Vishnu Institute of Pharmaceutical Education and Research (VIPER), Narsapur, 502313, Medak, Telangana
Recurrent aphthous stomatitis (RAS), or aphthous ulcers, is a common chronic inflammatory mucosal oral disease in about 20% of the world's population. RAS has three subtypes that are seen clinically: minor ulcers (most common, shallow and <10 mm in diameter), major ulcers (larger, deeper, and longer in duration with scarring capability), and herpetiform ulcers (many small group lesions). Although self-limiting in most cases, RAS considerably interferes with the quality of life of patients with severe pain, dysphagia, and frequent relapses, sometimes requiring medical treatment. The exact etiology of RAS is still multifactorial and not yet completely elucidated. Nevertheless, current data emphasize an immune-dysregulatory central role in its pathogenesis. An overactive T-cell-mediated immune response—a Th1/Th17-predominant cytokine environment—facilitates mucosal damage. Dysregulated innate immunity, oxidative damage, and compromised epithelial antioxidant defenses concomitantly enhance tissue damage. Genetic predisposition, particularly HLA polymorphisms, in addition to microbiome dysbiosis and environmental stimuli like stress, nutritional deficiencies, and hormonal changes, are precipitating factors. Clinically, RAS is not just restricted to localized oral findings but can also be an indicator of systemic illnesses like Behçet's disease, inflammatory bowel disease, celiac disease, or HIV infection. Newer management options include topical corticosteroids, antimicrobial mouthwashes, lasers, and nutraceuticals such as probiotics and vitamins. For severe or refractory conditions, systemic immunomodulators and biologics against TNF-? and IL pathways have been promising. In spite of these advances, present treatment is still mostly symptomatic and non-curative. There is a real need for extensive immunophenotyping to stratify patients and allow personalized therapeutic schemes. Future research must focus on clarifying molecular biomarkers, microbiota-host immune interactions, and precision-targeted biologic development for long-term disease modulation.
Recurrent aphthous stomatitis (RAS), commonly known as aphthous ulcer, is the most frequent chronic inflammatory disorder affecting the oral mucosa. It is characterized by the repeated emergence of painful, round or oval, shallow ulcers with erythematous halos. These lesions typically manifest on non-keratinized mucosal surfaces such as the inner lips, cheeks, floor of the mouth, soft palate, and the underside of the tongue, while sparing keratinized regions like the hard palate and gingiva. RAS is non-contagious, self-limiting, and predominantly idiopathic, although in some instances it may be indicative of underlying systemic conditions. Clinically, RAS is classified into three main subtypes based on the size, number, duration, and healing characteristics of the ulcers[1]. Minor RAS, the most common form, accounts for about 80–85% of cases and presents with small (<10 mm), shallow, round or oval ulcers that typically heal within 7–14 days without scarring. Major RAS, also known as Sutton’s disease, involves larger (>10 mm), deeper ulcers that may persist for 2–6 weeks and often heal with scarring, sometimes forming extensive necrotic areas. Herpetiform RAS, despite its name, is unrelated to herpes simplex virus and presents as clusters of numerous (10–100) small (1–3 mm) ulcers that can coalesce, making it the most painful and recurrent but least common variant.
1.1. Epidemiology and Demographics
RAS affects approximately 20–25% of the global population, although prevalence varies geographically, with higher incidence reported in high-income countries. It most commonly presents in childhood or adolescence, with peak onset between the 2nd and 3rd decades of life. In most individuals, the condition becomes less severe or resolves with age, but 5–10% may experience persistent or severe recurrences into adulthood[2].
The disease shows no consistent sex predilection, though some studies suggest a slightly higher frequency in females, possibly due to hormonal influences. RAS occurs across all ethnicities but is more prevalent in individuals of European and North African descent compared to East Asian populations.
1.2. Clinical Impact and Significance
Although RAS is not life-threatening, its clinical burden is substantial, especially in patients with frequent or severe episodes. The lesions are often painful, particularly during eating, speaking, swallowing, or oral hygiene, significantly impairing oral function. In children, this may result in avoidance of food intake, leading to weight loss, malnutrition, and psychosocial withdrawal. The pain intensity, combined with ulcer recurrence, negatively affects oral health-related quality of life (OHRQoL). Recurrent flares may also disrupt sleep, reduce concentration, and contribute to emotional stress or anxiety. In some cases, patients may self-medicate or overuse topical corticosteroids, risking mucosal thinning or secondary infections.
1.3. Etiopathogenesis: Multifactorial Origins
The pathogenesis of RAS is multifactorial and not yet completely understood. However, it is believed to result from a complex interplay between genetic susceptibility, immune dysregulation, mucosal barrier defects, and environmental triggers.
1.3.1 Genetic Predisposition
There is strong evidence supporting a heritable component in RAS. Studies report familial aggregation in up to 40–50% of patients, and monozygotic twins show a higher concordance than dizygotic twins. HLA associations have been implicated, particularly HLA-B12, HLA-B51, HLA-DR2, and HLA-Cw7, although these vary across populations. Genome-wide association studies (GWAS) and candidate gene analyses have also identified polymorphisms in TNF-α, IL-1β, IL-10, NOD2, and TLR4 genes that may influence susceptibility or severity[3].
1.3.2 Nutritional Deficiencies
Deficiencies in iron, vitamin B12, folic acid, and zinc have been associated with the onset and recurrence of aphthous ulcers. These micronutrients play critical roles in epithelial integrity, immune regulation, and oxidative stress defense. For instance, B12 deficiency impairs DNA synthesis and epithelial repair, while zinc is essential for wound healing and T-cell function[4].
1.3.3 Local Trauma and Irritants
Even minor mucosal injuries—such as those from orthodontic appliances, rough brushing, or accidental biting—can precipitate ulceration in susceptible individuals. The use of toothpaste containing sodium lauryl sulfate (SLS), a common foaming agent, has been shown to delay healing and increase recurrence due to its mucosa-drying and desquamating effects[5].
1.3.4 Hormonal Influences
Hormonal fluctuations, particularly those associated with the menstrual cycle, pregnancy, or oral contraceptive use, may influence ulcer frequency and severity. Estrogen and progesterone are known to affect vascular permeability and mucosal immune cell profiles, possibly modulating mucosal inflammation[6].
1.3.5 Psychological Stress
Psychological stress is a well-established trigger for RAS. Elevated levels of cortisol, a stress hormone, can suppress mucosal immunity, reduce salivary IgA, and impair epithelial regeneration, increasing susceptibility to ulcer formation[7]. Additionally, stress may also alter the oral microbiota and promote behavioral changes (e.g., lip biting, poor diet) that contribute to ulcer onset.
1.3.6 Microbiota Dysbiosis
Recent advances in oral microbiome research suggest that dysbiosis plays a role in RAS pathogenesis. Patients exhibit reduced microbial diversity, depletion of beneficial species such as Streptococcus salivarius, and enrichment of opportunistic bacteria like Acinetobacter johnsonii and Pseudomonas spp. These changes may disrupt mucosal homeostasis and trigger immune activation through pathogen-associated molecular patterns (PAMPs) and TLR signaling pathways[8].
1.3.7 Immunological Mechanisms
A key hypothesis in RAS pathogenesis is that it results from a dysregulated T-cell-mediated immune response. Lesions show increased infiltration of CD8+ cytotoxic T cells, Th1 cytokines (e.g., IFN-γ, TNF-α), and reduced levels of regulatory T cells (Tregs) and anti-inflammatory cytokines (e.g., IL-10)[9]. The result is mucosal damage and delayed re-epithelialization. The involvement of Th17 responses and IL-22 in recent studies suggests even broader immune involvement than previously appreciated.
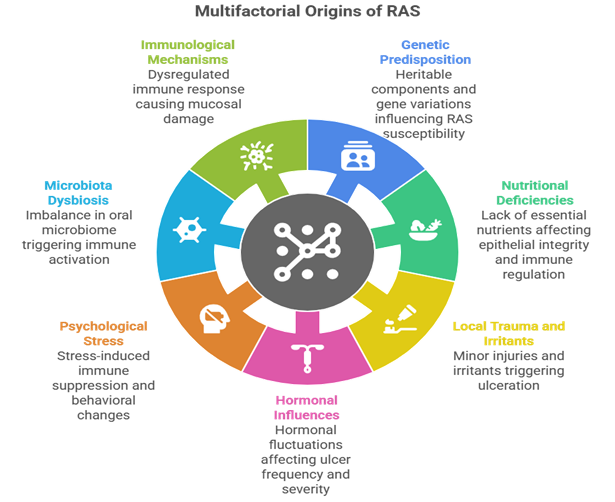
Figure 1: Multifactorial Origins of Recurrent Aphthous Stomatitis (RAS)
1.5 Rationale for Review
Despite decades of research, the exact immunopathogenic mechanisms behind RAS remain elusive. While the condition is often dismissed as benign and idiopathic, emerging evidence links it to systemic diseases, such as Behçet’s disease, celiac disease, HIV/AIDS, and inflammatory bowel disease. Moreover, current management remains largely symptomatic, lacking targeted or disease-modifying therapies. This review aims to consolidate current knowledge on the clinical characteristics, systemic relevance, and immunological underpinnings of RAS, and to identify emerging therapeutic opportunities, especially those targeting immune pathways. A comprehensive understanding of the immunopathogenesis could pave the way for precision medicine, personalized therapy, and improved outcomes for patients suffering from recurrent aphthous ulcers.
2. Clinical Features and Differential Diagnosis
Recurrent aphthous stomatitis (RAS), also known as canker sores, presents a distinct clinical profile characterized by painful, round or oval-shaped ulcers with a yellowish-white pseudo-membrane and surrounding erythematous halo. These lesions most commonly affect the non-keratinized mucosa of the oral cavity, such as the inner lips, buccal mucosa, floor of the mouth, soft palate, and ventral tongue. RAS is broadly classified into three subtypes: minor, major, and herpetiform, each with its own clinical behavior. Minor aphthous ulcers are the most prevalent form, accounting for approximately 80–85% of RAS cases. These ulcers typically measure 3–10 mm in diameter, heal spontaneously within 7–10 days without scarring, and are usually limited to 1–5 lesions per episode. In contrast, major aphthous ulcers (Sutton’s disease) are deeper, larger (>10 mm), more painful, and may persist for 2–6 weeks. Healing in major RAS is often accompanied by scar formation, and these ulcers can significantly interfere with oral intake, occasionally resulting in weight loss or secondary infections. Herpetiform aphthous ulcers, although rare, present as multiple (10–100) clusters of pinpoint-sized (1–3 mm) lesions that can coalesce into larger erosive areas. Despite the high number of ulcers, they generally heal within a week and are not associated with systemic symptoms. A key distinguishing feature of RAS is its restriction to non-keratinized mucosal sites. The hard palate, attached gingiva, and dorsal tongue are typically spared, unlike in other ulcerative conditions such as herpes simplex virus (HSV) infection, which commonly affects keratinized mucosa. The ulcers are preceded by a prodromal burning or tingling sensation 24–48 hours before eruption and are often triggered by minor trauma, stress, hormonal changes, or nutritional deficiencies[10]. Pain is a prominent symptom and may interfere with eating, drinking, speaking, and oral hygiene practices, leading to considerable reductions in quality of life, especially during recurrent or severe episodes. Given the clinical overlap with several other ulcerative disorders, a thorough differential diagnosis is essential. Behçet’s disease, for example, should be suspected in patients with recurrent oral ulcers accompanied by genital ulcers, uveitis, and systemic vasculitis. Oral ulcers in Behçet’s are often deep, major-type, and may mimic RAS; however, the presence of systemic findings, pathergy phenomenon, and HLA-B51 positivity aid in diagnosis. HSV infection, especially the primary form, can present with multiple painful oral ulcers, often preceded by vesicles and accompanied by systemic symptoms such as fever and malaise. Lesions in HSV infection favor keratinized sites and can be confirmed via PCR or viral culture[11]. In immunocompromised individuals, particularly those with HIV/AIDS, oral ulcers may be more frequent, larger, and resistant to treatment. They are often associated with other opportunistic infections such as oral candidiasis or hairy leukoplakia. CD4 counts and viral load assessments are crucial in establishing immune status and tailoring treatment. Other important differentials include drug-induced ulcers (notably with NSAIDs, nicorandil, and beta-blockers), autoimmune blistering diseases like pemphigus vulgaris, and premalignant conditions such as oral lichen planus or early squamous cell carcinoma[12]. Each of these conditions has distinct histopathological and clinical features that must be carefully considered.
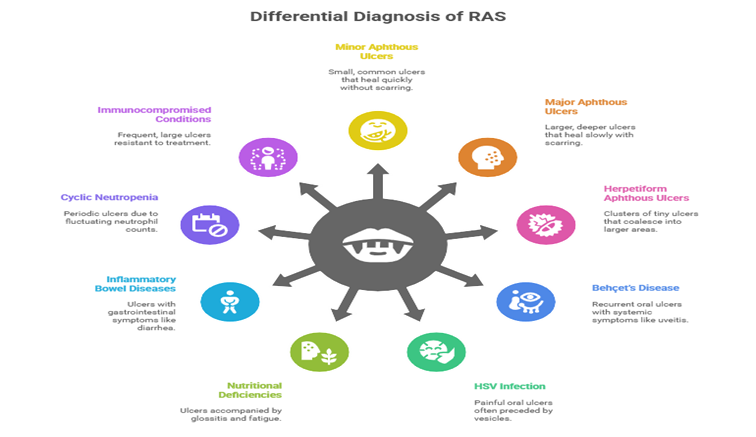
Figure 2: Clinical Features and Differential Diagnosis of Recurrent Aphthous Stomatitis
3. Etiologic and Precipitating Factors
The development of recurrent aphthous stomatitis (RAS) is believed to be multifactorial, involving a complex interplay between host genetic predisposition, nutritional status, environmental influences, and mucosal immune responses. Although the precise etiology remains elusive, numerous internal and external triggers have been implicated in initiating or exacerbating ulcer episodes. One of the most consistently reported contributors to RAS is nutritional deficiency, particularly involving water-soluble vitamins and trace elements critical to mucosal integrity and immune function. Hypovitaminosis of vitamin B12, folate, and iron has been frequently observed in RAS patients, with deficiencies leading to mucosal epithelial thinning, impaired cellular turnover, and reduced immune resilience[13]. Recent studies also indicate a possible role for vitamin C deficiency, which may compromise collagen synthesis and wound healing. Correction of these deficiencies has led to symptomatic improvement in many cases, highlighting the need for routine hematological screening in patients with frequent or severe ulceration. Genetic susceptibility is another major factor, with approximately 40–45% of RAS patients reporting a positive family history. Several studies have identified associations between RAS and human leukocyte antigen (HLA) alleles, including HLA-B51, B12, Cw7, and DR2. While these associations vary across ethnicities, they suggest a heritable component influencing immune recognition and response to mucosal antigens[14]. Moreover, polymorphisms in genes encoding cytokines and immune regulatory proteins—such as IL?6, IL?10, and NLRP3 (part of the inflammasome pathway)—have been linked to increased susceptibility to RAS[15]. These genetic variations may modulate the inflammatory cascade and mucosal immune surveillance, contributing to a hyperreactive state upon exposure to trivial triggers. A broad array of environmental and systemic triggers have been documented to precipitate or aggravate RAS. Psychological stress is one of the most frequently cited factors, potentially through its effects on neuroendocrine signaling and local immune suppression. Hormonal fluctuations, particularly during the menstrual cycle or pregnancy, have been shown to influence disease activity, possibly through changes in mucosal vascularity and immune modulation. Interestingly, smoking cessation is paradoxically associated with increased aphthous ulcer frequency, likely due to the loss of keratinizing stimuli from tobacco smoke, leading to reduced mucosal barrier function. Other external agents such as sodium lauryl sulfate (SLS)—a common foaming agent in toothpaste—may disrupt mucosal epithelium and exacerbate ulcer formation. Local trauma, including accidental bites, orthodontic irritation, or vigorous brushing, can act as a physical trigger, particularly in genetically susceptible individuals. Dietary antigens and food sensitivities, including to gluten, chocolate, coffee, or citrus fruits, have also been reported as potential aggravating factors, though the evidence remains largely anecdotal. Emerging research highlights the role of oral microbiome dysbiosis in RAS pathogenesis. Patients with RAS demonstrate reduced microbial alpha diversity in saliva, alongside significant shifts in mucosal microbial communities. Notably, beneficial commensals such as Streptococcus salivarius, known for their immunomodulatory and antimicrobial properties, are often depleted in affected individuals. In contrast, opportunistic or low-abundance species such as Acinetobacter johnsonii may be enriched, possibly contributing to immune dysregulation or secondary inflammation. The altered microbiota may influence local immune responses, barrier function, and epithelial repair, positioning microbiome modulation as a promising therapeutic avenue. Together, these findings underscore the multifactorial nature of RAS and the necessity for personalized assessment of triggers in each patient. An integrative understanding of genetic, nutritional, microbial, and behavioral factors will be crucial in refining prevention strategies and advancing individualized therapeutic interventions.
4. Immunopathogenesis
Recurrent aphthous stomatitis (RAS) is increasingly understood as an immunologically mediated condition characterized by the interplay of innate and adaptive immune dysregulation, oxidative stress, microbial triggers, and possible autoimmune phenomena. Although the initiating trigger may vary among individuals, the resulting immune cascade often culminates in mucosal injury and ulcer formation.
4.1 Innate Immunity and Oxidative Stress
Innate immune activation is the earliest event in aphthous ulcer development. Neutrophils infiltrate the ulcer base and release reactive oxygen species (ROS) as part of the defense mechanism. However, in RAS patients, neutrophil hyperactivity leads to overproduction of ROS, such as superoxide anions and hydrogen peroxide, which contribute to oxidative damage of epithelial cells. Simultaneously, antioxidant defense systems are compromised[16]. Reduced activity of key antioxidant enzymes like superoxide dismutase (SOD), catalase, and glutathione peroxidase has been consistently documented in RAS lesions and saliva. This imbalance between oxidants and antioxidants results in oxidative stress, aggravating tissue destruction.
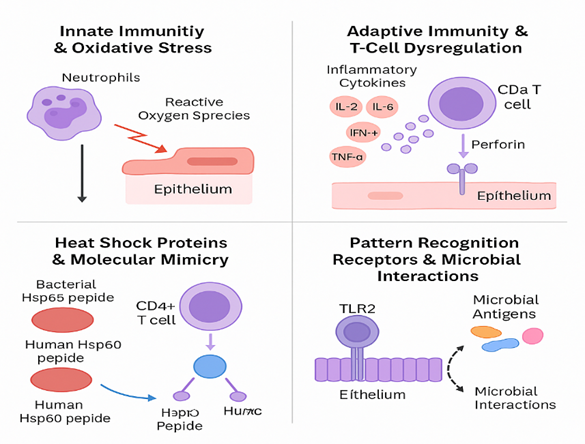
Figure 3: Oxidative stress and mucosal damage in RAS
4.2 Adaptive Immunity and T-cell Dysregulation
The adaptive immune response in RAS is characterized by a predominance of T-lymphocytes (~80% of infiltrates), particularly cytotoxic CD8+ T cells in the ulcerative phase. These cells induce apoptosis of basal epithelial cells through perforin/granzyme pathways. Immunophenotypic studies also reveal a systemic imbalance in T-helper and T-regulatory cell function[17]. Elevated levels of pro-inflammatory Th1 cytokines, such as interleukin-2 (IL-2), IL-6, interferon-gamma (IFN-γ), and tumor necrosis factor-alpha (TNF-α), are detected both locally and systemically in RAS patients. In contrast, immunoregulatory cytokines like IL-10 and transforming growth factor-beta (TGF-β) are significantly decreased, indicating impaired regulatory T-cell (Treg) activity[18]. A recent case-control study showed that salivary IL-2 and IL-22 levels are markedly elevated in RAS patients compared to controls, suggesting that these cytokines could serve as novel biomarkers and potential therapeutic targets[19].
Table 1: Key cytokine imbalances in RAS
|
Cytokine |
Role |
Observed Change in RAS |
|
IL-2 |
T-cell proliferation |
↑ Elevated |
|
IL-6 |
Acute phase response |
↑ Elevated |
|
IFN-γ |
Macrophage activation |
↑ Elevated |
|
TNF-α |
Inflammation and apoptosis |
↑ Elevated |
|
IL-10 |
Anti-inflammatory |
↓ Decreased |
|
TGF-β |
Tissue repair and Treg activation |
↓ Decreased |
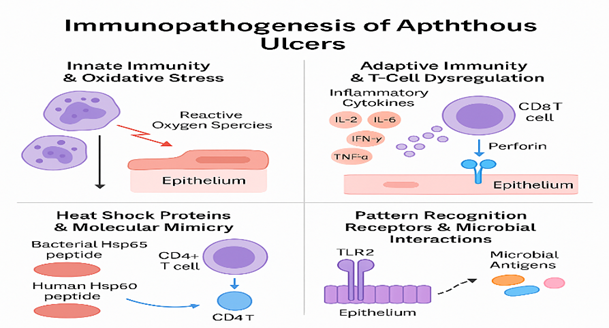
Figure 4: Molecular mimicry hypothesis in RAS
4.3 Heat Shock Proteins and Molecular Mimicry
The concept of molecular mimicry (shown in the figure 4) has been proposed to explain autoimmune features of RAS. Microbial heat shock protein 65 (Hsp65), found in certain bacterial pathogens like Mycobacterium and Streptococcus, shares epitope homology with human mitochondrial heat shock protein 60 (Hsp60), particularly within residues 91–105. Cross-reactivity of T-cells sensitized to microbial Hsp65 with host Hsp60 may trigger an autoimmune-like cytotoxic response, leading to epithelial destruction[20].
4.4 Pattern Recognition Receptors and Microbial Interactions
Pattern recognition receptors (PRRs), notably Toll-like receptors (TLRs), are key mediators of innate immunity in the oral mucosa. RAS patients show heightened expression of TLR2 and TLR4 in epithelial and lamina propria tissues[21]. This upregulation may render the mucosa hypersensitive to normal commensal or dysbiotic microbial signals. When activated, these TLRs trigger intracellular signaling cascades that lead to the release of pro-inflammatory cytokines and chemokines, contributing to sustained mucosal inflammation. Oral microbiome studies have also revealed decreased alpha diversity and a decline in beneficial species like Streptococcus salivarius in RAS patients[22]. Conversely, rare or potentially pathogenic bacteria like Acinetobacter johnsonii are enriched, possibly perpetuating inflammation through continuous TLR stimulation.
Table 1:. TLR signaling abnormalities in RAS
|
TLR |
Ligand |
Expression in RAS |
Downstream Effect |
|
TLR2 |
Lipoproteins (Gram+ bacteria) |
↑ Increased |
IL-6, TNF-α production |
|
TLR4 |
LPS (Gram- bacteria) |
↑ Increased |
NF-κB activation, cytokine release |
5. Immunology–Clinical Correlations
A growing body of evidence highlights the intricate interplay between immunological dysregulation and clinical manifestations in recurrent aphthous stomatitis (RAS). Among the most significant correlations is the relationship between pro-inflammatory cytokines—particularly tumor necrosis factor-alpha (TNF-α) and interferon-gamma (IFN-γ)—and the severity, frequency, and duration of ulcerative episodes. Elevated levels of these cytokines in saliva and serum are consistently associated with delayed healing and increased pain intensity, emphasizing their role in perpetuating mucosal inflammation and tissue breakdown. These cytokines not only amplify local immune responses but also recruit cytotoxic T-cells to the lesion site, intensifying epithelial injury[23]. Nutritional deficiencies—especially of vitamin B12, folate, iron, and vitamin C—further exacerbate this immune imbalance. Deficiencies in these micronutrients impair epithelial integrity, weaken antioxidant defenses, and compromise immune regulation, thereby increasing susceptibility to mucosal damage. Additionally, systemic factors such as hormonal fluctuations have been observed to influence the clinical course of RAS. For example, some female patients report higher lesion frequency during menstruation, likely due to hormonal modulation of mucosal immunity and vascular permeability. Psychological stress is another well-established precipitating factor. Cortisol, the principal stress hormone, can alter immune dynamics by suppressing anti-inflammatory pathways and skewing the T-helper cell balance toward a Th1-dominant profile. This shift promotes the expression of IFN-γ and TNF-α, contributing to lesion exacerbation during periods of emotional or physical stress. Interestingly, recent clinical studies suggest that interventions targeting the oral microbiome can influence both immune responses and clinical outcomes in RAS. Probiotic therapies, especially those containing Lactobacillus and Streptococcus salivarius strains, have shown promise in restoring microbial homeostasis and reducing lesion frequency. These probiotics may enhance mucosal immunity, downregulate pro-inflammatory cytokines, and promote epithelial repair, positioning microbiome modulation as a viable adjunctive approach in RAS management.
6. Therapeutic Strategies & Immunomodulatory Insights
The management of Recurrent Aphthous Stomatitis (RAS) is multifaceted and tailored according to ulcer severity, frequency, patient discomfort, and underlying pathophysiological contributors. Topical therapy remains the first line of management for most cases. Corticosteroids such as triamcinolone acetonide and dexamethasone are widely used to suppress local inflammation, reduce pain, and accelerate epithelial healing. Another topical agent, amlexanox, has demonstrated efficacy due to its anti-inflammatory and anti-allergic properties, acting through the inhibition of inflammatory kinases and reducing the release of histamine and leukotrienes[24]. Recent network meta-analyses have provided a comparative assessment of multiple interventions. Among them, low-level laser therapy (e.g., diode and Nd: YAG lasers) shows significant short-term benefits by alleviating pain and enhancing mucosal healing, primarily through the modulation of cytokines and improvement in local circulation[25]. Probiotics, especially strains like Lactobacillus rhamnosus and Streptococcus salivarius, have gained attention for their long-term efficacy in reducing recurrence frequency and extending ulcer-free periods[26]. These benefits are attributed to microbiome restoration and immune modulation. Other effective adjuncts include natural remedies such as honey, which exhibits antibacterial and wound-healing properties, insulin liposome gels that promote cellular regeneration, and glycyrrhiza (licorice extract), known to inhibit inflammatory pathways including cyclooxygenase and lipoxygenase systems[27][28]. Doxycycline and penicillin-based preparations have also been evaluated, though their use is tempered by higher risks of adverse events, including hypersensitivity and microbial resistance. Natural adjuncts continue to attract clinical interest due to their favorable safety profiles. Propolis, a bee-derived resinous substance, has been substantiated by meta-analyses for its efficacy in reducing ulcer size, pain, and frequency. Its action is multifactorial—encompassing antibacterial, antioxidant, and immunomodulatory effects[29]. Other promising natural agents include curcumin, known for inhibiting NF-κB and downregulating inflammatory cytokines; aloe vera, which supports mucosal healing; and chamomile, traditionally used for its soothing and anti-inflammatory properties[30]. In cases where RAS presents with severe, widespread, or recurrent lesions unresponsive to topical treatments, systemic therapies are employed. Systemic corticosteroids such as prednisolone are effective in controlling inflammation but are recommended only for short durations due to their side effect profile. Immunomodulatory agents like colchicine act by inhibiting neutrophil chemotaxis and have shown efficacy in both idiopathic RAS and Behçet’s-associated oral ulcers[31]. Pentoxifylline, a TNF-α inhibitor, improves microvascular circulation and reduces cytokine levels. Thalidomide, despite its potent TNF-α suppression and ulcer-healing properties, is restricted due to its risk of teratogenicity and neuropathy[32]. Recently, biologic agents such as anti-TNF drugs (e.g., adalimumab, infliximab) have been explored for refractory RAS cases, particularly those mimicking or overlapping with Behçet’s disease[33]. However, these require further validation through large, controlled trials to establish long-term safety and efficacy. A holistic approach is increasingly recognized as essential in the long-term management of RAS. Stress-reduction techniques—including cognitive behavioral therapy (CBT), mindfulness-based interventions, and yoga—are shown to lower cortisol levels and modulate immune responses, particularly by shifting the Th1/Th2 balance. Nutritional interventions targeting deficiencies in iron, folate, vitamin B12, and zinc are crucial, as these micronutrients play vital roles in epithelial integrity and immune competence. Dietary adjustments, such as avoiding spicy foods, gluten (in sensitive individuals), or acidic fruits, can also mitigate ulcer triggers. Oral hygiene modifications, particularly the use of sodium lauryl sulfate (SLS)-free toothpaste, are recommended to prevent mucosal irritation, which may exacerbate ulcer formation. In refractory cases, allergy testing and targeted elimination diets can help identify potential antigenic triggers. In summary, therapeutic strategies for RAS have evolved from symptom-centered topical treatments to more nuanced, immunologically informed interventions. While current modalities provide significant relief, there remains a need for targeted therapies based on an individual’s immunogenetic and microbiome profile. Emerging research into cytokine modulation, probiotics, and biologics offers hope for more personalized and effective future therapies.
Table 2: Summary of RAS Treatment Modalities
|
Treatment Category |
Examples |
Mechanism |
Evidence Level |
|
Topical Corticosteroids |
Triamcinolone, Dexamethasone |
Anti-inflammatory |
High |
|
Kinase Inhibitors |
Amlexanox |
Inhibits TNF-α and histamine release |
Moderate |
|
Laser Therapy |
Diode, Nd:YAG |
Promotes healing, analgesia |
High |
|
Natural Products |
Propolis, Honey, Licorice |
Antioxidant, mucosal protection |
Moderate–High |
|
Systemic Drugs |
Colchicine, Thalidomide, Anti-TNF agents |
Immunosuppressive |
Moderate |
|
Probiotics |
L. rhamnosus, S. salivarius |
Microbiome modulation |
High |
|
Holistic Approaches |
Stress reduction, Nutritional support |
Immune balance, prevention |
Moderate |
CONCLUSION AND FUTURE DIRECTIONS
Recurrent Aphthous Stomatitis (RAS) remains one of the most prevalent and clinically impactful mucosal disorders, affecting approximately 20% of the global population. Despite its benign nature, its recurrent course, painful presentation, and multifactorial etiology result in significant morbidity and impaired quality of life. This review has highlighted the intricate interplay between genetic susceptibility, nutritional imbalances, mucosal trauma, psychological stress, and dysbiosis of the oral microbiome in the pathogenesis of RAS. The evolving understanding of its immunopathogenesis—marked by dysregulation in innate and adaptive immune pathways, particularly Th1-predominant cytokine profiles, oxidative stress, and altered T-cell responses—has opened new avenues for targeted management. Therapeutically, while corticosteroids and conventional topical agents continue to form the cornerstone of treatment, recent insights have driven the exploration of novel interventions such as probiotics, low-level laser therapy, and biologics targeting cytokine networks like TNF-α and IL-2. Additionally, the recognition of lifestyle, nutritional, and psychoneuroimmunological influences emphasizes the importance of a holistic and patient-centered management approach. Looking forward, future research must aim to delineate the immunophenotypic and molecular subtypes of RAS through integrative omics—transcriptomics, proteomics, and microbiomics—to enable precision therapy. The development of predictive biomarkers for disease onset, severity, and treatment response could revolutionize personalized care. Furthermore, large-scale randomized controlled trials are needed to validate emerging therapies, especially biologics and immune modulators, ensuring long-term safety and efficacy. In conclusion, bridging the gap between clinical manifestations and immunological mechanisms in RAS holds promise for transforming its diagnosis, prognosis, and therapeutic landscape. A multidisciplinary, systems-biology approach is essential to unlock curative strategies and reduce the disease burden across diverse populations.
REFERENCES


Banoth Machendhar Naik, M. Shivaprasad, Shiva Prasad Goud, Pravanya Ramraj, Rahul Molla*, Maryat Gigi, Aphthous Ulcer: Clinical Implications and Immunological Factors, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 1, 420-433. https://doi.org/10.5281/zenodo.18163997
 10.5281/zenodo.18163997
10.5281/zenodo.18163997
