1,3,4,5,6Matoshri Institute of Pharmacy, Dhanore, Yeola.
2MET Institute of Pharmacy, Nashik.
The use of amlodipine is very common due to the effects of amlodipine on hypertension and coronary artery disease (CAD) like chronic stable angina, vasospastic angina (Prinzmetal’s or variant angina), and angiographically documented CAD. Amlodipine is involved in several combinations with other antihypertensive drugs. The analysis of amlodipine and its co-drugs is reported using several analytical methods such as spectrophotometric, capillary electrophoresis and chromatographic methods. To our knowledge, there is no comprehensive reports which address all analytical methods for the analysis of amlodipine and combination, therefore we tried to gather as much as reports in one review paper to help researchers and industrial experts to easily access the information related to amlodipine analysis
Amlodipine besylate is chemically described as 3-Ethyl-5-methyl (±)-2-[(2-aminoethoxy) methyl]-4-(2- chlorophenyl)-1,4-dihydro-6-methyl-3,5-pyridinedicarboxylate, monobenzenesulphonate. Its empirical formula is C20H25CIN2O5•C6H6O3S, and its structural formula is:
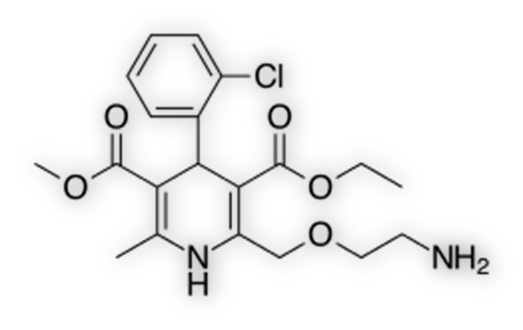
Structure of Amlodipine Besylate
Amlodipine besylate is a white crystalline powder with a molecular weight of 567.1. It is slightly soluble in water and sparingly soluble in ethanol. NORVASC (amlodipine besylate) tablets are formulated as white tablets equivalent to 2.5, 5 and 10 mg of amlodipine for oral administration. In addition to the active ingredient, amlodipine besylate, each tablet contains the following inactive ingredients: microcrystalline cellulose, dibasic calcium phosphate anhydrous, sodium starch glycolate, and magnesium stearate.
Mechanism of Action:
Mechanism of Action Amlodipine is a dihydropyridine calcium antagonist (calcium ion antagonist or slow-channel blocker) that inhibits the transmembrane influx of calcium ions into vascular smooth muscle and cardiac muscle. Experimental data suggest that amlodipine binds to both dihydropyridine and nondihydropyridine binding sites. The contractile processes of cardiac muscle and vascular smooth muscle are dependent upon the movement of extracellular calcium ions into these cells through specific ion channels. Amlodipine inhibits calcium ion influx across cell membranes selectively, with a greater effect on vascular smooth muscle cells than on cardiac muscle cells. Negative inotropic effects can be detected in vitro but such effects have not been seen in intact animals at therapeutic doses. Serum calcium concentration is not affected by amlodipine. Within the physiologic pH range, amlodipine is an ionized compound (pKa=8.6), and its kinetic interaction with the calcium channel receptor is characterized by a gradual rate of association and dissociation with the receptor binding site, resulting in a gradual onset of effect. Amlodipine is a peripheral arterial vasodilator that acts directly on vascular smooth muscle to cause a reduction in peripheral vascular resistance and reduction in blood pressure. The precise mechanisms by which amlodipine relieves angina have not been fully delineated, but are thought to include the following: Exertional Angina: In patients with exertional angina, NORVASC reduces the total peripheral resistance (afterload) against which the heart works and reduces the rate pressure product, and thus myocardial oxygen demand, at any given level of exercise. Vasospastic Angina: NORVASC has been demonstrated to block constriction and restore blood flow in coronary arteries and arterioles in response to calcium, potassium epinephrine, serotonin, and thromboxane A2 analog in experimental animal models and in human coronary vessels in vitro. This inhibition of coronary spasm is responsible for the effectiveness of NORVASC in vasospastic (Prinzmetal’s or variant) angina. [1]
Literature Survey:
01) Amlodipine in human plasma was analysed by Feng teamwork using LC-MS. Necardipine was used as internal standard and both drugs were extracted from plasma using ethyl acetate. Samples were injected into C18 column and the mobile phase was methanol - 1% glacial acetic acid (65-35% v/v). The temperature which used for the analysis was set to 35?C and the flow rate was 0.8 ml/min. For detection, an air pressure ionization single quadruple mass spectrometer equipped with an ESI interface was used and it was operated in positive-ionization mode. Methanol was used to prepare standard stock solutions. Samples were prepared and extracted by spiking 1 ml of plasma with amlodipine and internal standard and extracting it by adding NaOH(1M) and ethyl acetate. The organic layer was separated and evaporated and the remaining were dissolved in methanol to inject in the column. The results showed that the method was linear over the range of 0.1-20 ng/ml. the results of precision, accuracy and recovery were satisfactory. The method was applied to analyse amlodipine in human plasma for 10 mg dose study and the results were like those reported by previous methods. The authors concluded that their method is simple, fast, accurate and precise and the extraction method is simple. The use of MS detector gave the method more specificity and selectivity [2]. 02) Nirogi and team developed and validated liquid chromatography/tandem mass spectrometry assay for the analysis of amlodipine in human plasma. According to the author this method was developed to get very low LLOQ which is 50 pg / ml of amlodipine in human plasma. Samples were injected into a reverse phase C18 column. A mixture of water–acetonitrile–formic acid (30:70:0.03, v/v) was used as mobile phase with a flow rate of 0.1 ml/ min. The detection was achieved using MS detection in the multiple reaction monitoring mode. Tamsulosin was used as internal standard. The standard solutions were prepared using methanol and diluted in methanol- water 50:50 v/v. The plasma samples were prepared by liquid-liquid extraction using diethyl ether- dichloromethane 7:3 v/v and drying the organic layer and then dissolving it in methanol-water 50:50 v/v. The stability study of amlodipine in human plasma and the extraction recovery were studied using this method. This method was applied in pharmacokinetic study for healthy volunteers. The results showed linear range of 50-10000 pg/ ml of amlodipine in human plasma and LLOQ achieved was 50 pg/ml. The recovery of extraction was 74.7±4.6 %. The total time for the run was 1.5 min. The author concluded that this method is simple, rapid (run of 1.5 min), and economic [3]. 03) Donger and co-workers developed and validated new reverse phase HPLC method for the simultaneous the analysis of metoprolol succinate (MS) and amlodipine besylate (AB) in tablet dosage form. Chromatography was carried out using Hypersil BDS cyano (250mm×4.6 mm, 5_m) column. The detection was achieved using PDA detector at 254 nm. Two drugs were eluted using isocratic mobile phase consisting of a mixture of aqueous triethylamine buffer pH 3 and acetonitrile in the ratio of 85:15 (v/v) and phosphoric acid was used to adjust the pH. The flow rate was 1.0 mL/min. Standard solutions and sample solutions were prepared using methanol and mobile phase. The method was validated according to ICH guidelines and the method was found linear over the range 42-98µg/ml. The authors concluded that their method is specific, accurate, rapid and precise. Authors recommended their method to be used for routine analysis of amlodipine besylate and metoprolol succinate in quality control analysis of pharmaceutical preparations containing these drugs [4]. 04) Naidu and co-workers developed and validated new RP – HPLC method for simultaneous determination of amlodipine besylate and benazepril hydrochloride in their combined pharmaceutical dosage form. This method was also used mainly to determine the degradation in these two drugs in their samples. The degrades resulted from thermal, photolytic, hydrolytic and oxidative degradation were studied by this method. Chromatographic conditions used were optimized and chosen as the column used in this study was Zorbax SB C18, 5 um, 250 mm × 4.6 mm i.d. Phosphate buffer and acetonitrile in the proportion of 65:35 (v/v) with pH adjusted to 7.0 was used as mobile phase, and the detector was photodiode array detector with wavelength of 240 nm. Methanol and mobile phase were used to prepare the standard solutions and tablet samples. The results showed linearity for amlodipine over the range of 6–14 µg/ml. The recovery study approved the accuracy of the method and statistically study showed the precision of this method. The method showed good resolution between two drugs and their degradants in all degradation methods. The authors concluded that this method is specific, accurate and precise and it can be used as stability indicating method for assay of amlodipine besylate and benazepril hydrochloride in their combination product [5].
05) Another study of kinetic spectrophotometric method developed and validated by Mahmoud et al. (2012) to determine amlodipine besylate in its pharmaceutical tablets. The method was based on the condensation reaction of AML with 7-chloro-4-nitro-2,1,3-benzoxadiazole in an alkaline buffer (pH 8.6) producing a highly-colored product. The color development was monitored spectrophometricaly at the maximum absorption λmax 470 nm. Here, both the activation energy and the specific rate constant (at 70 °C) of the reaction were found to be 6.74 kcal mole−1 and 3.58 s−1, respectively. Under the optimum reaction conditions, the limits of detection and quantification were 0.35 and 1.05 μg/mL, respectively. The precision of the method was satisfactory; the relative standard deviations were 0.85–1.76%. The proposed method was successfully applied to the analysis of AML in its pure form and tablets with good accuracy; the recovery percentages ranged from 99.55±1.69% to 100.65±1.48%. The results were compared with that of the reported method [6]. 06) Basavaiah and team developed indirect spectrophotometric method to determine amlodipine besylate in pharmaceuticals. This method depends on brominating amlodipine using fixed excess amount of bromated bromide mixture in acidic medium of HCl. The remaining amount of bromine was reacted with fixed known amount of metanil yellow die and the remaining dye was determined by absorbance measuring at 530 nm. All factors influencing the method were studied and validated including the concentration of die and amount of HCl and the time of taking the absorbance. The absorbance against the concentration of amlodipine was linear in the range of 1.25-7.20 µg/ml, while the LOD and LOQ were 0.17 and 0.56 µg/ml respectively. This method was applied for determination of amlodipine in two commercial formulations and there was close agreement between this method and reference methods. Amlodipine was determined in the same paper using HPLC method. The author concluded that those methods are simple and rapid. They also concluded that their spectrophotometric method did not need any heating or extracting [7]. 07) New spectrophotometric and spectrofluorimetric method were developed and validated by Ayad and his co-workers for the simultaneous analysis of amlodipine besylate and doxazosin mesilate. The methods depend on the reaction of amlodipine besylate and doxazosin mesilate with acetyl acetone and formaldehyde to form a yellow compound which can be quantified either spectrophotometrically or spectrofluorimetrically. Standard and samples were prepared by dissolving amlodipine besylate and doxazosin mesilate in least amount of methanol and dilute with water. The reaction conditions were studied and optimized to give the optimum compound. All the parameters for the reaction such as pH, heating time and the concentration of acetyl acetone and formaldehyde were studied and optimized. The methods were applied successfully on the commercial pharmaceutical form. The spectrophotometric method was linear over the range of 6-44μg/ mL for amlodipine besylate and 8-36μg/mL for doxazosin mesilate. The linear range for spectrophotometric method was 1.6-7.6μg/mL and 0.02- 0.22μg/mL for amlodipine besylate and doxazosin methylate, respectively. The methods were studied for precision and accuracy and the results were in acceptable ranges. In conclusion, authors claimed that their method is simple, sensitive, precise and accurate. These methods can be used in routine analysis for studied drugs [8]. 08) Chromatographic separation of the two drugs was achieved on an Eclipse XDB C-8 (150 mm X 4.6 mm), 5mm. The mobile phase constituted of Buffer: Acetonitrile (65:35) and pH adjusted to 2.6 with dilute Ortho- Phosphoric Acid was delivered at the flow rate 1.0 mL/min. Detection was performed at 210 nm. Separation was completed within 8 min. Calibration curves were linear with correlation coefficient between 0.99 to 1.0 over a concentration range of 8 to 60 mg/mL of Perindopril Erbumine and 10 to 75 mg/mL of Amlodipine Besylate. The relative standard deviation (R.S.D) was found <2.0%.[9] 09) The chromatographic analysis was performed on Athena C18 column(250×4.6mm, 5 μ particle size) with mobile phase consisting of methanol and phosphate buffer (pH 4) in the ratio of 70:30 v/v, at a flow rate of 1 mL/min and eluents monitored at 240 nm. The method was validated for linearity, accuracy, precision, robustness and application for assay as per International Conference on Harmonization (ICH) guidelines. The retention times of amlodipine besylate and telmisartan were 2.3 and 3.4 min, respectively. The calibration curves of peak area versus concentration, which was linear from 2.5-15 μg/mL for amlodipine besylate and 20-120 μg/mL for telmisartan, had regression coefficient (r2) greater than 0.998. The method had the requisite accuracy, precision, and robustness for simultaneous determination of amlodipine besylate and telmisartan in tablets. And force degradation also performed. The proposed method is simple, economical, accurate and precise, and could be successfully employed in routine quality control for the simultaneous analysis of amlodipine besylate and telmisartan in tablet form. [10] 10) The chromatographic separation was achieved on Water Xterra R18, 150×4.6 mm, 3.5u (C18) using Mobile Phase A : ACN: Water: OPA (950:50:01) and Mobile Phase B: ACN: Water: OPA (50:950:01), and the λmax of Amlodipine Besylate was detected at 237nm, where Candesartan Cilexetil exhibits sufficient absorbance at 254 nm. The linear range for Candesartan Cilexetil and Amlodipine Besylate were (2.8-42ppm) and (6.4-96) was obtained with correlation coefficients ≥0.999 for each analyte. The retention time were found to be 4.2 and 8.5 min Candesartan Cilexetil and Amlodipine Besylate respectively. Candesartan Cilexetil and Amlodipine Besylate was subjected to stress conditions (hydrolysis (acid, base) oxidation, photolysis, thermal degradation and humidity degradation) and the stressed samples were analyzed by use of the method. The major degradation was observed in base and minor in acid, thermal, oxidation, humidity and photolysis. [11]
CONCLUSION:
There are number of generic formulations and combinations of amlodipine and other antihypertensive drugs available in the market. Analytical method for these combination drugs are not listed in the pharmacopeia yet. To optimize the analytical method, it becomes very difficult for the analyst to design and fulfil the specification of the drug. So far there are several reports on the analysis of amlodipine and its formulation following spectroscopic, chromatographic and capillary electrophoresis methods using wide range of detectors such as UV, diode array, fluorescence, electrochemical, and MS detectors. In this work, we strive to gather as many methods related to amlodipine analysis suitable for the researchers to extract important information to establish their own method. There are still lacks of proper analytical method which can comply with the international guideline for the analysis of the drugs. In coming days’ researcher and industries are expected to come out with more suitable analytical methods for the analysis of amlodipine and its formulation. It is very important to mention that the door is still open for more work in analysis side of amlodipine either in research or industrial set up.
REFRENCES


Dashpute S. N.*, Kotkar A. V., Khilari Tejas, Bothe Om, Ahire Sushant, Gunjal Hari, Amlodipine in the Current Management of Hypertension, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 344-349. https://doi.org/10.5281/zenodo.14988060
 10.5281/zenodo.14988060
10.5281/zenodo.14988060
