Sagar Institute of Research and Technology –Pharmacy.
Curative therapy represents a significant advancement in modern medicine, aiming to completely eliminate diseases rather than merely managing their symptoms. Unlike palliative care, which focuses on symptom relief and improving the quality of life, curative therapy strives to address the root cause of illness to restore full health. This distinction marks a transformative shift in how chronic and life-threatening conditions are approached. With ongoing innovations in gene therapy, personalized medicine, targeted drug regimens, and minimally invasive surgical procedures, curative therapies are now providing viable treatment options for diseases once thought to be incurable. The introduction of these therapies has not only improved survival rates but also enhanced the overall well-being of patients. Additionally, the ripple effects of these treatments extend to families and society by reducing long-term healthcare costs and dependency on prolonged supportive care. As the healthcare landscape continues to evolve, curative therapy symbolizes hope and progress, offering the possibility of complete recovery and a better quality of life. Continued research, ethical application, and equitable access will be essential in ensuring these breakthroughs benefit a broader population across various health systems.
Curative therapy refers to medical treatments aimed at completely eradicating a disease or significantly reversing its effects, ultimately leading to the restoration of normal health. Unlike palliative care, which focuses on relieving symptoms and improving quality of life, curative therapies strive to eliminate the root cause of the illness. With rapid advancements in medical science, such as gene therapy, targeted drug regimens, and advanced surgical interventions, curative treatments have become increasingly available for diseases that were once deemed incurable. These therapies not only offer hope to patients but also bring profound changes in the lives of their families and the broader community.
The impact of curative therapy on families is multifaceted. On an emotional level, the possibility of a cure brings immense relief, reducing stress and anxiety that accompany chronic or life-threatening conditions. Financially, although the cost of curative treatments can be high, successful outcomes often reduce the longterm burden of healthcare expenses, hospital visits, and lost productivity. Families regain stability and can redirect their resources towards education, employment, and personal growth. Socially, the stigma often associated with chronic illness begins to fade as patients recover and reintegrate into everyday life. This renewed participation strengthens family bonds and social connections. On a societal level, the implications are even more extensive. A healthier population contributes to greater productivity, reduced healthcare costs, and improved quality of life. Communities benefit from increased economic output, lower disease transmission, and reduced dependency on public health systems. Additionally, curative therapies often pave the way for scientific innovation and medical breakthroughs, setting new standards in healthcare delivery. However, challenges remain in ensuring equal access to such therapies, particularly in low-income settings, where socioeconomic disparities may limit their availability. In conclusion, curative therapy holds transformative potential not only for individual patients but also for their families and society at large. It restores hope, reduces long-term healthcare burdens, and fosters a more resilient, inclusive, and productive community. As healthcare systems evolve, it is essential to balance innovation with accessibility to ensure that the benefits of curative treatments reach all segments of the population.
Curative therapy
Our definition of curative therapy is a time-limited treatment that removes the symptoms of a disease through permanent (or semi-permanent) correction of the underlying condition. In contrast, a pill that a patient needs to take for the rest of their life to manage symptoms or disease progression is not curative.
From our analysis, we have defined three archetypes of curative treatments:
A biology-modifying drug is one that targets a particular mechanism that contributes to, or is responsible for, the underlying disease. An example is the hepatitis C virus (HCV) treatment Sovaldi (Gilead Sciences), in which a nucleoside analog interferes with viral replication, thereby curing the patient of hepatitis. Gene therapy addresses the underlying causes of a disease by correcting the missing or mutated genes. It can be divided into somatic and germ-line therapy, with the latter treatment curing not only the current patient but also their future offspring. Examples include Luxturna from Spark Therapeutic for patients with inherited retinal diseases (IRDs). . The number of curative treatments is increasing. Analysis of the clinical trials pipeline undertaken by Arthur D. Little shows that approximately 5 percent of all drugs currently registered as active in clinicaltrials.gov are potentially curative 1. The highest share of potentially curative treatments can be observed in phase I (the earliest testing phase), which indicates that we will see a significant increase in the number of curative treatments reaching the market over the next 10 years. Curative treatments have the potential to lower the overall impact and cost that particular diseases have on healthcare systems, as they eliminate the need for long-term chronic care. This will change the way we treat patients and impact how healthcare providers organize care and its delivery.:- The sales and upfront cost profiles of these new treatments will have an immense impact on payers and providers. It will demand the development of new models for payment and reimbursement in order for their introduction to be affordable. Impact on a cancer center if multiple expensive curative treatments were introduced in the same year. This higher variability in costs makes it increasingly difficult to plan and budget – aspects that are key to healthcare systems given that they are under continuous cost pressure This impact is already being seen. Many one-payer health systems have observed significant increases in drug spending directly attributable to the introduction of Sovaldi, which costs $84,000 for a threemonth course of treatment. For budgetary reasons, England’s National Health Service (NHS) tried to delay its availability (along with next-generation therapy Havoni) to patients and looked to cap the annual number of patients receiving the treatment. In the US, some state Medicaid programs and private health insurers restricted access to curative therapies, which led to warnings from federal officials and lawsuits from patients. Medicaid programs in 29 states said Sovaldi was the first or second most costly pharmaceutical outlay that they had to make. While payers recognize that drugs such as Sovaldi lead to bigger medical savings later on – for example, if Hepatitis C is left untreated, it can lead to cirrhosis, liver failure, or liver cancer – its immediate financial impact has a profound effect on the current budgets of insurers and payers. And this is for a drug that is relatively low cost compared to some other curative treatments. In contrast, imagine the cost and operational
3.The Principles of Curative Therapy
1. Most cancers are systemic at the time of diagnosis. 2. The disease which is delineated by the most sophisticated imaging studies is not all the disease the patient has. 3. The invisible disease is by far more lethal than the visible one. 4. The strategy of treatment that addresses the local disease first is good for the doctor but not for the patient. 5. Systemic therapy should be the first assault on the disease in most instances. B. Principles of therapy: 1. The first battle against cancer is the most important one. 2. Consequently, one must use the most overwhelming aggressive treatment in the beginning. 3. The standard strategy of using less aggressive treatment in the beginning and refraining from using the most effective agents until the disease relapses is a strategy for failure. 4. Use the maximum tolerated dose of a drug. 5. Treatment should be continued until the progression of the disease or achievement of a complete remission. 6. The most common mistake is cessation of therapy on achievement of a complete remission. 7. Failure to achieve a remission after one, two or three regimens should not mean that the patient will not benefit from further treatment. C. What does it take to deliver the above principles:
4. Key Factors to Consider in Anticipation of Curative Therapies
Curative therapies have the potential to disrupt the healthcare market and, most importantly, to dramatically improve the lives of patients struggling with significant, long-term conditions. A number of questions need to be addressed by the pharma companies providing treatments, care providers, payers, and policymakers in order to control the market disruption caused by curative treatments while also maximizing their positive impact.
4.1Curative Care vs. Palliative Care
Palliative care or hospice care is given to patients with serious or terminal illnesses and diseases, including heart failure and cancer. Aside from palliative care, these patients receive palliative medicine from the cancer center, public health facility, or other healthcare systems where they are confined. They receive care designed for their specific illness, and treatments and therapies are provided to alleviate their symptoms and pain. It may seem as if you are no longer given hope for a cure when undergoing palliative care or hospice care, but this is not the same as the end of life. Palliative care offers palliative medicine to improve a patient’s quality of life. Despite having an illness without a cure, palliative care aims to prolong your life. Palliative care or hospice care makes life easier to live despite your terminal illness or serious medical problem. On the other hand, curative care is similar to how you get cured of any disease or illness – by taking medicine and getting proper care. Curative care therapies provide comfort by addressing your specific health concerns and giving proper treatments to help you heal. Curative care is similar to having a disease, for example, a skin allergy. When you have this health concern that is giving you discomfort, you will go to a doctor to seek treatment. The doctor may provide medicine, such as antibiotics, which you will take or apply. You only have to note that patients usually suffer from more serious medical problems than a skin allergy when they seek curative care. The more complicated the disease is, the more complicated the therapies and medications you need to undergo and take.
Here are some examples of curative care:
The Three Archetypes of Curative Treatments
Curative care involves treatments given to patients for a limited time. These treatments target the cause and symptoms of the underlying disease to correct them permanently or semi-permanently. Curative care does not include medicines a patient needs to take for the rest of their life. Take a look at the three archetypes of curative care:
Drug
This drug modifies a patient’s biology. It targets and heals whatever the cause of the symptom, pain, and specific illness. For example, hepatitis is cured by preventing viral replication through nucleoside analog interference. This is made possible through curative care medicine called Sovaldi (Gilead Sciences), which treats a patient with the hepatitis C virus.
Gene therapy
It corrects the mutated or missing genes to cure the illness and alleviate pain. This curative care can be divided into germ-line and somatic therapy. The germ-line therapy treats the patient and the kids they might conceive in the future. A good example of this is Spark Therapeutic’s Luxturna. This curative care is given to patients with IRDs or inherited retinal diseases.
Re-engineering cells
Some good samples of this curative care are stem cell and CAR-T treatments. Curative care can be used alongside palliative care for patients who are experiencing serious or chronic illnesses. Using both types of health care service options allows patients who are suffering from life-threatening diseases to fight the disease while receiving relief from debilitating symptoms until it is cured. More complicated problems often involve more complicated treatments. The challenge is that there is often more than one way to treat a given problem and that each treatment choice has different risks and benefits.
Examples of curative care include:
5. Goal

Figure 1.
Curative care is a health care service that aims to cure disease or provide recovery from injury or illness. Curative treatment is a medical treatment that cures the disease, illness, or injury and is contrasted with palliative treatment, which focuses on providing symptom relief. Curative treatment services can be provided in a variety of settings, including homes, residential facilities, offices of general practitioners, specialized facilities, and hospitals. The complexity of the medical condition and the needs of the patient will determine where the curative treatment is provided. Curative treatments are used to treat conditions such as cancer, bacterial infections, kidney failure, stroke, blood disorders, heart disease, cystic fibrosis, and some neurological disorders. Fig1. Curative and non-curative states in prostate cancer. Localized prostate cancers (CaPs) can be divided into low-, intermediate- and high-risk (including locally advanced) groups using T-category, pre-treatment prostate-specific antigen (PSA). level and the pathologic Gleason score. These groups have an increasing probability of CaP-specific mortality. Low-risk tumors can be aggressively followed using active surveillance. By contrast, intermediate-risk tumors are treated with surgery, external beam radiotherapy (EBRT), or brachytherapy. In cases where a local recurrence occurs after surgery, patients can be treated with post- operative EBRT and convert a local failure into a cure. In high-risk CaP, there is an increased probability for occult systemic metastases, therefore -free survival by months. These therapies include additional ADT (including the use of newer agents, such as abiraterone and enzalutamide), chemotherapy, immunotherapy, systemic radionucleotides (RA233), and the use of bespoke molecular-targeted agents. It is argued that an understanding of the genomic and microenvironmental factors that lead to occult metastases could drive intensification protocols using systemic agents in the localized CaP setting to improve the cure rates with radiotherapy and surgery. LHRH, luteinizing hormone-releasing hormone; Post-op, post-operative; RA223, radium-223.

Figure 2.
Despite a multitude of treatment options, there are no individualized clinical tests that absolutely tell which patients are unlikely to fail local treatment from those patients who are most likely to fail local treatment within a given clinical risk 9 category. This problem is illustrated by the fact that despite the use of stringent clinical criteria to place patients into clinical prognostic groups, 30–50% of males can still fail precision RT or surgery owing to local resistance and/or systemic spread.1–3 Despite the publication of Phase III dose-escalated EBRT clinical trials in CaP designed to counteract failure due to CaP radioresistance, none of these trials have shown benefit in decreasing PCSM.8 The lack of an effect on survival with EBRT dose escalation can be explained by the fact that in a significant proportion of patients, treatment failure is due to the presence of occult systemic disease rather than local resistance and that these patients need to be treated with intensification of systemic therapy, not EBRT dose intensification, to decrease CaP mortality.1,8 Personalized CaP medicine, therefore, requires genomic- or biology-based biomarkers, in addition to existing clinical biomarkers, to explain interpatient heterogeneity in outcomes. Furthermore, even if an increased probability of occult metastases can be predicted, even more biomarkers will be required to favor the use of one systemic agent vs another, let alone the scheduling of these agents relative to each other. An additional complication to personalized medicine is the knowledge that many low-risk CaPs are indolent and that their overtreatment results in significant morbidity. Two-thirds of low-risk CaPs have an indolent course that can be followed without radical treatment when appropriately placed into AS protocols, thereby preventing the side effects and costs of RT or surgery. The corollary is that one-third of these low-risk patients are being inaccurately classified as having indolent cancers and require treatment.5 On an individual basis, there are no assays that can predict with confidence the need for therapy in low-risk CaP. So, how do we move forward in precision medicine for CaP using precision RT when faced with such clinical conundrums? One approach is to take advantage of technological advances in genomic medicine to determine patient-specific CaP genomics that reflect tumor progression and metastatic disease in addition to novel biology.12,13 State-of-the-art wholegenome sequencing technologies have the capacity for generating a breathtaking amount of genomic data (in excess of 10 billion bases per day) at a fraction of the cost than a decade ago. DNA- and RNA-based prognostic tests to predict CaP recurrence are being actively developed within the industry and academia for clinical use. Finally, there is also a rich history in radiation oncology for characterizing the tumor microenvironment, including assays for subregions of hypoxia within localized CaPs, which have a prognostic impact.
Approach And Future Aspects Of Curative Therapy
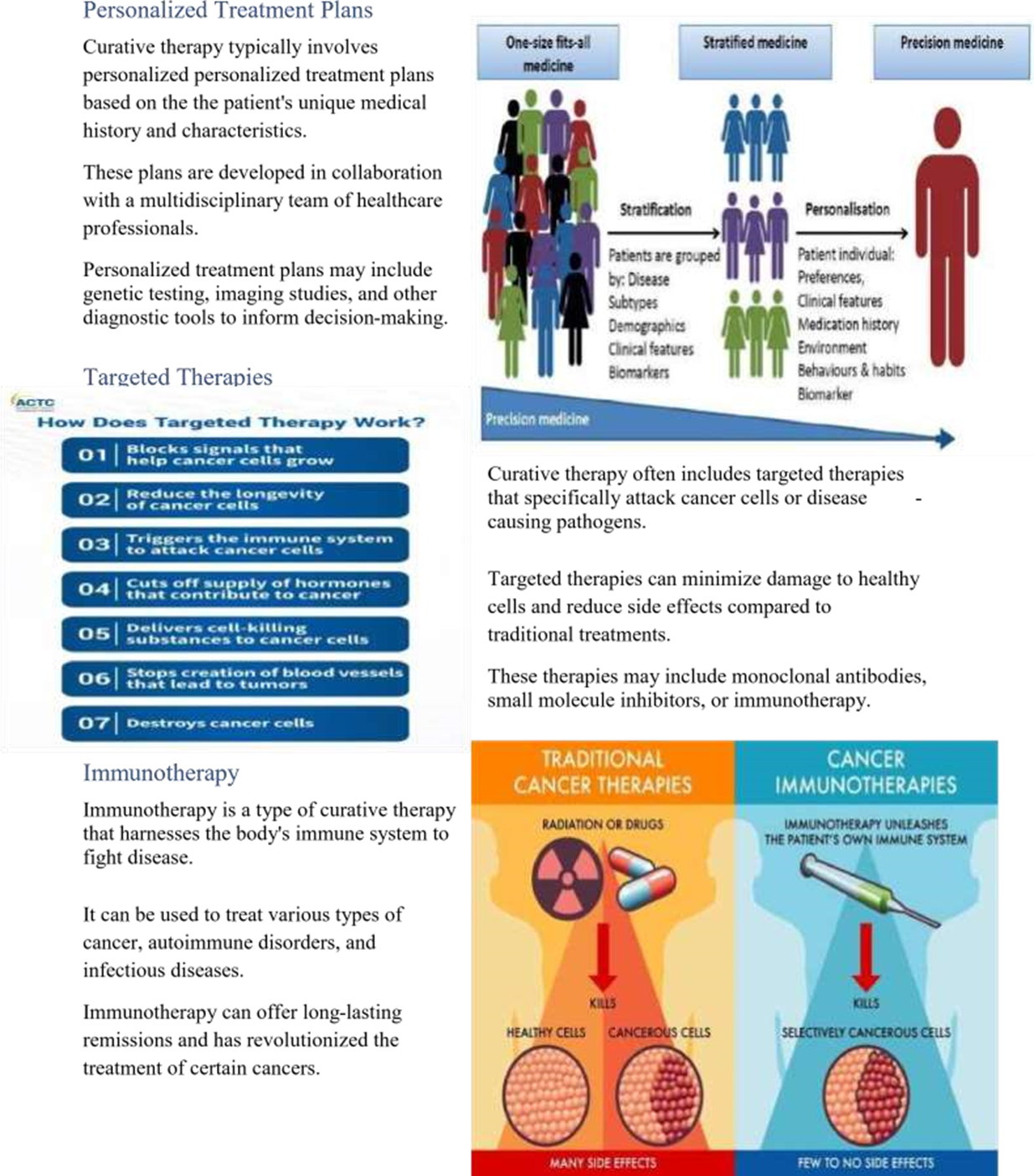
Introduction to Curative Therapy Curative therapy aims to eliminate or cure a disease or condition. It focuses on treating the root cause of the illness rather than just managing symptoms. The approach and features of curative therapy can vary depending on the specific disease or condition being treated.
Multimodal Approach
Curative therapy often involves a multimodal multimodal approach, combining different different treatments for optimal outcomes. outcomes. This may include surgery, medication, radiation therapy, and/or other interventions. The combination of treatments is tailored to the individual patient's needs and the specific characteristics of their condition.
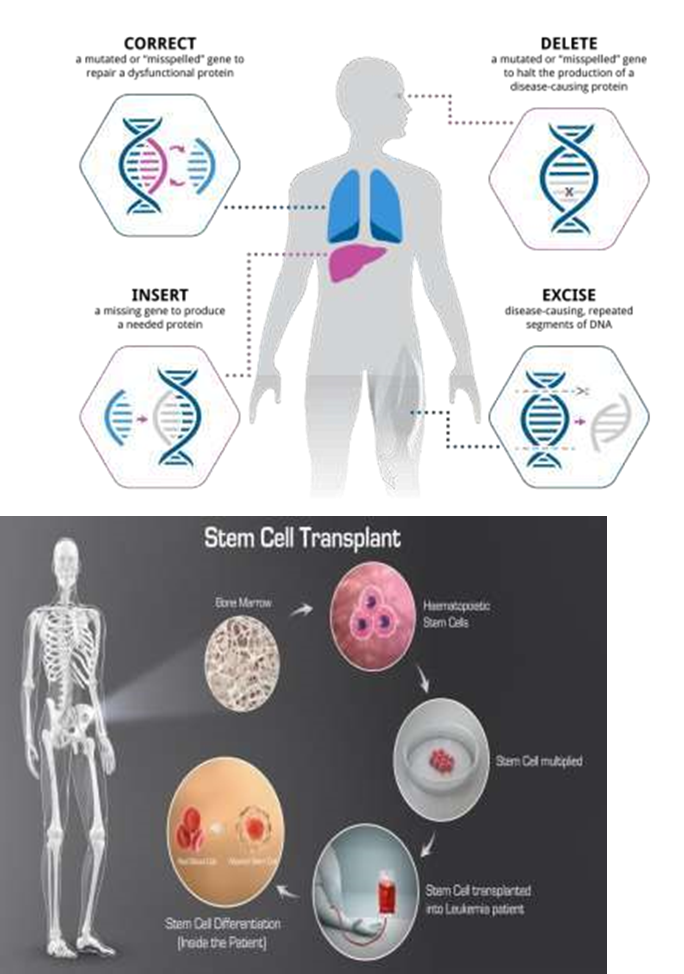
Gene Therapy
Gene therapy is a cutting-edge curative approach that aims to correct or replace faulty genes to treat genetic disorders.
It holds promise for treating conditions such as cystic fibrosis, muscular dystrophy, and certain types of cancer. Gene therapy is still in the early stages of development but shows great potential for the future of curative therapy.
Stem Cell Transplantation
Stem cell transplantation is a curative therapy used to treat conditions such as leukemia, lymphoma, and certain genetic disorders. It involves replacing damaged or diseased cells with healthy stem cells that can regenerate and restore normal function. Stem cell transplantation can offer a potential cure for some patients with otherwise incurable diseases.
Surgical Intervention
Surgery plays a crucial role in curative therapy for many conditions, including cancer, heart disease, and neurological disorders. Surgical interventions aim to remove tumors, repair damaged organs, or correct structural abnormalities. Advances in surgical techniques, such as minimally invasive procedures and robotic surgery, have improved outcomes and reduced recovery times.
Combination Therapies
Combining different modalities of curative therapy, such as surgery, chemotherapy, and radiation, can improve treatment efficacy. Combination therapies can target different aspects of the disease process and enhance overall treatment outcomes. A multidisciplinary approach is essential in coordinating and optimizing combination therapies for individual patients.

Monitoring and Follow-Up
Monitoring patients during and after curative therapy is crucial to assess treatment effectiveness and detect any potential complications.
Regular follow-up
appointments, imaging studies, and laboratory tests are used to track progress and ensure longterm success. Close collaboration between healthcare providers and patients is essential for ongoing monitoring and management of the disease.
.The latest evidence for possible HIV-1 curative strategies
Curative therapies (CTx) to achieve durable remission of HIV disease without the need for antiretroviral therapy (ART) are currently being explored. Our objective was to model the long?term health and cost outcomes of HIV in various countries, the impact of future CTx on those outcomes, and the country?specific value?based prices (VBPs) of CTx We developed a decision?analytic model to estimate the future health and economic impacts of a hypothetical CTx for HIV in countries with pre?existing access to ART (CTx+ART), compared to ART alone. We modeled populations in seven low- and middle-income countries and five high?income countries, accounting for localized ART and other HIV?related costs and calibrating variables for HIV epidemiology and ART uptake to reproduce historical HIV outcomes before projecting future outcomes to the year 2100. Health was quantified using disability?adjusted life?years (DALYs). For the base case, pessimistic and optimistic scenarios were modeled for CTx+ART and ART alone. Based on long?term outcomes and each country's estimated health opportunity cost, we calculated the country?specific VBP of CTx.The introduction of a hypothetical CTx lowered HIV prevalence and prevented future infections over time, which increased life?years, reduced the number of individual son ART, reduced AIDS?related deaths, and ultimately led to fewer DALYs versus AR alone. Our base case estimates for the VBP of CTx ranged from $5400 (Kenya) up to $812,300 (United States). Within each country, the VBP was driven to be greater primarily by lower ART coverage, lower HIV incidence and prevalence, and higher CTx cure probability. The VBP estimates were found to be greater in countries where HIV prevalence was higher, ART coverage was lower, and the health opportunity cost was greater. Our results quantify the VBP for future curative CTx that may apply in different countries and under different circumstances. With greater CTx cure probability, durability, and scale-up, CTx commands a higher VBP, while improvements in ART coverage may mitigate its value. Our framework can be utilized to estimate this cost given a wide range of scenarios related to the attributes of a given CTx as well as various parameters of the HIV epidemic within a given country.
8.The long?term impact and value of curative therapy [HIV: a modelling analysis]:-
Curative therapies (CTx) to achieve durable remission of HIV disease without the need for antiretroviral therapy (ART) are currently being explored. Our objective was to model the long?term health and cost outcomes of HIV in various countries, the impact of future CTx on those outcomes, and the country?specific value?based prices (VBPs) of CTx. We developed a decision?analytic model to estimate the future health economic impacts of a hypothetical CTx for HIV in countries with pre?existing access to ART (CTx+ART), compared to ART alone. We modeled populations in seven low- and middle-income countries and five high?income countries, accounting for localized ART and other HIV?related costs, and calibrating variables for HIV epidemiology and ART uptake to reproduce historical HIV outcomes before projecting future outcomes to the year 2100. Health was quantified using disability?adjusted life?years (DALYs). For the base case, pessimistic and optimistic scenarios were modeled for CTx+ART and ART alone. Based on long?term outcomes and each country's estimated health opportunity cost, we calculated the country?specific VBP of CTx. The introduction of a hypothetical CTx lowered HIV prevalence and prevented future infections over time, which increased life?years, reduced the number of individuals on ART, reduced AIDS?related deaths, and ultimately led to fewer DALYs versus ART?alone. Our base case estimates for the VBP of CTx ranged from $5400 (Kenya) up to $812,300 (United States). Within each country, the VBP was driven to be greater primarily by lower ART coverage, lower HIV incidence and prevalence, and higher CTx cure probability. The VBP estimates were found to be greater in countries where HIV prevalence was higher, ART coverage was lower, and the health opportunity cost was greater. Our results quantify the VBP for future curative CTx that may apply in different countries and under different circumstances. With greater CTx cure probability, durability, and scale-up, CTx commands a higher VBP, while improvements in ART coverage may mitigate its value. Our framework can be utilized to estimate this cost given a wide range of scenarios related to the attributes of a given CTx as well as various parameters of the HIV epidemic within a given country
9.METHODS
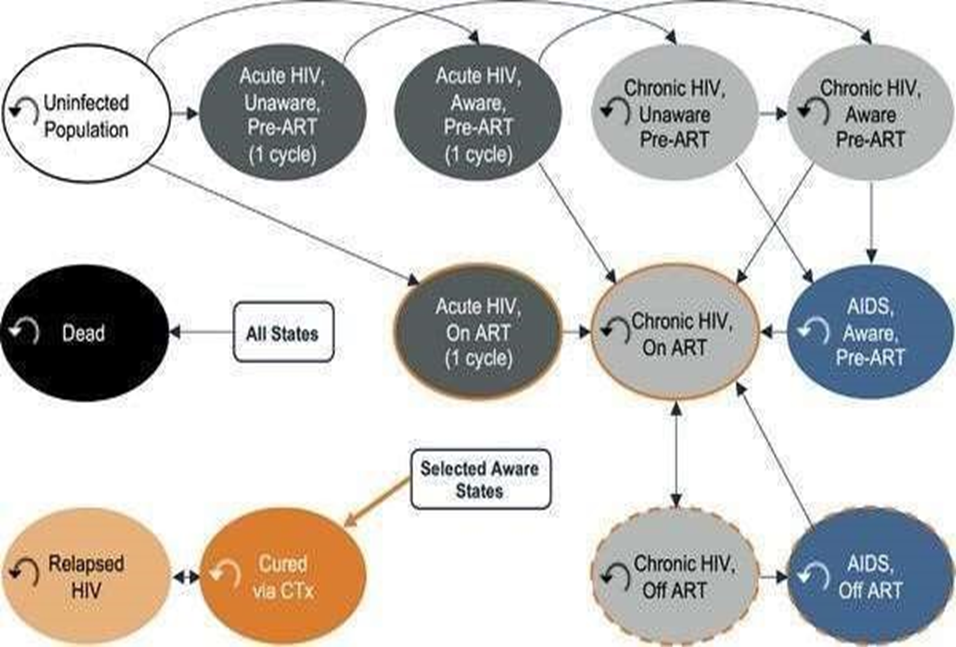
We developed an open cohort state?transition model, which (in contrast to closed cohort models) allows new individuals to enter the analysis in each model cycle to compare the introduction of a novel CTx for HIV in settings with pre?existing access to ART (CTx+ART) versus ART alone (Figure 1). The model was developed in Microsoft Excel and is Figure 3:
available for download here. All model parameter data were collected from October 2021 to July 2023 and can be found in the online Appendix Table A1, as well as citations within the model itself. We made assumptions where data were lacking and have documented these instances as such. We utilized a semi?annual model cycle duration and a healthcare payer perspective, and we discounted all future HIV?related costs and health outcomes by a constant 3% per year to reflect their present value.
Figreat
HIV state transition model. Individuals could transition from uninfected to an HIV health state or from one HIV health state to another. Individuals automatically transitioned from early HIV infection to chronic HIV after a single semi?annual model cycle. In the CTx+ART comparator arm, eligible individuals could receive CTx. As determined, however, by the modeled durability of the CTx cure, they could transition to a relapsed HIV health state with costs and disability weights equivalent to chronic HIV until they either received another CTx administration or died. Individuals could transition to death via AIDS?associated mortality or the background mortality of the modeled country. The model incorporates 2010–2021 UNAIDS HIV epidemiological estimates for each modeled country to “burn in” and extrapolate HIV epidemic levels until an assumed future CTx rollout. This process included calibration of ART? and disease stage?specific parameters to minimize the difference between the UNAIDS?reported HIV prevalence, incidence, and ART coverage between 2010 and 2021 per country and the respective analogous values in the model. Post?2021, the model then estimates the diverging (post?introduction of CTx in year x) trajectories of CTx+ART and ART alone until the year 2100 (the latest available year of US Census international population projections), for a total model time horizon of 90 years. The analysis concerned differences between comparators post?CTx rollout; prior to this rollout, the trajectories of the CTx+ART and ART alone comparators were equivalent. A 15? to 49?year?old population, for which HIV epidemiological statistics are widely available for each included country, entered the model in the year 2010. We did not explicitly model the sex distributions of the populations. Using a decision tree, individuals were distributed among health states in the first model cycle according to country?specific 2010 estimates of HIV prevalence and model?calibrated parameters. Most individuals entered the model in the uninfected health state; those already HIV positive entered the model with either early HIV (defined as CD4+ cell count of >500/μl of blood), chronic HIV (CD4+ 200–499/μl) or AIDS (CD4+ <200/μl). Individuals with HIV could be on or off ART based on country?specific estimates. In subsequent model cycles, new 15?year?olds entered the model, a small fraction of whom were HIV positive. Individuals could transition from uninfected to an HIV health state or from one HIV health state to another. Individuals automatically transitioned from early HIV infection to chronic HIV after a single semi?annual model cycle. In the CTx+ART comparator arm, eligible individuals could receive CTx. As determined, however, by the modeled durability of the CTx cure, they could transition to a relapsed HIV health state with costs and disability weights equivalent to chronic HIV until they either received another CTx administration or died. Individuals could transition to death via AIDS?associated mortality or the background mortality of the modeled country. The modeled population size and weighted age composite were based on population projections to the year 2100 derived from the international database tool provided by the US Census Bureau. All individuals entering the model each year were tracked until death or the end of the modeled time horizon.
Parameter calibration
For each country, we implemented a calibration process to derive estimates for unknown model parameters. We utilized an ordinary least squares approach wherein we minimized the sum of the squared residuals among UNAIDS?reported HIV prevalence, incidence, and ART coverage from 2010 to 2021 and the corresponding model?calculated outputs. Calibrated parameters included those for the levels of disease progression among affected individuals, time until HIV diagnosis, and ART uptake (post?diagnosis) and re?uptake (post?ART discontinuation) rates.
HIV incidence
The annual probability of HIV infection was dynamically imputed for each semi?annual model cycle using a constant, country?specific underlying risk of HIV transmission per person per unit (A) time, multiplied by a time?varying coefficient (B). The constant transmission risk for each country (A) was estimated from the proportion of individuals in each health state in the first model cycle, their respective relative risk of transmissions, and the incidence rate reported for that country in that year by UNAIDS. The dynamic force of infection coefficient was re?estimated in each model cycle from two sub?components: availability (linearly increasing per year) and efficacy of pre?exposure prophylaxis (PrEP) and condom usage, and the relative risks of transmission according to health state multiplied by the proportion of individuals in each health state. Thus, CTx and ART transition probabilities directly impacted force of infection calculations via the effect they have in moving individuals into health states with lower risk of mortality and of transmission. The relative risk of transmission was highest in early?stage individuals (26.0x) followed by those with AIDS (7.2x), chronic individuals who have discontinued ART (3.6x), chronic individuals who are on ART (0.08x) and chronic individuals yet to start ART were the reference relative risk (1x). Uninfected and CTxcured individuals were modeled as having a relative transmission risk of zero, while relapsed individuals were assumed to have a relative transmission risk equivalent to being on ART (0.08x).
Curative therapy
Presently, no CTx for HIV exists, and our conceptualization of a future CTx is intended to provide qualitative guidance for interested stakeholders. While we made no assumptions regarding the biological mechanism of the hypothetical CTx, we assumed in all modeled scenarios that it would be administered to age 15+ individuals with HIV infection as a single dose with a one?time cost and that successful CTx administration led to prompt ART?free suppression of HIV within 6 months. We further assumed that recipients of CTx who have not relapsed: (1) have equivalent quality of health to those in the uninfected population; (2) incur no additional ART cost; (3) are not infectious; (4) cannot be re?infected upon subsequent exposure to HIV [7]; and (5) that recipients of CTx who have relapsed have the same quality of health and infectiousness as those in the chronic HIV health state.
Curative therapy for gastric cancer
Gastric cancer (GC) is a major public health issue, and it is the fourth most common cancer and the second leading cause of cancer-related death[1]. It is usually diagnosed at an advanced stage, and consequently, the prognosis is dismal. Although surgery is the definitive therapy, rates of recurrence are high, creating the need for neoadjuvant or adjuvant therapy. These therapies have improved significantly the 5-year survival of these patients, but not all patients benefit equally from these treatment options. The ability to predict patient response to specific therapies would be particularly valuable and would allow for the stratification of patients for personalized treatment strategies, likely with less toxicity. Recent advances have improved our understanding of gastric carcinogenesis with an unprecedented opportunity of developing novel therapeutic strategies. Exploring and validating tissue-based biomarkers are ongoing processes that will certainly open new avenues for treating and improving the prognosis of patients with GC. RISK FACTORS FOR GC Like other human cancers, GC is the end result of the interplay of environmental and susceptibility factors. The striking geographic variation in GC incidence reflects the early role of environmental exposure rather than genetics, as migration studies have confirmed a decline in incidence in subsequent generations. The only environmental factor that is considered to be a type I carcinogen by the World Health Organization is Helicobacter pylori (H. pylori)[2]. This bacterium can have a lifelong uneventful relation with its host but, in a minority of cases, causes peptic ulcer, both intestinal and diffuse type gastric adenocarcinoma and gastric mucosa-associated lymphoid tissue (MALT) lymphoma. About 50% of the world’s population is infected with H. pylori, but less than 0.5% of infected individuals will develop GC. This disparity reflects the variation in the pathogenicity of bacterial strains as well as host inflammatory genetic susceptibility factors such as interleukin (IL)-1B, IL-8, IL-10, interferon. (IFN)-gamma, and tumor necrosis factor beta (TNF-β) polymorphisms[2]. H. pylori infection causes chronic inflammation, accumulation of reactive oxygen species (ROS), and oxidative damage in the gastric mucosa, thereby promoting the sequential progression of normal gastric epithelium through atrophic gastritis, intestinal metaplasia, and dysplasia to carcinoma. Advanced atrophic corpuspredominant gastritis and subsequent development of intestinal metaplasia provide the histological base for GC genesis[3]. This model of precancerous lesions is currently accepted, and surveillance recommendations apply to patients at increased risk[3]. The intestinal-type GCs are more related to atrophic gastritis, intestinal metaplasia, and dysplasia, but H. pylori infection is also associated with an increased risk of diffuse-type GC. In addition to H. pylori, dietary and lifestyle factors may also modify the risk of developing GC. Low socioeconomic status and associated conditions have been linked with a two-fold increase in GC risk[4]. Subjects belonging to a low socioeconomic status have a higher prevalence of H. pylori infection, more frequent smoking habits, and less vegetable and fruit intake than the general population[5]. In an analysis of the European Prospective Investigation into Cancer and Nutrition (EPIC-EURGAST), there was a 45% higher risk of GC associated with ever smoking compared to never smoking[6]. In a meta-analysis with 42 articles, Ladeiras-Lopes et al. [7] concluded that smoking is the most important behavioral risk factor for GC. Heavy alcohol intake has been linked to some increased GC risk, mainly in men[8]. Nonetheless, as heavy drinkers usually smoke and have a poor diet, there may be some confounding factors in these conclusions[4]. Among dietary factors, N-nitroso compounds (including nitrosamine) are proven animal carcinogens. Potential sources of N-nitroso compounds are beer, processed (smoked, cured, salted, and preserved) meats, red meat, and tobacco smoke[8]. In the EPIC cohort, the authors found no association between nitrites and nitrosodimethylamine intake and GC risk, but endogenous production of N-nitroso compounds was significantly associated with non-cardia cancer risk[9]. A meta-analysis in 2012, including 2076498 patients, showed a significant positive association between high salt intake and GC[10]. High salt intake damaged gastric mucosa and increased the susceptibility to carcinogenesis in studies with rodents. With respect to protective factors, intake of non-starchy vegetables and fruits has been associated with a moderately decreased risk of GC in many cohort-, population- and hospital-based case-control studies[4,5]. In a reanalysis of the EPIC cohort, a negative and significant association was observed between total vegetable, fruit, and flavonoid intake and dietary total antioxidant capacity and risk of GC[11-13]. This protection afforded by vegetables and fruits may derive from their content of antioxidants (such as vitamin C), which may reduce the formation of Nnitroso compounds in the stomach[5]. A recent large European prospective cohort study investigated the combined impact of the above-cited behaviors on GC risk using a healthy lifestyle index[14]. The authors concluded that adopting a combination of lifestyle behaviors, including not smoking, limiting alcohol consumption, following a healthy dietary pattern (represented by the Mediterranean diet), and having a normal body mass index, can dramatically decrease the burden of GC. In 2003, in a meta-analysis by Wang et al. [15] including 2831 GC patients, regular NSAIDs users had a reduced risk of GC (OR = 0.78, 95%CI: 0.69-0.87). These results have recently been confirmed in a wide systematic review[16]. The pro-apoptotic and antiangiogenesis effects of NSAIDs are known to inhibit carcinogenesis in patients with colonic polyps, and NSAIDs may act in a similar way in gastric mucosa[4]. To date, no randomized controlled studies exist on the long-term effect of NSAIDs alone on the development of GC, and the alleged protective effect could simply reflect the “protective user effect,” as most individuals eligible for sustained NSAID chemoprophylaxis do not usually suffer from the gastric disease. The decrease of distal GC prevalence that has been consistently described in a number of studies[17] could very well be the result of lifestyle changes associated with improvement of economic status, better hygiene, and consequent decrease of H. pylori infection.
10.Curing cancer - Curative cancer treatment based on complexity theory
Network medicine. Adult cancer, which accounts for almost all cancer deaths, is a systemic disease. It arises from and is maintained due to dysfunctional cellular networks, not just mutated genes in a simple pathway. A network is a complex set of interactions, or relationships, between different entities. By contrast, a simple pathway is a linear process with changes that occur one step at a time (e.g., an assembly line). Scientists often think about biological pathways as a circular assembly line with small changes at each step until the pathway's function is completed, such as activating an enzyme; then, the pathway begins again.
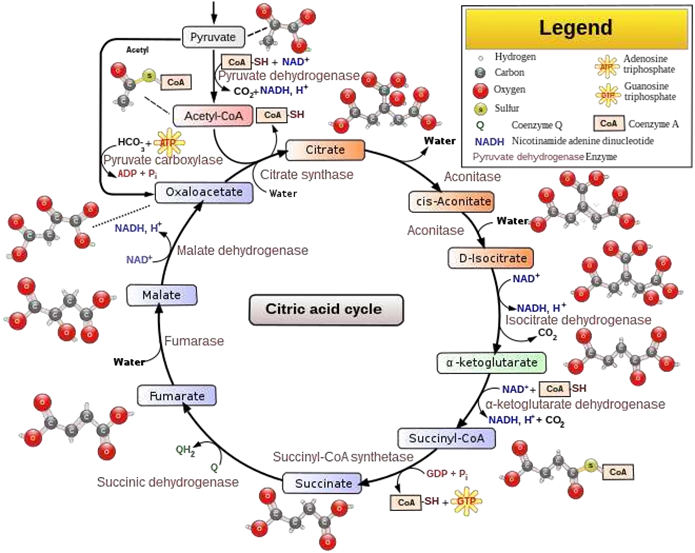
Figure 4. Citric Acid Circle
In contrast, complex biological pathways, such as those related to cell division, interact with each other at many steps, resembling sets of intersecting circles forming a three-dimensional web of pathways that, when viewed as a whole, may perform a higher level function.
Figure 5.
Advanced disease in adults may begin with simple changes, but large cancers are sustained by years or decades of supportive network changes throughout the body, which is called altered systems biology. These systemic changes typically will not revert to normal even if a substantial number of cancer cells are destroyed. Thus, a focus on "network medicine" is mandatory. Kill as many cancer cells as possible. High cancer cell killing is important because (a) cancer cells directly damage normal cells, tissue, and organ systems, interfering with their physiologic functions, which maintain life; (b) cancer cells create an increased workload, both by producing biological substances that interfere with optimal physiology and by stimulating a response to destroy them; and (c) cancer cells have molecular heterogeneity so the death of any cancer cell may also destroy a different strategy of the cancer cell and its progeny to overcome the body's anticancer defences. Block multiple pathways and block each pathway at multiple points. We have cured some cancers in children and young adults, including childhood leukemia, Hodgkin lymphoma, and testicular cancer. These cancers are caused by inherited or constitutional cancer predisposition or developmental mutations and exhibit a limited number of somatic (acquired) cancer mutations. However, single therapies are not curative. In the 1940s, Dr. Sidney Farber, a Harvard pathologist, gave his childhood leukemia patients a new drug, aminopterin, which blocked the effect of folic acid, which is needed for cells to divide, accessed 31 May 22). Amazingly, these children, who usually died within weeks of diagnosis, went into remission. But their cancer soon became resistant to treatment, and the children relapsed. We now know that it may take 3-5 drugs with different mechanisms of action to create enough blocks to completely disable these cancer cell networks in children. Disabling the activity of dysfunctional networks often requires drug combinations due to the weblike interaction of networks that can readily bypass a single block in a particular pathway. In addition, some treatments do not work for some patients. Curing adult cancers may require even more treatment diversity due to (a) their complex and heterogeneous mutational landscape, (b) the field effects generated by cancer promoters/risk factors acting over decades of exposure, and (c) associated systemic network changes that must also be addressed by treatment. Although drug combinations are typically more effective than single agents, determining which combinations are most effective is time-consuming. However, "deep learning" and other computational approaches and modeling methods may help screen possible combinations for effectiveness. Combining different types of therapy may also be effective; for example, regional hyperthermia may kill therapy-resistant cancer stem cells, be synergistic with immune checkpoint inhibitors, and improve survival.
Combinations of combinations of treatment. Since adult cancers are due to dysfunction in many key systemic networks (see below), with each often requiring a different set of combinatorial therapies, curative therapy may require combinations of combinations of treatment to adequately alter these networks. We speculate that for each cancer type, even the most aggressive, there exists a combination of 8-10 therapies that individually may be only partially effective but together can be substantially effective. However, determining the optimal combinations will be difficult.
Move local cancer cell networks into less lethal states. Curative treatment, in addition to killing large numbers of cancer cells through multiple mechanisms, should "normalize" or reduce the malignant traits of cancer cells that survive. Fifty years ago, Kauffman discovered that a complex network of thousands of mutually regulating genes in normal cells might produce a stable equilibrium state called an attractor that corresponds to gene expression profiles specific to each cell type. Essentially, the environment of biological substances, when together, forces them to have a limited behavior even though they behave very differently when isolated. Attractors have been analogized to a low energy state or valley on a topographic diagram that pulls in cells with similar network configurations, see diagrams at. By targeting inflammation, the vasculature, stroma, and extracellular matrix. For example, antiVEGF or anti-VEGF receptor treatment can normalize vasculature by reducing vascular permeability. Normalizing the microenvironment may also enhance drug delivery and effectiveness or make existing cancers or premalignant states more susceptible to immune system attack. Repair immune system dysfunction that coevolves with carcinogenesis. The immune system consists of a web of interacting networks whose effectiveness is systematically degraded with malignant progression.
Immune dysfunction in cancer is typically not just the failure of one particular pathway. Curative treatment should attempt to improve immune system function with combinatorial therapy that targets multiple aspects of immune dysfunction.
Antagonize hormonal expression that promotes cancer cell growth. Physiologic
(i.e., normal) levels of estrogens and androgens and elevated levels of insulin are associated with breast, endometrial/uterine, prostate, and pancreatic cancer. The primary mechanism may involve the promotion of cell growth at a stage when these cells are particularly vulnerable to instability. Simple antagonism of hormonal pathways is possible using tamoxifen for estrogens, antiandrogens for testosterone, and metformin for insulin. One block in these hormonal networks is apparently adequate for normalization, in contrast to the 3-5 blocks required for other cancer cell networks. Behavioral changes, such as weight loss, exercise, a healthier diet, and reducing alcohol and tobacco use may also be therapeutic by either altering hormone levels or changing their interaction with other risk factors.
11. Investigate attacking global changes of cancer cells:
(a) Promote the activation of gene networks that support stable, multicellular processes and suppress networks that promote unicellular processes that enable malignant type behavior. Multicellular organisms evolved from unicellular organisms by adding new genes and more intricate controls to existing networks for metabolism and replication. This enables greater communication and coordination between cells and makes possible higher level functions, such as cell differentiation and programmed cell death. The new control mechanisms keep cellular and systemic processes on track and shift the survival focus from individual cells toward the organism as a whole. The operation of multicellular and unicellular programs appears to be somewhat mutually exclusive. Inflammation and DNA alterations may damage these multicellular controls, activating the existing genetic toolkit of preprogrammed, malignant behavior in unicellular networks based on what has been described as the atavism hypothesis of cancer. Theoretically, it should be possible to shift the balance towards the promotion of the multicellular networks and repression of the unicellular networks
Repress epithelial-mesenchymal transition, a common mechanism of malignancy. Epithelialmesenchymal transition (EMT) is a physiological process in which epithelial cells attain the properties of mesenchymal cells, both morphologically (in appearance) and physiologically (in function). Since EMT plays an important role in tumor progression through metastasis, apoptotic resistance, and immune evasion, repressing EMT may be important for curative therapy.
b)Target the weaknesses of cancer cells by applying specific cellular stress that is readily dealt with by healthy cells using evolved capabilities or multicellular programming but not by cancer cells with predominantly unicellular programming. This includes "lethal challenges" of high-dose methotrexate with leucovorin rescue or targeting other aspects of chaotic or unstable states, such as cellextracellular matrix detachment.
Antagonize inherited genetic changes that promote malignant behavior.
Genetic testing of noncancer cells (germline testing) is recommended for all patients with pancreatic cancer and select patients with other cancers or family histories of cancer. Results are currently used to determine anticancer therapy as well as for cancer screenings, reproductive choices, and genetic counseling. We suggest using these results also to provide treatment that moves premalignant or malignant cells into less harmful pathways as discussed above or to counter common germline changes in inflammation, DNA repair, cell cycle stability, immune system function, or other networks that promote malignancy.
Focus on reducing death and disability and not necessarily killing every cancer cell.
Although killing every cancer cell is important for curing placental choriocarcinoma, and as discussed in this may not be an appropriate treatment goal for all adult tumors, some patients may benefit from strategies of cancer growth containment rather than eradication. It may also be important to achieve "marginal gains" at all steps of the disease process by optimizing specific aspects of care, even if minor, such as reducing perioperative morbidity, improving management of jaundice, and addressing malnutrition. These small efforts may aggregate to produce substantial improvements, leading to additional treatment options and a reduction in the sense of futility that may promote death. We should also study whether guiding therapy based on patient preference, to the extent possible, reduces cancer death.
Monitoring key networks.
To optimize treatment, it may be important to monitor the status of key networks as treatment is given, including the inflammatory process in general, the immune system's anticancer capabilities, different aspects of the cancer microenvironment, embryonic networks that promote lack of cell differentiation, hormonal expression that promotes cancer cell growth and inherited changes that promote malignant behavior. For each of these networks, we must determine which biological molecules to monitor, how best to do so, how changes in their expression affect treatment, and how these values will impact long-term survival rates.
12.Early cancer deaths.
We should identify key physiologic networks disturbed in early cancer death and develop treatment strategies to rapidly normalize them and prevent death. Once these physiologic networks are stabilized, the underlying cancer can then be treated.
13.Clinical trials.
Every cancer patient should be enrolled in a clinical trial, if possible. These trials are needed to determine (a) the effectiveness of individual treatments, combinations of treatments, and combinations of combinations of treatments, (b) long-term survival rates, (c) how to reduce side effects, and (d) what adjustments to make for particular patients.
14.Public health and preventative programs.
Government at all levels, the private sector, and nonprofits should promote a culture of healthy living and low cancer risk that includes reducing tobacco use, excess weight, and alcohol abuse, encouraging a healthy diet and exercise, and obtaining appropriate medical care and vaccinations.
CONCLUSION:
Our results quantify the VBP for future curative CTx that may apply in different countries and under different circumstances. With greater CTx cure probability, durability and scale up, CTx commands a higher VBP, while improvements in ART coverage may mitigate its value. Our framework can be utilized for estimating this cost given a wide range of scenarios related to the attributes of a given CTx as well as various parameters of the HIV epidemic within a given country.
REFERENCES

Himanshi Shrivastava*, Priyal Jain, Dr. Jitendra Banweer, Curative Therapy: Impact on Family Care and Society, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 5, 3372-3395. https://doi.org/10.5281/zenodo.15472421
 10.5281/zenodo.15472421
10.5281/zenodo.15472421
