Raosaheb Patil Danve College of Pharmacy Badnapur, Jalna.
Pharmacovigilance is the science of finding, checking, understanding, and preventing side effects or other problems caused by medicines. It is closely connected to proper information management. Information plays a very important role in pharmacovigilance, as it helps in collecting, studying, and sharing data to keep patients safe. The base of pharmacovigilance is a strong information system that gathers reports of side effects from doctors, patients, and other healthcare workers. Over time, new sources of data such as electronic health records, wearable devices, and real-world evidence have made it possible to collect more detailed and useful information for analysis. Modern technologies like artificial intelligence (AI) and machine learning (ML) are now changing pharmacovigilance. These tools can automatically detect safety signals, study large amounts of data, predict risks, and help in making regulatory decisions. Another important part of pharmacovigilance is proper information sharing between regulatory authorities, pharmaceutical companies, and healthcare providers. Sharing safety information quickly and clearly helps to respond to new risks and to create good safety management plans.
The historical development of word “ pharmacovigilance” includes the Greek word pharmanacon= drug or medicinal substance and the Latin word Vigilare = ‘to keep watch.1
Absolutely, pharmacovigilance is indeed a critical aspect of the entire drug development process. It involves the constant monitoring, assessment, and understanding of potential adverse effects or any issues related to medications. This helps ensure patient safety by evaluating this risks and benefits associated with specific drugs .With the aid of information technology.2
Pharmacovigilance has significantly improved, allowing for more efficient monitoring and enhancing clinical safety practices. It’s apivotal part of ensuring the safety, efficacy and cost-effectiveness of medications throughout their lifecycle from discovery to post-marketing surveillance.3
According to WHO Pharmacovigilance is a set of practices aiming at the identification, understanding and assessment of the risks associated with drugs . It starts from the pre-marketing phase of a new drug and continues beyond the post-marketing phase covering the entire life cycle of the product .4
There are a bunch of examples of drugs, which have been detached from the market owing to reported adverse effects. Rosiglitazone holds the first position in the market; other well-known drugs, including terfenadine, cisapride, phenylpropanolamine, rofecoxib, cerivastatin, Gatifloxacin, cisapride were withdrawn because of their adverse reactions.5
It has been observed that an adverse reaction is the major cause of hospitalization and drug withdrawals proves expensive for the patients as well for the manufacturing companies. Though a new drug molecule has to undergo various clinical and non-clinical trials yet the need of Pharmacovigilace becomes mandatory; as the information generated from the clinical trial is not sufficient to evaluate the safety of the drug with regard to adverse drug reactions for its being limited to a few number of patients and the conditions for the use of medicines differ from that in clinical practice and for regular use by the patients.6
The main objective of Pharmacovigilance post market surveillance is to regulate and ensure the safety & efficacy after the entry of the new drug molecule into the market for the treatment of diseases of the general population with different medical conditions.7
Recently the concern of Pharmacovigilance has been widened to include herbals, medicines, blood products, biological products, medical devices and vaccines.8
Every medication has potential adverse/side-effects. Also many medications have potential interaction with other substances. When a new drug is prescribed, there is an exponential increase of interaction. So, to prevent these types of adverse effects, there is also a need of skilled health care practitioners & other health care members who can select & prescribe the best & safest medicines according to the medical needs of the patients.9
Thus pharmacovigilance program includes public awareness and education of patients and health care professional in reporting the adverse drug reactions so as to ensure better health care worldwide. This article covers various terms associated with Pharmacovigilance & adverse drug reactions as discussed in Table1 and puts special emphasis on the effects of ADRs on market share due to withdrawals of blockbuster molecules which lead to tremendous loss to the pharmaceutical industry. The article also highlights the various types of ADRs & consequences of reporting and non-reporting of adverse drug reactions with due examples of reported ADRs & their recalls. The article also emphasises on the pharmacovigilance program in European Union, United States and India, strategies for reducing the ADRs and future aspect of pharmacovigilance programs.10
Drugs are essential for the treatment of various diseases, but there are drug-related problems, such as adverse drug reactions (ADR) 11. Post-marketing information on medicines reports a benefit-risk balance obtained from clinical studies. Never the less, drug surveillance is necessary to evaluate safety in real-life and long-term conditions 12. .
For this reason, ADR voluntary reports are needed, thus spontaneous reporting is the pillar of pharmacovigilance. In countries with pharmacovigilance programs well-established, there port number is about 200 or more per million in habitant13 .
However, in many countries, pharmacovigilance programs are still under development, and this fact may result in a low drug safety culture that translates into under reporting of ADR. Low notification rates make it difficult to detect signs in the general population that, limits evaluation of ADR causality and the issuance of health alerts. Under reporting can be explained by the low participation of health professionals due to a lack of knowledge and negative attitudes toward pharmacovigilance, such as ignorance (only important serious ADR reports) or lethargy (disinterest in reporting) 13–15
Different strategies have been evaluated to increase ADR notification, such as the implementation of educational interventions for health professionals16–18.
Purpose is to raise awareness about drug safety issues to improve ADR reporting to obtain statistical assessments by detecting signs and issuing health alerts 19-20. Therefore, the aim of this systematic review with meta-analyses was to synthesize the evidence of EI efficacy in health professionals to increase ADR reporting, attitudes, and knowledge of pharmacovigilance.
METHODS:-
A systematic review and meta-analyses were conducted according to the PRISMA statement 21 and the protocol was prospectively registered in PROSPERO with registration number CRD42021254270.
Search strategy:-
A systematic literature search was carried out in the following electronic databases: PubMed, LILACS, Cochrane Central Register of Controlled Trials (CENTRAL), Scopus and episteme onions. Unpublished literature, Looked up in the abstracts of randomized controlled trials (RCTs) indexed in Scopus Conference Papers and Science Direct. Searches were conducted from inception until January 2022 and were not limited by years or language. The strategy search was constructed using the following Me SH terms and keywords:“ health personnel”, “physicians”, “pharmacists”, “nurses” ;“models educational”, “education medical”; “adverse drug reaction reporting systems”, “pharmacovigilance”, “adverse drug reaction reporting”. The search strategy was adapted to each data base. In addition, all references identified by systematic reviews were analyzed to identify potentially relevant studies.
Study selection:-
Studies were included if they met the following criteria:1 RCT, including multi-arm trials;2 participants were health professionals (physicians, consultants, nurses, pharmacists, and dentists);3 participants received an educational inter vention in pharmacovigilance including telephone-based interventions, workshop, educational material, electronic supplementary material, letters, lectures, sessions group, email and combined intervention; in the control group, part icipantsdid not receive educational activity or received training from their pharmacovigilance unit; 4
Study results were a number of ADR reports and knowledge and attitude mean scores obtained through a questionnaire, in both groups. Studies were excluded if the educational intervention was aimed at patients or if the comparison was made between health professionals and patients, as well as studies that were sponsored by the pharmaceutical industry or involved economic incentives. Two independent reviewers (MJC and LMU) assessed all titles and abstracts to identify studies via the inclusion criteria and excluded non-relevant studies. All potentially relevant articles were retrieved and read in full text. Reviewers were blinded to each other’s decisions. Discrepancies were discussed and resolved with a third reviewer (ODC). The inter-rater reliability was evaluated using kappa coefficient.
Data extraction and risk of bias assessment:-
Selected studies were reviewed independently by two reviewers (MJC and LMU) to extract in an Excel data base the following data: publication year, author, health professionals, I, time of intervention, control group, the sample size of the intervention group as the control group, participants in both groups, follow-up time, the number of ADR reports, knowledge, and attitude in pharmacovigilance mean score, country, attitude, and knowledge questionnaire (validated or not), change of result over time, ADR type (severe, unexpected, high-causality and new-drugs). Discrepancies in data extraction were resolved by consensus. In case any data was not reported in the article, the authors were contacted to obtain it.
Drug Interactions, Pharmacokinetics and Polypharmacy:-
Modern cancer therapy is based on complex treatments involving combinations of chemotherapeutic agents, biologic agents, endocrine agents, growth factors, and targeted therapies. Furthermore, caregivers often add palliative and analgesic therapies, antiemetics and non-pharmaceutical complementary and alternative medicines to help manage ADRs. These complex combinations may increase the number of interactions among drugs or between drugs and other products, including natural ones. These pharmacodynamic and pharmacokinetic interactions can be dangerous to patients and may reduce the benefits of therapy. In addition, since anticancer treatments are increasingly personalized, molecularly targeted therapies (i.e. those that act on specific molecules expressed by particular types of cancer) can have a variety of individual pharmacokinetic responses, which may exacerbate the problem of drug–drug interactions. There may be, for example, genetic variability (polymorphisms) that alters drug transporters or enzymes
That metabolize drugs leading to differences in toxicity and efficacy among individuals 28.The situation of a patient taking multiple medicines concomitantly is called polypharmacy. In general medicine,
Poly pharmacy is defined as a series of medications that have likely been prescribed inappropriately 29. Hence, in general medicine, poly pharmacy is often correctable 30.
In oncology, in contrast, regimens of antitumor combinations are indicated by guidelines and international consensus and have a strong rationale, which is to attack the two more with multiple, synergic strategies, while at the same time, to support the body with ancillary therapies. Therefore, in clinical practice, the critical nature of poly pharmacy must be referred to the type of setting 31
Impacts on Practice :-
Pharmacovigilance studies are essential in oncology, because the under-reporting phenomenon is especially relevant in this field. In particular, physicians often underestimate the adverse reactions caused by oncological drugs, because they consider them common and they rather focus on efficacy of the drugs.
Pro-active pharmacovigilance is important to improve spontaneous reporting that can generate new signals on adverse drug reactions (ADRs). These signals can lead the Competent Authority to make a decision on each single drug (alerts, recommends…). Real life conditions are needed to detect the real incidence of the ADRs; Individual patient monitoring improves their compliance, because patients receive more information and they are directly involved in treatment.
Activities Therefore, pharmacists have a vital role in pharmacovigilance activities to ensure safety in drug use. A study by showed that pharmacy students had adequate knowledge about pharmacovigilance and a positive perception of ADR reporting. Related in Indonesia found that most respondents had good knowledge and attitudes about pharmacovigilance.
Several studies regarding the level of knowledge and perceptions related to pharmacovigilance have been conducted in several countries However, no recent similar studies have been found in Indonesia, especially in Yogyakarta. This study aims to describe the level of knowledge, 10 % hospital admission in some countries. To triumph over this issue, national pharmacovigilance systems have been established in many countries around the world. ADR reporting is the cornerstone of pharmacovigilance system considered globally. Pharmacists occupy a fundamental position in drug safety by contributing to the prevention, identification, documentation and reporting of ADRs. Studies have shown that pharmacist can play a significant role in the reporting system . Our study showed similar results that 58.9% considered pharmacist to be the most competent healthcare professional to report ADRs. The present study revealed that 98.37% of the pharmacy students have the knowledge of ADRs, 96.05% knows the different types of ADRS. It reflects the sound knowledge and understanding of prospective pharmacist regarding ADRs. 89.79% of the students understand the role of pharmaceutical company and ministry of health in ADR reporting. Only 44.77% of the respondents have information about the availability DRAP form for reporting of ADR. Majority of the students 88.63% agreed that the ADR reporting system in Pakistan needs further improvement. This evidently highlights that the prospective pharmacist realized the necessity for the enhanced awareness as well as implementation of the rules and regulation to improve the quality of life of Pakistani population. There is great need of time that pharmaceutical companies, regulatory bodies and ministry of health of Pakistan strive together for the betterment of society by maintaining safety profiles of the drugs.
The knowledge and perception of pharmacists pertaining to pharmacovigilance had major impact on the practice of pharmacovigilance. So if pharmacists are trained, there would be a positive drive towards increase in reporting and thereby would help in maintaining the safety profiles of drugs. Approximately 74% of the students have the confidence to discuss ADR with their colleagues.52.66% and 49.88% of the pharmacy students know where to report and how to report ADRs respectively. Underreporting of ADRs is a widespread observable fact in spontaneous post marketing surveillance programs. Underreporting may be impediment in signal detection and cause underestimation of the size of a problem. Correcting the underreporting scenario is complex as the extent is unidentified and inconsistent. It is an alarming condition that 54.98% of the pharmacy students find it difficult to decide whether an ADR has occurred or not. In another study , 32.3% and 36.4% respectively agreed that level of clinical knowledge makes it difficult to decide whether or not an adverse drug reaction has occurred.
Our study indicates the higher percentage of deciding about the ADR occurrence as compared to studies conducted in other countries. Major obstacles to reporting also include reluctance to report reactions about which a degree of uncertainty exists. Education and training have a significant influence on ADR reporting and should be continued and re-enforced in order to improve ADR reporting by pharmacists.
The perception of pharmacy students towards ADR and pharmacovigilance ideates study’s eagerness to e?ha??e their a?areness about pharmacovigilance and ADR reporting. Only 34.33 % agreed that pharmacovigilance is well covered in my pharmacy curriculum and 70.53% of the participants emphasized that pharmacovigilance should be included as a core topic in pharmacy education. Research has shown that pharmacists who receive more education and training on ADR reporting are More likely to report ADRs. The prospective Pharmacist signifies the extensive incorporation of Pharmacovigilance and ADR in the clinical pharmacology and therapeutics curricula of medical schools .66.82% respondents agreed that they can report adverse drug reactions during their clerkship. More than 50% of the participants considered themselves well prepared to report any adverse drug reporting in their future practice. About 86.54% of the prospective pharmacists considered that ADR reporting should be made compulsory for the pharmacist. The results are far better than the study conducted in India.
To the best of our knowledge, this is the first study that evaluates the knowledge and perception of pharmacy students toward pharmacovigilance and ADRs reporting in Pakistan. The present study revealed a positive attitude and perception of pharmacy students towards ADR reporting and pharmacovigilance. The students realize the importance of pharmacist being health care professional to report ADR which is a good.
Indication for providing pharmaceutical care as it is revealed that the effective participation of the pharmacy students has led to increase in number of ADR-reporting. Several studies have shown that Adverse drug reaction reporting can be improved by providing appropriate education, spending Further time with patients, creating more knowledge informing how to report adverse drug reactions to senior pharmacy students, making reporting System simple, and acknowledging the receipt of the report and participation of the pharmacists in ward rounds. International Journal of Pharmacy Teaching & Practices.
Data extraction and risk of bias assessment:-
Selected studies were reviewed independently by two reviewers (MJC and LMU) to extract in an Excel data base the following data: publication year, author, health professionals, EI, time of intervention, control group, the sample size of the intervention group as the control group, participants in both groups, follow-up time, the number of ADR reports, knowledge, and attitude in pharmacovigilance mean score, country, attitude, and knowledge questionnaire (validated or not), change of result over time, ADR type (severe, unexpected, high-causality and new-drugs). Discrepancies in data extractions were resolved by consensus. In case any data was not reported in the article, the authors were contacted to obtain it.
Drug Interactions, Pharmacogenetics and Polypharmacy:-
Modern cancer therapy is based on complex treatments involving combinations of chemotherapeutic agents, biologic agents, endocrine agents, growth factors, and targeted therapies. Furthermore, caregivers often add palliative and analgesic therapies, antiemetic’s and non-pharmaceutical complementary and alternative medicines to help manage ADRs. These complex combinations may increase the number of interactions among drugs or between drugs and other products, including natural ones. These pharmacodynamic and pharmacokinetic interactions can be dangerous to patients and may reduce the benefits of therapy. In addition, since anticancer treatments are increasingly personalized, molecularly targeted therapies (i.e. those that act on specific molecules expressed by particular types of cancer) can have a variety of individual pharmacogenetic responses, which may exacerbate the problem of drug–drug interactions. There may be, for example, genetic variability (polymorphisms) that alters drug transporters or enzymes.
That metabolize drugs leading to differences in toxicity and efficacy among individuals 28.The situation of a patient taking multiple medicines concomitantly is called polypharmacy. In general medicine, polypharmacy is defined as a series of medications that have likely been prescribed inappropriately 29. Hence, in general medicine, poly pharmacy is often correctable 30.
In oncology, in contrast, regimens of anti tumoral combinations are indicated by guidelines and international consensus and have a strong rationale, which is to attack the tumor with multiple, synergic strategies, while at the same time, to support the body with ancillary therapies. Therefore, in clinical practice, the critical nature of polypharmacy must be referred to the type of setting 31.
Data analysis:
Statistical analyses were performed using RevMan 5.4 14. ADR reports were pooled using an odds’ ratio (OR) with 95% confidence intervals (95%CI). Knowledge and attitude in pharmacovigilance scores were analysed with a standardized mean difference (SMD) with 95%CI. All analyses were performed with a random-effects approach. I² test was used to assess the heterogeneity of each evaluate results, and I² > 50% was considered with signification heterogeneity 15 Sub analysis by type of educational intervention was performed to identify the most effective intervention, as well as to explore.
Results:-
Characteristics of the studies:-
In the systematic search, a total of 875 citations were identified in databases, and the study selection process is illustrated in Fig. 1. After duplicate removal, 705 articles were screened by title and abstract for potential eligibility. In addition, 29 unpublished records were identified. No additional studies were identified in references of previously published systematic reviews. After screening, twenty-four studies.
Were assessed for eligibility, and 13 studies were excluded 16–28. Non-comparative studies were the main cause of exclusion, and all reasons are shown in the Suppl. 3. Interrater agreement was suitable (kappa=0.83). Eleven studies fulfilled the inclusion criteria of the systematic review, and the characteristics of the included studies are summarized in Table 1. Two authors were contacted for data to be included in the meta-analyses 29, 30, only one responded, however the information could not be pooled. Eight studies were included in the meta-analysis 29, 31–. For country, RCTs were principally conducted in Portugal (four articles) and Sweden (two articles). Geographically, all the studies were conducted in Europe and Asia. The EI varied from one day to nine months, and follow-up ranged from 0 to 20 months. The average participation rate (a healthcare professional who agreed to participate into the study) varies in each study between 7.9 and 84.0%, and participants had more adherences to combined interventions and electronic ADR information. Four studies involved physicians 29, 31, 33, 35, two involved nurses 29, 35, four involved pharmacists 32, 33, 34, 35 and two studies evaluated primary healthcare units that included physicians and nurses 30, 31. The professionals mainly studied were physicians (six studies with 5097 participants and 136 primary healthcare units), followed by the pharmacist (four studies with 887 participants) Workshops were the most common educative interventions used into studies 31, 33, 34, followed by intervention combined (session group and educative material) 29, 32, 35, telephone-based interventions31,34 . lecture31 educational material (transparencies, brochures, and posters) 30, electronic information sheet of ADR 32, E-mail interventions 39 and one-page ADR information letter 30. Three studies included continuing education by the pharmacovigilance unit as a control group 32, 35, , while eight studies did nothing 29–30, 31, 32, 33
ADR reports:-
Ten studies informed the number of ADR reports 29–32, 32–33. Five studies were excluded from the meta-analysis because these have incomplete data such as number of participants, or the total number of ADR reports 29-30. Five studies present complete data for meta-analysis, and classified ADR as total, serious, high probability, unexpected, and new drugs by control and intervention groups 31–35
Two studies presented three arms (workshop, telephone-based interventions, and control group) 31-34 and three studies with two arms (combined intervention or workshop vs. control group) 32, 33, 35. Educational interventions increased the reporting of all ADRs in comparison with control group (OR=4.74, [95%CI, 2.46 to 9.12], I 2=93%, 5 studies). In the sensitivity. Analysis, after removed31 educational interventions showed consistency in increasing ADR reporting In subgroup analysis, workshops increased ADR reporting, more than combined interventions while telephone-based interventions no showed a difference (Figs. 2). ADR reporting change over time is shown in In the workshop intervention, the increase in the number of reports was significant up to 16 months after IE for total and severe ADRs, but only increased over 12 months for unexpected, high-causality, and new drug ADRs. In contrast, telephone-based interventions only increased the number of total reports and serious ADRs by 4 months. Interestingly, the combined interventions increased the number of unexpected and new drug ADRs for at least 12 months, although for total, serious, and high-causality ADRs, the effect was seen from 12 months onwards.
Knowledge, and Attitude in Pharmacovigilance:-
Regarding the change in knowledge in pharmacovigilance, three studies evaluated 4 educative interventions. The meta-analysis results showed a tendency to increase pharmacovigilance knowledge mean scores in participants whreceived EI in comparison with the con . After removing the highest risk of bias study part in cipits in EI group shown an augmented the pharmacovigilance knowledge to . In sub group analysis the participants who received lecture and workshop increased their knowledge; this effect was not observed in those who received the combined intervention or letter with ADR information Two studies evaluated ADR reporting attitudes among health professionals however, the measurement scales obtained by the questionnaire are different, so it was not possible to perform a meta-analysis. One study conducted in pharmacist showed a positive attitude toward ADR Reporting after the intervention. Likewise, a positive effect in behaviour related to reporting was observed in physicians and nurses after educative intervention.
Risk of Bias Assessment:-
In risk of bias assessment (Fig. 4), 73% of studies had adequate random sequence generation 29-32–33 Only 54% describe the randomization process completely 29-30,-35 presenting low-risk allocation concealment, because the randomization was carried out by a person outside the study, or they avoided contamination between groups by randomizing health centers. The performance bias had a high risk in at least 81% of articles, due to differences in interventions ranging from a phone call to a combined intervention 29–35, With respect to blinding outcome assessment, in 4 studies the ADR reports evaluator was blinding 32–35. In 63% of the studies 30–34 no missing data were seen, while reporting bias was considered a low risk in 72% of studies 30–35 Additionally, in other potential sources of bias, 80% (9 of 11 studies) of the selected studies were rated with a low risk of bias 29–34 .
Discussion:-
ADR report is paramount for causality analysis and drug safety assessment. Nonetheless, ADR occurrence generates distrust in health professionals due to the fear of being judged and punished40. To avoid this, EIs in pharmacovigilance are intended to increase knowledge about drug safety, improve attitudes towards ADRs, and consequently increase the reporting. The results of this systematic review with meta-analysis showed that EI in pharmacovigilance increases the ADR reports, and present positive changes in pharmacovigilance knowledge and attitude in health care professionals. To synthesize the best available evidence on the role of EI in increasing ADR reporting, only RCTs were included in this systematic review. Study results show that EI increases by about four times the ADR report. Similar results were reported in a systematic review that synthesized the evidence on interventions to increase the spontaneous reporting of ADRs in healthcare professionals and patients 8. Likewise, two previous systematic reviews, which included pre-post experimental design, quasi-experimental and RCT studies, concluded that the interventions evaluated were considered effective 6-8 However, no previous systematic review has evaluated efficacy by intervention type. In this study, the workshops have greater ADR reporting efficacy compared to others that could be explained by the person-person interaction of the workshop allows a better understanding of the concept compared to reading information in a letter. In this sense, the score of knowledge observed in workshop participants is two-fold increase in comparison with participants who received a letter with ADR information. Previous results indicated that interactive sessions enhance participant activity and provide the opportunity to practice skills can effect change in professional practice In addition, the effectiveness over time reveals that EI with interaction between people such as workshops .
Limitation of study:-
This systematic review has the following limitations, which should be considered when interpreting the results:
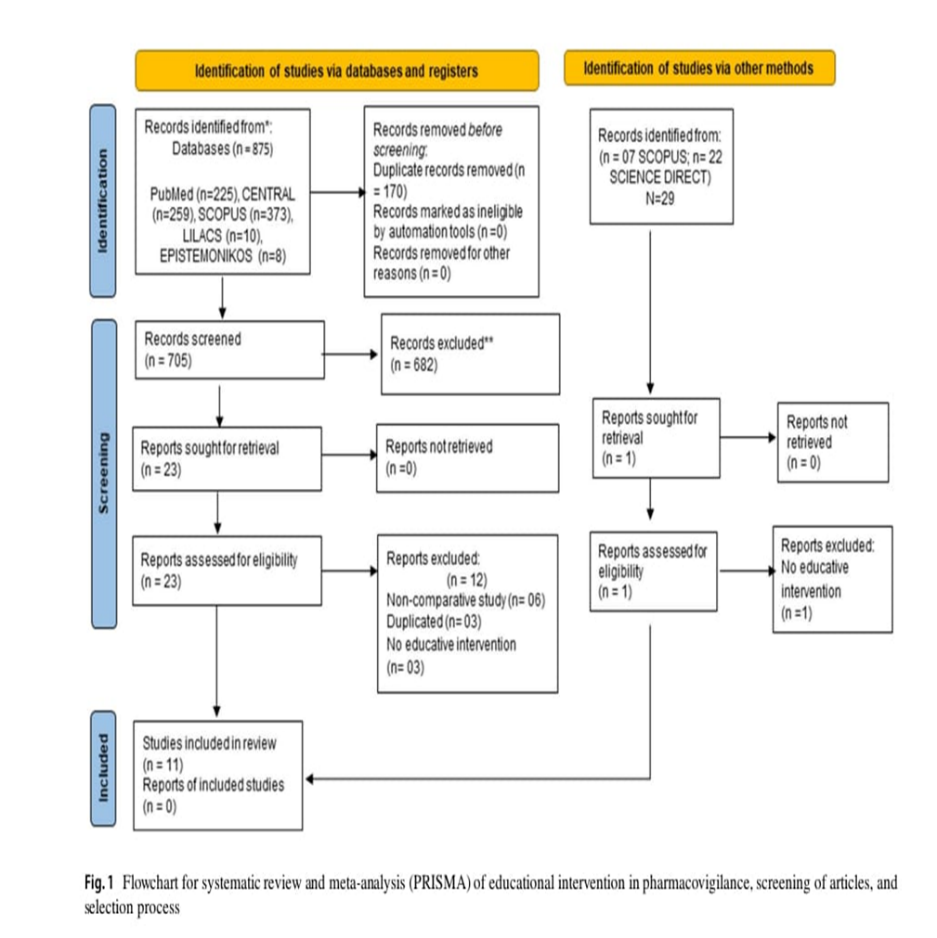
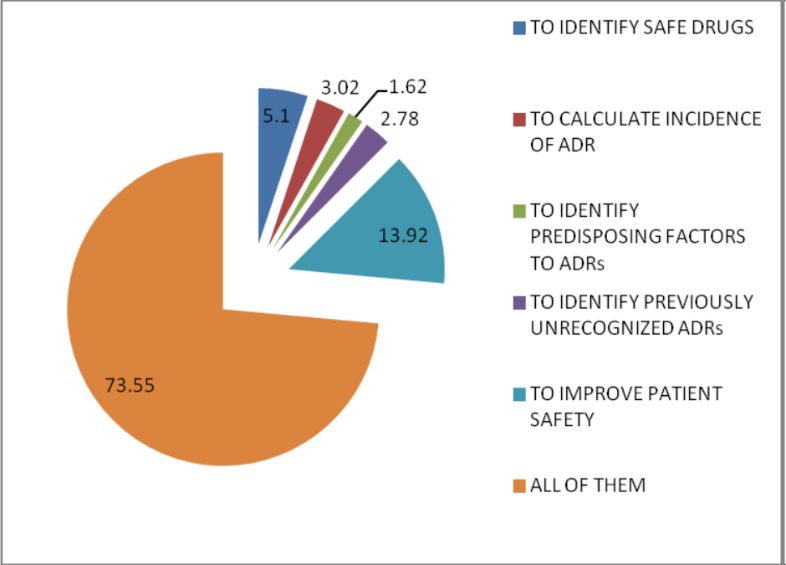
Fig 2 . Purpose of reporting ADR from students’ point of view.
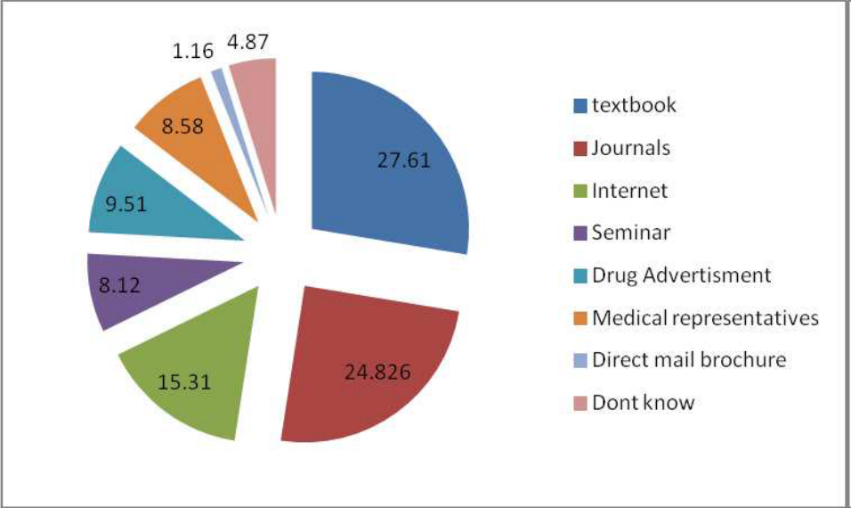
Fig .3 Most reliale soure of ADR fro studets’point of view.
MATERIALS AND METHODS
Calabria Biologics Pharmacovigilance Program :-
The Calabria Biologics Pharmacovigilance Program (CBPP) is a multi Center pharmacovigilance study aimed at improving the continuous monitoring of safety of bombards treatment in clinical practice. The purpose of the program is to implement a simple active AEs reporting system in all tertiary rheumatology clinics dealing with bDMARDs distributed across Calabria Region (Italy) indifferent fields of medicine including rheumatology, gastroenterology and dermatology. Since its starting in 2016, the program develops through regular
Training sessions for physicians during dedicated one-day pharmacovigilance courses (at least two courses/year) in order to improve awareness/compliance and therefore boost the reporting (stimulated reporting) attitude during scheduled follow-up visits. The physician dealing with an AE is provided with a direct interface with the Clinical Pharmacology and Pharmacovigilance Unit at University of Catanzaro “Magna Graecia” by either email, program website and dedicated phone number.
Structured data are collected for each AE, including Medical Dictionary for Regulatory Activities (MedDRA) classification of the event, duration, severity and outcome. Furthermore, during the whole follow-up period, patients received periodical phone calls by a clinical pharmacologist (approximately one every three months) aimed at identifying new events, stimulating self-awareness and encouraging reporting to the physician during the subsequent follow-up visit for minor AEs. The global costs associated with the program for the rheumatology therapeutic area are related to the recruiting of one dedicated clinical pharmacologist (EUR 28.000/year) and the expenses for the organization of training courses and meetings (approximately EUR 10.000/year).
The study protocol was approved by the local Ethics Committee (ComitatoEtico Regionale Calabria, Italy), protocol number 278/2015. Informed consent was obtained from all patients at the time of enrolment which were informed that medical records will be anonymously utilized for this study. All procedures were performed in accordance with the 1964 Declaration of Helsinki and its later amendments.
Patients:-
In this preliminary report, we provide the data obtained during the first two years of the CBPP Rheumatology therapeutic area. To this purpose, all consecutive patients undergoing Pharmacovigilance program for biologics used in rheumatology in Calabria Region, Italy 3 / 12treatment with one bDMARD at eight rheumatology centers (Rheumatology Outpatient Clinic, Azienda Ospedaliera “Pugliese-Ciaccio”, Catanzaro, Italy; Rheumatology Unit, Grande Ospedale Metropolitano “Bianchi-Melacrino-Morelli”, Reggio Calabria, Italy; Rheumatology Outpatient Clinic, Azienda Ospedaliera “Mater Domini”, Catanzaro, Italy; Rheumatology Outpatient Clinic, Azienda Ospedaliera Provinciale Crotone, Crotone, Italy; Rheumatology Unit, Azienda Ospedaliera “SS Annunziata”, Cosenza, Italy; Rheumatology Outpatient Clinic Azienda Ospedaliera Cosenza, Cosenza Italy; Rheumatology Unit, Ospedale Castrovillari, Castrovillari, Italy; Rheumatology Outpatient Clinic, Azienda Sanitaria Provinciale Vibo Valentia, Vibo Valentia, Italy) between January 1, 2016 and December 31, 2017 and satisfying predefined criteria were included. These centres account for > 90% of total bDMARDs prescription for the rheumatology area in Calabria Region.
Patients were included in the protocol if met all the following inclusion criteria:
The date of the first bDMARD prescription during the study period represented the “index date” for each individual patient. From the index date onward, the patient was started on a hybrid reporting system, characterized by “stimulated” reporting of AEs by the managing physician during each outpatient visit and intermediate phone calls to the patients by a clinical pharmacologist as described above.
For each patient, the following information were collected: demographic andclinical characteristics including age, sex, diagnosis (RA, PsA or AS), disease duration, current or prior use of ant rheumatic medications includingcsDMARDs, corticosteroids and bDMARDs, comorbidities, discontinuation or switch/swap to another molecule with reason, and adverse events. Patients were considered to have discontinued treatment if they did not take that specific agent after the recommended dosing interval had passed, regardless of whether they subsequently switched to another biological agent; conversely, patients were defined “persistent” if they were still on treatment with the same drug during the last 3 months of the follow-up period. The reasons for treatment discontinuation were classified as inefficacy or AEs. Furthermore, patients were classified as switchers if they were initiatedon treatment with a bDMARD other than the one reported on the indexdate during the study follow-up period.
Furthermore, AEs were collected through active reporting and phone calls. Foreach AE, the investigator (clinician or pharmacologist) recorded a detailed description of the detected AE, including the onset date, severity, time-course, duration and outcome. All AEs were coded according to the MedDRA dictionary version 20.0. SAEs were defined as events that were fatal or life threatening and resulted in a persistent or major disability or incapacity ,required prolonged inpatient hospitalization, or led to a congenital anomaly or birth defect. For comparison, the number of AEs spontaneously reported for the same molecules in the same centers before starting the protocol (January 1, 2014 to December 31, 2015) were used.
Statistical analysis:-
Demographic and baseline characteristics were summarized using descriptive statistics. Continuous data are presented as mean ± standard deviation (SD) or median (25–75 percentile) as appropriate, while ordinal data are expressed as number (percentage). The Fisher’s exact test for qualitative variables was used to compare the number of ADRs before and after implementing.
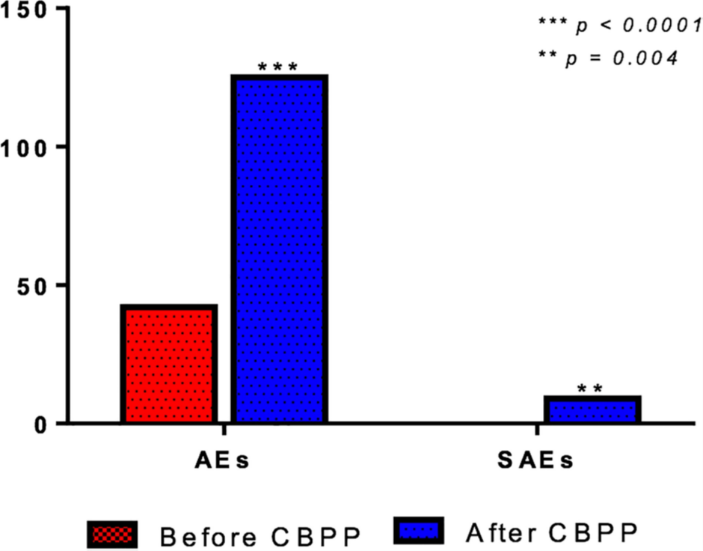
Fig 4. Prevalence of adverse events (AEs) and serious adverse events (SAEs) before and after CBPP protocol implementation.
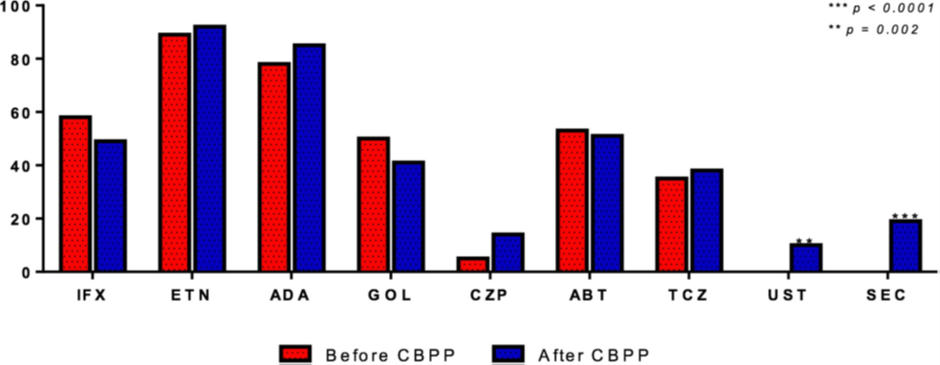
Fig 5. Prevalence of adverse events (AEs) before and after CBPP protocol implementation for individual bDMARDs.
Advantages of Pharmacovigilance
Ensures Patient Safety
Improves Drug Quality & Efficacy
Supports Regulatory Decisions
Enhances Rational Use of Medicines
Early Detection of Drug Interactions
Helps in Post-Marketing Surveillance
Builds Public Trust
Reduces Healthcare Costs
Disadvantages of Pharmacovigilance
Underreporting of ADRs
Requires High Cost & Resources
Delayed Reporting
Data Quality Issues
Lack of Trained Personnel
Difficulty in Establishing Causality
Need of Study:-
Aim and Objective:-
Aim :- To study and analyse adverse drug reactions through pharmacovigilance and to evaluate the role of clinical pharmacy and medication therapy management in improving patient safety and effective use of medicines.
Objective:-
CONCLUSION:-
Pharmacovigilance is the only way to insure the safety of the medicine throughout the life cycle. It's veritably important pivotal as the clinical trials have limitation to descry the rare and veritably rare ADRs.
The knowledge and information available regarding safety of any medicine is veritably important to take applicable decision by medicine controllers to safe guard public health. Healthcare professionals are the main journalists of the reporting reported encyclopedically. It's the major challenge of moment. In malignancy of those limitations, robotic reporting system remains as a most extensively habituated system to report ADRs and is suitable to induce signal of rare and veritably rare types of ADRs. However, we can make our world safer.
SUMMARY:-
This project focuses on the importance of monitoring the safety and proper use of medicines. Pharmacovigilance helps in identifying, understanding, and preventing the harmful effects of drugs. Adverse Drug Reactions (ADRs) are unwanted effects of medicines that can sometimes be serious and need close attention.
Clinical Pharmacy plays a key role in improving patient care by guiding doctors and patients in the safe and effective use of medicines. Medication Therapy Management (MTM) ensures that patients get the right medicines, in the right doses, and at the right time, reducing risks of side effects and improving treatment out comes.By studying ADRs and practicing MTM, healthcare professionals can improve patient safety, reduce healthcare costs, and build trust in medical treatment. This project highlights the need for teamwork between doctors, pharmacists, and patients to make medicine use safer and more effective.
FUTURE SCOPE :-
Future developments will see increased integration of innovative technologies like Artificial Intelligence (AI) and Machine Learning (ML) to automate signal detection and predictive modeling from vast datasets.
The use of electronic health records, wearable devices, and real-world evidence will enhance the depth and breadth of information available for analysis.
Promoting education and effective communication about pharmacovigilance and drug safety to healthcare professionals and the public is a key future goal.
Continued global collaboration and robust monitoring systems are essential to identify new safety issues and minimize risks.
Clinical pharmacists can play a major role in optimizing therapy, preventing medication errors, and ensuring better outcomes.
Growth of pharmacogenomics will help predict patient-specific ADR risks.Future systems may integrate genetic testing data for personalized drug therapy, reducing the likelihood of severe ADRs.
For early prediction and prevention of adverse drug reactions.
REFERENCES

Suchita Lathi, Baliram Sable, Radheshyam Jadhav, Shaikh Shahebaj, Ajinkya Pisule, A Review on Pharmacovigilance Adverse Drug Reactions Analysis Clinical Pharmacy Medication Therapy Management, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 908-925. https://doi.org/10.5281/zenodo.17830272
 10.5281/zenodo.17830272
10.5281/zenodo.17830272
