1Department Of Pharmacology, Divine College of Pharmacy, Satana (Nashik), India
2Department Of Pharmaceutical Chemistry, Divine College of Pharmacy, Satana (Nashik), India
Blood cancer or hematologic malignancy, comprises a range of disorders affecting the bone marrow, lymphatic system and blood circulation, leading to severe complications such as anemia, immune dysfunction and bleeding disorders. This review explores the underlying mechanisms of blood cancer, emphasizing genetic mutations, chromosomal abnormalities, dysregulated signaling pathways, epigenetic modifications and immune system evasion. Understanding these factors provides insights into targeted therapeutic strategies. Additionally, the role of natural products in blood cancer treatment is gaining recognition due to their bioactive compounds with potential anticancer properties. Various phytochemicals exhibit anti-leukemic effects through mechanisms such as apoptosis induction, oxidative stress modulation, and inhibition of key cancer-related pathways. Medicinal plants have demonstrated promising anticancer activity. This review highlights the significance of natural products in the development of novel blood cancer treatments and calls for further research and clinical validation to integrate these compounds into therapeutic regimens effectively.
Blood cancer, also known as hematologic malignancy, is a group of disorders characterized by the uncontrolled proliferation of abnormal blood cells, affecting the bone marrow, lymphatic system, and blood circulation. These malignancies disrupt normal hematopoiesis, impair immune function, and lead to severe clinical manifestations, including anemia, increased susceptibility to infections, and bleeding disorders. Blood cancers primarily originate from mutations in hematopoietic stem cells, resulting in the aberrant growth of leukocytes, erythrocytes, or platelets [1]. The three major categories of blood cancer include leukemia, lymphoma, and multiple myeloma. Leukemia is a malignancy of the bone marrow and blood, wherein abnormal white blood cells proliferate uncontrollably, hindering the production of normal blood cells [2,3]. Lymphoma affects the lymphatic system, leading to the abnormal growth of lymphocytes, which compromises immune function. Multiple myeloma, on the other hand, is characterized by the excessive proliferation of plasma cells in the bone marrow, resulting in complications such as bone lesions, kidney dysfunction and immunodeficiency [4].
Figure 1: Blood cancer
The exact etiology of blood cancer remains multifactorial, with genetic predisposition, environmental factors, viral infections, and exposure to carcinogens playing significant roles. Genetic mutations in key regulatory genes, such as TP53, JAK2, and BCR-ABL, have been implicated in the pathogenesis of hematologic malignancies. Additionally, factors such as ionizing radiation, exposure to benzene, and viral infections (e.g., Epstein-Barr virus, human T-cell leukemia virus) contribute to the development of blood cancers [5]. Advancements in diagnostic modalities, including molecular profiling, cytogenetics, and next-generation sequencing, have enhanced our understanding of blood cancer pathophysiology. Early detection through hematological tests, bone marrow biopsy, and flow cytometry has improved patient prognosis and treatment outcomes. Conventional therapies such as chemotherapy, radiotherapy, and hematopoietic stem cell transplantation (HSCT) remain the cornerstone of blood cancer treatment. However, recent advancements in targeted therapy, immunotherapy, and CAR-T cell therapy have revolutionized treatment approaches, offered improved survival rates and reduced adverse effects [6,7]. Despite significant progress in blood cancer research, challenges persist in treatment resistance, disease relapse, and managing therapy-induced complications. Further exploration of precision medicine, novel biomarkers, and gene-editing technologies holds promise in overcoming these obstacles and enhancing patient outcomes [8]. This review aims to provide a comprehensive overview of blood cancer, covering its epidemiology, pathophysiology, diagnostic approaches, and recent advancements in therapeutic strategies. By elucidating the current understanding of hematologic malignancies, this article seeks to contribute to the ongoing efforts in developing more effective and personalized treatment modalities for patients battling blood cancer.
Types of Blood Cancers
Blood cancers are broadly classified into three main types: leukemia, lymphoma, and multiple myeloma. Each type has subcategories that vary in pathophysiology, clinical presentation, and treatment approaches.
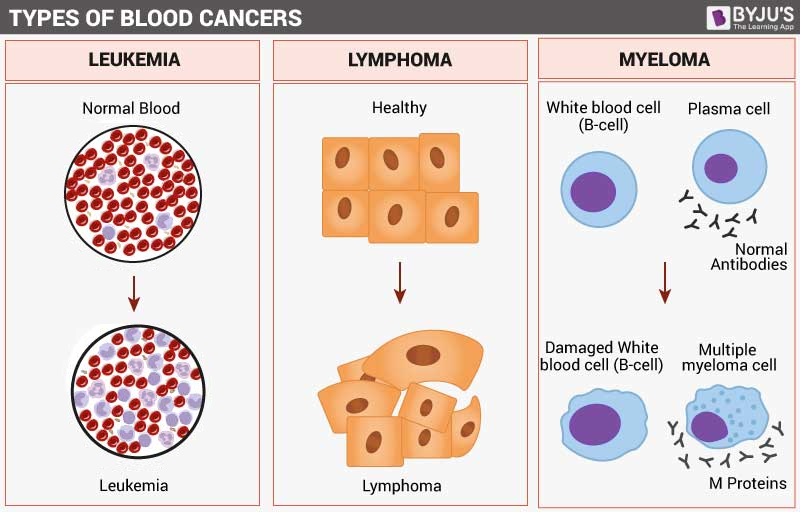
Figure 2: Types of Blood cancer
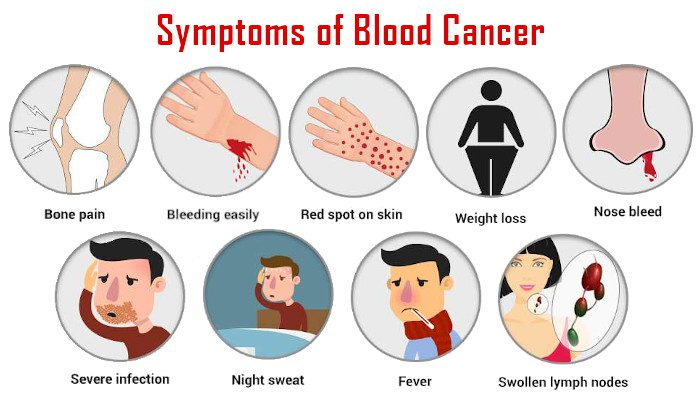
Figure 3: Symptoms of Blood cancer
Causes of Blood Cancer
Blood cancer arises from a combination of genetic, environmental and lifestyle factors.
Genetic Mutations
Inherited mutations in genes like TP53, BRCA1, and BRCA2 increase susceptibility. Somatic mutations, such as BCR-ABL translocation in CML, drive malignant transformation, leading to uncontrolled cell growth and impaired regulation of normal blood cell production.
Exposure to Radiation and Chemicals
Ionizing radiation from medical treatments or environmental exposure significantly raises the risk of developing blood cancers. Carcinogens like benzene and formaldehyde are well-documented contributors to DNA mutations, leading to hematologic malignancies.
Viral Infections
Certain viruses are closely linked to the development of blood cancers. Epstein-Barr virus (EBV) is associated with Burkitt’s lymphoma and Hodgkin lymphoma, while Human T-cell leukemia virus (HTLV-1) has been implicated in adult T-cell leukemia/lymphoma.
Weakened Immune System
Individuals with compromised immune function, such as those with autoimmune disorders or undergoing immunosuppressive therapy (e.g., organ transplant patients), have an increased likelihood of developing blood cancers due to reduced immune surveillance.
Lifestyle Factors
Smoking has been linked to an elevated risk of acute myeloid leukemia (AML) and other hematologic malignancies. Additionally, poor dietary habits, obesity, and a sedentary lifestyle contribute to overall cancer risk and progression.
Family History
A family history of leukemia, lymphoma, or multiple myeloma significantly raises an individual's predisposition to developing blood cancer. Genetic predisposition plays a crucial role in determining susceptibility to hematologic malignancies [12-14].
Mechanism of Blood Cancer
The development of blood cancer is driven by a series of genetic, molecular, and environmental factors that disrupt normal hematopoiesis and immune regulation. The primary mechanisms involved in the pathogenesis of blood cancers include:
Genetic alterations play a crucial role in the initiation and progression of blood cancer. Mutations in tumor suppressor genes (e.g., TP53, RUNX1) and oncogenes (e.g., JAK2, BCR-ABL) lead to uncontrolled cellular proliferation, apoptosis resistance, and impaired differentiation of hematopoietic cells. Chromosomal translocations, such as the Philadelphia chromosome (t [9;22]) in chronic myeloid leukemia (CML), result in the formation of fusion proteins that drive cancerous growth [15].
Aberrant activation of signaling pathways such as JAK-STAT, PI3K-AKT, and NF-κB contributes to sustained cell survival, proliferation, and evasion of immune surveillance. These pathways promote the expansion of malignant blood cells while suppressing normal hematopoietic differentiation.
Epigenetic modifications, including DNA methylation, histone acetylation, and chromatin remodeling, affect gene expression in hematologic malignancies. Dysregulation of epigenetic regulators such as DNMT3A and TET2 leads to aberrant stem cell self-renewal and leukemic transformation [16].
The bone marrow microenvironment provides critical support for hematopoietic cells through cytokines, growth factors, and stromal cell interactions. In blood cancer, the microenvironment becomes altered, favoring the proliferation and survival of malignant cells while inhibiting normal hematopoiesis. In multiple myeloma, for example, bone marrow stromal cells secrete interleukin-6 (IL-6), which promotes myeloma cell growth and drug resistance [17].
Cancerous blood cells employ multiple mechanisms to evade immune detection, including downregulation of major histocompatibility complex (MHC) molecules, production of immunosuppressive cytokines, and induction of regulatory T cells (Tregs). This immune evasion facilitates the unchecked growth of malignant cells.
Apoptosis, or programmed cell death, is a crucial process in maintaining normal cell populations. Blood cancers often involve mutations in pro-apoptotic (e.g., BAX) or anti-apoptotic (e.g., BCL-2) genes, leading to resistance against cell death and enhanced survival of malignant cells.
Certain viruses, such as the Epstein-Barr virus (EBV) and human T-cell leukemia virus type 1 (HTLV-1), contribute to blood cancer development by integrating their genetic material into host cells, leading to oncogenic transformation. For instance, EBV is strongly associated with Burkitt's lymphoma and Hodgkin’s lymphoma [18-20].
Diagnosis of Blood Cancer
Blood cancer is diagnosed through a combination of laboratory tests, imaging studies, and biopsies. Common diagnostic methods include:
Role of Natural Products in Blood Cancer
Natural products, especially plant-based medicines and remedies have been studied since time immemorial due to their therapeutic effectiveness against various maladies and illnesses. This prompted the exploration and isolation of numerous phytoconstituents with clinical benefits and these compounds have had profound impacts in medical science. For cancer therapy, up to 60% of anticancer candidates in clinical use that exhibited significant efficacy are natural product derivatives [23]. They serve as good sources of lead molecules and offer affordable materials in modern drug discovery. Plant-based natural products cause fewer undesirable side effects probably due to their similarity with chemical entities found in the human diet that have significant tolerance induction ability. The secondary metabolites of plants such as flavonoids, tannins, alkaloids and terpenoids are well known to possess substantial anticancer capabilities. They trigger, promote or modulate the metabolic pathways that can alter proliferation, migration and apoptosis in cancer cells via a multitude of biological mechanisms. Thus, not surprisingly phytoconstituents are the principal sources of chemotherapeutic drug investigations in preclinical and clinical studies of cancer. For instance, paclitaxel, a plant alkaloid was discovered in 1962 while screening natural products for treatment of cancer. It is commercially marketed in the name of Taxol® and has become one of the most effective drugs till date against breast and ovarian cancer [24]. The drug development process from its source to a finished product is an extremely costly and complex process that can take 12–15 years. The toxicity of natural products and isolated compounds is a major concern in drug discovery and development. Therefore, an in-depth investigation for safer natural drugs is always a prerequisite. Preclinical and clinical phases for the new chemical entities (NCEs) are important obligatory steps in drug development to assess the safety and efficacy of the test compound with an aim to predict any potential adverse events that may result after treatment. Toxicity tests are also imperative to identify the relationship between a dose, its potential side effects, anomalies on genetic material and on vital organs as well as to estimate toxicokinetic profiles. Besides, some of the major challenges encountered during drug development are low solubility, functional group reactivity, molecular complexity, and instability of investigational new drugs [25]. Therefore, the current review is an attempt to summarise a few plant extracts and phytoconstituents that are in the limelight in the past decade for significant anticancer activity.
1. Vincristine
Vincristine is a potent anticancer alkaloid derived from the Madagascar periwinkle plant (Catharanthus roseus). It belongs to the vinca alkaloid class and plays a crucial role in cancer therapy, particularly for hematological malignancies. Vincristine works by binding to tubulin proteins, which are essential for microtubule formation. By inhibiting microtubule polymerization, it prevents the proper formation of the mitotic spindle, leading to cell cycle arrest in metaphase and ultimately inducing apoptosis in rapidly dividing cancer cells. Due to its mechanism of action, vincristine is widely used in the treatment of acute lymphoblastic leukemia (ALL), Hodgkin’s lymphoma, and non-Hodgkin’s lymphoma. It is often included in combination chemotherapy regimens such as CHOP (cyclophosphamide, doxorubicin, vincristine, prednisone) for lymphomas. However, vincristine's clinical use is limited by dose-dependent neurotoxicity, which can cause peripheral neuropathy, making careful dose adjustments necessary [26].
2. Vinblastine
Vinblastine is another vinca alkaloid derived from the Madagascar periwinkle plant (Catharanthus roseus), sharing a similar mechanism of action with vincristine. It disrupts microtubule formation by binding to tubulin, inhibiting spindle fiber assembly during mitosis, and thereby halting cancer cell proliferation. However, vinblastine exhibits a slightly different toxicity profile compared to vincristine, with more pronounced myelosuppression but less neurotoxicity. This makes it an important chemotherapeutic agent in the treatment of Hodgkin’s lymphoma, non-Hodgkin’s lymphoma, and multiple myeloma. It is commonly used in the ABVD regimen (Adriamycin, Bleomycin, Vinblastine, Dacarbazine) for Hodgkin’s lymphoma. Due to its bone marrow-suppressing effects, careful monitoring of white blood cell counts is required to avoid severe neutropenia and infection risk [26,27].

3. Etoposide
Etoposide is a semi-synthetic derivative of podophyllotoxin, originally extracted from the American Mayapple plant (Podophyllum peltatum). This drug is classified as a topoisomerase II inhibitor, meaning it interferes with the enzyme responsible for relaxing supercoiled DNA during replication. By stabilizing the DNA-topoisomerase II complex, etoposide causes double-stranded DNA breaks, which leads to the accumulation of DNA damage and eventual apoptosis of cancer cells. It is a key component in the treatment of acute myeloid leukemia (AML) and Hodgkin’s lymphoma, often used in combination with other chemotherapeutic agents [28]. Etoposide is administered either orally or intravenously, and its effectiveness depends on cell cycle specificity, primarily targeting cells in the S and G2 phases of the cell cycle. However, one of its major drawbacks is bone marrow suppression, which can lead to anemia, leukopenia, and increased infection risk. Long-term use is also associated with an elevated risk of secondary leukemias.

Figure 5: Podophyllum peltatum
4. Homoharringtonine (Omacetaxine Mepesuccinate)
Homoharringtonine, also known as Omacetaxine mepesuccinate, is a plant alkaloid derived from the Chinese plum yew (Cephalotaxus harringtonia). It functions primarily as a protein synthesis inhibitor, disrupting the elongation phase of mRNA translation. This leads to a depletion of short-lived survival proteins, particularly affecting leukemic cells that rely on continuous protein synthesis for survival. Homoharringtonine has shown remarkable efficacy against chronic myeloid leukemia (CML), including cases that have developed resistance to tyrosine kinase inhibitors (TKIs) such as imatinib. This makes it a valuable treatment option for patients who have failed conventional targeted therapies. Unlike vinca alkaloids and etoposide, its primary toxicity is related to hematological side effects, including thrombocytopenia and neutropenia, rather than neurotoxicity. Despite these side effects, it remains a vital option for refractory CML cases, particularly in patients who do not respond to BCR-ABL inhibitors [29].

Figure 6: Cephalotaxus harringtonia
CONCLUSION
Natural products have played a pivotal role in the treatment of blood cancers, with these four drugs demonstrating remarkable efficacy and unique mechanisms of action. Vincristine and vinblastine target microtubules, etoposide inhibits topoisomerase II, and homoharringtonine disrupts protein synthesis, all leading to cancer cell death. While these drugs are highly effective, they come with distinct toxicity profiles that require careful management. As research progresses, new derivatives and combination therapies continue to improve survival outcomes and minimize side effects in hematological malignancies.
REFERENCES


Kiran Aher, Nandini Bagul, Manjusha Chavan, Gaurav Kasar*, Dipti Chavan, Dr. Chandrashekhar Patil, Dr. Sunil Mahajan, Advances in Blood Cancer: Pathophysiology, Diagnosis and Emerging Therapeutic Strategies, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 5, 4218-4228. https://doi.org/10.5281/zenodo.15512403
 10.5281/zenodo.15512403
10.5281/zenodo.15512403
