Departments Of Pharmaceutical Sciences, Satyajeet College of Pharmacy, Mehkar- Buldana (Maharashtra).
Recent developments in anticancer pharmacology have significantly enhanced the efficacy and specificity of cancer treatments. Innovations in drug design, including targeted therapies and immunotherapies, have improved outcomes for various malignancies. Key advancements include the use of monoclonal antibodies, small molecule inhibitors, and checkpoint inhibitors that leverage the immune system to recognize and destroy cancer cells. Additionally, the integration of personalized medicine approaches, utilizing genomic profiling, allows for tailored therapies that maximize therapeutic benefit while minimizing toxicity. Novel delivery systems, such as nanoparticles and liposomes, enhance drug bioavailability and reduce side effects. Ongoing research continues to explore combination therapies and novel agents, promising to further improve survival rates and quality of life for cancer patients. These advances underscore the importance of a multidisciplinary approach in developing effective anticancer strategies. Ceramide drug use for cancer treatment they work in a irrevissible cell injury means apoptosis process. Ceramide are the classical anticancer drug.
In cancer research each cancer sample presents the researcher with an altered genome that contains a unique and unpredictable number of point mutations, indels, translocations, fusions, and other aberrations. Since many of these alterations might never have been observed before and might not necessarily reside in coding regions of the genome, whole-genome sequencing is increasingly seen as the only rigorous approach that can find all the variants in a cancer genome. Among all these

alterations are a select few that drive the progression of the disease. Based on the assumption that changes in gene expression levels impact disease progression, RNA- Seq is increasingly employed as a useful technique to determine if these genetic alterations impact disease progression. Genetic alterations have the potential to impact all cellular processes, including chromatin structure, DNA methylation, RNA splice variants, RNA editing, and microRNA (miRNA) to name but a few. Real progress in cancer research will come through the measurement and integrated analysis of all these interdependent processes. The key characteristic of next-generation sequencing technologies is that billions of independent sequence reads are generated in parallel, with each read derived from a single molecule of DNA. The resultant data approximate a random sample of DNA molecules which, in turn, represents the genomes of individual cells contained in the tumor sample.1 This provides us with a powerful toolbox to untangle the causes and mechanisms of cancer. (See Technical Considerations for additional information.) …(1-6)
Anticancer Drugs
Cancer is a disease of cells characterized by Progressive, Persistent, Purposeless and Uncontrolled Proliferation of tissues.

Both normal and cancerous cells must pass through the following phases of cell cycle
G0 phase (resting phase): Cells stop dividing temporarily or permanently (7)
Cell Cycle- Specific (Ccs) Or Phase- Specific Drug
Antimetabolites: Methotrexate, 6-mercaptopurine (6-MP)
Antibiotic: Bleomycin
Taxane: Paclitaxel
Epipodophyllotoxins: Etoposide, teniposide
Vinca alkaloids: Vinblastine, vincristine
Ccs drugs act mainly on dividing cells
Alkylating agents: Cyclophosphamide, busulphan, mechlorethamine, melphalan
Anticancer antibiotics: Doxorubicin, daunorubicin, mitomycin, actinomycin D
Metal complexes: Cisplatin, carboplatin
Novel mechanisms of action of classical chemotherapeutic agents on sphingolipid pathways:
Generation of ceramide: Ceramide can be generated by two distinct sphingolipid
pathways. The first pathway is initiated by hydrolysis of the phospholipid sphingomyelin that is preferentially concentrated in the plasma membrane of mammalian cells. This hydrolysis occurs within seconds to minutes after exposure to cytokines (i.e., TNF?, Fas), hormones,radiation, or environmental stresses (Verheij et al., 1996).
Rapid catabolism of membrane-bound sphingomyelin to ceramide (Figure 1) is mediated by the action of the neutral or the acid sphingomyelinase (ASMase), which are sphingomyelin-specific forms of phospholipase C (Fukset al., 1995). Alternatively, the second pathway involves de novo synthesis of ceramide via the condensation of the sphingoid base sphinganine and fatty acyl-CoA catalyzed by the enzyme (dihydro-
)ceramide synthase (CerS) to form dihydroceramide, which is then oxidized to ceramide by dihydroceramide desaturase (Figure 1). Ceramide is generated in the endoplasmic reticulum and transferred to the Golgi apparatus to be functionalized as the primary hydroxyl (Hirschberg et al., 1993; Shimeno et al., 1995; Spiegel et al., 1996). De novo sphingomyelin biosynthesis depends on non-vesicular ceramide trafficking by the CERamide Transfer (CERT) protein ( Hanadaetal., 2003). The ceramide-producing pathways are cell-type specific. In bovine aortic endothelial cells, it was shown that ionizing radiation, like TNF?, induces rapid sphingomyelin hydrolysis to ceramide (Haimovitz-Friedman et al., 1994). Conversely, in epithelial cells, the slower CerS pathway is predominant (Kolesnick and Fuks, 2003; Mesicek et al., 2010). Moreover, a selective tissue and subcellular distribution of six mammalian CerS isoforms was described combined with distinct fatty acyl chain length substrate preferences, implicating differential functions of specific ceramide species in cellular signaling (Mesiceket al., 2010). Interestingly, overexpression of CerS2 results in partial protection from irradiation-induced apoptosis, whereas overexpression of CerS5 increases apoptosis in HeLa cells (Mesicek et al., 2010). Generation of long chain ceramides C16-ceramide and C18-ceramide led to the inhibition of cell proliferation and induction of apoptosis, whereas very long chain ceramide, such as C24:0-ceramide and C24:1- ceramide, increased cell proliferation in MCF-7 (breast cancer) and HCT-116 (colon cancer) cells (Hartmann et al., 2012). Thus, in addition to the balance of ceramide producing and metabolizing pathways, the chain length of the resulting ceramide species generated seems to be important for inducing cell death or survival.
Mechanisms of ceramide-induced apoptosis
Ceramide acts as a second messenger in initiating apoptosis via the mitochondrial

system. Apoptotic cell death refers to an inducible preprogrammed pathway that
Figure 1: Pathways of ceramide can be synthesized de novo, released from sphingomyelin or generated from sphingosine, glucosylceramide or ceramide 1-phos generation. Ceramide phase. 5-FU, 5-fluoruracile; Cer, ceramide; Cer1P, ceramide 1- phosphate; GlcCer, glucosylceramide; PDMP, 1-phenyl-2-Decanoylamino-3- morpholino-1-propanol; PPMP, 1-phenyl-2-palmitoylamino-3-morpholino-1-propanol; S1P, sphingosine 1-phosphate; SM, sphingomyelin; SMase, sphingomyelinase.Involves sequential events that ultimately lead to activation of calcium- and magnesium- dependent endonucleases that fragment the nuclear chromatin at specific Internucleosomal linker sites. Elevation of ceramide with Exogenous ceramide analogs was shown to be enough For induction of apoptosis in bovine aortic endothelial Cells (Haimovitz-Friedman et al., 1994). Moreover, protein Kinase C (PKC) activation blocked both radiation-induced Sphingomyelin hydrolysis and apoptosis, and apoptosis Was reinstated by exogenously added ceramide analog (Haimovitz-Friedman et al., 1994).In addition to inducing apoptosis, ceramides are also Involved in autophagy by down- regulating nutrient transporters (Guenther et al., 2008). Autophagy refers to a survival pathway responsible for the breakdown of damaged Organelles, protein aggregates and long-lived proteins. This Process is initiated by the generation of double-membrane Vacuoles, the autophagosomes, which engulf these cellular Components. Subsequent fusion of the autophagosomes With the lysosomes results in the formation of single membrane autolysosomes in which the cellular contents are Degraded by hydrolytic lysosomal enzymes. Autophagy is Therefore a catabolic survival pathway that plays a role in Cancer suppression (Klionsky, 2007).It was shown that senescent fibroblasts are more Resistance to TNF?-induced apoptosis as the result of, At least in part, interrupted ceramide signaling, which Suggests that senescence may be another way to escape Apoptosis (Wright and Shay, 2001; DeJesus et al., 2002). In cancer cells, senescence can be induced by two distinct mechanisms: replicative senescence which involves Inhibition of telomerase, and senescent-like state induced Through the overexpression of cell-cycle-inhibitory proteins or DNA damage. Senescent cells present a barrier To the effective treatment of cancer because they might Be capable of subsequently re-entering active cell cycling Or could provide support to other cancer cells, including Stem cells (Modrak et al., 2009).Lastly, short-chain ceramide (C8- ceramide) was Shown to be capable of inducing both senescence and Apoptosis in a dose-dependent manner (Modrak et al., 2009). C8-ceramide-induced senescence occurred at lower Concentrations, whereas apoptosis was observed at higher Concentrations.
Immunotherapy and targeted therapies in cancer treatment:
Immunotherapy=
Cancer Immunotherapy
Helping the immune system work better at destroying cancer cells.
Cytokines are Cell signalling molecules that aid cell to cell communication in immune responses.
Anterleukins heln the immune system produce
05 Cancer Vaccines
ability to fight infections and disease. There are two broad types of cancer vaccines:
C. BCG Vaccines
BCG is a weakened form of the bacteria that causes Tuberculosis (Mycobacterium bovis). When inserted directly into the Bladder with a catheter, BCG causes an immune response against Cancer cells.
Administration Of Immunotherapy
Side Effects Of Immunotherapy
Introduction
?Drugs or other substances that block the growth and spread of cancer by interfering with specific molecules (“molecular targets”) involved in progression, and spread of cancer. The growth,
?”Molecularly targeted drugs,” “molecularly targeted therapies,” “precision medicines,”
?The major modalities (pharmacotherapy) for cancer. Of medical treatment
?Interfere with specific targeted molecules needed for carcinogenesis and tumor growth rather than by simply interfering with all rapidly dividing cells (e.g. with traditional chemotherapy).
Difference Between Targeted Therapy And Chemotherapy
|
Targeted Therapy |
Chemotherapy |
|
Act on specific molecular targets that are associated with cancer Deliberately chosen or designed to interact with their target Often cytostatic |
Act on all rapidly dividing normal and cancerous cells. Identified because they kill cells. Cytotoxic |
Target Identification For Targeted Therapie
Proteins present in cancer cells but not normal cells or more abundantin

cancer cells especially if they are known to be involved in cell growth or survival.
Example
Target identification cont’d….
Example:
The cell growth signaling protein BRAF is present in an altered form (known as BRAF V600E) in many melanomas.
? Vemurafenib (Zelboraf®) targets this mutant form of the BRAF protein and is approved to treat patients with metastatic melanoma that contains this altered BRAF protein.
Target identification cont’d….
Abnormalities in chromosomes present in cancer cells but not in normal cells. Sometimes these result in the creation of a fusion gene whose product, called a fusion protein, may drive cancer development. Such fusion proteins are potential targets for targeted cancer therapies.
Development Of Targeted Therapy
The main categories of targeted therapy are currently small molecules and monoclonal antibodies.
Monoclonal antibodies are relatively large and generally cannot enter cells, so they are used only for targets that are outside cells or on the cell surface.


Small Molecule Targeted Therapy
Identified in what are known as “high-throughput screens,” in which the effects of thousands of test compounds on a specific target protein are examined. Compounds that affect the target (sometimes called “lead compounds”) are then chemically modified to produce numerous closely related versions of the lead compound.
These related compounds are then tested to determine which are most effective and have the fewest effects on nontarget molecules.
Monoclonal Antibodies As Targeted Therap
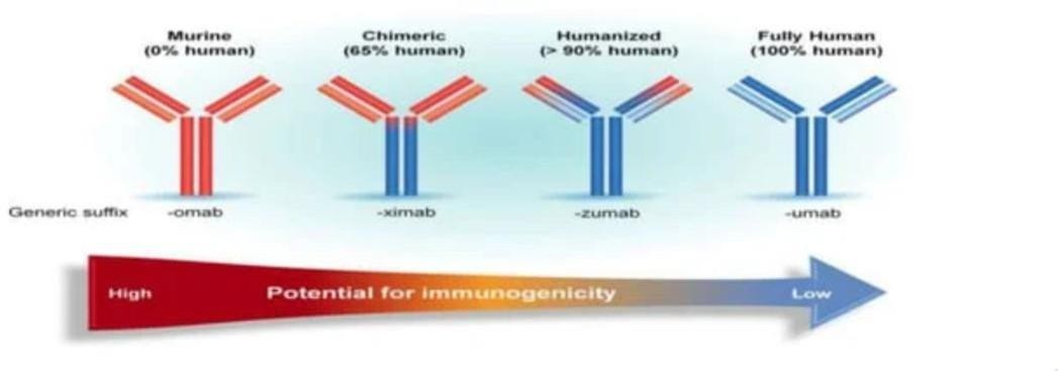
Developed by injecting animals (usually mice) with purified target proteins, causing the animals to make many different types of antibodies against the target.
Antibodies are then tested to find the ones that bind best to the target without binding to non target proteins.
Before monoclonal antibodies are used in humans, they are “humanized” by replacing as much of the mouse antibody molecule as possible with corresponding portions of human antibodies.


Side Effects Of Targeted Cancer Therapy
Common side effects: diarrhea and liver problems, such as hepatitis an elevated liver enzymes.
Others include:
Patients who develop acneiform rash while being treated erlotinib (Tarceva®) or gefitinib (Orissa®), have tended to respond better to these drugs than patients who do not develop the rash.
Patients who develop high blood pressure while being treated with the angiogenesis inhibitor bevacizumab generally have had better outcomes.
CONCLUSION
Immunotherapy and targeted therapy represent transformative approaches in cancer treatment, offering personalized strategies that enhance the body’s immune response or target specific cancer cell mechanisms. Ultimately, their combination can improve efficacy, reduce resistance, and lead to better patient outcomes. Continued research is essential to optimize these therapies and identify the best candidates for treatment. Would you like to delve deeper into a specific type of cancer or therapy Significant advances have been made in the chemotherapeutic management of cancer. Many new cytotoxic drugs that can potentially be used for the treatment of cancer, this life-threatening disease still causes near 7 million deaths every year worldwide and the number is growing.Cancer chemotherapy is usually accompanied by severe side effects and acquired drug resistance. We anxiously await the development of target therapy that will allow greater tumor specificity and less toxicity. So, targeted therapies using small molecules or monoclonal antibodies gaing importence due to its high specificity almost negligible effect on neighbouring cells Despite the promising clinical results from the agents that is highlighted, there is still significant limitation to the concept of “pathway-specific” targeted therapies as that most solid tumors are the result of numerous genetic mutations, and thus inhibiting a single cellular pathway may not result in a significant therapeutic outcome.
REFERENCES






Ravindrasing Patil, Tushar Ambhore, Hariom Chankhore, Tejas Sharma, Vinod Chaware, Dr. Shivshankar Mhaske, A Review on Advances in Anticancer Pharmacology, Int. J. of Pharm. Sci., 2024, Vol 2, Issue 12, 2257-2267. https://doi.org/10.5281/zenodo.14499676
 10.5281/zenodo.14499676
10.5281/zenodo.14499676
