Fabtech College of Pharmacy, Sangola, Solapur, Maharashtra -413307
Millions of people worldwide suffer from renal stones, a common urological condition that significantly increases morbidity and costs money. One promising method for managing kidney stones is homeopathy, a model encompassing alternative and supportive therapeutic systems By examining the effectiveness, safety, and possible mechanisms of action of homeopathy, this review seeks to critically assess the body of research on the subject. The Cochrane Library, PubMed, and Scopus were among the primary databases used in a thorough literature search. Included were studies that looked into the use of homeopathic medicines in the treatment of kidney stones and were published in English. Twenty-five studies, including case reports, observational studies, and clinical trials, were found through the search. According to the review, kidney stones have historically been treated with a number of homeopathic remedies, including Sarsaparilla, Lycopodium clavatum, and Berberis vulgaris.
The medical term urolithiasis originates from three Greek roots: “ouron,” which denotes urine “oros,” which denotes flow; and “lithos,” which means stone form.It refers to the formation of stones within the urinary tract, including the bladder, urethra, urinary ducts, or kidneys It is regarded as one of the key prevalent pertaining to urinary disorders conditions worldwide. According to epidemiological research, urolithiasis is influenced by a wide range of characteristics, including age, sex, industrialization, socioeconomic position, nutrition, and environment.[1]
Overview frequent urological condition medically identified as Nephrolithiasis is brought on by crystallization of minerals in the urinary tract, such as struvite, uric acid, or calcium oxalate.If left untreated, they frequently result in excruciating pain, blockage of the urine, and recurring episodes. Analgesics, surgical excision, and lithotripsy are examples of conventional therapeutic approaches; nevertheless, these may have adverse consequences and recurrence rates. By easing pain, facilitating stone ejection, and lowering the chance of recurrence, homeopathy, a holistic medical approach, has been investigated for its possible function in kidney stone therapy. Based on each patient's unique symptomatology, remedies like Sarsaparilla, Lycopodium clavatum, Berberis vulgaris, and Cantharis are commonly recommended. Research indicates that homeopathic remedies could provide safe, noninvasive, and customized methods for controlling and preventing renal calculi.[2]
The development of urinary calculi at any level of the urinary tract is known as nephrolithiasis or urolithiasis. Renal calculus is derived from the Latin words "renes," which means "kidneys," and "calculus," which means "pebble." It is necessary to distinguish between urolithiasis and nephrolithiasis because not all uroliths, originate in The development of nephrolithiasis at any level of the urinary tract is known as nephrolithiasis or urolithiasis. Renal calculus is derived from the Latin words "renes," which means "kidneys," and "calculus," which means "pebble." It is necessary to distinguish between urolithiasis and nephrolithiasis because not all or uroliths, originate in the kidney; some can form in the bladder. However, as the disease process and treatment are identical regardless of the distinction, the terms are frequently used informally as synonyms.[3]
WHAT ARE KIDNEY STONES
Renal stones, calculi of the renal system, or nephrolithiasis are crystalline masses composed of minerals that originate in the renal system. They develop as an outcome of crystallized brought due to a difference in the elements of the stool, including urea, calcium, magnesium, and ammonia. These stones, which block the circulation of urine, vary in shape from tiny grains to larger stones. Common indications include hemorrhage (blood found in the urine), nausea, urgency in the urine, and severe flank discomfort. If neglected, they may result in disease or harm to the kidneys. [4]
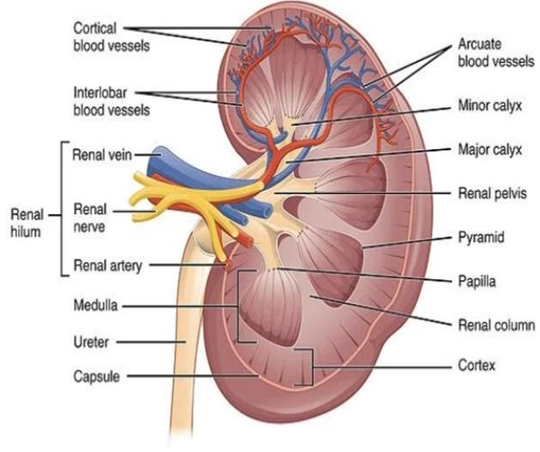
Fig1. Normal kidney.
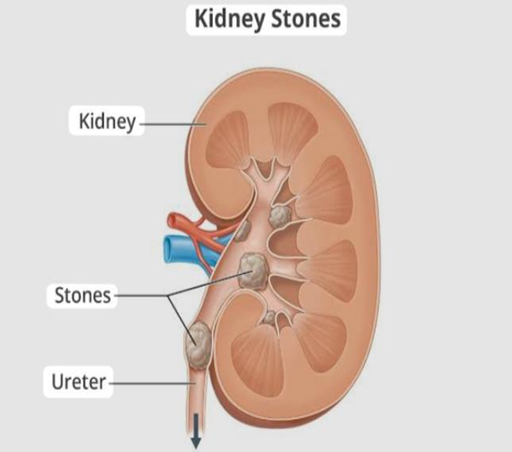
Fig 2.Kidney stone
PATHOPHYSIOLOGY OF KIDNEY STONE
Renal stones are created by two main processes and are made up salts that are insoluble in urine. crystal aggregation with a matrix of non-crystalline proteins of is first mechanism. During order to aggregate crystals cause enable them to develop into a into a bulk large enough as to produce clinical symptoms, the salts in the urine precipitate and crystallize.[5] Stone formation on a calcium phosphate nidus in the renal papillaries, typically Randall's plaque (which is always made of calcium phosphate), is second process, which is primarily in charge of calcium oxalate stones.[6]
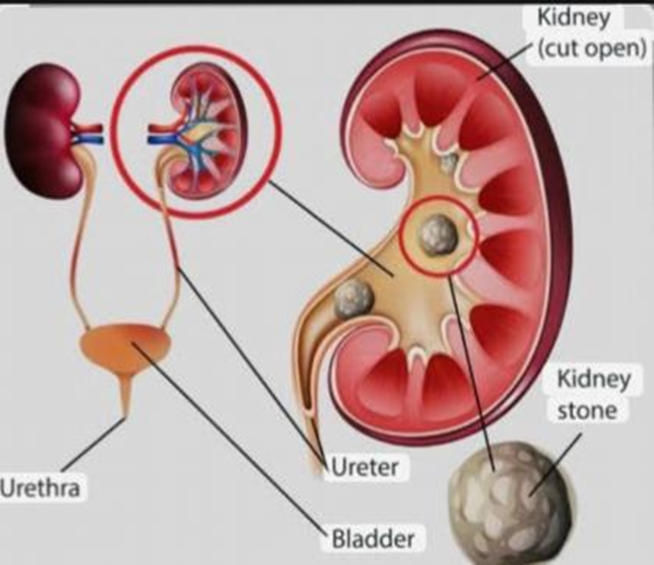
Fig 3. Pathophysiology of Renel stone
TYPES OF KIDNEY STONES
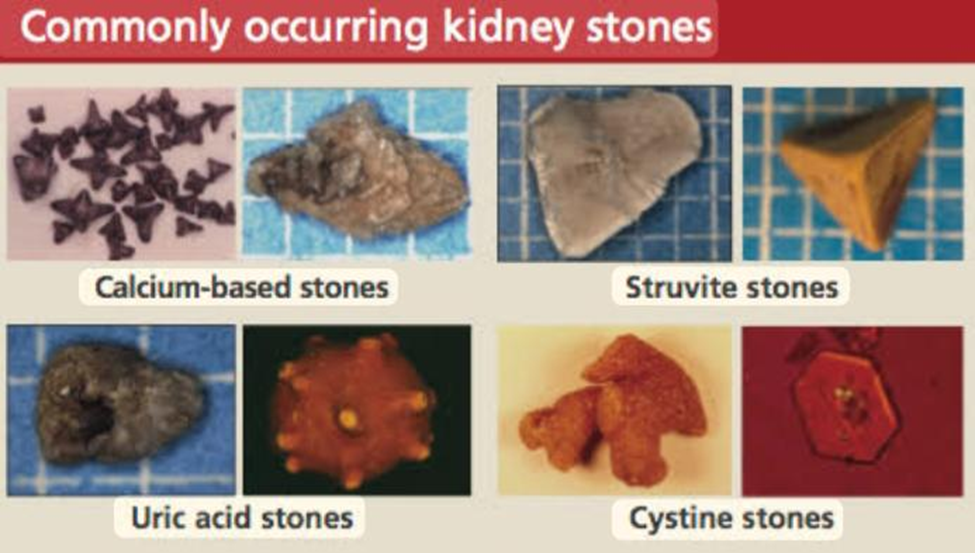
Fig 4.Different types of kidney stones
Calcium oxalate's super-saturation decreases when urine oxalate levels fall. The only method that has been found to lower endogenous oxalate production in case with the typical form of renel lithiasis is refraining from megadose of vitamin c supplementation. First, you should stay away from foods like spinach, rhubarb, and potatoes that have a lot of oxalates. People with exceeding than desirable urinary oxalate levels has to be advised to employ enough calcium because higher calcium intake decreases oxalate absorption. Natural inhibitors of calcium phosphate and calcium oxalate stones include citrate. Increased nutrient consumption high in pH regulating compound such as edible plant material ought to be promoted. Stones made of calcium phosphate The same is true with calcium phosphate stones.
Raising the pH of urine is the cornerstone of preventing the production of uric acid stones. While alkalinizing the urine can be easily accomplished by consuming more foods high in alkali (such fruits and vegetables) and fewer foods that create acid (like animal flesh), acidifying the urine can be difficult. To achieve the ideal pH range of 6–7 during the day and night.
A urologist must remove these stones completely. By preventing UTIs, new stone formation can be prevented.[7][8][9]
Cystineuria, a genetic disorder, is the cause of cystine stones. The amino acid cystine leaks from the kidneys into the urine as a result of this condition.[10]
HOMEOPATHIC MEDICINE
The term "barberry," which refers to Berberis vulgaris Linn. (F. Berberidaceae). A better treatment option for removing the kidney stone on the left side is B. vulgaris. Stones and other urinary tract conditions are among the anomalies of the urinary system for which B. vulgaris has been utilized in the homeopathic medical system. In kidney stone illness, berberine, an isoquinoline alkaloid, is the primary component with therapeutic benefits.[11]

Fig.5 Berberis vulgaris
Often referred to as cantharis, the toxic Spanish fly (Cantharis sp.) is outwardly equivalent. It includes a terpene called cantharidin, which is used in homeopathic treatment. This amazing homeopathic renal stone medication might help patients with kidney stones who experience scalding discomfort in the urethral tract. Nonetheless it is particularly effective when burning micturition is the defining symptom.[12]
Although only a few drops, frequently mixed with blood, are passed each time, there is a persistent urge to urinate. It happens before, during, and after urinating and is excruciating. The patient's renal region is plagued by severe episodes of searing and cutting pain. There is considerable strangury and tenesmus. Urine passes drop by drop and has a scorching effect. It may have membrane scales that resemble bran in water and have a shreddy or jelly-like appearance. Urinary tract hypersensitivity is noticeable throughout. Bladder pain is exacerbated even by consuming tiny amounts of wat[13]

Fig 6.Spanish fly
Lycopodiaceae is a family of lycopods, including Lycopodium, which is also known as moss creeping plants. These stems are upright, prostrate, branching, and flowerless. The leaves cover the stem like needles. With a geological history spanning more than 380 years, Among the ancient family’s essential homeopathic remedies is L. clavatum..[14]
The two main symptoms are severe back pain that is more pronounced In the afternoon and red sand in the urine. A common and effective medication is lycopodium, which has a deep-acting effect. L. clavatum controls protein metabolism, treats kidney stones and gout, and influences the total fat metabolism, which is a troubling one in humans. The symptoms listed in materia medica include a strong odor and urine with reddish-yellow sand. Lycodoline, lucidioline, alphaobscuring, are among the alkaloids found in L. clavatum. The Sarsaparilla plant, Smilax sp. It is the Sarsaparilla that climbs or trails. [15]

Fig 7. Lycpodium calvatum
Smilax sp., or sarsaparilla The genus Smilax includes the tropical American climbing or trailing plant known as sarsaparilla. The lily family member Sarsaparilla is commonly found in warm, marshy, and temperate regions. It has alternating leaves and umbels of flowers. Sarsaparilla is a right-sided medication according to homeopaths; it can also remove a left-sided stone and, depending on the symptoms, is just as successful in treating conventional treatment for cancer, joint pain, eczema, ulcers, and malignancies. Male rejuvenation, sarsaparilla possesses testosterogenic, and progesterogenic properties.[16]
Sarsaparilla is primarily composed of flavonoids, including ,motilin, phenolic compounds, including resveratrol and ferulic acid; and steroids, including diosgenin, sarasaponin, sarsasapogenin, sarasaparilla is a far better treatment. For the urine with a white deposit. At the end of urinating, there is intense discomfort. Additionally, after urinating, there is burning and an acidic taste in the urethra. A thin, ragged stream is overflowing with urine. Sarsaparilla roots contain saponins that are known to improve the body’s absorption of various medications.[17]

Fig 8.sarsaparilla root
Hairy rupturewort,is a bloom bearing plant that belongs to the Caryophyllaceae family. they are found in to North America and other terrestrial region. Phenolics, flavonoids, flavonols, and saponins were all present in H. labra. In rat models of nephrolithiasis, H. glabra is tested as a prophylactic treatment for kidney stones.The experimental investigation included both normal and Kidney stones due to calcium oxide rat.The findings showed that it increases the rats’ water intake and urine output. However, particularly during the third week of treatment, their urine pH dropped.[18]

Fig 9. Herniaria glabra
The Umbelliferae family includes the flowering plant Ammi visnaga. Visnaga, khella, toothpick-weed, and toothpick-plant are a some of the well-known names. It is a natural plant found in North Africa, Asia, and Europe. A. visnaga is frequently used to treat kidney stones and other illnesses. Khellin, visnagin, and visnadine, which are coumarin derivatives derived from A. visnaga seeds, are the active chemical ingredients and have anti-nephrolithiasis properties.[19]

Fig 10.visnaga(Ammi visnaga)
PROCESS OF KIDNEY STONE FORMATION
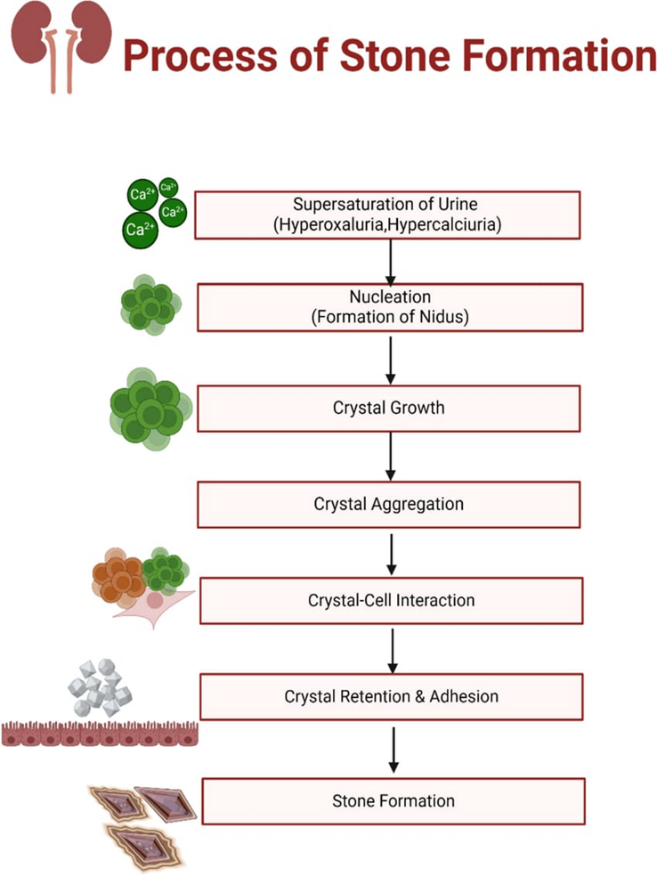
Fig 11.Process of kidney stone Formation
DIAGNOSIS
Diagnosis of nephrolithiasis made based on clinical findings, and confirmation is frequently sought by testing. The vitals of a patient could reveal information about the severity of their pain because tachycardia and hypertension would be present. The doctor should look for nephrolithiasis-specific symptoms throughout the examination. Many patients may have an uneventful examination, with the exception o any discomfort the patient expresses. Others might experience pain below the costovertebral angle. As previously stated, the clinical diagnosis derived from the patient's history and examination is the only basis for the testing. Any urinary problem may call for a basic urine dipstick test, regardless of whether patients report a change in urine color.
In situations of infection, nitrites would be positive, and microscopic haematuria is frequently detected. It would be helpful to have a complete blood count because infectious cases may exhibit fever. Since many patients have nausea and vomiting when they first arrive, it might represent important for examine levels of ions . That would also be beneficial determine which kind of stone is causing the issue .A blood creatinine test may be necessary for patients with a history of chronic illness or recurrent infections in order to assess renal function. When females appear with renal stones, they are particularly vulnerable to chronic kidney injury and, as previously indicated, would require ongoing renal function monitoring.[20]Imaging modalities such as Ultrasonography, pyelography, and nuclear imaging tomography are Ultrasonography, pyelography, and nuclear imaging tomography are employed diagnosis of nephrologic disease. Hydronephrosis, persistent blockage, and recurrent stones are among the consequences of renal stones that these imaging modalities are frequently more crucial to detect.[21]
Different diagnosis
This is dependent on where the pain is located and if pyrexia is present or not.
RISK FACTORS AND CLINICAL MANIFESTATIONS
Renal lithiasis is caused by a number of variables, such as metabolic problems, genetic susceptibility, dietary habits, dehydration, and certain drugs. The size and position of the stone affect the clinical appearance. Severe flank discomfort, frequency of urination, hematuria, dysuria, nausea, vomiting, and in extreme situations, fever and chills, are typical symptoms. [23][24]
TREATMENT AND PREVENTION OF KIDNEY STONES
Treatments for stone prevention that involve diet and medication should take patient preferences and recurrence risk into account. If dietary interventions are ineffective, medication may be used in addition to dietary modifications. A 24-hour urine analysis following the stone’s passage or removal can aid in directing preventive treatment. By increasing fluid consumption, it is possible to manage a smaller urine volume (less than 2 L) so the urine output surpasses two Litres in a twenty-four-hour period. Great salt consumption raises the amount of sodium in the urine (>100 mmol/24 h), which raises the amount of calcium in the urine (>250 mg/24 h). Therefore, a low-salt diet (1500–2000 mg/24 h) can be used to manage elevated urine calcium. A thiazide diuretic, such as chlorthalidone 25 mg daily, can also reduce elevated urine calcium. Reduce the amount of citrate in the urine (<300 mg/24 hours; a crystallization inhibitor) less than 6.5 for uricacid stones, or a lower urine pH Potassium citrate, such as twenty to thirty mEq twice daily, can be used to manage both. Although thiazide diuretics and potassium Citric acid has been shown in randomized studies to stop recurrent stones, it is unclear whether determining the composition of stones a 24-hour urine analysis to customize therapy is helpful. For that reason, routine testing of twenty-four-hour urine chemistries or stone composition is not advised by the American College of Physician.[25]
Fig 12. Treatment of kidney stone
The first line of treatment for preventing stone recurrence should be a greater fluid consumption sufficient generate at no fewer than 2.5 L of pee daily.
According to the type of stone and the findings of metabolic examination, different prevention strategies are recommended. Following treatment, subsequent reasons of stone development. The treatment of recurring stones caused by hypercalciuria heavily relies on dietary changes. Since calcium decreases intestinal uptake of oxalate, it lowers excretion of oxalate into the urine, hence dietary calcium intake shouldn’t be limited. AUA guidelines suggest consuming 1,000–1,200 mg of calcium each day. Furthermore, limiting dietary calcium intake to less than 800 mg per day the daily allowance that is currently advised for adults Could result in bone loss and a negative calcium balance. Hypercalciuria is also influenced by sodium consumption. Because active reabsorption of sodium creates a concentration gradient, calcium is passively reabsorbed in the proximal tubule. Volume expansion brought on by a high sodium intake increases calcium excretion while decreasing proximal sodium and calcium reabsorption.[26]
CONCLUSION
As this review has shown, homeopathy can be used to cure kidney stones, alleviate symptoms, and enhance quality of life. According to the research, homeopathic remedies including Berberis vulgaris, Lycopodium clavatum, sarasaparilla, cantharis, hairy rupturewort visnaga can aid in the dissolution of stones, the reduction of inflammation, and the promotion of healing. The homeopathy can be helpful in treating this illness. A holistic approach to treatment is provided by homeopathy, which considers a person's mental, emotional, and physical well-being.
To sum up, homeopathy is a safe and efficient way to treat kidney stones. It can be combined with traditional therapies to offer complete care. Although further research is required to completely comprehend the effects of homeopathy in the management of renal stones, the evidence that is already available indicates that it is a worthwhile therapy option that merits more attention.
REFERENCE


Punam Vagare, Dr. Sanjay Bais, A Review on Significance of Homeopathic Medicine in Kidney Stone, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 4216-4225. https://doi.org/10.5281/zenodo.17724747
 10.5281/zenodo.17724747
10.5281/zenodo.17724747
