POMO Naik Tandaa, po. Jalna, Dist. Jalna
Malaria is a life-threatening disease caused by parasites of the genus Plasmodium, which are transmitted to humans through the bites of infected female Anopheles mosquitoes. It remains a significant global health concern, especially in tropical and subtropical regions, where environmental conditions favour mosquito breeding. The disease manifests with symptoms such as fever, chills, and flu-like illness, and can progress to severe complications or death if untreated. Despite ongoing efforts, malaria continues to pose a major public health challenge due to issues like drug resistance, limited access to healthcare, and the lack of an effective vaccine in widespread use. Current control strategies include the use of insecticide-treated nets, indoor residual spraying, and antimalarial medications. Advancements in diagnostic tools, treatment protocols, and vaccine development are critical to reducing the global burden of malaria and achieving long-term eradication goals.
Malaria is a serious and potentially fatal disease caused by protozoan parasites of the genus Plasmodium. It is primarily transmitted to humans through the bites of infected female Anopheles mosquitoes. Among the five Plasmodium species known to infect humans, Plasmodium falciparum and Plasmodium vivax are the most common, with P. falciparum being the most deadly. Malaria remains a major global health issue, particularly in parts of Africa, Asia, and Latin America, where climatic conditions support year-round mosquito activity. The disease presents with symptoms such as fever, chills, headache, and muscle pain, often resembling the flu, making early diagnosis essential. Although significant progress has been made in reducing malaria cases and deaths through preventive measures and treatment options, the emergence of drug resistance and challenges in vaccine implementation continue to hinder eradication efforts. Understanding the biology, transmission, and control strategies of malaria is crucial in the global fight against this disease. Malaria is a parasitic disease that continues to pose a major threat to global public health, particularly in tropical and subtropical regions. The illness is caused by protozoan parasites belonging to the genus Plasmodium, which are transmitted to humans through the bites of infected female Anopheles mosquitoes. Of the five Plasmodium species known to infect humans—P. falciparum, P. vivax, P. ovale, P. malariae, and P. knowlesi, P. falciparum is the most deadly and prevalent, especially in sub-Saharan Africa. Malaria is characterized by symptoms such as high fever, chills, sweating, headache, muscle pain, and nausea. If left untreated, it can lead to severe complications such as anemia, organ failure, coma, and even death. The disease poses a heavy burden on healthcare systems and affects economic development in many low- and middle-income countries. Despite being preventable and treatable, malaria remains a major global challenge. Factors such as poverty, lack of access to healthcare, climate conditions favorable to mosquitoes, and the development of resistance to both drugs and insecticides hinder control efforts. Strategies to combat malaria include the use of insecticide-treated bed nets, indoor residual spraying, early diagnosis, and effective antimalarial treatments. In recent years, advancements have been made in vaccine research, with the RTS, S/AS01 vaccine marking a significant milestone, although its widespread use is still being scaled up. Efforts by global health organizations, governments, and communities have led to a decline in malaria cases and deaths over the past two decades. However, the disease has not yet been eradicated, and ongoing investment in research, education, and public health infrastructure is essential to eliminate malaria and reduce its impact on vulnerable populations.Top of Form
Bottom of FormEpidemiology of Malaria
Malaria remains one of the most widespread infectious diseases globally, with its burden most heavily concentrated in tropical and subtropical regions. The disease is endemic in over 85 countries, with the highest transmission rates observed in sub-Saharan Africa, followed by parts of South Asia, Southeast Asia, and Latin America. According to global health reports, hundreds of millions of cases are recorded annually, and hundreds of thousands of people—particularly children under five and pregnant women—die each year due to the disease. The distribution and intensity of malaria transmission are influenced by several factors, including environmental conditions, vector density, socioeconomic status, and public health infrastructure. Regions with warm climates, high humidity, and consistent rainfall tend to have year-round transmission due to favorable conditions for mosquito breeding. Rural and remote areas, where healthcare access is limited and vector control measures are often insufficient, experience the highest burden. The Plasmodium species responsible for malaria vary in prevalence by region. P. falciparum is the dominant species in Africa and is associated with the most severe form of the disease. P. vivax is more common in Asia and Latin America and has the ability to remain dormant in the liver, causing relapses months after the initial infection. Less common species, such as P. ovale, P. malariae, and P. knowlesi, are found in specific geographic areas and often present with milder symptoms, though they can still cause serious illness. Efforts to control and eliminate malaria have led to significant progress over recent decades. Widespread distribution of insecticide-treated bed nets, improved access to diagnostic tools, availability of effective antimalarial drugs, and targeted indoor residual spraying have all contributed to the decline in malaria incidence and mortality. However, emerging challenges such as resistance to antimalarial drugs and insecticides, as well as the impact of climate change on mosquito habitats, continue to pose serious threats to malaria control programs. Effective malaria surveillance and reporting systems are essential for tracking the disease’s spread, targeting interventions, and evaluating progress. With coordinated global efforts and sustained funding, there is hope for further reductions in malaria cases and an eventual path toward elimination in endemic regions.
Symptoms of Malaria
Malaria symptoms typically begin within 10 to 15 days after being bitten by an infected mosquito. However, in some cases—especially with Plasmodium vivax and Plasmodium ovale—the parasites can remain dormant in the liver and cause symptoms weeks or even months later. The early signs of malaria often resemble those of the flu, making it difficult to diagnose without proper testing. Common initial symptoms include:
As the infection progresses, the fever may become more cyclical, often occurring in a pattern that includes a cold stage (chills and shivering), a hot stage (high fever), and a sweating stage (profuse sweating and drop in temperature). In severe cases, especially those caused by Plasmodium falciparum, the disease can lead to serious complications such as:
Young children, pregnant women, travelers from non-endemic areas, and individuals with weakened immune systems are at greater risk of developing severe malaria. Early diagnosis and treatment are critical to prevent complications and reduce the risk of death.
Life Cycle of Malaria
The life cycle of the malaria parasite is complex and involves two hosts: humans and female Anopheles mosquitoes. The parasite responsible for malaria belongs to the genus Plasmodium, and its life cycle is divided into two main stages: the human (asexual) stage and the mosquito (sexual) stage.
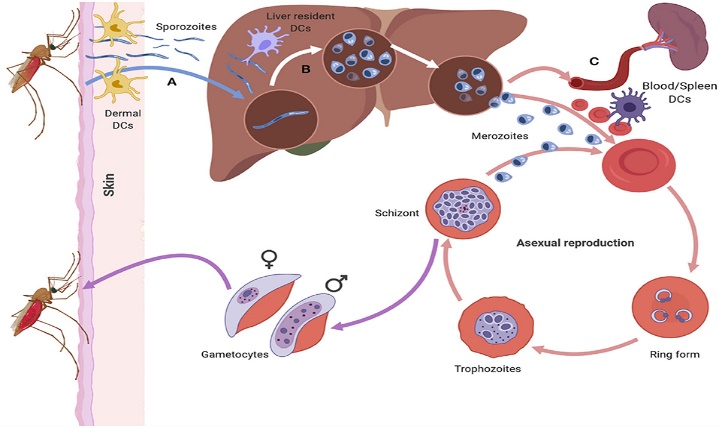
Fig no 1.1 malaria life cycle.
1. Transmission to Humans (Infective Stage)
The cycle begins when an infected female Anopheles mosquito bites a human, injecting sporozoites (the infectious form of the parasite) into the bloodstream.
2. Liver Stage (Exo-erythrocytic Cycle)
The sporozoites travel through the bloodstream to the liver, where they enter liver cells. Inside the liver cells, they multiply and mature into merozoites. This stage can last from a few days to several weeks. In the case of P. vivax and P. ovale, some parasites can become dormant (called hypnozoites) and reactivate later, causing relapses.
3. Blood Stage (Erythrocytic Cycle)
The merozoites are released from the liver into the bloodstream, where they invade red blood cells. Inside the red cells, they multiply again, eventually causing the cells to burst and release more merozoites. This repeated cycle is responsible for the characteristic symptoms of malaria, such as fever and chills. Some parasites develop into gametocytes, the sexual forms needed for mosquito transmission.
4. Transmission to Mosquito
When a mosquito bites an infected person, it ingests the gametocytes along with the blood. Inside the mosquito’s gut, the gametocytes develop into male and female sex cells, which then fuse to form a zygote.
5. Mosquito Stage (Sporogonic Cycle)
The zygote transforms into a motile form called an ookinete, which penetrates the mosquito’s gut wall and develops into an oocyst. The oocyst grows and produces thousands of new sporozoites. When the oocyst bursts, the sporozoites travel to the mosquito’s salivary glands, ready to infect a new human host when the mosquito feeds again. This cycle continues, enabling the parasite to spread and persist in regions where mosquitoes and human hosts are present. Understanding this life cycle is crucial for developing prevention and treatment strategies, including vaccines, drugs, and mosquito control efforts.
Pathophysiology of Malaria
Malaria develops when Plasmodium parasites, transmitted through the bite of an infected female Anopheles mosquito, enter the human body and begin to multiply. The disease’s pathophysiological effects are mainly caused by the parasite's interaction with liver cells and red blood cells, as well as the immune system's response to infection.
1. Liver Invasion and Parasite Development
After a mosquito bite, Plasmodium sporozoites enter the bloodstream and quickly migrate to the liver. There, they invade liver cells and mature into schizonts, which eventually burst and release thousands of merozoites into the bloodstream. In some cases (P. vivax and P. ovale), the parasites can remain dormant in the liver as hypnozoites and reactivate later.
2. Erythrocytic Stage – Red Blood Cell Destruction
Merozoites released from the liver invade red blood cells. Inside the cells, they multiply and develop through different stages (ring, trophozoite, and schizont). Infected red blood cells eventually rupture, releasing more merozoites that infect new cells. This destruction of red blood cells leads to anemia, one of the hallmark features of malaria. The release of waste products and parasitic toxins during this cycle stimulates the immune system, causing periodic fever, chills, and sweating—the classic symptoms of malaria.
3. Immune Response and Inflammation
The breakdown of red blood cells and release of parasite materials activate the immune system. Inflammatory cytokines such as tumor necrosis factor (TNF) and interleukins are released, contributing to fever and other systemic symptoms. In severe cases, excessive immune responses can lead to complications such as shock or organ dysfunction.
4. Severe Malaria Complications
Infections caused by Plasmodium falciparum are more likely to result in severe outcomes. This species can cause infected red blood cells to stick to blood vessel walls (a process called cytoadherence), especially in the brain, lungs, and kidneys. This can lead to life-threatening conditions like:
These complications arise from both the parasite’s actions and the body's inflammatory response. Understanding the pathophysiology of malaria is essential for developing effective treatments and for managing severe cases, especially in high-risk populations such as children, pregnant women, and individuals with weakened immune systems.
Diagnosis of Malaria
Accurate and timely diagnosis of malaria is essential for effective treatment and to prevent complications. Since the symptoms of malaria—such as fever, chills, headache, and fatigue—are similar to many other illnesses, laboratory confirmation is necessary to ensure the correct diagnosis.
1. Clinical Assessment
The first step in diagnosing malaria involves a medical history and physical examination. Doctors typically ask about recent travel to malaria-endemic regions, exposure to mosquitoes, and any previous episodes of malaria. However, clinical symptoms alone are not enough to confirm the disease.
2. Microscopic Examination (Blood Smear)
The most common and reliable method for diagnosing malaria is examining a blood sample under a microscope. A thick blood smear is used to detect the presence of malaria parasites, while a thin smear helps identify the specific species of Plasmodium. This method also allows doctors to estimate the level of parasitemia (how many red blood cells are infected), which can help determine the severity of the disease.
3. Rapid Diagnostic Tests (RDTs)
Rapid diagnostic tests are useful when laboratory facilities are not available. These tests detect specific proteins (antigens) produced by malaria parasites in a drop of blood. RDTs provide results within 15–20 minutes and are especially helpful in rural or low-resource settings. However, they may not always differentiate between species or measure parasite load accurately.
4. Molecular Tests (PCR)
Polymerase chain reaction (PCR) tests are used in research or specialized settings to detect malaria DNA in the blood. These tests are highly accurate and can identify species and detect low-level infections, but they require advanced laboratory equipment and are not typically used for routine diagnosis.
5. Serological Tests
Serological (antibody) tests can detect past malaria infections but are not useful for diagnosing current, active cases. They are mostly used for epidemiological studies.
Etiology of Malaria
Malaria is caused by infection with protozoan parasites of the genus Plasmodium. These parasites are transmitted to humans through the bite of infected female Anopheles mosquitoes, which serve as the primary vectors. Among the five Plasmodium species that infect humans, the most common and clinically significant are:
The life cycle of the parasite begins when an infected mosquito injects sporozoites into a person’s bloodstream during a blood meal. These sporozoites travel to the liver, multiply, and then enter red blood cells, where they continue to reproduce and cause symptoms. In addition to mosquito transmission, malaria can also spread through blood transfusions, organ transplants, sharing of contaminated needles, and from mother to child during childbirth, although these modes are far less common. The development and spread of malaria are influenced by environmental factors such as temperature, rainfall, and mosquito breeding sites. Human behavior, such as lack of mosquito protection and living in endemic areas, also plays a key role in disease transmission.
Management of Malaria
The management of malaria involves prompt diagnosis, effective treatment, and preventive measures to reduce transmission and complications. Successful control of the disease requires both individual care and broader public health strategies.
1. Treatment
The choice of treatment depends on several factors, including the type of Plasmodium species, the severity of the illness, the patient’s age, pregnancy status, and drug resistance patterns in the region.
For most cases of uncomplicated malaria, especially those caused by Plasmodium falciparum, the World Health Organization (WHO) recommends artemisinin-based combination therapies (ACTs). These combine artemisinin with another antimalarial drug to improve effectiveness and prevent resistance. Other antimalarial drugs, such as chloroquine, may be used for P. vivax, P. ovale, or P. malariae, where the parasite is still sensitive.
Severe or complicated malaria, often caused by P. falciparum, requires immediate hospitalization. Intravenous antimalarial drugs such as artesunate or quinine are administered, along with supportive care to manage complications like anemia, seizures, and organ failure.
In cases of P. vivax and P. ovale, additional treatment with primaquine or tafenoquine is given to target dormant liver-stage parasites and prevent relapses. However, these drugs are used only after screening for G6PD deficiency to avoid harmful side effects.
2. Supportive Care
Managing symptoms and complications is crucial, especially in severe cases. Supportive measures may include:
3. Prevention and Control
Preventive measures are essential for managing malaria at the community level. These include:
4. Vaccine Development
Although malaria vaccines have historically been difficult to develop, recent advances have shown promise. The RTS, S/AS01 (Mosquirix) vaccine has been introduced in some African countries for children and has demonstrated partial protection against P. falciparum malaria.
Pharmacological Treatment of Malaria
The pharmacological management of malaria depends on the species of Plasmodium, disease severity, patient factors, and regional drug resistance patterns. Effective treatment aims to eliminate the parasite from the bloodstream, prevent complications, and reduce transmission.
1. Artemisinin-Based Combination Therapies (ACTs)
ACTs are currently the first-line treatment for uncomplicated Plasmodium falciparum malaria worldwide. These combinations pair artemisinin or its derivatives (such as artesunate or artemether), which act rapidly to reduce parasite load, with a partner drug that clears remaining parasites and reduces the chance of resistance. Common ACTs include artemether-lumefantrine and artesunate-amodiaquine.
2. Treatment of Non-Falciparum Malaria
For Plasmodium vivax and Plasmodium ovale, chloroquine is often effective where resistance is not present. Additionally, to prevent relapses due to dormant liver stages (hypnozoites), patients receive primaquine or tafenoquine after screening for glucose-6-phosphate dehydrogenase (G6PD) deficiency, as these drugs can cause hemolysis in susceptible individuals.
3. Severe Malaria Treatment
Severe malaria requires urgent intravenous therapy. Intravenous artesunate is the preferred treatment due to its superior efficacy and safety profile compared to quinine. Quinine or quinidine may be used if artesunate is unavailable. Supportive care, including management of complications such as anemia, hypoglycemia, and organ failure, is critical during treatment.
4. Chemoprophylaxis
Preventive antimalarial drugs are recommended for travelers to endemic areas and certain high-risk groups. Options include atovaquone-proguanil, doxycycline, and mefloquine. The choice depends on factors such as duration of exposure, local resistance patterns, and patient tolerance.
SUMMARY
Pharmacological treatment of malaria is tailored to the parasite species, disease severity, and patient-specific factors. The widespread use of ACTs has significantly improved malaria outcomes, though challenges such as drug resistance and drug safety monitoring remain important considerations.
CONCLUSION
Malaria remains a significant global health challenge, particularly in tropical and subtropical regions where environmental conditions favor transmission. Despite advances in diagnosis, treatment, and prevention, the disease continues to cause substantial morbidity and mortality, especially among vulnerable populations such as children and pregnant women. Effective management relies on timely diagnosis, appropriate use of antimalarial drugs, and comprehensive preventive strategies including vector control and public education. Continued research, improved healthcare infrastructure, and international collaboration are essential to overcome challenges like drug resistance and to move closer toward the goal of malaria elimination worldwide.
REFERENCES

Umesh Adhe*, Bhaghshree Dhotre, Review on Malaria, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 5, 4705-4713. https://doi.org/10.5281/zenodo.15543211
 10.5281/zenodo.15543211
10.5281/zenodo.15543211
