Rajarambapu College of Pharmacy, Kasegaon, India
Ocular keratitis, particularly fungal keratitis, remains a significant cause of visual impairment globally, especially in tropical and subtropical regions. Conventional ophthalmic formulations like eye drops often suffer from poor ocular bioavailability due to rapid precorneal elimination, tear turnover, and blinking. To address these limitations, the present research aimed to develop a fluconazole-loaded in-situ gel (ISG) using temperature-sensitive polymers for sustained ocular drug delivery. The study utilized Poloxamer 407, in combination with mucoadhesive agents such as xanthan gum and carbopol 934, to formulate a sol-to-gel system that undergoes gelation upon contact with physiological temperature. A 3² factorial design was employed to optimize the formulation based on critical parameters including gelation temperature, viscosity, and drug release profile. The optimized ISG formulation was characterized for clarity, pH, viscosity, gelation time and temperature, mucoadhesive strength, in vitro diffusion, and release kinetics. The antifungal efficacy of the optimized formulation was tested against Candida albicans and confirmed via agar diffusion studies. Additionally, the formulation exhibited sustained drug release, improved ocular residence time, and was found to be non-irritating in the HET-CAM test. Stability studies further validated the physical and chemical integrity of the formulation over a defined period. This study successfully demonstrates the potential of fluconazole-loaded thermosensitive ISGs as an effective, patient-compliant strategy for the targeted treatment of fungal keratitis, enhancing both therapeutic efficacy and drug bioavailability.
Ocular drug delivery is one of the most challenging areas in pharmaceutical sciences due to the complex anatomy and physiology of the eye. The eye possesses multiple protective mechanisms—such as tear turnover, nasolacrimal drainage, blinking reflex, and the tightly structured corneal epithelium—which serve as efficient barriers to foreign substances, including topically applied drugs (1). These physiological barriers significantly reduce drug absorption and therapeutic efficacy, making it difficult for conventional ocular formulations to deliver therapeutic drug levels to intraocular tissues. As a result, less than 5% of the administered dose of eye drops typically penetrates to exert a pharmacological effect (2).
Among the various ocular conditions, fungal keratitis has emerged as a severe and potentially blinding infection of the cornea, especially in tropical and subtropical regions. It is primarily caused by pathogenic fungi, including filamentous species such as Fusarium and Aspergillus, and yeast-like organisms such as Candida species (3). These infections often result from trauma with vegetative matter, prolonged use of corticosteroids, ocular surface disease, or improper contact lens hygiene. The condition requires prompt and effective antifungal treatment to prevent progression and vision loss.
Fluconazole, a triazole antifungal agent, is widely known for its broad-spectrum antifungal activity, particularly against Candida species. It exerts its antifungal effect by inhibiting cytochrome P450-dependent 14α-demethylase, an essential enzyme in the fungal ergosterol biosynthesis pathway (4). Despite its favorable pharmacokinetic profile and excellent penetration into ocular tissues, fluconazole’s clinical use in ophthalmology is hindered by its rapid elimination from the ocular surface. Frequent instillation is required to maintain therapeutic drug concentrations, which adversely affects patient compliance and overall treatment efficacy (5).
To overcome these limitations, novel ocular drug delivery systems are being explored, with in-situ gels (ISGs) gaining considerable attention. These are liquid upon instillation but undergo a phase transition to form a gel in response to physiological stimuli, such as changes in temperature, pH, or ionic strength (5). This phase transition not only enhances the retention time of the drug on the ocular surface but also provides sustained drug release, thus improving therapeutic outcomes and patient compliance.
Among the various types of ISG systems, thermosensitive in-situ gels are particularly promising. These formulations remain in liquid form at room temperature and gel upon contact with the ocular surface temperature (~35°C). Poloxamer 407, a thermoresponsive polymer, is widely used for this purpose due to its reverse thermal gelation properties. At lower temperatures, Poloxamer 407 exists as a free-flowing solution, but it transforms into a semi-solid gel at physiological temperatures owing to micellization and packing of its copolymer blocks (6). However, Poloxamer gels alone may lack sufficient mucoadhesive strength and mechanical integrity to withstand tear dilution and blinking forces. To address this, additional polymers like xanthan gum and carbopol 934 are incorporated. These polymers enhance viscosity, bioadhesion, and structural stability, resulting in improved ocular retention and prolonged drug action (7).
To systematically develop and optimize such a complex formulation, the 3² factorial design is a robust statistical approach. It allows for the evaluation of the interaction between multiple formulation variables and their influence on critical quality attributes. In this study, two independent variables—concentration of xanthan gum and carbopol 934—were varied at three levels to assess their impact on key parameters such as gelation temperature, viscosity, mucoadhesive strength, and drug release behavior.(8)
Objectives:
Methodology
Materials
Fluconazole was procured as the active pharmaceutical ingredient (API) for antifungal activity. Poloxamer 407 (Pluronic F127) was employed as the primary thermosensitive polymer. Xanthan gum and carbopol 934 were used as mucoadhesive and viscosity-modifying agents. All other chemicals and reagents used in the study were of analytical grade and used as received without further purification.
UV visible spectroscopy
UV visible spectroscopy of Fluconazole in water
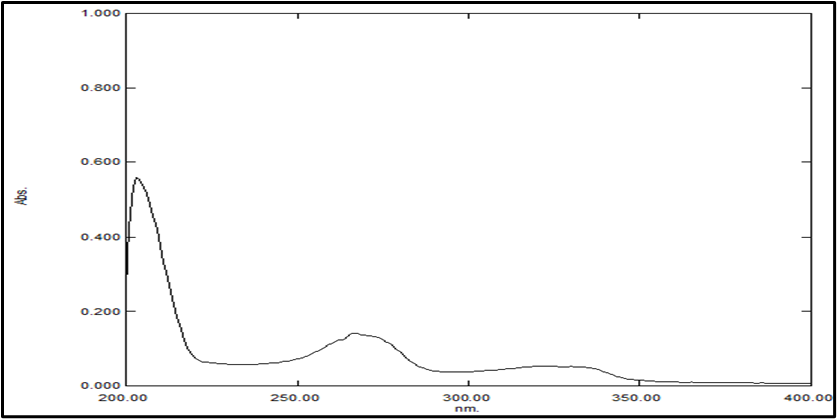
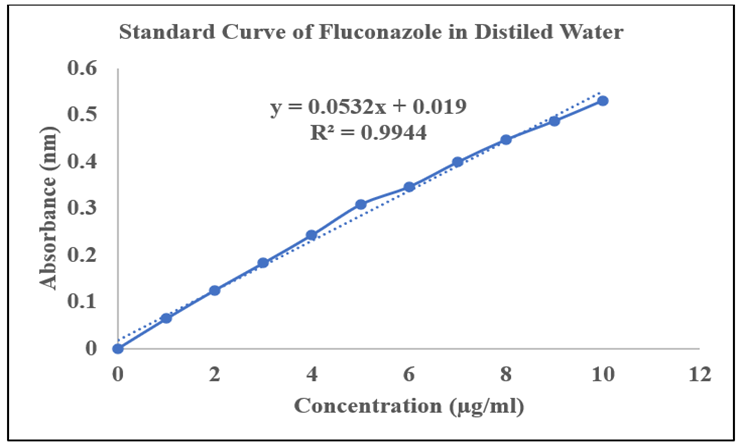
Table No.1: Absorbance of Calibration Curve of Fluconazole in water
|
Sr. no |
Concentration (µg/ml) |
Absorbance ± SD* |
|
1. |
0 |
0 |
|
2. |
2 |
0.064±0.0032 |
|
3. |
4 |
0.125±0.0023 |
|
4. |
6 |
0.183±0.0015 |
|
5. |
8 |
0.243±0.0011 |
|
6. |
10 |
0.308±0.0017 |
|
7 |
12 |
0.346±0.0031 |
|
8 |
14 |
0.399±0.0024 |
|
9 |
16 |
0.447±0.0019 |
|
10 |
18 |
0.487±0.0023 |
|
11 |
20 |
0.531±0.0028 |
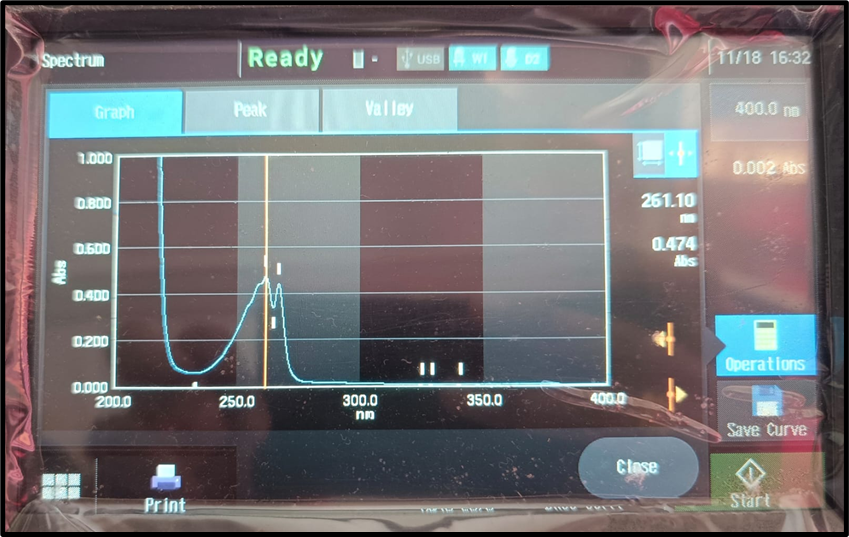
UV visible spectroscopy of Fluconazole in STF
Calibration Curve of Fluconazole in STF pH 7.4:
Calibration curve Fluconazole carried composition of STF pH 7.4 at λmax 261 nm. The preparation of standard curve between absorbance and concentration is shown in Figure no. 8.3 and values of absorbance are shown in Table No. 8.4.
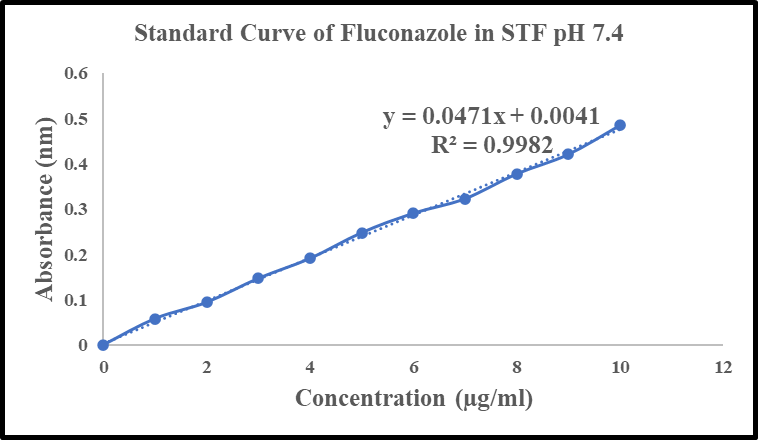
Absorbance values for the Fluconazole calibration curve were measured in STF at pH 7.4.
|
Sr. No. |
Concentration (µg/ml) |
Absorbance± SD* |
|
1 |
0 |
0 |
|
2 |
2 |
0.058±0.0032 |
|
3 |
4 |
0.094±0.0023 |
|
4 |
6 |
0.147±0.0015 |
|
5 |
8 |
0.191±0.0011 |
|
6 |
10 |
0.248±0.0017 |
|
7 |
12 |
0.291±0.0031 |
|
8 |
14 |
0.323±0.0024 |
|
9 |
16 |
0.378±0.0019 |
|
10 |
18 |
0.421±0.0023 |
|
11 |
20 |
0.485±0.0028 |
FTIR Spectroscopy of Fluconazole:
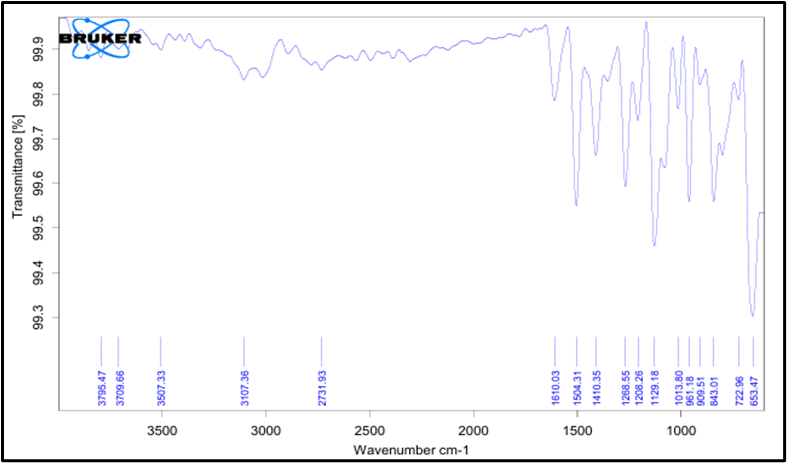
Fig No 1: FTIR of Fluconazole
Table No 3. Result of FTIR Fluconazole
|
Observed Peak (cm1) |
Functional group |
Type of vibration |
Indication |
|
3032.56 |
Aromatic ring |
Stretching |
C-H |
|
2981.77, 2925.45 |
Alkyl group |
Stretching |
C-H |
|
1590.78, 1507 |
Aromatic |
Stretching |
C-H |
|
1383.61 |
Nitrate ion |
Stretching |
NO3 |
|
1279.56 |
Imidazole or ether ring |
Stretching |
C-N |
|
1039.96, 1039.90 |
Possible ether or nitrate |
Stretching/ overlap |
C-O/SO2 |
|
829.96, 721.56 |
Aromatic ring |
Bending |
C-H |
|
625.65 |
Imidazole/ benzene ring |
Ring deformation |
- |
8.3.1.2. FTIR Spectroscopy of Poloxamer 407:
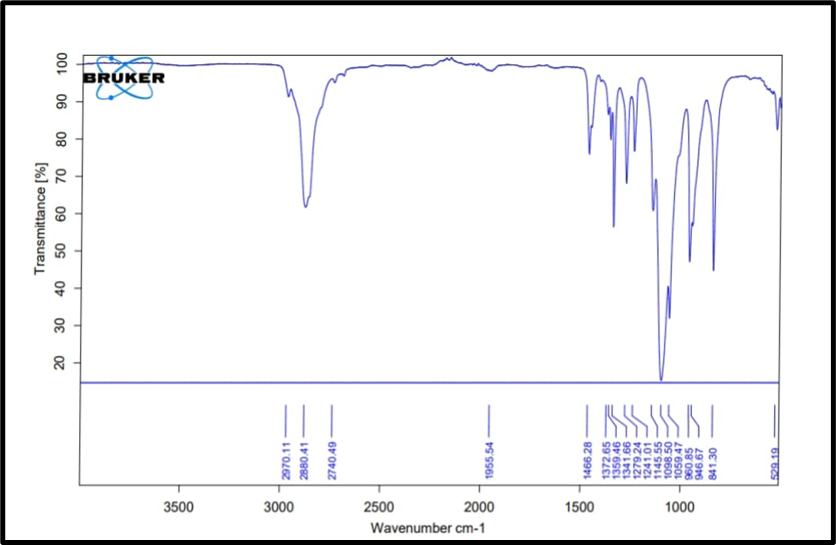
Fig No 2: FTIR of Poloxamer-407
Table No. 4. Results of FTIR of Poloxamer-407
|
Observed Peak (cm-1) |
Functional group |
Type of vibration |
Indication |
|
2880.33 |
Amide |
Stretching |
N-H |
|
2742.89 |
Alkane |
Stretching |
C-H |
|
2238.95 |
Nitrile |
Stretching |
C≡N |
|
1644.5 |
Amide |
Stretching |
C=O |
|
1464.19 |
Aromatic ring |
Stretching |
C=C |
|
838.883 |
Aromatic ring |
Bending |
C-H |
8.3.1.3. FTIR Spectroscopy of Xanthan Gum:
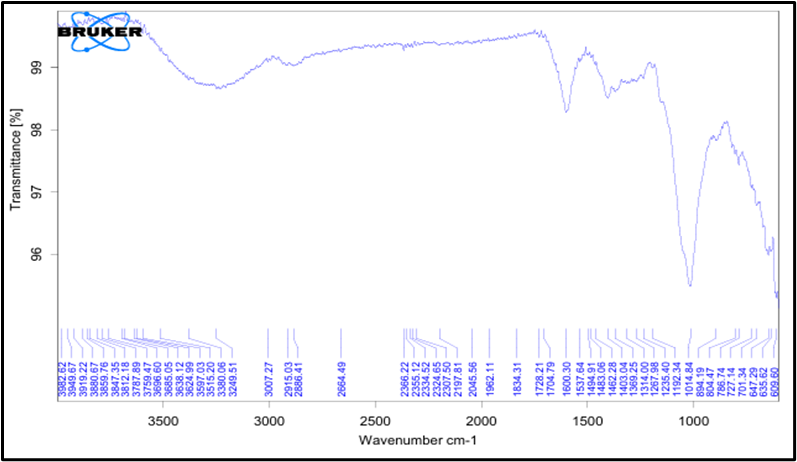
Fig No 3: FTIR of Xanthan Gum
Table No 5. Results of FTIR of Xanthan gum
|
Observed Peak (cm-1) |
Functional group |
Type of vibration |
Indication |
|
2918.73 |
Alkane |
Stretching |
C-H |
|
1728.21 |
Carboxylic group |
Stretching |
C=O |
|
1600.30 |
Aromatic ring |
Stretching |
C=C |
|
1014.84 |
Ether |
Stretching |
C-O-C |
|
780.14 |
Alkyl halide |
Stretching |
H-Cl |
8.3.1.4. FTIR Spectroscopy of Physical Mixture
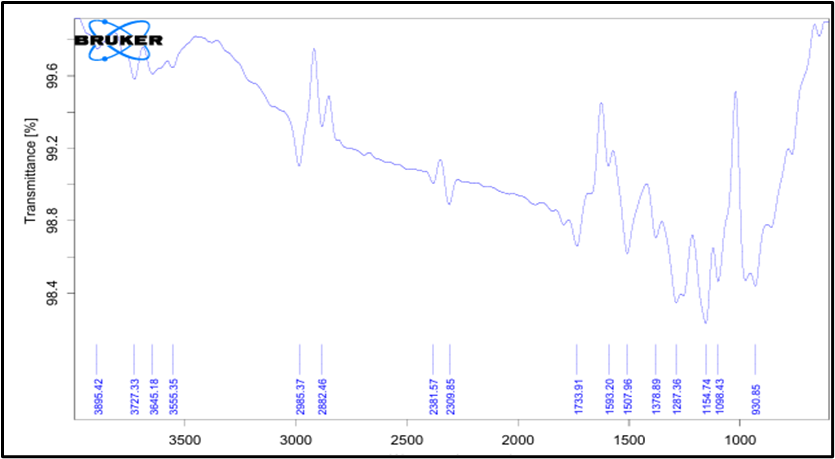
Fig No 4: FTIR of Physical Mixture
Table No 6. Results of FTIR of Physical Mixture
|
Observed Peak (cm-1) |
Functional group |
Type of vibration |
Indication |
|
2927.78 |
Aliphatic |
Stretching |
C-H |
|
1733.91 |
Ester |
Stretching |
C=O |
|
1154.74 |
Amide |
Stretching |
C-N |
|
1378.89 |
Alkyl Halide |
Stretching |
C-F |
|
1154.74 |
Ether |
Stretching |
C-O-C |
RESULT AND DISCUSSION :
Formulation of Fluconazole loaded in-situ gel batches:
In-situ gel technology shows promise as an effective formulation approach, especially for water-soluble drugs like fluconazole. In laboratory settings, the cold method is employed to develop these ISG’s. To prepare the ISG’s, various concentrations of poloxamer 407 and xanthan gum were used. Poloxamer 407 was first dispersed in cold distilled water, after which xanthan gum was incorporated. Fluconazole was dissolved separately and then added to the xanthan gum mixture. Finally, the poloxamer solution was adjusted accordingly. The poloxamer solutions were partially hydrated and stirred at intervals until clear and uniform solutions were formed.
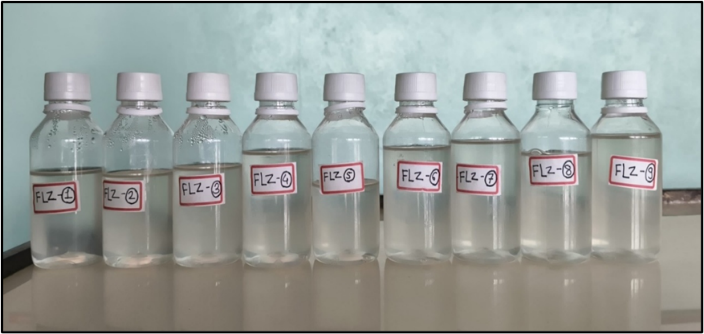
Fig. No 5: Formulation of FLZ-ISG using 32 Factorial Design
Fig. No 6: Optimized batch of FLZ-ISG
8.7 Characterization of final batches of FLZ-ISG using 32 full factorial design:
Table No 7. Final batches of FLZ-ISG using 32 full factorial design
|
Batches code |
Drug (%) |
Poloxamer-407(%) |
Xanthan gum (%) |
Gelation temperature(0C) |
Gelation time (sec) |
Drug Release (%) |
|
FLZ1 |
300 |
16 |
50 |
37.5 |
140 |
95.52 |
|
FLZ2 |
300 |
16 |
75 |
36.3 |
105 |
92.34 |
|
FLZ3 |
300 |
16 |
100 |
34.6 |
73 |
88.83 |
|
FLZ4 |
300 |
17 |
50 |
34.8 |
75 |
92.81 |
|
FLZ5 |
300 |
17 |
75 |
33.8 |
65 |
88.2 |
|
FLZ6 |
300 |
17 |
100 |
32.4 |
60 |
85.01 |
|
FLZ7 |
300 |
18 |
50 |
33.2 |
60 |
88.51 |
|
FLZ8 |
300 |
18 |
75 |
32.3 |
65 |
83.9 |
|
FLZ9 |
300 |
18 |
100 |
30.2 |
75 |
80.23 |
Visual Appearance and Clarity:
The formulation of thermoreversible ocular ISG of Fluconazole was found to be clear (++) and transparent at room temperature in liquid phase and also in gel form was found to be clear (++) and transparent. It is represented in following observation Fig. No 8.
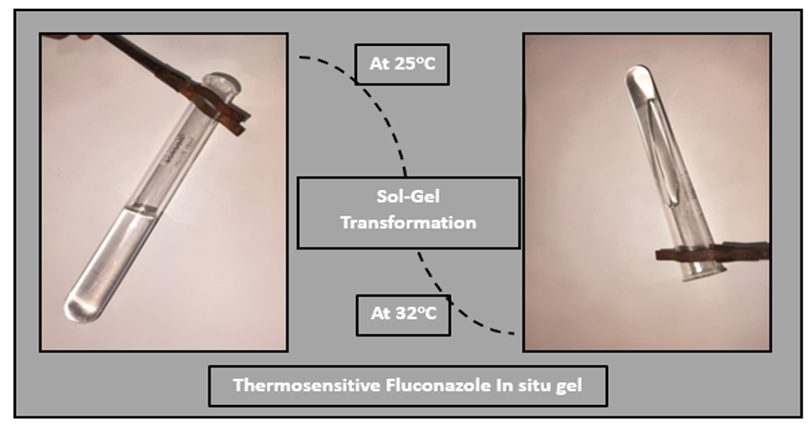
Fig. No.7: Visual Appearance and Clarity
Table No.8: Visual Appearance and Clarity
|
Sr. No. |
Formulation Code |
Appearance of solution |
Appearance of gel |
|
1 |
FLZ 1 |
Transparent |
Transparent |
|
2 |
FLZ 2 |
Transparent |
Transparent |
|
3 |
FLZ 3 |
Transparent |
Transparent |
|
4 |
FLZ 4 |
Transparent |
Transparent |
|
5 |
FLZ 5 |
Transparent |
Transparent |
|
6 |
FLZ 6 |
Transparent |
Transparent |
|
7 |
FLZ 7 |
Transparent |
Transparent |
|
8 |
FLZ 8 |
Transparent |
Transparent |
|
9 |
FLZ 9 |
Transparent |
Transparent |
pH
The pH of all ocular ISG of Fluconazole formulations was found to be in the range of 6.5– 7.0 it is represented in following observation Table No. 8.22
Table No. 9: pH of All Formulation Batches
|
Sr. No. |
Formulation Code |
pH |
|
1 |
FLZ 1 |
6.6 |
|
2 |
FLZ 2 |
6.5 |
|
3 |
FLZ 3 |
6.6 |
|
4 |
FLZ 4 |
6.8 |
|
5 |
FLZ 5 |
6.9 |
|
6 |
FLZ 6 |
7.1 |
|
7 |
FLZ 7 |
6.5 |
|
8 |
FLZ 8 |
6.7 |
|
9 |
FLZ 9 |
7.0 |

Fig.No.8: pH of optimized batch
Viscosity
The viscosity of all ISG of Fluconazole formulations were measured by Brookfield Viscometer with spindle no. 62 at 100 rpm in before gelation and after gelation. It is represented as following observation Table No. 8.23
Table No. 10: Viscosity (cps) of All Formulation Batches
|
Sr. No. |
Formulation Code |
Viscosity of solution at 100 rpm(cP) |
Viscosity of gel at 100rpm(cP) |
|
1 |
FLZ 1 |
79.0 |
1109 |
|
2 |
FLZ 2 |
119.0 |
1265 |
|
3 |
FLZ 3 |
130.0 |
1582 |
|
4 |
FLZ 4 |
111.6 |
1267 |
|
5 |
FLZ 5 |
194.0 |
1987 |
|
6 |
FLZ 6 |
275.1 |
2840 |
|
7 |
FLZ 7 |
207.8 |
2165 |
|
8 |
FLZ 8 |
357.0 |
3234 |
|
9 |
FLZ 9 |
398.0 |
3889 |
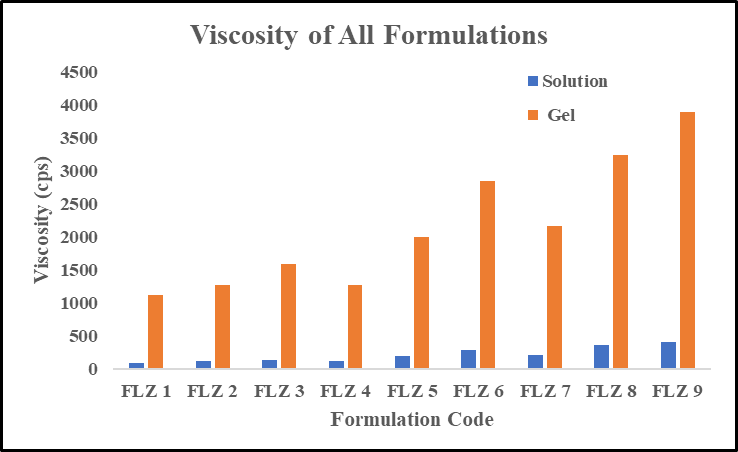
Fig. No. 9: Viscosity (cps) of All Formulation Batches
Gelation Temperature:
The study of gelation temperature of all ocular ISG of Fluconazole was studied. It is determined in following observation Table. No. 8.24.
Table No. 11: Gelation Temperature of All Formulation Batches
|
Sr. No. |
Formulation Code |
Temperature (ºC) |
|
1 |
FLZ 1 |
37.5 |
|
2 |
FLZ 2 |
36.3 |
|
3 |
FLZ 3 |
34.6 |
|
4 |
FLZ 4 |
34.8 |
|
5 |
FLZ 5 |
33.8 |
|
6 |
FLZ 6 |
32.4 |
|
7 |
FLZ 7 |
33.2 |
|
8 |
FLZ 8 |
32.3 |
|
9 |
FLZ 9 |
30.2 |

Fig.No.10: Gelation Temperature measurement
Gelation Time
The study of gelation time of all ocular ISG of Fluconazole was studied. It is determined in following observation Table. No. 8.25.
Table No. 12: Gelation Time of All Formulation Batches
|
Sr. No. |
Formulation Code |
Time (sec) |
|
1 |
FLZ 1 |
140 |
|
2 |
FLZ 2 |
105 |
|
3 |
FLZ 3 |
73 |
|
4 |
FLZ 4 |
75 |
|
5 |
FLZ 5 |
65 |
|
6 |
FLZ 6 |
60 |
|
7 |
FLZ 7 |
60 |
|
8 |
FLZ 8 |
65 |
|
9 |
FLZ 9 |
75 |
Eye irritation test: HET-CAM
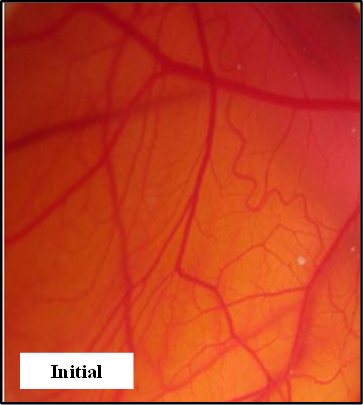
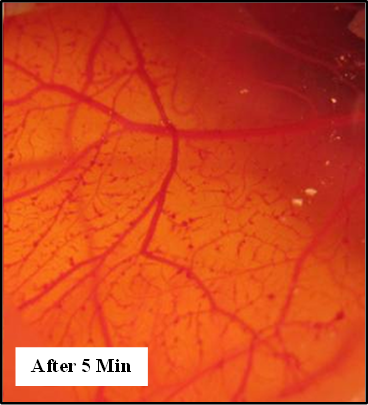
Fig No 11: A sequence of images shows the changes on the membrane when treated with 0.9% saline solution (negative control) over a duration of five minutes.
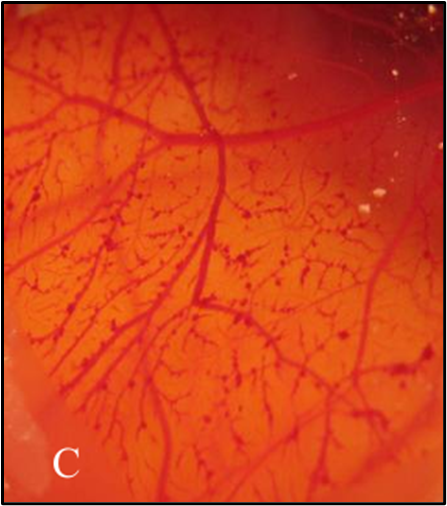

Fig No 12: A sequence of images shows the changes on the membrane when treated with 1 M NaOH (positive control) over a duration of five minutes.

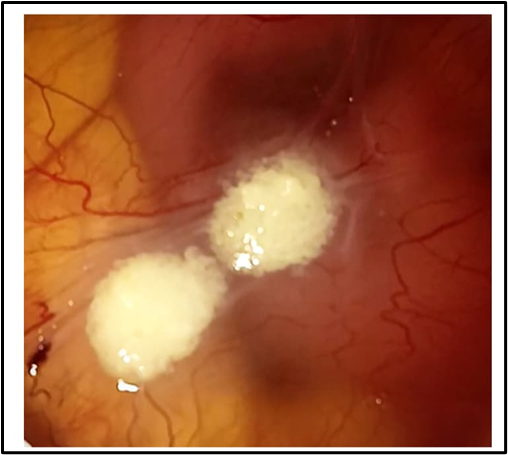
Fig No 13: A sequence of images shows the changes on the membrane when treated with B4 (test) over a duration of five minutes.
The HET-CAM test was conducted to assess the immediate irritant potential of the optimized formulation FCZ 4 by observing any signs of irritation on the CAM membrane. The positive control (1 M NaOH) induced irritation, leading to bleeding and normal hyperemia, while the negative control (0.9% saline solution) exhibited no irritancy, maintaining normal tissue vascularization. When compared with these controls, it was evident that the optimized ISG formulation FCZ 4 did not trigger any inflammatory responses and preserved the normal vascular structure of the CAM tissue (arteries, veins, and capillaries). This indicates that formulation B4 is non-irritant and does not cause vascular damage.
This study confirmed that the optimized formulation FCZ 4 is safe and non-irritant, making it a promising platform for the effective delivery of Fluconazole to ocular tissues, particularly for Fungal Keratitis.
Antifungal activity:
The agar well diffusion method was used to assess the antifungal efficacy of FLZ-ISG formulations against Candida albicans. A standard fluconazole solution and a blank control were used to evaluate two test formulations, Sample A (FLZ 4) and marketed eye drop (ZOCON).
Each sample was evaluated at two concentrations (100 µL and 200 µL) to look for dose-dependent antifungal effects. The formulation's efficacy in inhibiting fungal growth was demonstrated by the measurement of the zone of inhibition (ZOI) in nanometers (nm).
Visual Observations:
1) Sample A (FLZ 4) is displayed on the left petri plate, and Sample B (MCZ 5) is displayed on the right petri plate.
2) The wells holding the sample solutions exhibit distinct zones of inhibition.
3) As anticipated, the standard fluconazole (Std) has a noticeably greater inhibitory zone than the samples.
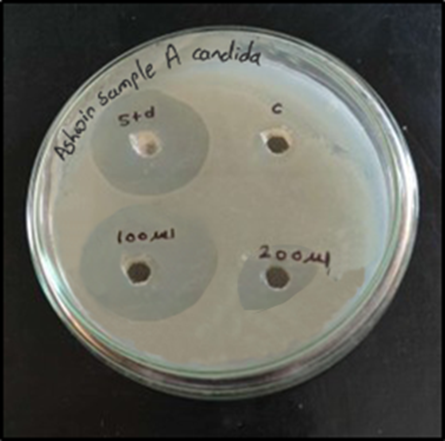
Fig.No.14. Antifungal Activity: A) Sample A FCZ And Marketed ZOCON
Table No 8.30. Antifungal activity by candida Albicans
|
Sr. No |
Sample |
Concentration |
Zone of Inhibition(nm) candida Albicans |
Observation |
|
1. |
Control |
|
- |
No antifungal activity (negative control) |
|
2. |
Standard Fluconazole |
1mg/ml |
15 |
Shows good antifungal activity (positive control) |
|
3. |
Sample-A
|
100μl |
35 |
Strong antifungal activity |
|
200μl |
7 |
Moderate increase in activity with higher dose |
The antifungal activity results confirm that the FLZ-ISG formulations possess antifungal potential, with Sample A (FLZ 4) demonstrating better efficacy than (marketed eye drop ZOCON). This demonstrates that in situ gel formulations have the potential to treat ocular fungal infections, particularly when it comes to maintaining drug release and offering localized action at the infection site.
8.11.13 Stability study:
The stability study was conducted over a period of 30 days. The optimized formulation was stored in a stability chamber at 40?±?2?°C with 75?±?5% relative humidity, while room temperature conditions were also used for comparison. The study monitored the stability of the optimized formulation under these conditions, and the following observations were recorded.
Table No. 14: Stability evaluation of the optimized batch (FLZ4) conducted at 40 ± 0.5°C and 75 ± 5% relative humidity conditions.
|
Days |
Appearance |
Clarity |
pH |
Viscosity (cps) |
Drug Content (%) |
|
0 |
Transparent |
Clear |
6.8 |
1260 |
94.43 |
|
7 |
Transparent |
Clear |
6.8 |
1298 |
94.03 |
|
15 |
Transparent |
Clear |
6.9 |
1387 |
93.49 |
|
30 |
Transparent |
Clear |
6.9 |
1511 |
93.41 |
CONCLUSION:
A fluconazole-loaded in situ gel was effectively designed and optimized in this study utilizing a 3² factorial design to treat ocular fungal keratitis. Appropriate pH (6.8), fast gelation at physiological temperature (34.8°C), and sustained drug release with 92.81% drug diffusion were among the optimal formulation's ideal physicochemical characteristics. A non-Fickian diffusion mechanism and the Higuchi kinetic model supported the drug release, suggesting a combination of diffusion and polymer relaxation-controlled release. The formulation demonstrated significant antifungal activity against Candida albicans, The ISG was found to be a viable substitute for traditional eye drops in the therapy of fungal keratitis due to its overall superior ocular retention, extended medication availability, and increased patient compliance.
REFERENCES



Ashwinkumar Budhanale, Dr. Mangesh Bhutkar, Sangram Patil, Design and Evaluation of Fluconazole loaded In-Situ Gel for Ocular Keratitis, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 7, 3463-3477. https://doi.org/10.5281/zenodo.16421220
 10.5281/zenodo.16421220
10.5281/zenodo.16421220
