustules and cyst. It comes in the areas of the skin with plentiful hair growth such as in the upper chest, back, legs and face, Sebaceous glands get infected and clogged. Development of several large and small eruptions.Hickey, pimple, zit:
A small inflamed elevation of the skin; a pustule or papules which are common symptoms in acne. Difference between a pimple and acne Unlike common Acne, rosacea is not primarily a disease of teenagers but occurs most often in adults (ages 30-50), especially in those with fair skin. Different than acne, there are usually no blackheads or whiteheads in rosacea. Certain people get one or two spots off and on while others get frequent eruption of spots with lots of pus-filled pimples indicates acne which is a chronic or prolonged condition that affects many teens and adults. More or less all human beings in the world gets pimples at some point of time sooner the body enter into puberty stage at the age of 12, there commence to release hormones and start to function in the bodies of man or woman irrespectively and at this juncture food or pollution, ought to upset hormonal balance thereafter. [4,5]
Pimples or spots come out when the skin produces much more oil, causes breeding bacteria which clog the existing pores creating swelling and redness on the skin. Pimples are not at all contagious. Out of various kinds of
Six types of pimples:
Acne can be found anywhere on your body. Commonly it develops on the face, back, neck, chest, and shoulders. If you have acne, you will typically notice pimples that are white or black in appearance. Both blackheads and white heads are known as come downs. Black heads open at the surface of the skin giving them black appearance. White heads are closed just under the surface of the skin, giving them a white appearance. While whiteheads and blackheads are the most common types of acne, other lesions can occur. Inflammatory lesions namely papules, pustules, nodules and cysts are more likely to create scarring of the skin.
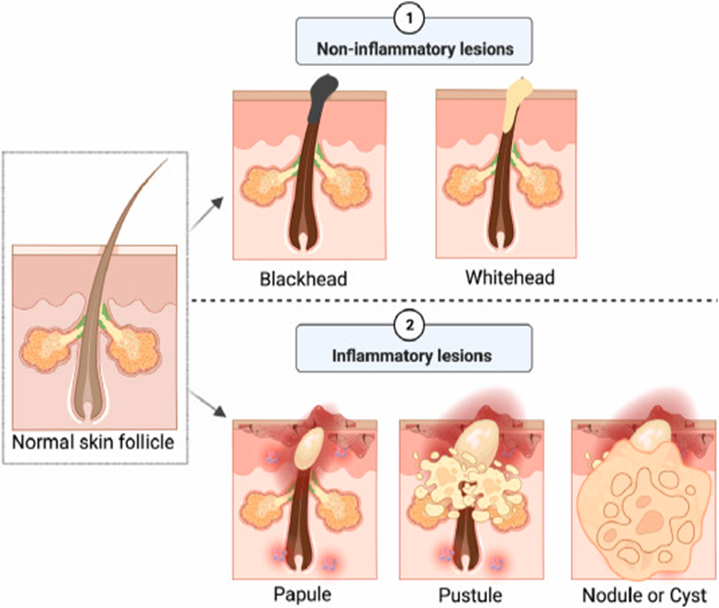
Fig.1 Type of acne vulgaris [15]
5.Pathogenesis of Acne Vulgaris/pathophysiology:
Acne is a disease of pilosebaceous glands. Multiple factors are responsible for pathogenesis of acne as sebum, abnormal follicular differentiation, hormones, Propionibacterium acne, inflammation and nutrition. Hormones: Androgens have only the priming role in acne development as they (testosterone and dehydrotestosterone) stimulate proliferation and differentiation of sebocytes and infundibular keratinocytes during puberty. Increased dehydrotestosterone (DHT) may lead to hyperkeratinisation by their action on infundibular keratinocytes.
The hyperkeratinisation In follicular infundibulum and sebaceous duct is one of the most crucial events in the development of acne lesions. Sebum: Sebum is the lipid-rich secretion product of sebaceous gland, secreted by sebocytes which along with keratinocytes may act as immune cells of the skin. The severity of acne is directly proportional to the sebum production 16. The secretion of sebum increases due to enlargement of sebaceous glands under the stimulatory action of androgens. The sebum of acne patients is characterized by the presence of lipoperoxides due to peroxidation of squalene and diminished levels of sebum antioxidant vitamin E.
Abnormal follicular epithelial differentiation-It marks the most primary change in the pilosebaceous unit in acne patients. Desquamated cornified cells of upper canal of the follicle become abnormally adherent; instead of undergoing the normal process of shedding and discharge through follicular orifice, these cells form a retained, microscopic hyperkeratotic plug (the microcomedo) in follicular canal. This process called comedogenesis. The progressive enlargement of microcomedo give rise to clinically visible comedo which can be open comedo/ black heads (appearing flat or slightly raised and distend from follicular orifice), have black color due to oxidation of melanin pigment, or as closed comedo/white heads, having closed overlying surface Bacteria-Propionibacterium acne is an anaerobic obligate diptheroid that resides beneath the surface of human skin. And populates the androgen stimulated sebaceous follicles. The oxidative stress within the pilosebaceous unit changes the environment from aerobic to anaerobic which is the best suited for this gram positive bacterium. It causes inflammatory acne 18. Staphylococcus epidermis is also the resident of human skin flora and is the aerobic organism associated with superficial infections within the sebaceous units. This sequence of events occurs in development of acne shown in figure 1 and 2.[4-6]
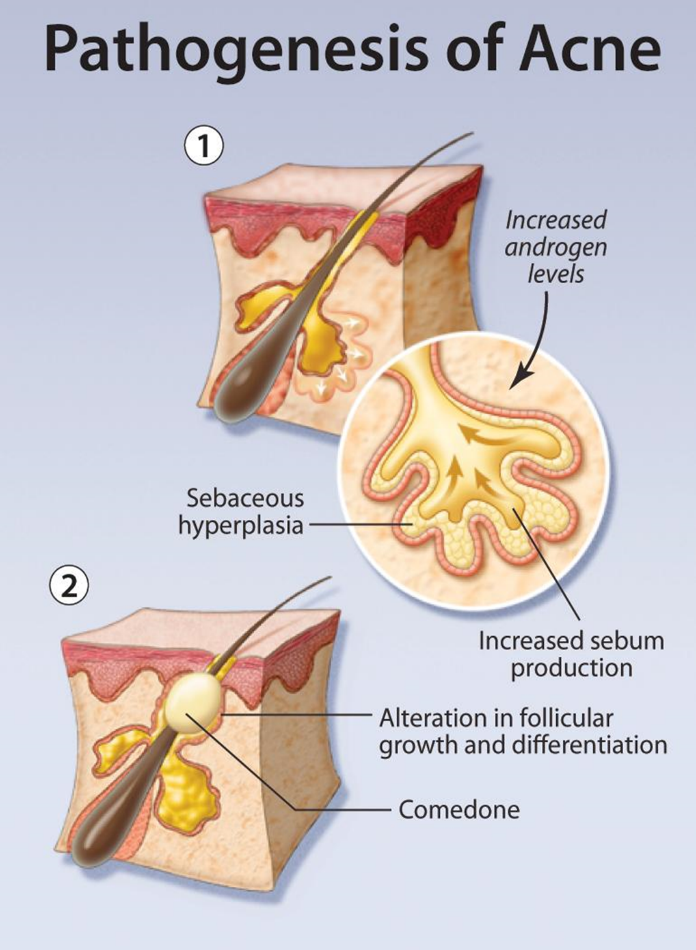
Fig.2pathogenesis of acne [16]
Etiology:
Acne develops as a result of hypersensitivity of the sebaceous glands to normal levels of circulating androgens. This process is further exacerbated by the presence of Cutibacterium acnes (C acnes), a bacterial species, and subsequent inflammation.
Proposed contributory factors for acne include:
Pathophysiology:
The pathogenesis of acne vulgaris involves the interaction of several host factors, including the stimulation of sebaceous glands by circulating androgens, dysbiosis of the pilosebaceous follicle microbiome, and cellular immune responses. In addition, other factors such as genetics and diet may also influence the development and progression of the disease. The microcomedo serves as the primary lesion and is the precursor for all clinical manifestations of acne vulgaris. It is characterized by a small, hyperkeratotic plug primarily composed of corneocytes and located in the lower region of the follicular infundibulum. Microcomedones gradually evolve and develop into other acne lesions, which include closed comedones (whiteheads), open comedones (blackheads), and inflammatory papules, pustules, and nodules. The progression of microcomedones into other types of acne lesions has been theorized to involve the following 4 primary pathogenic events:
The gradual accumulation of keratinous material and sebum converts a micro comedo into a closed comedo. Through continuous distension, the follicular orifice gradually expands, resulting in the formation of an open comedo. Oxidized lipids and melanin within the comedo contribute to its characteristic dark black color. C acnes and its antagonizing cellular immune responses contribute to the development of inflammatory pustules and papules. Eventually, follicles rupture with the release of bacteria, keratin, and proinflammatory lipids into the surrounding dermis, exacerbating the inflammation with subsequent nodule formation.[10]
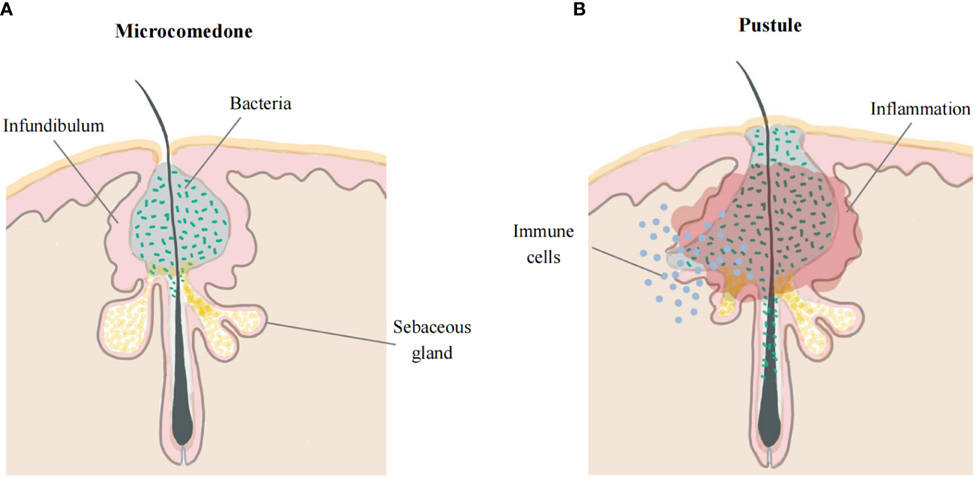
Fig.3 pathophysiology of acne vulgaris [17]
Role of Androgens:
Most patients with acne vulgaris typically have normal androgen levels in their body. However, in certain conditions such as congenital adrenal hyperplasia, polycystic ovarian syndrome, and adrenal or ovarian tumors, excessive androgen production is produced in the body, ultimately leading to acne. This observation supports the significance of androgens in the development of acne. Furthermore, acne does not typically develop before an individual reaches adrenarche, which is the stage when levels of dehydroepiandrosterone sulfate (DHEAS), an adrenal androgen precursor, are high. However, there is an exception in infantile acne, a condition resulting from excessive androgen production by immature adrenal glands or gonads. Furthermore, it is noteworthy that individuals with androgen insensitivity, specifically men, do not experience the development of acne.[11]
The role of androgens In the development of acne involves various mechanisms, as listed below:
Role of C acnes
C acnes is widely considered a prominent commensal bacterium within the microbiome of the pilosebaceous follicles. The presence of C acnes can trigger both innate and adaptive immune responses, thereby contributing to the inflammatory responses observed in acne. The population of C acnes can be categorized into 3 major divisions. One of these divisions, which includes an epidemic clone known as phylotype IA, is significantly associated with moderate-to-severe acne. The other 2 divisions, phylotypes II and III, are associated with normal skin health and opportunistic infections.
The development of cane involves several factors associated with C acnes and the immune response as listed below:
Role of Genetics
Genetics plays a substantial role in the development of acne, as mentioned below:
Histopathology:
A dilated follicle can be observed with a keratin plug in typical acne lesions. In more advanced cases, the dilated follicle can lead to the formation of an open comedo. When the thin wall of a follicle ruptures, it can lead to the presence of bacteria and signs of inflammation within the surrounding area. In cases where large acne lesions are subjected to trauma, they can develop fibrosis and scarring as part of the healing process.[19]
History and Physical:
Acne occurs on the affected individuals’ face, neck, chest, upper back, and upper arm areas, where large, hormonally responsive sebaceous glands are abundant. Acne presents as a variety of polymorphic lesions from grade 1 to grade 4. Starting with comedones, as listed below:
Grade 1: Also known as “comedones,” and is categorized into two types, open and closed. Open comedones form when the pilosebaceous orifice becomes plugged with sebum and appears as papules with a central, dilated follicular orifice containing gray, brown, or black keratotic material. On the other hand, closed comedones form when keratin and sebum block the pilosebaceous orifice beneath the skin surface. They appear as dome-shaped, smooth papules that can be skin-colored, whitish, or grayish in appearance.
Grade 2: Inflammatory lesions present as a small papule with erythema.
Grade 3: Pustules.
Grade 4: Many pustules coalesce to form nodules and cysts called nodulocystic acne.[20,21]
Some variants of acne vulgaris include:
Acne conglobata: Acne conglobata is a rare but severe form of nodulocystic acne in young males. It usually presents with tender, disfiguring, double- or triple-interconnecting comedones, cysts, inflammatory nodules, and deep burrowing abscesses on the face, shoulders, back, chest, upper arms, buttocks, and thighs. Systemic symptoms are usually absent.
Acne fulminans or acne maligna: Acne fulminans or acne maligna is a rare skin disorder presenting as an acute, painful, ulcerating, and hemorrhagic clinical form of acne. It may or may not be associated with systemic symptoms such as fever and polyarthritis. Acne fulminans also may cause bone lesions and laboratory abnormalities.[22]
Acne excoriée: Acne excoriée is a condition often seen in young women with an underlying psychiatric disorder. It presents with mild acne, including comedones, that are obsessively picked and excoriated, leading to scarring.
Infantile acne: Infantile acne often commences between the ages of 3 and 6 months due to increased androgens produced by the immature adrenal gland in girls and the immature adrenal gland and testes in boys. Androgen levels revert to normal by the time a child attains the age of 1 or 2, with subsequent improvement in acne.[23]
Evaluation
Acne vulgaris is typically diagnosed based on physical examination rather than laboratory tests. Laboratory or radiological tests are required for patients when their clinical evaluation indicates the presence of underlying hyperandrogenism or other specific conditions that require further testing. Skin biopsy is typically not required for diagnosis. However, in women of childbearing age, it is essential to inquire about their history of hirsutism or dysmenorrhea. If the history of hirsutism or dysmenorrhea is positive in women of childbearing age, it is advisable to order further tests to measure the levels of testosterone, luteinizing hormone (LH), follicle-stimulating hormone (FSH), and dehydroepiandrosterone (DHEA).
The sudden onset of severe, recalcitrant acne should raise the suspicion of hyperandrogenism induced by either an ovarian or adrenal tumor. In this case, laboratory and imaging tests may be essential.
Patients diagnosed with acne fulminans should undergo a comprehensive evaluation, including complete blood count, liver function tests, erythrocyte sedimentation rate, and C-reactive protein. This evaluation is particularly important for patients presenting with systemic symptoms. In addition, assessing serum cholesterol and triglyceride levels, performing a urine or serum pregnancy test for women, and considering radiographs when symptoms suggestive of joint or bone involvement are present are recommended. This thorough evaluation aims to assess the systemic involvement of acne fulminans and aids in preparing for isotretinoin therapy. [24-26]
Treatment:
Some herbal formulations used in treatment of acne vulgaris
|
Source |
Botanical name |
Use |
|
Neem |
Azadirachta indica |
Antibacterial, anti-fungal, anti-inflammatory, antiseptic and highly beneficial for oily and acne prone skin |
|
Turmeric |
Curcuma longa |
Antibacterial, antifungal and It protects the skin from many skin infections and also adds glow to the face. |
|
Nutmeg seed |
Myristica fragrance |
Antibacterial, anti-inflammatory, antiseptic, bactericide. |
|
Honey |
Apis dorsaa |
Light humectant and nutrient used as a thickening agent to give body to facial masks, creams and lotions |
|
Lemon juice |
Citrus limon |
To lighten skin and reduce blemish marks on the skin. It also quite effective for treating acne and pimples, as a natural pH adjuster in cosmetic |
|
Rose water |
Rosmarius officinalis |
Used as solvent; it also has antibacterial and antiseptic properties which eventually cure acne |
|
Walnut |
Juglans regia |
Scrubbing action of walnut granules helps break up The mild oil deposits and clear away dead skin cells and debris. |
|
Aloevera |
Aloe barbadensis |
Treat conditions like burns, acne and minor wounds |
|
Wheat |
Triticum sativum |
Prevent loss of moisture from skin |
|
Khirni |
Wrightia tinctoria |
Antibacterial and astringent |
|
Wild carrot, Queen Annes |
Daucus carota |
Sunscreen and fragrance |
|
Gum ghatti |
Anogeissus latifolia |
Binder, emulsifier, and suspending agent |
|
Tragacanth |
Astragalus gummifer |
Thickening agent, demulcent, suspending agent, emulsifying agent, emollient in cosmetics, and sustained release agent |
|
Atanza |
Abizazygia |
Nomdomg agent |
|
Aloe mucilage |
Aloe species |
Gelling agent and sustained release agent. |
|
Bavchi mucil |
Ocimum canum |
Suspending agent and emulsifying agent |
|
Gum acacia |
Acacia arabica |
Suspending agent, emulsifying agent binder in tablets, demulcent an emollient in cosmetics |
|
Khaya gum |
Khaya grandifoliola |
Binding agent |
|
Shatavari mucilage |
Asparagus racemosus |
Binding agent and suspending agent in tablet |
|
Tamarind seed |
Tamarindus indica |
Binding agent and emulsifier |
|
Gellan gum |
Pseudomonas elodea |
Disintegrating agent |
|
Senna tora |
Cassia tora Linn |
Binding agent |
Herbal oils
|
Source |
Botanical name |
Use |
|
Almond oil |
Prunus amygdalus |
Give nourishing the skin, anti-inflammatory, help in vitamin deficiency, good source of vitamin E, weight maintenance, increase hair health,sun damage agging prevention and blood sugar controller |
|
Castor oil |
Ricinus communis |
Relieves various inflammatory conditions of skin |
|
Coconut oil |
Cocos nucifera |
Emollient |
|
Arachis oil |
Arachis hypogaea |
Use to treat acne, sensitive skin, Antispasmodic |
|
Olive oil |
Olea europaea L. |
Moisturize dry skin, remove makeup and as a base for DIY body scrub |
|
Light liquid paraffin |
|
Hydrated dry, scaly skin, use as stabilizer in perfumes and soap s |
|
Heavy liquid paraffin |
|
Moisturizer, relieves itching and inflammation |
Waxes
|
Source |
Botanical name |
Uses |
|
Bees wax |
Apis mellifera, Apis cerana |
Antibacterial, soothes acne, soothes irritated skin, moisturizing ingredient that binds moisture to itself |
|
Carnauba wax |
Copernica prunifera |
Thickening agent, emollient and hardening agent |
|
Paraffin wax |
|
Forms a protective barrier, soften the skin, enhance product absorption |
Colorants
|
Source |
Botanical name |
Use |
|
Cochineal |
Dactylopius cocus |
Give bright red colour |
|
Annatto |
Bixa orellana |
Antioxidant, anti-inflammatory, reduce oilness, UV protection, antimicrobial and soothing |
|
Saffron |
Crocus sativum |
Brightens skin and even tone, reduce signs of agging, antioxidant,hydrate the skin |
Perfumes
|
Source |
Botanical name |
Use |
|
Rose |
Rosmarius officinalis |
Rose water Rosmarius officinalis Used as solvent; it also has antibacterial and antiseptic properties which eventually cure acne |
|
Jasmin essential oil |
Jasminum grandiflorum |
Improve appearance, improve skin tone, moisturize skin, anti-aging power, anti wrinkle, improve skin elasticity |
|
Levender oil |
Lavandula officinalis |
Reduce acne,soothes dry skin conditions,,heals injuries, prevent wrinkle,protect skin from free radical, relieves anxiety and fatigue |
|
Geranium oil |
Pelargonium graveolens |
Balance hormones, reduce stees and anxiety,boosts immune system,aids in wound healing,alleviates respiratory issues,natural skin clearance,heals acne and blemishes, soothes skin irritation |
|
Tubersose oil |
Epimedium accuminatum |
Antifungal, antibacterial, soothes fine line and wrinkles |
|
Champa oil |
Michelia champaca |
Reduce wrinkles, anti-aging, soothing property anti-oxidant, reduce dryness and pigmentation |
|
Neroli oil |
Citrus aurantium |
Anti-inflammatory,pain relieving, anti-inflammatory |
Antioxidants
|
Source |
Botanical name |
Use |
|
Tamarind |
Tamarindus indica |
|
|
Orange peel extract |
|
Anti-oxidant, antiinflammatory, anti-microbial Orange-peel properties can maintain the natural balance of skin oils and tighten the skin by absorbing excess oils and removing dead skin cells |
|
Almond |
Prunus amygdalus |
Give nourishing the skin, anti-inflammatory, help in vitamin deficiency, good source of vitamin E, weight maintenance, increase hair health,sun damage agging prevention and blood sugar controller |
|
Pomegranate |
|
|
|
Resveratrol |
|
|
|
Ferulic acid |
|
|
|
Liquorice |
Glycyrrhiza glabra |
|
CONCLUSION:
Acne Vulgaris is a prevalent, chronic inflammatory disorder of the pilosebaceous unit that, while most common in adolescence, can affect individuals of all ages. The disease manifests through a polymorphic spectrum of lesions, ranging from non-inflammatory comedones to severe, disfiguring nodules and cysts, which are distinct from adult-onset conditions like Rosacea.
Seborrhea: Excess sebum production stimulated by androgens.
Hyperkeratinization: The pathophysiology Is multifactorial, driven by four primary pathogenic events: Abnormal follicular differentiation leading to microcomedo formation.
Microbial Colonization: Proliferation of Cutibacterium acnes (formerly Propionibacterium acnes) in the anaerobic, lipid-rich follicle.
Inflammation: Immune responses triggering follicular rupture and tissue damage
The therapeutic role of herbal and natural ingredients in acne management. It details a wide array of botanicals-such as Neem, Turmeric, and Aloe Vera-along with natural oils and excipients that possess critical antibacterial, anti-inflammatory, and antioxidant properties, offering a natural pharmacological approach to treatment
REFERENCES

Harshada Khandu Pardhi*, Herbal Formulations Used in Treatment of Acne Vulgaris, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 1549-1561 https://doi.org/10.5281/zenodo.17862737
 10.5281/zenodo.17862737
10.5281/zenodo.17862737
