Shri Ram Nath Singh Mahavidyalaya (Pharmacy) Gormi, Bhind, (m. p.)
The pharmacokinetic advantage relies on the criterion that, drug release from the fast-releasing layer leads to a sudden rise in the blood concentration. However, the blood level is maintained at steady state as the release from sustained layer. Particularly bilayer tablets are commonly used to avoid chemical incompatibilities of formulation components by physical separation, and release profile. The tablet is the most widely used dosage form because of its convenience in terms of self-administration, compactness and ease in manufacturing.4 Tablets are solid dosage forms containing medicinal substances with or without suitable diluents.5 According to Indian Pharmacopoeia Pharmaceutical tablets are solid, flat or biconvex dishes, unit dosage form, prepared by compressing a drugs or a mixture of drugs, with or without diluents.6 They are varying in size and weight, depending on amount of medicinal substances and the intended mode of administration. It is most popular dosage form and 70% of the total medicines are dispensed in the form of tablet There are different types of tablets are available in market conventional tablet, immediate tablet, fast dissolving tablet, controlled release tablet, sustained release tablet, delayed release tablet.Immediate release tablets are those which disintegrate rapidly and get dissolved to release the medicaments.10 For immediate release formulation, super disintegrants play key component. Super disintegrants are used to improve the efficacy of solid dosage form. This achieved by various mechanisms, swelling, porosity and capillary action, heat of wetting, particle repulsion forces, deformation recovery, enzymatic reaction by which the tablets are broken into small particles.
Oral route is most commonly employed route of drug administration. Although different route of administration is used for the delivery of drugs, due to flexibility in dosage form design and patient compliance oral route is preferred.1 The popularity of the oral route is attributed ease of administration, patient acceptance, accurate dosing, cost effective manufacturing method and generally improved shelf-life of the product.There are several techniques of conventional drug delivery system where tablets, capsules, pills, liquids, are used as drug carrier. Among them, solid formulation does not require sterile conditions and are therefore, less expensive to manufacture. The tablet is the most widely used dosage form because of its convenience in terms of self-administration, compactness and ease in manufacturing. Tablets are solid dosage forms containing medicinal substances with or without suitable diluents.5 According to Indian Pharmacopoeia Pharmaceutical tablets are solid, flat or biconvex dishes, unit dosage form, prepared by compressing a drugs or a mixture of drugs, with or without diluents.They are varying in size and weight, depending on amount of medicinal substances and the intended mode of administration. It is most popular dosage form and 70% of the total medicines are dispensed in the form of tablet. There are different types of tablets are available in market conventional tablet, immediate tablet, fast dissolving tablet, controlled release tablet, sustained release tablet, delayed release tablet. Immediate release tablets are those which disintegrate rapidly and get dissolved to release the medicaments. For immediate release formulation, super disintegrants play key component. Super disintegrants are used to improve the efficacy of solid dosage form. This achieved by various mechanisms, swelling, porosity and capillary action, heat of wetting, particle repulsion forces, deformation recovery, enzymatic reaction by which the tablets are broken into small particles. Categories of the drug which are preferable for immediate release are analgesic and anti-inflammatory drugs such as Ibuprofen, Diclofenac sodium. Anti-coagulants such as Dicoumarol, Dipyridamol. Anti-Depressants such as Amoxapiine. Anti-diabetic such as Glipizide. Antihypertensive drug such as Amlodipine, Minoxidil, Nifedipine are most preferable for the immediate release.
Sustained release systems include any drug over an extended period of time. If the system is successful in maintaining constant drug levels in the blood or target tissue, it is considered as a controlled release system. If it is unsuccessful of this day nevertheless extends the duration of action over that achieved by conventional delivery, it is considered as a prolonged released system.
Drug in the outside layer exposed to the bathing solution is dissolved first and then diffuses out of the matrix. This process continues with the interface between the bathing solution and the solid drug moving toward the interior. It follows that for this system to be diffusion controlled, the rate of dissolution of drug particles within the matrix must be much faster than the diffusion rate of dissolved drug leaving the matrix.
Bi-layer tablets are prepared with one layer of drug for immediate release while second layer designed to release drug later, either as second dose or in an extended-release manner. Bilayered tablet is suitable for sequential release of two drugs in combination, separate two incompatible substances, and also for sustained release tablet in which one layer is immediate release as initial dose and second layer is maintenance dose. The basic goal of therapy is to achieve a steady state drug in blood level for an extent period of time.
MATERIAL AND METHOD
MATERIALS-
Table 1: List of materials
|
S. No |
Ingredients |
Company Name |
|
1. |
Divalproex sodium |
Gift sample from ROAQ Chemicals Pvt. Ltd. Vadodara |
|
2. |
Sodium Starch Glycolate |
S.D. Fine Chem. Ltd, Mumbai |
|
3. |
Croscarmellose |
S.D. Fine Chem. Ltd, Mumbai |
|
4. |
HPMC K4M |
Yarrow Chem Products, Mumbai |
|
5. |
HPMC K100M |
Yarrow Chem Products, Mumbai |
|
6. |
Lactose |
S.D. Fine Chem. Ltd, Mumbai |
|
7. |
Micro Crystalline Cellulos |
S.D. Fine Chem. Ltd, Mumbai |
|
8. |
PVP K 30 |
S.D. Fine Chem. Ltd, Mumbai |
|
9. |
Ponceau 4R |
Indian fine chemicals, Mumbai-20 |
|
10. |
Magnesium Stearate |
S.D. Fine Chem. Ltd, Mumbai |
|
11 |
Talc |
S.D. Fine Chem. Ltd, Mumbai |
LIST OF INSTRUMENTS-
Table 2: List of Equipment’s
|
S. No. |
Equipment |
Model/company |
|
1. |
Fourier Transform Infrared spectrophotometer |
Thermo Nicolet |
|
2. |
UV-Visible spectrophotometer |
UV-1800, Shimadzu |
|
3. |
Electronic balance |
Essae-Teraoke |
|
4. |
Hot air oven |
Kemi |
|
5. |
Multi tablet Punching machine |
LAB PRESS, CipMachinaries Ltd. Ahmedabad |
|
6. |
Roche Friabilator |
PSM Industries, Bangalore |
|
7. |
Hardness tester |
Monsanto hardness tester |
|
8. |
Disintegration test apparatus |
DT-1500, Lab India |
|
9. |
Dissolution test apparatus |
DS-800, Lab India |
|
10. |
FTIR- spectrophotometer |
Tensor 27 Bruker |
|
11. |
DSC Apparatus |
DSC-60, Shimadzu |
|
12. |
Stability chamber |
106 Model/ LabTop, Sky Lab Instruments & Engineering Pvt.Ltd. |
PRE-FORMULATION STUDIES
Pre-formulation testing is the first step in rational development of dosage forms of a drug substance. Pre-formulation study is the process of optimizing the delivery of drug through determination of physicochemical properties of the excipients that could affect drug performance and development of as efficacious, stable and safe dosage form.
1. Determination of λ max
Divalproex sodium was dissolved in methanol further diluted with the same and scanned for maximum absorbance in UV double beam spectrophotometer (Shimadzu 1800) in the range from 190 to 380 nm.
2. Solubility
The solubility of Divalproex sodium was determined in distilled water, methanol, ethanol, acetone, chloroform and pH 6.8 phosphate buffer by shake flask method. An excess amount of Divalproex sodium is added to each vial containing 10 ml of selected solvent till the saturation of the solution.
3. Melting point
Melting point of the Divalproex sodium was determined by capillary method in triplicate.
4. Standard Curve for Divalproex sodium
100 mg of Divalproex sodium was accurately weighted and dissolved in 100 ml of methanol to prepare first stock solution. 10 ml of above solution was taken and diluted to 100 ml with the same solvent to prepare II stock solution. .
Formulation Design
Calculation of dose
The total dose of Divalproex sodium for once daily formulation was calculated by the following equation, using available pharmacological data.
Dt = Dose (1+0.693xt/t1/2)
Where, Dt = Total dose of drug,
Dose = Dose of immediate release part.
t = time in hr during which the sustained release is desired (18 hrs)
t1/2 = half life of the drug (9 hrs)
Therefore,
Dt = 125(1+0.693x18/9), Dt ≈ 298.25
Therefore, maintenance dose = 298.25-125 = 173.25 mg.
Hence, the formulation should release 125 mg drug within 1 hour and 173.25 mg drug in 18 hours.
Table 4: Formulation of immediate release layer (IRL)
|
S.NO. |
Ingredients |
IF1 |
IF2 |
IF3 |
IF4 |
IF5 |
IF6 |
|
1. |
Divalproex sodium |
125 |
125 |
125 |
125 |
125 |
125 |
|
2. |
Lactose |
82 |
79.5 |
82 |
79.5 |
82 |
79.5 |
|
3. |
Croscarmellose sodium |
10 |
12.5 |
- |
- |
5 |
6.25 |
|
4. |
Sodium starch glycolate |
- |
- |
10 |
12.5 |
5 |
6.25 |
|
5. |
Microcrystalline cellulose |
25 |
25 |
25 |
25 |
25 |
25 |
|
6. |
Ponceau 4R |
0.02 |
0.02 |
0.02 |
0.02 |
0.02 |
0.02 |
|
7. |
Magnesium stearate |
3 |
3 |
3 |
3 |
3 |
3 |
|
8. |
Talc |
5 |
5 |
5 |
5 |
5 |
5 |
|
9. |
Total |
250 |
250 |
250 |
250 |
250 |
250 |
Table 5: Formulation of sustained release layer (SRL)
|
S.NO. |
Ingredients |
SF1 |
SF2 |
SF3 |
SF4 |
SF5 |
SF6 |
SF7 |
SF8 |
SF9 |
|
1. |
Divalproex sodium |
173.25 |
173.25 |
173.25 |
173.25 |
173.25 |
173.25 |
173.25 |
173.25 |
173.25 |
|
2. |
Lactose |
52.75 |
45.25 |
37.75 |
52.75 |
45.25 |
37.75 |
52.75 |
45.25 |
37.75 |
|
3. |
HPMC K4M |
45 |
52.5 |
60 |
- |
- |
- |
22.5 |
26.25 |
30 |
|
4. |
HPMC K100M |
- |
- |
- |
45 |
52.5 |
60 |
22.5 |
26.25 |
30 |
|
5. |
Microcrystalline cellulose |
20 |
20 |
20 |
20 |
20 |
20 |
20 |
20 |
20 |
|
6. |
Magnesium stearate |
3 |
3 |
3 |
3 |
3 |
3 |
3 |
3 |
3 |
|
7. |
Talc |
6 |
6 |
6 |
6 |
6 |
6 |
6 |
6 |
6 |
|
8. |
Total |
300 |
300 |
300 |
300 |
300 |
300 |
300 |
300 |
300 |
Preparation of IRL
IRL of Divalproex sodium (DS) was prepared by wet granulation by using different Super disintegrants such as SSG and Croscarmellose sodium. PVP K30 solution with containing coloring agent was used as binding solution. As DS was oily in characteristics, MCC was used as adsorbent.
Preparation of SRL
Accurately weighed Divalproex sodium and polymer and others ingredients were taken in mortar and pestle and mixed well. The powder was mixed with sufficient quantity for PVP K30 solution until wet mass formed.
Preparation of bi-layered tablet
By the study of disintegration and drug release profile of IRL and SRL, best formulations of each layer were chosen and bi-layered tablet were prepared by double compression in single rotatory tableting machine.
Evaluation of Pre-formulation Parameters:
The angle of repose of granules was determined by the funnel method the accurately weighed granules were taken in a funnel. The height of the funnel was adjusted in such a way that the tip of the funnel just touched the apex of the heap of the granules. The granules were allowed to flow through the funnel Greely onto the surface.
θ =tan-1 (h/r)
Where, θ = the angle of repose
h = height of the heap of the powder
r = radius of the heap of the powder
Table 6: ANGLE OF REPOSE
|
S.NO. |
Angle of Repose(θ) |
Type of flow |
|
1. |
? 25 |
Excellent |
|
2. |
25-30 |
Good |
|
3. |
30-40 |
Passable |
|
4. |
? 40 |
Very poor |
A quantity of 2 g of the powder (W) from each formula was introduced into a 25 ml measuring cylinder. After the initial volume was observed, the cylinder was allowed to fall under its own weight onto a hard surface from the height of 2.5 cm at 2 sec intervals. The tapping was continued until no further change in volume was noted. The bulk density, and tapped density were calculated using following formulas.
It helps in measuring the force required to break the friction between the particles and the hopper. It is expressed in % and given by

Table 7: % COMPRESSIBILITY INDEX
|
S.NO. |
% Compressibility index |
Property |
|
1. |
5-12 |
Free flowing |
|
2. |
12-16 |
Good |
|
3. |
18-21 |
Fair |
|
4. |
23-35 |
Poor |
|
5. |
33-38 |
Very poor |
|
6. |
? 40 |
Extremely poor |
Hausner’s ratio is an indirect index of ease of powder flow. Hausner’s ratio was measured by the ratio of tapped density to bulk density.

Table 8: HAUSNER’S RATIO
|
S.NO. |
Hausner’s ratio |
Property |
|
1. |
0-1.2 |
Free flowing |
|
2. |
1.2-1.6 |
Cohesive flowing |
Evaluation of prepared formulations Evaluation of Divalproex sodium IRL, SRL and bi-layered tablet
The tablets prepared were evaluated for the following parameters:
Weight Variation Test:
To study weight variation, 20 tablets of each formulation were weighted using electronic balance and the test was performed according to the official method.
Table 9: IP standards of Uniformity of weight
|
S.NO. |
Avg. Weight of Tablet (mg) |
% of Deviation |
|
1. |
≤80 mg |
10 |
|
2. |
? 80 mg – 250 mg |
7.5 |
|
3. |
≥250 mg |
5 |
Hardness:
The resistance of tablets to shipping or breakage under condition of storage, transportation and handling before usage depends on its hardness. The hardness of each batch of tablet was checked by using Monsanto hardness tester. The hardness was measured in the terms of kg/cm2. 5 tablets were chosen randomly and tested for hardness. The average hardness of 5 determinations was recorded.
Friability:
Friability generally refers to loss in weight of tablets in the containers due to removal of fines from the tablet surface. Friability generally reflects poor cohesion of tablet ingredients. 10 tablets were weighed and the initial weight of these tablets was recorded and placed in Roche friabilator and rotated at the speed of 25 rpm for 100 revolutions.

Tablet thickness:
Thickness of the tablet is important for uniformity of tablet size. Thickness was measured using Vernier Calipers. It was determined by checking the thickness of ten tablets of each formulation.
In-vitro dissolution studies of immediate release layer:
The in-vitro dissolution studies were performed using USP-II (paddle) dissolution apparatus at 100 rpm. Phosphate buffer pH 6.8 dissolution media is maintained at 37±0.500C. A 5 ml was withdrawn at specific time intervals and same volume of fresh medium was replaced.
In vitro dissolution studies of sustained release layer:
The in vitro release of sustained release layer was carried out for 18 hours using USP type-II apparatus (DT-1200) at 100 rpm for the first 45 minute in 900 ml 0.1N HCL maintaining at 37 ±0.50C and then at phosphate buffer pH 6.8 in 900ml for another 18 hour.
Drug Content for IRF, SRF and Bi-layered tablet:
Ten tablets were weight and average weight is calculated. All tablets were crushed and powder equivalent to 100 mg drug was dissolved in pH 6.8 phosphate buffer and the volume was made up to 100 ml with pH 6.8 phosphate buffer.
Stability Studies:
The optimized formulation was subjected for two-month stability study according to standard guidelines. The selected formulations were packed in aluminum foils, which were in wide mouth bottles closed tightly. They were stored at 400C / 75% RH for 3 months and evaluated periodically.
RESULT AND DISCUSSION-
Determination of λmax
The λmax of Divalproex sodium was found to be 210 nm in methanol and phosphate buffer pH 6.8.
Standard curve of Divalproex sodium.
The absorbance was measured in a UV spectrophotometer at 210 nm against methanol.
Table 10: Spectrophotometric data of Divalproex Sodium

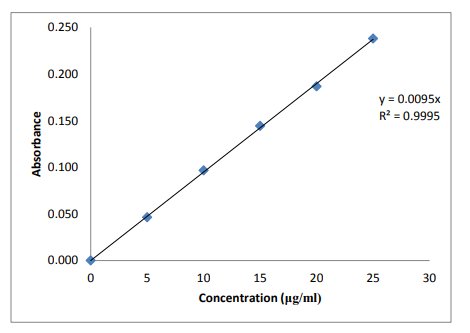
Figure 4: Standard graph of Divalproex sodium
Drug solubility studies -
The solubility studies of drug were done by using various media like distilled water, methanol, chloroform and phosphate buffer pH 6.8. The result shows maximum solubility in chloroform.
Table 11: Solubility of Divalproex sodium
|
Solvents |
Solubility (mg/ml) |
|
Distilled water |
7.35 |
|
Methanol |
48.45 |
|
Chloroform |
55.24 |
|
Phosphate buffer pH 6.8 |
29.73 |
Result showed that Divalproex sodium is more soluble in chloroform in compare to other solvents.
Melting Point
Melting point of drug was determined by capillary method. The result is found to be 219- 2230C.
EVALUATION OF PRE-COMPRESSION PARAMETERS
Table 12: Pre-compression parameters for IRL and SRL
|
Formulation |
Bulk Density Mean ± SD |
Tapped Density Mean ± SD |
Car’s Index Mean ± SD |
Haunsers Index Mean ± SD |
Angle of Repose Mean ± SD |
|
IF1 |
0.557±0.002 |
0.637±0.005 |
12.610±0.217 |
1.145±0.030 |
16.596±0.356 |
|
IF2 |
0.556±0.005 |
0.655±0.004 |
15.084±0.226 |
1.174±0.020 |
18.360±0.275 |
|
IF3 |
0.523±0.004 |
0.626±0.003 |
15.773±0.109 |
1.164±0.022 |
19.421±0.173 |
|
IF4 |
0.585±0.003 |
0.684±0.003 |
13.899±0.177 |
1.163±0.013 |
20.147±0.156 |
|
IF5 |
0.612±0.010 |
0.682±0.007 |
11.767±0.206 |
1.133±0.009 |
17.913±0.039 |
|
IF6 |
0.666±0.004 |
0.755±0.006 |
11.148±0.157 |
1.142±0.025 |
17.101±0.077 |
|
SF1 |
0.592±0.005 |
0.694±0.003 |
13.779±0.206 |
1.154±0.009 |
19.604±0.279 |
|
SF2 |
0.591±0.008 |
0.699±0.002 |
14.494±0.328 |
1.169±0.017 |
18.480±0.063 |
|
SF3 |
0.605±0.004 |
0.681±0.003 |
11.223±0.186 |
1.133±0.009 |
18.201±0.088 |
|
SF4 |
0.623±0.005 |
0.703±0.002 |
11.531±0.127 |
1.132±0.010 |
22.548±0.280 |
|
SF5 |
0.596±0.004 |
0.710±0.004 |
16.144±0.249 |
1.200±0.028 |
18.331±0.077 |
|
SF6 |
0.591±0.004 |
0.727±0.002 |
18.716±0.397 |
1.256±0.029 |
18.168±0.104 |
|
SF7 |
0.615±0.003 |
0.728±0.004 |
14.825±0.673 |
1.174±0.028 |
18.467±0.091 |
|
SF8 |
0.512±0.001 |
0.623±0.002 |
17.564±0.436 |
1.243±0.024 |
19.347±0.072 |
|
SF9 |
0.620±0.002 |
0.693±0.001 |
10.754±0.181 |
1.124±0.017 |
17.396±0.021 |
POST-COMPRESSION EVALUATION PARAMETERS:
Table 13: Post-compression parameters for IRL and SRL
|
Batch code |
Weight variation Mean ± SD |
Hardness (kg/cm2) Mean ± SD |
Friability (%) Mean ± SD |
Thickness Mean ± SD |
Drug content (%) Mean ± SD |
In vitro disintegration time (sec) Mean ± SD |
|
IF1 |
249.9±1.57 |
5.95±0.05 |
0.74±0.09 |
2.87±0.04 |
98.12±1.19 |
120.33±1.52 |
|
IF2 |
250.3±1.60 |
4.18±0.10 |
0.58±0.04 |
2.91±0.10 |
97.65±1.82 |
91.66±2.08 |
|
IF3 |
250.9±1.60 |
6.35±0.03 |
0.56±0.06 |
2.90±0.07 |
98.65±1.28 |
73.33±2.51 |
|
IF4 |
251.55±1.99 |
6.17±0.07 |
0.65±0.05 |
2.87±0.03 |
99.61±0.94 |
48.33±3.05 |
|
IF5 |
251.45±2.52 |
4.14±0.04 |
0.63±0.03 |
2.92±0.06 |
99.43±1.32 |
59.33±2.08 |
|
IF6 |
250.05±1.81 |
4.53±0.11 |
0.69±0.04 |
2.89±0.09 |
99.51±1.81 |
37.33±1.52 |
|
SF1 |
302.6±1.41 |
5.38±0.10 |
0.32±0.06 |
3.34±0.09 |
99.38±1.19 |
- |
|
SF2 |
302.9±2.29 |
4.33±0.02 |
0.35±0.02 |
3.30±0.14 |
98.61±1.03 |
-- |
|
SF3 |
302.5±1.59 |
6.14±0.04 |
0.43±0.03 |
3.31±0.03 |
97.43±1.28 |
- |
|
SF4 |
301.75±1.14 |
6.23±0.06 |
0.36±0.02 |
3.28±0.05 |
98.57±0.85 |
- |
|
SF5 |
300.65±1.37 |
5.14±0.03 |
0.41±0.06 |
3.30±0.06 |
98.43±1.27 |
- |
|
SF6 |
302.30±1.31 |
4.52±0.02 |
0.48±0.03 |
3.33±0.03 |
97.63±0.61 |
- |
|
SF7 |
303.20±1.46 |
6.74±0.04 |
0.42±0.06 |
3.28±0.08 |
99.47±1.04 |
- |
|
SF8 |
301.25±1.55 |
6.16±0.02 |
0.37±0.04 |
3.30±0.04 |
99.51±1.20 |
- |
|
SF9 |
302.42±1.04 |
6.56±0.03 |
0.31±0.03 |
3.32±0.07 |
98.49±0.93 |
- |
Table 14: Post-compression parameters for bi-layered tablet
|
Formulation |
Weight variation Mean ± SD |
Hardness Mean ± SD |
Friability Mean ± SD |
Thickness Mean ± SD |
Drug content (%) Mean ± SD |
|
BTF |
550.75±0.46 |
7.05±0.15 |
0.38±0.01 |
6.28±0.14 |
99.23±0.53 |
In-vitro dissolution study
Table 15: in vitro dissolution study of IRL
|
Time in min |
% CUMULATIVE DRUG RELEASE |
|||||
|
IF1 |
IF1 |
IF1 |
IF1 |
IF1 |
IF1 |
|
|
0 |
0.000±0.000 |
0.000±0.000 |
0.000±0.000 |
0.000±0.000 |
0.000±0.000 |
0.000±0.000 |
|
1 |
17.056±0.612 |
21.226±0.872 |
20.847±0.450 |
26.532±1.306 |
30.323±1.125 |
36.008±1.174 |
|
3 |
31.805±1.075 |
31.908±1.280 |
33.738±2.620 |
54.965±2.391 |
56.561±0.778 |
60.653±2.255 |
|
5 |
53.454±2.280 |
56.489±2.100 |
56.488±1.288 |
68.244±0.593 |
64.455±2.346 |
68.247±1.723 |
|
10 |
64.837±2.481 |
68.251±3.001 |
68.250±1.176 |
81.525±0.896 |
77.735±1.791 |
83.424±2.060 |
|
15 |
71.106±1.634 |
78.121±1.913 |
74.141±1.523 |
89.829±1.107 |
81.543±0.873 |
92.918±1.314 |
|
20 |
80.408±1.038 |
83.445±1.088 |
82.685±0.582 |
94.829±0.788 |
87.246±1.865 |
98.624±0.722 |
|
25 |
86.676±1.427 |
92.366±1.472 |
90.280±1.281 |
97.497±0.931 |
92.376±1.325 |
98.827±1.427 |
|
30 |
91.047±2.031 |
94.842±1.632 |
93.135±0.852 |
98.075±1.265 |
96.743±1.731 |
99.404±1.162 |

Figure 5: Release profile of immediate release layer
Table 16: In vitro dissolution study of SRL
|
Time in min |
% CUMULATIVE DRUG RELEASE |
|||||||
|
SF1 |
SF2 |
SF3 |
SF4 |
SF5 |
SF6 |
SF7 |
SF8 |
|
|
0 |
0.000±0.000 |
0.000±0.000 |
0.000±0.000 |
0.000±0.000 |
0.000±0.000 |
0.000±0.000 |
0.000±0.000 |
0.000±0.000 |
|
60 |
15.408±1.222 |
7.905±1.234 |
6.017±1.508 |
13.469±1.222 |
6.741±1.281 |
5.558±1.591 |
13.006±1.994 |
5.391±0.882 |
|
120 |
25.634±1.764 |
19.263±1.532 |
18.231±1.281 |
25.637±0.732 |
18.521±1.421 |
12.635±0.751 |
21.351±1.317 |
17.527±1.114 |
|
240 |
34.323±2.715 |
24.502±1.083 |
23.091±1.547 |
33.235±1.164 |
25.279±1.003 |
17.697±1.151 |
33.589±1.503 |
24.917±1.426 |
|
360 |
42.342±0.632 |
31.362±1.321 |
29.735±0.941 |
38.852±1.521 |
33.852±1.835 |
25.742±1.427 |
45.247±0.941 |
36.518±0.831 |
|
480 |
57.151±1.196 |
43.141±1.974 |
36.936±1.251 |
56.674±2.061 |
47.993±0.539 |
33.733±2.378 |
53.869±1.510 |
46.331±0.891 |
|
600 |
62.342±0.412 |
48.234±0.826 |
43.752±1.423 |
62.316±1.839 |
50.491±0.694 |
39.513±1.114 |
59.523±1.163 |
52.852±0.792 |
|
720 |
76.620±1.642 |
56.263±2.227 |
54.964±2.137 |
70.315±2.001 |
65.327±1.779 |
47.031±1.480 |
68.215±0.906 |
64.017±0.710 |
|
960 |
98.183±0.352 |
82.430±1.267 |
66.957±1.402 |
87.123±0.645 |
86.182±0.467 |
54.439±2.565 |
88.053±0.676 |
77.498±0.918 |
|
1080 |
101.512±1.093 |
97.816±0.630 |
84.113±1.317 |
98.822±1.325 |
97.692±0.844 |
67.057±1.191 |
100.859±2.165 |
94.298±0.560 |

Figure 6: Release profile of sustained release layer
Table 17: Dissolution study of Bi-layered Tablet
|
Time in min |
% CDR |
|
|
|
BTF |
|
|
IRL |
SRL |
|
|
0 |
0.000±0.000 |
0.000±0.000 |
|
10 |
83.424±1.063 |
- |
|
20 |
98.351±1.147 |
- |
|
30 |
99.413±0.731 |
- |
|
60 |
- |
5.384±1.032 |
|
120 |
- |
17.512±0.853 |
|
240 |
- |
23.483±1.520 |
|
360 |
- |
36.164±0.638 |
|
480 |
- |
46.054±0.825 |
|
600 |
- |
52.854±0.841 |
|
720 |
- |
64.781±0.527 |
|
960 |
- |
76.149±0.952 |
|
1080 |
|
95.823±0.614 |

Figure 7: Release profile of Bi-layered Tablet
Stability Studies:
Table 18: Stability data
|
Stability period |
400C / 75% RH |
||||
|
Hardness Mean ± SD |
% Friability Mean ± SD |
% Drug content Mean ± SD |
Drug release |
||
|
IRL (30 min) |
SRL (1080 min) |
||||
|
Initial |
7.05±0.67 |
0.36±0.01 |
99.23±0.532 |
99.413 |
95.823 |
|
1 month |
7.08±0.49 |
0.43±0.03 |
99.35±0.751 |
99.581 |
95.421 |
|
2 months |
6.41±0.49 |
0.56±0.06 |
98.96±0.792 |
99.142 |
94.736 |
|
3 months |
5.33±0.60 |
0.73±0.03 |
96.94±0.921 |
98.728 |
94.381 |
The bi-layered tablets were subjected to short term stability study, storing the formulation at 400C / 75% RH for 3 months. The data for stability studies revealed that no considerable differences in physical parameters, drug content and in vitro drug release rate were observed.
DISCUSSION-
The present work is a formulation and evaluation of bi-layer tablet of Divalproex sodium, which is used in treatment of epilepsy, bipolar disorders and used in prophylaxis of migraine, was carried out. In the project, different formulations of immediate release and sustained release layer have been prepared separately. From above formulations best formulation of each immediate and sustained release layers were selected according to the dissolution profile and bi-layered tablet was prepared. Divalproex sodium a broad-spectrum antiepileptic drug was chosen as a model drug as it is a right candidate for immediate as well as sustained release formulations. Divalproex sodium is soluble in 0.1 N NaOH, phosphate buffer pH 6.8, chloroform, methanol, ethanol (95%), and sparingly soluble in water. The result shown that the Divalproex sodium is more soluble in chloroform in compare to other solvents. The absorbance maximum of the Divalproex sodium was found to be at 210 nm when scanned in between 200-400 nm using methanol as well as phosphate buffer pH 6.8 solutions. Calibration curve of Divalproex sodium in methanol measured at 210 nm showed the slope of 0.0094 and regression coefficient of 0.9995.Best formulations for preparation of bi-layered tablet were selected depending upon the dissolution profile as all the formulation showed good content uniformity, friability, hardness and other physical parameters. Pre-formulation studies were carried out for all the formulation. Powder properties such as angle of repose, Carr’s index, Hausner’s ratio, bulk density, tapped density were determined which shown on tablet number 12. Pre-formulation studies for the formulations depicted bulk density 0.512 to 0.66 gm/cm3 which indicated packing characteristics in dies. The carr’s compressibility index was found to be below 18% which suggested good compressibility of blend. The values of Hausner ratio and angle of repose were found in the range of 1.13 to 1.25 and 16.59 to 22.54o respectively suggested excellent flow property of powder blend. Though the batch size of formulations were limited to 50-80, weight variation was reasonably satisfying the IP Limits as given in table no 9 and the drug content uniformity of all formulations was found to be 97.43-99.61 which indicated uniform distribution of drug in all batches of the formulations. Further hardness and friability was also between 4-6 kg/cm2 and less 1% respectively indicating stability of tablets against physical shocks.
CONCLUSION-
In the present work bi-layered tablet of Divalproex sodium were prepared by wet granulation method, using super disintegrants such as sodium starch glycolate and croscarmellose for immediate release layer and polymer like HPMC K4M and HPMC K100M for sustained release layer. Best formulations of each layer were selected for bi-layered tablet and bi-layered tablet were prepared. Bi-layered tablet of Divalproex sodium were subjected to hardness, weight variation, friability, drug content uniformity, in vitro drug release and drug polymer interaction. Based on the observations, it can be concluded that the formulated bi-layered tablets of Divalproex sodium using super disintegrants, release retardant polymers and different excipients was capable of exhibiting all the properties of bi-layered tablet. They are thus reducing the dose intake, minimize dose related adverse effect, cost and ultimately improve the patient compliance and drug efficiency. According to the in vitro dissolution profile date one formulation of each layer were selected for bi-layered tablet. IF6 from immediate release formulations as they showed 98.62 % drug release within 20 minutes. SF8 from sustained release formulation as they showed 94.29 % drug release within 18 hours. Both immediate and sustained release layer were prepared by wet granulation method and punched separately. The prepared tablets of both layers were evaluated for post compression parameters.the bilayer tablets were prepared using the selected immediate and sustained release layer. T prepared tablets were found to be good and free from chipping and capping. hardness of the prepared tablets was found to be in the range of 5.85 to 7.05 kg /cm2The low values of the standard deviation of average weight of the prepared tablets indicate weight uniformity within the batches prepared. friability of the prepared tablet was found to be less than 1%. percentage drug content was uniform in all the formulations of prepared bi-layered tablets .In vitro drug release pattern of the bi-layered tablets were same as individual layer tablets. The stability study showed that no significant changes in tablets after 3 months study.
REFERENCES


Agam Kumar Chaubey*, Ashok Baghel, Dinesh Sharma, Yogendra Singh, Formulation And Evaluation of Bi-Layered Tablet of Divalproex Sodium, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 3, 501-513. https://doi.org/10.5281/zenodo.14993024
 10.5281/zenodo.14993024
10.5281/zenodo.14993024
