ST Pauls College of Pharmacy, Turkayamjal, Ibrahimpatnam.
To protect public health, pharmacovigilance—which monitors the safety of medications throughout their life cycle—is crucial. Underreporting, delays, and fragmented data frequently restrict the efficacy of standard pharmacovigilance systems. Manual data review and spontaneous adverse drug reaction (ADR) reporting are the fundamental pillars of these systems. The rise of digital health ecosystems and the rapid accumulation of diversified, large-scale healthcare data, or Big Data, have led to an increasing interest in integrating artificial intelligence (AI) to improve pharmacovigilance outcomes. This analysis centers on the ways in which artificial intelligence (AI) technologies—like machine learning, deep learning, and natural language processing (NLP)—are altering traditional techniques for identifying ADRs. Real-time monitoring, improved pattern identification, and early signal detection are all made feasible by AI algorithms’ capacity to handle organized and unstructured data from a range of sources. Regulatory agencies and the pharmaceutical industry have demonstrated through case studies and ongoing applications how AI may be used to automate safety procedures and improve post-marketing surveillance. But in order to ensure safe and effective adoption, problems like model transparency, data heterogeneity, regulatory alignment, and ethical considerations must be fixed. Ultimately, the integration of AI and Big Data analytics into pharmacovigilance signifies a paradigm shift towards a more proactive, accurate, and scalable drug safety monitoring system.
The scientific and regulatory discipline of pharmacovigilance is concerned with the detection, assessment, and prevention of adverse drug reactions (ADRs) and other drug-related problems. Ensuring the long-term safety of medications is crucial, particularly when they are introduced to the market and utilised by a larger patient population. Effective pharmacovigilance can lead to the detection of rare, severe, or delayed side effects that may not have been apparent during clinical[1]. Historically, this process has been facilitated by systems like as the FDA’s FAERS, WHO’s VigiBase, and EMA’s EudraVigilance, which gather safety data from makers, medical experts, and sometimes patients through spontaneous reporting procedures. Despite their importance throughout history, traditional pharmacovigilance methods have a number of shortcomings[2].Research shows that over 90% of adverse medication reactions globally go unreported, making underreporting the most important of them. Manual case review processes are time-consuming and resource-intensive, which often result in slow regulatory action and delayed signal identification[3].Important data from real-world contexts, such as clinical notes, patient experiences, and post-discharge observations, are also commonly overlooked since organised, voluntary reports are used[4].Conventional pharmacovigilance methods are less responsive and effective overall, and these issues are exacerbated by fragmented data storage and a lack of system compatibility[5].
3.1) Big Data Analytics and AI Ascents in Healthcare:
The Rise of Big Data Analytics and AI in Healthcare:
Large volumes of health-related data have been produced as a result of the healthcare industry’s recent dramatic shift towards digitalisation[6].Examples include electronic health records (EHRs), laboratory reports, medical imaging, and real-world data from wearable technology, mobile apps, and social media platforms[7].The explosion of high-velocity, heterogeneous data, known as “Big Data,” has great promise for enhancing drug safety monitoring[8].Its vast size and complexity, however, make it difficult to manage using conventional pharmacovigilance techniques[9].There is currently growing interest in applying Artificial Intelligence (AI) technologies, particularly machine learning (ML), natural language processing (NLP), and deep learning, to pharmacovigilance in order to make it a more proactive, intelligent, and scalable system as explained in the figure no 1[10].
Figure 1: It explains about the AI in pharmacovigilance
Near-real-time signal detection, complex pattern recognition in multi-modal datasets, and automatic extraction of ADR-related information from unstructured text are all made possible by AI as we can see in the below table no 1[11].
Table 1: Strategic Focus Area in AI Driven Pharmacovigilance:
|
Key Area |
Description |
Impact on ADR Detection |
|
Ai technologies in drug safety |
Utilisation of Machine learning, deep learning and NLP for analysing ADR Data |
Enhances Speed, accuracy and scalability of pharmacovigilance systems |
|
Big data integration |
Aggregation of Ehrs, spontaneous reports, social media and digital health data |
Enables comprehensive,multi source signal detection |
|
Real time signal detection |
Continuous monitoring and predictive modeling of ADRs |
Facilitates earlier risk identification and response |
|
Regulatory and Industry implementations |
FDA Sentinel,EU-ADR,Pharma AI pipelines |
Demonstrates practical viability and integration of Ai tools |
|
Algorithmic transparency and Bias |
Interpretability of black-box models, fairness across populations |
Supports ethical AI adoption in public health |
|
Future-proofing pharmacovigilance |
Federated learning, blockchain, explainable AI(XAI) |
Builds a secure, adaptable and trustworthy ecosystem |
3.2) AIM And Scope Of Review: This study aims to provide a comprehensive overview of recent developments and possible future directions in this rapidly evolving sector, because AI and Big Data analytics have the ability to completely transform pharmacovigilance capabilities[12].It explores how AI technologies are being utilised to improve the detection and assessment of adverse events, with an emphasis on real-world applications, state-of-the-art research, and case studies from regulatory agencies and the pharmaceutical industry[13].Data quality, algorithm interpretability, regulatory acceptance, and ethical considerations are some of the challenges that need to be addressed for the safe and effective incorporation of AI in pharmacovigilance workflows[14].This article attempts to synthesise current information and identify significant gaps to enable academics, physicians, and regulatory stakeholders come closer to a more dependable and data-driven approach to medication safety monitoring as we can see clearly in the table no 2[15].
Table 2: Core Objectives in AI Based Adverse Event Surveillance
|
Specific Aim |
Execution In the Context of AI Driven Pharmacovigilance |
|
Deploy AI to streamline adverse event recognition |
Use ML/NLP to analyse spontaneous reports, literature and social data |
|
Integrates heterogeneous real-world datasets |
Combine EHRS, mobile apps and online health discourse for richer insights |
|
Illustrate cross-sector application |
Highlight regulatory adoption and pharma innovation in ADR analytics |
|
Address risk of automation and Ai misuse |
Tackle data quality, explainability, privacy and ethical deployment changes |
|
Inspire next generation pharmacovigilance design |
Promote Ai systems that support precision medicine and patient- centred safety |
4) Methodology Of Literature Search: The application of artificial intelligence (AI) and big data analytics in pharmacovigilance was the subject of a comprehensive literature search to locate relevant peer-reviewed papers, regulatory documents, and technical reports. PubMed, Scopus, Web of Science, and Google Scholar were among the databases used in the search method, which focused on material published between January 2010 and April 2024. Specific keywords and search strings were created using Boolean operators and Mesh phrases in order to refine the results. “Pharmacovigilance,” “adverse drug reactions,” “AI in drug safety,” “machine learning pharmacovigilance,” “natural language processing ADR,” “Big Data healthcare analytics,” “signal detection artificial intelligence,” as well as combinations such as “(AI OR machine learning) AND (pharmacovigilance OR ADR detection)” were the primary searches.The FDA, EMA, and WHO–Uppsala Monitoring Centre regulatory databases were searched manually in order to locate reports, guidelines, and case studies pertaining to AI-assisted pharmacovigilance systems. Articles in English that discussed the development, application, or evaluation of artificial intelligence (AI), machine learning, natural language processing, or big data techniques in the context of pharmacovigilance were eligible for inclusion. We looked at studies on ADR detection, risk assessment, signal prioritisation, and post-marketing surveillance. The exclusion criteria were abstracts without full-text access, opinion pieces, research not directly related to pharmacovigilance or artificial intelligence, and articles written in languages other than English. Publications that solely addressed clinical trial pharmacovigilance without any post-marketing importance or duplicate records were also excluded. The complete text, abstract, and title of the literature were further screened to ensure that it was relevant to the review’s objectives.
5) Fundamentals Of Pharmacovigilance: According to the World Health Organisation (WHO), pharmacovigilance is “the science and activities relating to the detection, assessment, understanding, and prevention of adverse effects or any other drug-related problem’’[16].Maintaining public confidence in pharmaceutical interventions and ensuring patient safety are made possible by routinely evaluating the benefit-risk profile of pharmaceutical products throughout their lifespan[17].Particularly in light of the growing complexity of drugs, their worldwide distribution, and post-marketing exposures that go beyond the controlled environments of clinical trials, the significance of pharmacovigilance has significantly increased in recent decades[18].Effective pharmacovigilance enables safer prescribing practices, timely identification of adverse drug reactions (ADRs), and regulatory judgements about product withdrawals, safety label modification, and risk mitigation tactics[19].Pharmacovigilance is subject to a robust, globally standardised regulatory framework[20].EudraVigilance is administered by the European Medicines Agency (EMA), the FDA (FDA Adverse Event Reporting System) is administered by the FDA, and Vigi Base, a global ADR repository used by over 130 countries, is administered by the WHO-Uppsala Monitoring Centre[21].These regulatory agencies are opening up to integrating Big Data analytics and Artificial Intelligence (AI) into pharmacovigilance processes to increase responsiveness and efficiency[22].They also establish rules for gathering data, determining causality, identifying signals, and communicating risks[23].A variety of sources are used to collect data on adverse events. Traditional avenues include individual case safety reports (ICSRs), spontaneous reporting systems (SRS), and post-marketing surveillance studies[24].Clinical narratives, insurance claims, patient registries, and electronic health records (EHRs) are examples of real-world data (RWD), which has increased in popularity in recent years[25]. Additionally, new sources of patient-reported outcomes have emerged from digital platforms such mobile health apps, social media, and online health forums[26].The requirement for advanced tools for aggregation, cleaning, and analysis due to the diverse and dynamic nature of data sources emphasises the need for AI-driven approaches to modernise pharmacovigilance systems and enable more comprehensive through mobile health apps or social media as explained in the figure no 2[27].
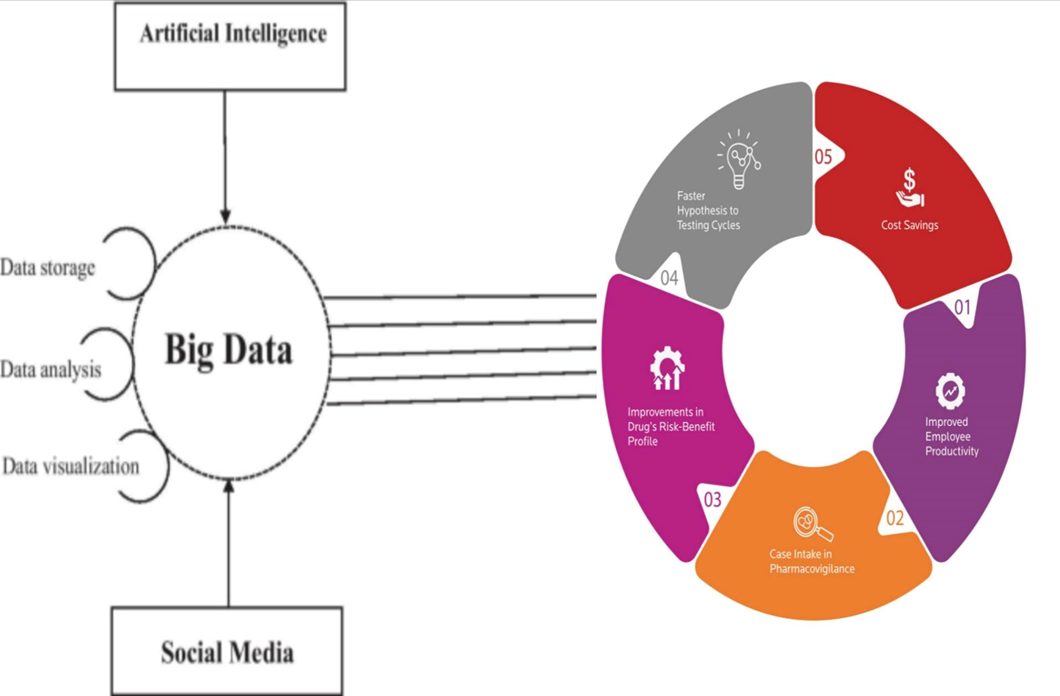
Figure No 2: We Can See the Advantages of Big Data Analytics in Above Figure
“Big data” refers to large, complex, and high-dimensional datasets that are not effectively processed or analysed using traditional data management technologies [28].
6) Role Of Big Data in Pharmacovigilance:
Pharmacovigilance uses the term “big data” to describe a wide range of information sources, such as genomics, wearable device outputs, clinical trial databases, insurance claims, electronic health records (EHRs), and patient-reported outcomes obtained through mobile health apps or social media[29].The “3Vs”—Velocity (the speed at which new data is generated and must be processed immediately), Variety (the range of data formats, including structured data like numerical lab values and unstructured data like doctor notes or online data), and Volume (the massive amount of data generated continuously across global healthcare systems)—are frequently used to describe the distinctive characteristics of big data. Big Data enables pharmacovigilance to shift from a reactive, passive paradigm to a predictive, proactive strategy. Multiple real-world data sources can be combined to better capture unusual occurrences, examine adverse drug reaction (ADR) patterns across a variety of populations, and detect safety signals earlier and more precisely[30].Big data also contributes to the personalisation of pharmacovigilance by offering insights into the ways in which genetic, behavioural, or demographic factors impact drug response and risk. However, the use of big data in pharmacovigilance presents some challenges. Heterogeneous datasets are inherently difficult to clean, harmonise, and interpret; data fragmentation amongst institutions; concerns about data privacy and governance; and a lack of standardisation in data formats and terminologies[31].
7) Role Of Artificial Intelligence in Pharmacovigilance:
Artificial intelligence (AI) is becoming seen as a transformative force in pharmacovigilance because to its great capacity to analyse vast, diverse, and complex datasets pertaining to drug safety monitoring[32].Without explicit programming, systems may learn from historical data and make inferences thanks to two of artificial intelligence’s most significant subfields: machine learning (ML) and deep learning (DL). Decision trees, support vector machines (SVM), random forests, and gradient boosting are machine learning methods that perform particularly well when processing structured datasets, such as spontaneous reports and claims data[33].These algorithms have the ability to stratify risk, rank cases for review, and identify previously unknown drug-event correlations. Deep learning uses multi-layered artificial neural networks, such as CNNs and RNNs, to analyse unstructured data such as social media material, clinical narratives, and electronic health records[34].Transformer-based models, such as BERT (Bidirectional Encoder Representations from Transformers), which have gained popularity in recent years, significantly improve natural language processing (NLP) tasks related to the extraction and interpretation of adverse medication reactions. AI has also altered signal identification methods such as Bayesian Confidence Propagation Neural Networks (BCPNN) and Proportional Reporting Ratios (PRR), which were previously dependent on disproportionality analysis. Modern AI systems can use multidimensional data, such as demographics, temporal trends, medicine combinations, and narrative context, to detect subtle or intricate safety signs as we can see in the table 3 & 4[35].
Table 3: Deep learning algorithms in Pharmacovigilance
|
Algorithm |
Application In Pharmacovigilance |
|
Convolutional Neural Networks (CNNs) |
Image based ADR Data or Sentence level ADR classification from clinical text |
|
Recurrent Neural Networks (RNNs) |
Sequence modelling of patient timelines, longitudinal EHR data |
|
Long Short-Term Memory (LSTM) |
Temporal detection of drug-event relationships over time |
|
Transformer models e.g.(BERT, BioBERT) |
Advanced NLP for extracting Adrs from literature and case reports |
Table 4: Signal detection algorithm in Pharmacovigilance
|
Algorithm |
Application In Pharmacovigilance |
|
Proportional reporting ratio (PRR) |
Measures disproportionate reporting of drug event combinations |
|
Reporting odds ratio (ROR) |
Compares odds of an Adr with drug vs all other drugs |
|
Bayesian confidence Propagation Neural Network(BCPNN) |
Probabilistic modeling used in WHOs VigiBase |
|
Emperical bayes geometrical mean(EBGM) |
Reduce false positives in signal detection |
|
Multi item Gamma Poisson shrinker (MGPS) |
Signal detection in large spontaneous report datasets (used in FDAs system) |
8) Ethical, Legal and Regulatory Considerations:
The integration of artificial intelligence (AI) and big data analytics raises difficult ethical, legal, and regulatory challenges that pharmacovigilance must address to ensure safe, equitable, and compliance use.Data privacy and patient permission are important concerns, especially when using private health information from electronic health records (EHRs), mobile health apps, and social media. Utilising such data necessitates strict adherence to global data protection standards, including the General Data Protection Regulation (GDPR) in the EU and the Health Insurance Portability & Accountability Act (HIPAA) in the US. These regulations require that patients be notified about the gathering, storing, and use of their data, and that any personally identifying information about them be de-identified or anonymised. Furthermore, especially in multinational pharmacovigilance collaborations, the extensive use of data for secondary purposes in AI modelling raises questions about informed permission and the appropriate level of data reuse[36].Accountability and openness of algorithms; Many AI models, particularly those based on deep learning, function as “black boxes,” making it difficult for developers, regulators, and even medical professionals to comprehend how outcomes are generated. This inability to be explained hinders the implementation of regulations and erodes confidence. Explainable AI (XAI) frameworks are being developed to provide interpretable insights into decision logic, feature importance, and model behaviour In the event of errors, biases, or unexpected outcomes, transparent algorithms are essential for both ethical validation and accountability. The establishment of clear documentation, audit trails, and validation procedures is crucial to ensuring that AI systems in pharmacovigilance are both legally and scientifically sound. Conformity with global regulatory standards; International regulatory criteria must also be strictly followed when integrating AI technology into official medication safety monitoring systems[37].The European Medicines Agency (EMA), the International Council for Harmonisation (ICH), and the U.S. Food and Drug Administration (FDA) are among the organisations that are increasingly recognising the importance of artificial intelligence (AI) and real-world evidence (RWE) in post-marketing surveillance. Several frameworks, including TRIPOD-AI, CONSORT-AI, and the FDA’s Action Plan for AI/ML-based Software as a Medical Device, are being created to standardise model development, validation, and reporting. These regulatory conditions must be met for AI tools to be extensively utilised and approved. In conclusion, while AI has the potential to completely transform pharmacovigilance, its success hinges on international regulatory harmonisation, privacy, and openness[38].
9) Challenges And Limitations:
Although AI-driven pharmacovigilance has seen some hopeful advancements, a number of important barriers and limitations still stand in the way of its broad use and effectiveness. Two major issues are inherent bias and the quality of the data. In the context of pharmacovigilance, the quality of input data—which often originates from a variety of unreliable sources, including as social media, electronic health records (EHRs), and spontaneous reporting systems—is essential to the precision and reliability of AI models. These data could be missing, unstructured, or inconsistently coded, creating noisy inputs that could skew model results. Selective and underreported adverse event data also introduce sample bias, which can lead to models that misrepresent the true safety profile of drugs, particularly when comparing individuals from different demographic and geographic backgrounds as simply explained in the figure no 3[39].

9.1) Model Interpretability:
An other significant disadvantage of the approach is its interpretability. Many state-of-the-art algorithms, especially deep learning models like neural networks and transformers, operate as complex “black boxes,” offering superior prediction accuracy but limited insight into the mechanisms that underlie decision-making. This lack of transparency is a major challenge in pharmacovigilance, as regulators and physicians want an understandable and evidence-based explanation for any safety-related decisions or actions. It is difficult to test, audit, or defend the outcomes produced by AI systems when interpretability is inadequate, which erodes confidence and delays regulatory adoption. Limits on infrastructure and resources; In addition, infrastructural and resource constraints remain a major barrier, particularly for smaller pharmaceutical firms or in low- and middle-income countries[40].
10) Future Perspectives:
Future developments in digital health infrastructure, artificial intelligence (AI), and data science have the potential to drastically alter pharmacovigilance. One of the most intriguing advancements in pharmacovigilance systems is the integration of state-of-the-art technologies such as explainable AI (XAI), block chain, and federated learning. Federated learning preserves patient privacy while increasing model resilience by enabling the collaborative training of AI models across several data sources without necessitating the transfer of sensitive patient data. The traceability and transparency of safety data are essential for data integrity and regulatory audits, and block chain technology offers these features through immutable, decentralised record-keeping. Explainable AI frameworks are making it easier to comprehend black-box models and provide important insights into model decision-making, which are crucial for boosting regulators and doctors’ trust. Another big shift that will happen soon is the rise of personalised pharmacovigilance, which aligns with precision medicine’s overarching objective. Artificial intelligence (AI) can help predict the probability of adverse drug reactions (ADRs) at the individual level by combining genetic data, lifestyle information, comorbidities, and empirical evidence, rather than relying solely on population-based signals. This would make it possible for doctors to more successfully and safely tailor pharmacological treatments, especially for patients who have unique polypharmacy risks or pharmacogenomic profiles. Personalised pharmacovigilance also supports more dynamic risk management strategies, as AI models continuously update risk evaluations based on fresh patient-specific data.
11) CONCLUSION:
A synopsis of the main conclusions With the merging of artificial intelligence and Big Data analytics, pharmacovigilance is experiencing a paradigm change that offers new methods to address long-standing issues with adverse drug reaction detection and drug safety monitoring. In particular, machine learning, deep learning, and natural language processing are examples of artificial intelligence (AI) technologies that have been highlighted in this review as having the potential to enhance signal detection, automate case processing, and extract valuable insights from a wide range of diverse and high-volume datasets, such as electronic health records, literature, social media, spontaneous reports, and more. Utilising these technologies has already been demonstrated to improve timeliness, scalability, and forecast accuracy in both regulatory and industry settings. The present obstacles to broad adoption, including as concerns about data quality, algorithm openness, and the requirement for robust ethical and legal frameworks, are also acknowledged in this analysis. The overall significance of this transformation lies in the possibility of moving away from reactive pharmacovigilance and towards a more proactive, predictive, and customised approach to medication safety. Near real-time decision-making, personalised risk profiling, and early signal detection may be made possible by AI-driven pharmacovigilance with further advancements in explainable AI, real-world data integration, and regulatory harmonisation. These advancements could ultimately lead to safer treatments and improved patient outcomes. Pharmacovigilance needs to stay up with the continuous digital transformation of healthcare by embracing technology innovation while upholding the scientific rigour and ethical responsibility that define the sector. Data scientists, physicians, regulators, and pharmaceutical stakeholders may work together to realise the goal of a fully connected, intelligent, and responsive drug safety ecosystem. This is becoming more and more necessary.
Conflicts Of Interest:
The authors declare no conflicts of interest related to the subject matter of this review.
Funding Statement:
This work is a pure systemic review and has no specific funding or financial support.
REFERENCES

G. Madhumitha*, AI-Driven Pharmacovigilance: Leveraging Big Data for Improved Adverse Event Detection, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 6, 5765-5776. https://doi.org/10.5281/zenodo.15770998
 10.5281/zenodo.15770998
10.5281/zenodo.15770998
