Shri K R Pandav Institute of Pharmacy
The seventh cranial (facial) nerve malfunctions in Bell’s palsy, an acute neurological condition marked by abrupt unilateral facial paralysis. Even though the illness is usually transient and not fatal, it can have a major impact on speech, facial expressions, and general quality of life. Although the precise cause of Bell’s palsy is still unknown, viral infections, especially Herpes Simplex Virus type-1 (HSV-1), are thought to play a significant role. Inflammation, ischemia, autoimmune reactions, and systemic diseases like diabetes and hypertension are additional potentials. Recent scientific interest has focused on the role of the gut–brain axis (GBA) and the gut microbiota in neurological disorders. Through neural, hormonal, and immune pathways, the gut microbiome—which is made up of trillions of microorganisms—communicates with the central nervous system in both directions. Dysbiosis, or imbalances in the gut microbiota, may exacerbate neuroinflammation and systemic inflammation, which may have an impact on Bell’s palsy recovery and facial nerve damage. Corticosteroids, antiviral drugs, eye protection, physical therapy, and, in extreme situations, surgical procedures are the main components of conventional management. Herbal remedies and complementary therapies like acupuncture are also used to promote nerve regeneration and lower inflammation. Gaining knowledge about the connection between Bell’s palsy, the gut-brain axis, and microbiota could lead to new discoveries regarding the causes of various disease mechanisms and open avenues for innovative therapeutic strategies. Future studies that concentrate on microbiome-targeted therapies may enhance recovery results and provide a more comprehensive method of treating Bell’s palsy.
Nerve cells or neurons in the PNS fulfill a variety of roles. Motor neurons, for example, help to govern muscular movement. Sensory neurons communicate pain, temperature, and pressure to the CNS. Paralysis occurs when nerve impulses are disrupted due to injury to the nerves, spinal cord, or brain.
Paralysis are of two types as:
Permanent paralysis: When muscles control never comes back.
Temporary paralysis: When some or all muscle control returns.
Paralysis can also be broken down into two types based on the site of injury in the nervous system.
Types of Paralysis includes:
TABLE:1
|
1. Monoplegia |
Patient can’t move one limb only, such as one arm or one leg. |
|
2. Diplegia |
Paralysis occurs on the same area on both sides of the body. For examples, Paralysis affects both arms, both legs or both sides of face. |
|
3. Hemiplegia |
Paralysis affects one side of the body can arm and a leg on the same side. |
|
4. Paraplegia |
Its influences both legs and sometimes parts of the torso. |
|
5. Quadriplegia [Tetraplegia] |
The damage could be on both arms and both legs and sometimes the entire area from the neck down. |
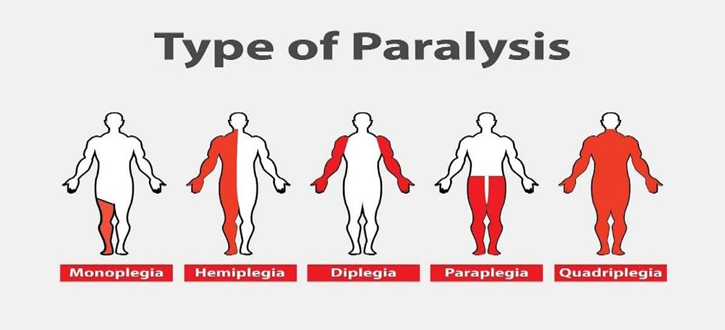
FIG:1 TYPES OF PARALYSIS
The most common causes of Paralysis:
Symptoms of Paralysis:
Risk Factors :-
Diagnosis and Tests:-
BRAIN GUT AXIS
The gut-brain axis [GBA] refers to the bidirectional communication between the gastrointestinal tract and the central nervous system. This communication is medicated by various signaling molecules, including neurotransmitters, hormones and immune factors. The GBA serves a pivotal role in maintaining homeostasis and significantly influencing numerous physiological processes. These processes include the regulation of mood, the response of stress, and various cognitive functions, all of which are integral to overall health and well-being. The importance of the GBA is highlighted by its critical involvement in both states of health and disease; disturbance or dysfunctions within this axis can result in a range of neurological and gastrointestinal disorders, thereby affecting the overall quality of life [2].
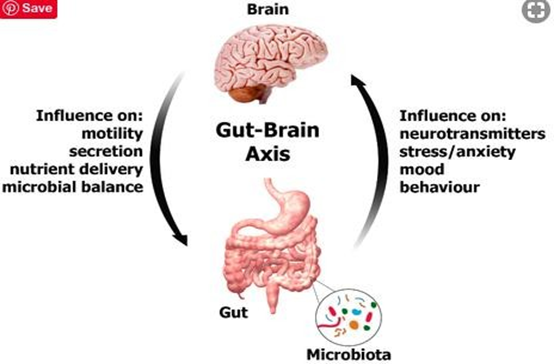
FIG:2 BRAIN GUT AXIS (BGA)
MICROBIOTA
The term ‘Microbiota’ refers to an ecological community of symbiotic and pathogenic microorganism that literally share our body space. Friedrich Escherich first cultured Escherichia coli from healthy people and Joshua Lederberg suggested the term Microbiota. There exists a symbiotic relationship between the host organism and the microbiota which are co-dependent on each other for survival. Total microbial cells in the gut are actually more than the human cells in the body. Total weight of the gut microbes is 1-2 kg. The gut has about 100 trillions of microbes -bacteria, yeasts, helminthes, viruses and protozoa[3].
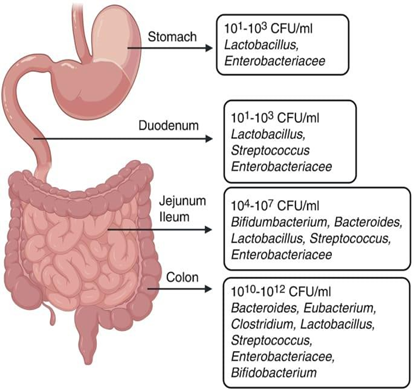
FIG: 3 COMPOSITION OF GUT MICROBIOME
BELL PALSY AND BGA CONNECTION WITH MICROBIOTA
The immune system and inflammation are two of the most significant ways the gut-brain axis influences neurological health. The term "neuroinflammation" describes inflammation in the brain or spinal cord, which is basically an overreaction of the immune system in the brain. Chronic neuroinflammation is a feature of several neurological conditions, including Parkinson's, Alzheimer's, and multiple sclerosis. What role does the stomach play in this, then?
A balanced immune response is maintained by the good bacteria in your gut, which serve as both a barrier and an immunological educator. However, an unbalanced gut (also known as gut dysbiosis) or a "leaky" gut lining can allow inflammatory chemicals to enter your bloodstream, causing inflammation throughout your body that could potentially affect your brain[4].
According to recent research, gut microorganisms may be able to control nervous system inflammation. For instance, some gut bacteria create chemicals that can either stimulate immune cells or migrate to the brain, which may increase or decrease neuroinflammation[5].
Our gastrointestinal tract's trillions of microorganisms produce chemicals that reach the circulation and have the potential to impact the brain, including some of the same neurotransmitters that our brains use. In actuality, the gut produces over 90% of the neurotransmitter serotonin, which is known to stabilize mood. It makes sense that scientists refer to our stomach as the "second brain," given that it produces numerous substances similar to those found in the brain and contains a vast nerve network of hundreds of millions of nerve cells[6].
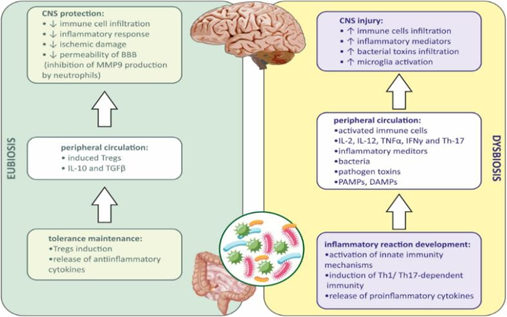
FIG: 4 CONNECTION OF MICROBIOTA WITH BGA AND BELL PALSY
BELL’S PALSY
Bell’s Palsy is a neurological disorder that causes facial paralysis or weakness on one side of face. It occurs when seventh cranial nerve become injured or stops working properly. Bell’s palsy is named after Sir Charles Bell [1774-1842] who first described the syndrome along with anatomy and function of facial nerve. The condition is not permanent, not fatal, not contagious and is not related to stroke.
The facial paralysis of Bell’s Palsy usually occur on just one side of face [Unilateral Palsy] but it can occur on both sides. Bilateral Bell’s Palsy is rare but possible for less than 1% of all cases. It occur usually without warning and can happen to anyone at any time.
Bell’s Palsy happens to approximately .025% of population which is 25 of every 10,00,000 people every year. The incidence of Bell’s Palsy in males and females as well as racially is approximately equal. The facial paralysis of Bell’s Palsy is usually short lived and recovery back to normal occur in majority of patients. The disorder usually progresses for 7 to 10 days, starting with the sudden onset of facial weakness. Recovery begins at 3 weeks for most [85%] patients, with a full recovery by 6 months. Between 4 to 6% experience severe deformity with very little return to normal facial movement, and 10 to 15% will be bother by asymmetrical movement of facial muscles. Patient who have had one episode of Bell’s Palsy have an 8% risk of recurrence.
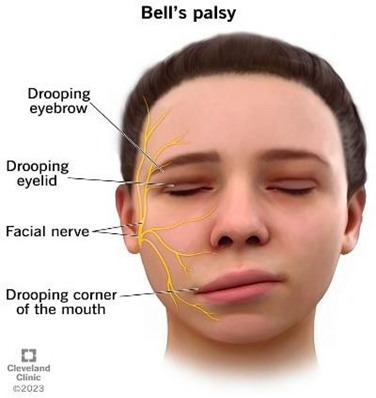
FIG: 5 CLINICAL FEATURES OF BELL’S PALSY
Typically,
SYMPTOMS
CAUSES
The cause of Bell’s Palsy, which has been demonstrated in several studies is thought to be the Herpes Simplex Virus Type 1 which attacks the facial nerve and causes swelling. In a 1995 study, Dr. Shingo Murakami and others determined that the HSV-1 was probably the most frequent cause of Bell’s Palsy at least 60 -70% of cases. Additionally research since then has been slowly reinforcing the conclusion.
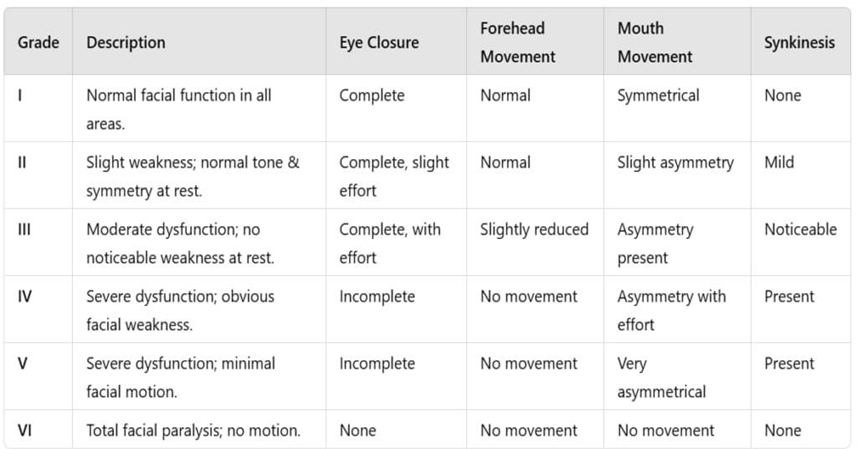
To clinically assess the severity of peripheral seventh cranial nerve palsy, a variety of scoring systems can be used. The House-Brackmann Facial Nerve Grading System (HBS) (Table 1) is widely used to classify the degree of facial paralysis. The House-Brackmann scale is a grading system that detects symmetry at rest and measures brow and lip movements to assess facial muscle functional recovery[8].
The House-Brackmann Facial Nerve Grading System
TABLE 2
ETIOLOGY
According to the statistics, there are numerous plausible causes of Bell’s palsy, but the etiology remains unknown. The causal agents are assumed to be herpes simplex virus 1 (HSV-1) and herpes zoster virus (HZV). However, HZV is the most dangerous virus be cause it propagates through the nerve via satellite cells. Aside from the virus, stroke and high blood pressure are the most likely reasons for sudden onset unilateral facial weakness with an obvious cause or idiopathic with an unknown cause.
According to the existing literature, numerous probable clinical diseases and pathologies might cause Bell’s palsy or facial palsy, but the actual etiology is unknown. Furthermore, the literature has identified several risk factors for the causes of Bell’s Palsy, such as anatomical changes or trauma, neoplastic changes, neurological abnormalities, viral infections, ischemia, inflammation, cold stimulation, and autoimmune responses, among others[9].
It is believed that compression of the seventh cranial nerve at the geniculate ganglion causes bell palsy. The labyrinthine segment, which is the first and narrowest part of the facial canal, is where most compression instances arise. Because of the facial canal’s small aperture, inflammation compresses and ischemias the nerve. A unilateral facial paralysis involving the forehead muscles is the most frequent finding.
Other causes of peripheral nerve palsies include Guillain-Barre Syndrome, Lyme disease, otitis media, Ramsay Hunt Syndrome, sarcoidosis and some influenza vaccines[10].
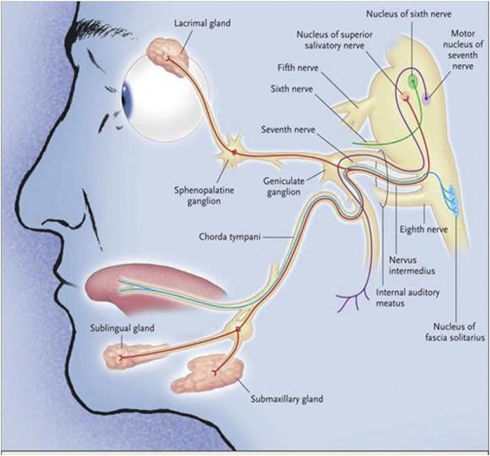
FIG 6: ETIOLOGY OF BELL’S PALSY
COMPLICATION OF BELL PALSY
The effects of Bell palsy will be felt for a long time.
Patient with Bell Palsy may be unable to close the eye on the affected side which can lead to irritation and corneal ulceration.
Permanent eyelid weakness may require implantation of gold weights in upper lid.
Facial asymmetry and muscular contractures may require cosmetic surgical procedures or Botulinum toxin (Botox) injections[11].
When nerve fibres are damaged, they can regenerate abnormally by connecting with the lacrimal ducts rather than the secretary glands. This causes tearing while eating or talking, which is referred to as "crocodile tears".
Similarly, poor motor neuron innervations cause erratic motions or facial synkinesis. In these circumstances, the facial clinometric examination scale (face) in conjunction with the House-Brackmann scale is used to track long-term patient satisfaction[12].
Bell palsy increases the risk of non-hemorrhagic stroke, according to research. Furthermore, as per studies, Bell palsy patients had a higher cumulative risk of stroke (4%) than the general population (1.6%)[13]
MANAGEMENT AND TREATMENT OF BELL’S PALSY
The first priority in treating Bell’s Palsy is to eliminate the source of nerve damage as quickly as possible. A minor compression of a nerve for a short period of time can result in mild, temporary damage. However, as time goes on with constant or increasing compression, damage to the nerve can also increase[14].
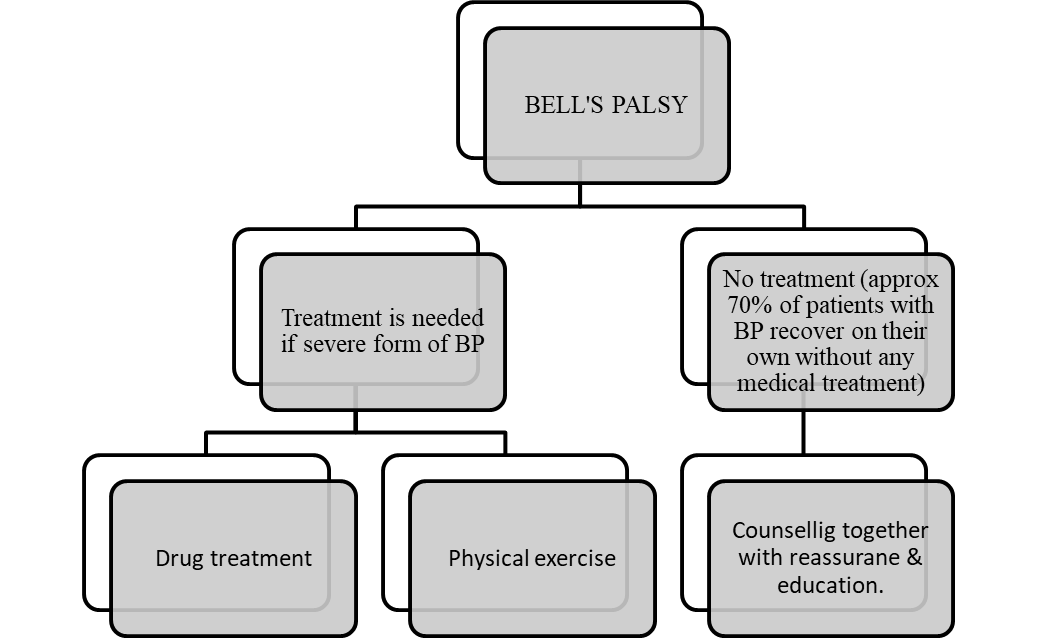
DRUG TREATMENT:
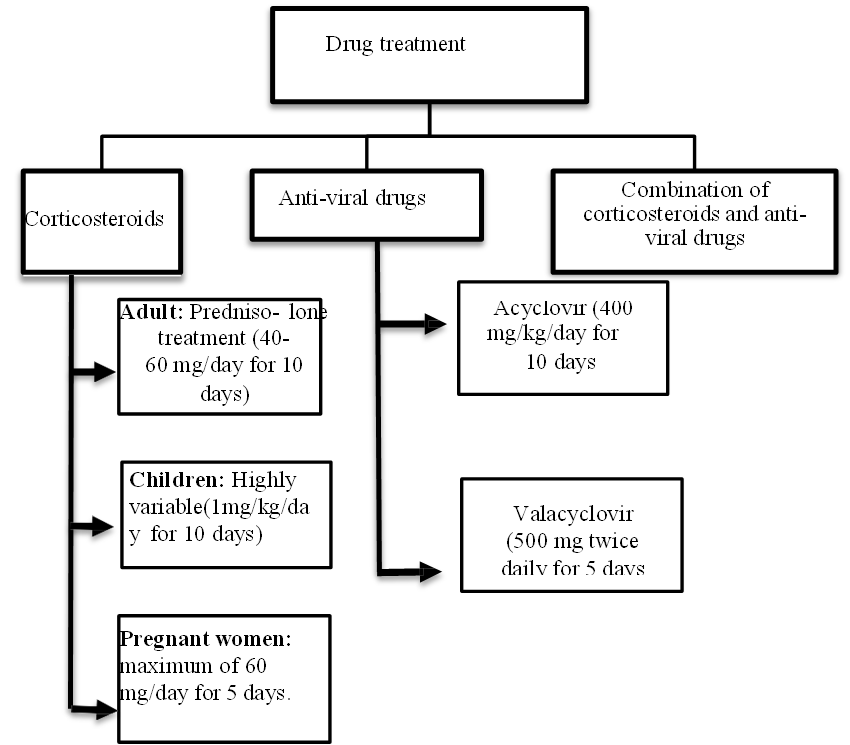
Since spontaneous healing does happen, the necessity of therapy is still debatable. The main course of therapy consists of corticosteroids, which are taken 60 to 80 mg each day for about a week. Research indicates that when corticosteroids and antivirals are taken together, the results can be better than when corticosteroids are taken alone. Antivirals were not statistically significant when added to steroids as a therapy for Bell palsy, according to a 2009 meta-analysis[15].
In patients with severe facial nerve palsy (House-Brackmann IV or above), antivirals and steroids may be used in combination. There has been no discernible rise in side effects associated with antivirals when compared to placebo or corticosteroids. In order to reduce the risk of corneal abrasion, patients should be instructed on how to use eye lubricant and put a patch to the afflicted eye before bedtime[16]. The long-term impact of this condition has decreased with the availability of botulinum toxin. As a final option, surgery can be necessary in situations that are persistent. There are intricate restorations available in situations where the face muscles do not degenerate over a number of years[17].
Methods for presenting ocular desiccation include muscle transfers and eyelid weights. Treatment options quality of earlier research assessing facial nerve compression was lacking. If no progress is shown after 4 weeks, it is advised to seek more aggressive therapies by referring the patient as soon as possible to a specialist, such as a plastic surgeon, neurologist, or otolaryngologist [18].
ACUPUNCTURE TREATMENT
Acupuncture treatment has been used in a variety of diseases including Bell’s palsy. The main advantage of this treatment is a low-risk, safe complementary treatment in both adults and children. Though acupuncture treatment is believed to produce a positive outcome in Bell’s Palsy, a variety of acupuncture methods are considered as a whole which misleads the effectiveness of diverse acupuncture procedures. There are various forms of acupuncture procedures, such as manual acupuncture, laser acupuncture, electroacupuncture, warm acupuncture, fire acupuncture, plum blossom acupuncture, and vertical acupuncture[19].
HERBAL TREATMENT
Herbal remedies are frequently employed in traditional medical systems such as Ayurveda and Traditional Chinese Medicine (TCM) as complementary treatments for Bell's palsy. Before beginning any new supplement regimen, it is crucial to speak with a healthcare provider. These are thought to help lower inflammation, enhance nerve function, and aid in healing[20].
MEDICINAL PLANTS FOR BELL’S PALSY
TABLE 3
|
Sr. No. |
Common name/ Vernacular name |
Scientific name |
Family |
Common uses |
|
1. |
Turmeric |
Curcuma longa |
Zingiberaceae |
Strong anti-inflammatory and antioxidant properties of curcumin may help lessen inflammation surrounding the facial nerve. |
|
2. |
Ashwagandha |
Withania somnifera |
Solanaceae |
It offer neuroprotective and adaptogenic qualities that improve the nervous system and lessen stress. |
|
3. |
Brahmi |
Bacopa monnieri |
Scrophulariaceae |
This herb is highly recognized as a brain and nerve tonic that may help regenerate nerves and lessen anxiety related to the illness. |
|
4. |
Bala |
Sida cordiflia |
Malvaceae |
Bala is well known for its neuroprotective and anti- inflammatory properties, which improve nerve function. |
|
5. |
Garlic |
Allium sativum |
Liliaceae |
Garlic enhance blood circulation, lessen discomfort and swelling, and open up bodily channels. |
|
6. |
Ginger |
Zingiber officinale |
Zingiberaceae |
Ginger, which is well-known for enhancing circulation and lowering inflammation, can aid in increasing blood flow to the muscles of the face. |
|
7. |
Licorice |
Glycyrrhiza glabra |
Fabaceae |
Has strong anti-inflammatory and antiviral properties |
|
8. |
Jatamansi |
Nardostachys jatamansi |
Caprifoliaceae |
Used to treat nerve-related disorders and soothe the brain. |
|
9. |
Nirgundi |
Vitex negundo |
verbenaceae |
Used to strengthen muscles and reduce nerve discomfort. |
|
10. |
Herba Siegesbeckiae |
Xixiancao |
Asteraceae |
Eliminate meridian channel blockages and control symptoms. |
CONSULTATION
Consultations that may be necessary when managing Bell palsy are as follows:
FUTURE SCOPE:
There is hope for even more advanced treatments in the future, both in terms of functional recovery and quality of life.
Future clinical trials and longitudinal studies will be essential in validating these approaches and ensuring that the benefits of these technologies can be fully realized.
A possible treatment for facial nerve palsy that has already been extensively studied in non- clinical publications is electrical stimulation of the orbicularis oculi muscle [22].
Telerehabilitation: The creation of portable electrical stimulation devices and remote monitoring systems to enable patients to carry out guided face exercises at home, perhaps enhancing results and lowering long-term consequences.
Surgical Innovations: Developments in nerve grafting, botulinum toxin injections, and facial reanimation surgery provide practical means of enhancing face symmetry and function for long-standing patients.
When there is no chance of further recovery of facial nerve function, a multidisciplinary team approach involving general practitioners, otolaryngologists, ophthalmologists, plastic surgeons, physiotherapists, and psychologists is crucial.
CONCLUSION
Bell’s palsy remains a multifactorial neurological disorder with a complex etiology involving viral infections, inflammation, immune dysregulation, and vascular factors. Emerging evidence suggests that the brain–gut axis and gut microbiota may play a significant role in modulating neuroinflammation and immune responses that influence the onset and recovery of facial nerve paralysis. Understanding how microbial imbalances can affect neural pathways opens new perspectives on holistic treatment approaches, combining conventional therapies—such as corticosteroids, antivirals, and physiotherapy—with microbiota-targeted interventions like probiotics, prebiotics, and dietary modifications.
Future research focusing on the gut–brain connection may unveil novel biomarkers for early diagnosis and personalized therapy, improving recovery outcomes and reducing recurrence. Thus, integrating microbiome science into the study of Bell’s palsy holds promising future aspects for developing preventive and therapeutic strategies that address not only the facial nerve but the entire neuro- immunological ecosystem of the body.
REFERENCES








Muskan Ramzan Sheikh, Nutan Hatwar, Bushra Shaikh, Aparna Markam, Chirag Jaiswal, Suresh Sonkusare, Vijaya Dhanki, Dhamsheela Gondane, A Review on Bell’s Palsy and The Brain-Gut Axis: Emerging Connection Between Microbiota, Int. J. of Pharm. Sci., 2026, Vol 4, Issue 3, 4212-4223. https://doi.org/10.5281/zenodo.19363240
 10.5281/zenodo.19363240
10.5281/zenodo.19363240
