Bharat Institute of Technology- Pharmacy, Mangalpally, Hyderabad, Telangana
A common antiepileptic and mood stabilizer, carbamazepine is used to treat bipolar affective disorder, trigeminal neuralgia, and seizure disorders. Despite its effectiveness, carbamazepine has been linked to toxic epidermal necrolysis (TEN) and Stevens-Johnson syndrome (SJS), two uncommon but serious cutaneous adverse drug reactions. Skin detachment, mucosal involvement, and extensive epidermal necrosis are the hallmarks of SJS, a potentially fatal mucocutaneous disease. It is thought that the pathogenesis entails a delayed-type hypersensitivity reaction that is mediated by cytotoxic T lymphocytes and is frequently linked to specific HLA genotypes, specifically HLA-B and HLA-A
Carbamazepine belongs to the class of anti-seizure drugs. Brand name of carbamazepine is Tigretol, used in treating epilepsy, neuropathic pain resulting from trigeminal neuralgia. Carbamazepine is a GABA (gamma amino butyric acid) agonist. Brain contains a large electrical network. These neurons communicate with each other through electrical signals. In an abnormal condition, the neurons produce electrical signals in a very fast and rapid way. Sodium channels are present in neurons which control the flow of electrical signals. During seizures and other conditions sodium voltage gated channels open and close too often causing overload to neurons. Carbamazepine blocks the activity of Na+ at sodium voltage gated channels in the neurons which then helps in controlling seizures. [1,2]
Carbamazepine
PHARMACOKINETICS
ABSORPTION
Carbamazepine has a bioavailability of 75–85% of the dose that is consumed.3. In a pharmacokinetic study, the Cmax carbamazepine was found to be 1.9 ± 0.3 mcg/mL following a single 200 mg oral extended-release dose. A Tmax of 19 ± 7 hours was recorded. Peak levels of carbamazepine were found to be 11.0 ± 2.5 mcg/mL following multiple doses of 800 mg every 12 hours. They lowered the Tmax to 5.9 ± 1.8 hours. Over a 200–800 mg range, extended-release carbamazepine showed linear pharmacokinetics. [3-8]
DISTRIBUTION
One pharmacokinetic study determined that the volume of distribution of carbamazepine was 1.0 L/kg. According to a different study, carbamazepine's volume of distribution falls between 0.7 and 1.4 L/kg. Unlike lung and brain tissue, carbamazepine is found in higher concentrations in the liver and kidney after crossing the placenta. The way carbamazepine passes through the blood-brain barrier varies. [3-8]
METABOLISM
The liver is where carbamazepine is mostly metabolized. The primary liver enzyme responsible for breaking down carbamazepine into its active metabolite, carbamazepine-10,11-epoxide12, is CYP3A4. Epoxide hydrolase then breaks it down into its trans-diol form. 16 CYP2C8, CYP3A5, and CYP2B6 are additional hepatic cytochrome enzymes that aid in the metabolism of carbamazepine. 17 Additionally, the UGT2B7 enzyme hepatically glucuronidases carbamazepine, and a number of other metabolic processes take place, leading to the production of quinone and minor hydroxy metabolites. 17 It's interesting to note that carbamazepine triggers its metabolism. [3-8]
ELIMINATION
Following an oral dose of radio-labelled carbamazepine, the urine contained 72% of the administered radioactive dose while the faeces contained the remaining portion. The majority of carbamazepine's excretion consists of conjugated and hydroxylated metabolites, with trace amounts of the original medication. [3-8]
PHARMACODYNAMICS
The main characteristic of carbamazepine's pharmacodynamics is that it functions as a voltage-gated sodium channel blocker, stabilizing neuronal membranes by stopping action potentials from firing repeatedly. By attaching itself to sodium channels that are not in use, it lowers neuronal excitability and, consequently, synaptic transmission. Additional effects include effects on neurotransmitter systems (serotonin and noradrenaline), possible modulation of other ion channels (such as calcium), and effects on the release of antidiuretic hormones. [9]
DOSE
ADVERSE DRUG REACTION
Fatigue, drowsiness, dizziness, vomiting and feeling queasy, loss of coordination, unsteadiness (ataxia), mouth dryness, headache, gaining weight, Painful, red or purple rash that spreads and blisters, Skin that peels off, Sores in your mouth, nose, genitals, Flu-like symptoms, including fever, Swelling of the face, eyes, tongue. Damage to the liver; serious liver damage manifests as jaundice, yellowing of the skin or eyes, either light coloured stools or dark urine, our stomach's right-side hurts.
Severe Skin Reactions - These can be life-threatening and include Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN). [11]
ALTERNATIVES TO CARBAMAZEPINE
Other medications are used to treat severe pain, neuralgia, epilepsy with less adverse drug reactions and safer than carbamazepine. Few of those drugs are gabapentin, oxcarbazepine, lamotrigine, zonisamide, valproate, topiramate etc.
Gabapentin: It belongs to the class anticonvulsants, which has structure similar to GABA (gamma aminobutyric acid). Gabapentin appears to block release of excitatory neurotransmitters in the presynaptic region by showing a strong affinity for binding sites throughout the brain that correspond to the presence of voltage-gated calcium channels.[12]
Lamotrigine: It belongs to anticonvulsants class of drug. Used as a second-line drug in treating seizures and also acts as mood stabiliser. It inhibits sodium voltage gated channels there by decreases neuronal excitability and seizures. It reduces the release of glutamate, a chemical that can overstimulate the brain if there’s too much of it. By keeping glutamate in check, lamotrigine may also help stabilize mood, especially in bipolar disorder particularly by preventing the low, depressive episodes.[13]
Oxcarbazepine: oxcarbazepine and gabapentin both belongs to the same class anticonvulsant. Oxcarbazepine shares similar mechanism of gabapentin, blocks voltage gated sodium channels.[14]
Valproate: Valproate acts in different mechanism like inhibiting GABA receptors, blocking voltage gated sodium channels, altering other genes and etc., which will eventually regulate neuronal excitability.[15]
Gabapentin
Lamotrigine
Oxcarbazepine
Valproate
STEVENS – JOHNSON SYNDROME
A flu infection and a few medications are the main causes of Stevens-Johnson syndrome, an allergic reaction. The skin is affected by this potentially fatal condition. Stevens-Johnson Syndrome (SJS) as an extreme, runaway allergic reaction that severely damages your skin and the moist linings (mucous membranes) of your body. A fast emergency treatment is required as it spreads rapidly and damages mucous and skin membranes. The syndrome stevens-Johnson is also known by terms like Lyell’s syndrome, toxic epidermal necrolysis, drug – induced SJS, mycoplasma – induced SJS, erythema multiforme exudative. toxic epidermal necrolysis spectrum. [16,17]
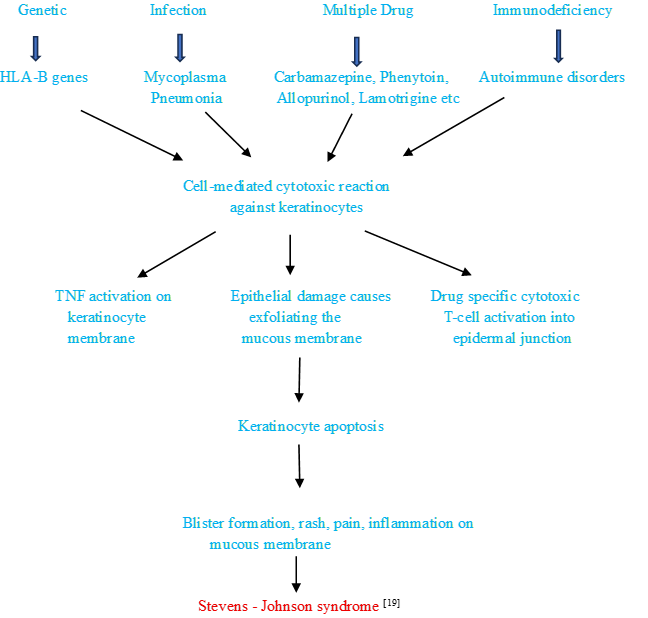
ETIOLOGY
PATHOPHYSIOLOGY
SYMPTOMS
Blisters that hurt, facial, lip, and throat swelling, vision issues, genital sores, and hypersensitivity reactions, sores in the mucous membranes, drooling, painful urination. [20]
DIAGNOSIS
Appearance of blisters on mucous membrane, pinkish- red colored sores.
Skin removal or peeling of skin, rashes, exfoliation of skin cells.
Medication history, other comorbidities
Presence of HLA-B genes
A small sample of skin is taken and examined under a microscope. The definitive histopathological finding in SJS is full-thickness epidermal necrosis (death of skin cells) with minimal inflammatory infiltrate.
A second skin biopsy may be taken for direct immunofluorescence testing. The results are typically negative, which helps differentiate SJS from other autoimmune blistering diseases like pemphigus.
Blood tests can find out abnormalities in any parameters of blood.
This test can determine the spread and strains of bacteria in the body as well as the presence of Mycoplasma pneumonia bacteria. [21]
MANAGEMENT
NON-PHARMACOLOGICAL THERAPY
PHARMACOLOGICAL THERAPY
Especially in the early stages of the disease, corticosteroids are used to suppress the overactive immune response that causes SJS. Their use is debatable, though, as some studies indicate early high-dose therapy may improve outcomes while others report no mortality benefit and an elevated risk of infection.
This treatment blocks the mechanisms that lead to widespread skin cell death by using antibodies from healthy donors. Studies on its effect on mortality have produced conflicting findings, and its efficacy is debatable.
TNF inhibitors such as infliximab and etanercept: Tumor necrosis factor-alpha (TNF-(alpha)), a protein implicated in skin cell inflammation and apoptosis (cell death), is the target of these biological medications. Larger-scale trials are required, but research in this area is just getting started, and some studies indicate they might be helpful.
Cyclosporin is an immunosuppressant which inhibits T-cells activation on skin cell.
This technique purges the blood of inflammatory substances and medication metabolites that might be contributing to the reaction. Plasmapheresis is a technique which purifies chemicals from the blood, also known as therapeutic plasma exchange technique. [23,24]
SUPPORTIVE THERAPY
NSAIDS and other painkillers are used to decrease pain at the effected regions on skin upon their peeling.
Eg: Acetaminophen
Corticosteroids used to reduce inflammation and redness of blisters on skin or mucous membrane.
Eg: Methylprednisolone, Prednisone.
Lubricant eyedrops containing corticosteroids, heparin eyedrops, cyclosporin eyedrops are used to protect from further reaction and protect the ocular surface and infections caused in the eyes.
Other medications include antacids, anticoagulant’s etc.,[25]
CASE DISCUSSION
A patient of 55 yrs female has admitted in medical department with the chief complaints of seizure activity at home – 3 episodes at 11;30 am lasting for 1 min and tongue bite, post-ictal status. Patient has a known history of seizure disorder since 2 yrs, not on medications. History of present illness is nausea sensation in the last 4 days, giddiness and sudden fall, there might be denova hypertension and denova diabetes mellitus type-2.
Past medical history (RX) was on anti-epileptic drugs but discontinued due to skin allergic reaction to carbamazepine 2 yrs ago. From then the patient was not on any medications.
Now the patient has admitted for further treatment, on examination the patient is conscious and coherent and Temperature – 98oF, Pulse rate -79 bpm, Blood pressure – 170/100mmHg, SPO2 -90% @RA, GRBS - 309mg/dl.
On 01/06/2025 the patients
Vitals of the patients were abnormal with blood pressure – 170/100mmHg, GRBS – 309mg/dl. Laboratory investigations were normal and advised for CT brain, MRI brain, 2DECHO. The drugs prescribed and given to the patient are INJ. PAN – 40mg, INJ. ZOFER – 4mg, INJ. PCM – 1gm, INJ. MANNITOL – 100ml, INJ. LEVIPIL – 500mg, TAB. NICARDIA – 10mg, INJ.MONOCEF – 1gm, INJ.OPTINEURON – 1 amp, TAB- QUIETIAPINE – 25mg.
On 02/06/2025 the patients
Vitals of the patient on second day with blood pressure – 150/70mmHg, GRBS – 145 mg/dl, Patient is highly irritable, post-ictal confusion. Glassgow coma scale (GCS) shows E3, V5, M6. Laboratory findings were normal. Reports of CT BRAIN gives right frontal bleed indicating intracranial frontal bleed, MRI BRAIN reports for the patient with hemorrhage location on right frontal region, 2DECHO reports are concentric LVH, NO LVRWMA, grade-2 DD, NO clot/VGH, ICV – normal. Same medications are followed and Betadine mouth wash.
On 03/06/2025 the patients
Vitals of patient on third day with blood pressure – 130/80 mmHg, GRBS -152 mg/dl. Continued same treatment. No abnormalities detected.
On 04/06/2025 the patients
Vitals of the patient on fourth day with blood pressure – 110/70 mmHg, GRBS – 141 mg/dl. Continued same treatment with addition of ZYLE GEL for oral application, removal of INJ.MANNITOL – 100ml.
On 05/06/2025 the patients
Vitals are blood pressure – 130/80 mmHg. Continued same treatment with the addition of TAB. V TOTAL women and the patient was not willing for further MRI + ANGINA SCAN + MRV examination.
CONCLUSION
The patient of 55 yrs female has diagnosed with seizure disorder, Intracranial bleed on right frontal region, Denova Hypertension, Denova diabetes mellitus type-2, Drug allergic to carbamazepine- Stevens-Johnson syndrome. Seizure disorder and abnormal eye movement are controlled by the drug LEVIPIL and QUITIAPINE. Patient had previously experienced allergic reaction, which is stevens-Johnson syndrome to carbamazepine but no allergic reaction found after discontinuation of drug.
ACKNOWLEDGMENTS
The authors would like to acknowledge the facilities provided by the Bharat Institutions- pharmacy in executing this article.
REFERENCE


Jarupla Mahika, Vangoori Tejaswi, Carbamazepine Induced Allergic Reaction; Stevens-Johnsons Syndrome, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 1435-1443. https://doi.org/10.5281/zenodo.17572508
 10.5281/zenodo.17572508
10.5281/zenodo.17572508
