1Shri Ganpati Institute of pharmaceutical science & research Centre Tembhurni.
2,4,5,6Bharati Vidyapeeth’s, College of Pharmacy, Sector-8, C.B.D. Belapur, Navi Mumbai-400 614.
3Shri Vithal Education & Research Institute's, College of Pharmacy, (Poly.), Gopalpur -Ranjani Road, Gopalpur Rd, Pandharpur, Maharashtra-413304.
Organophosphate (OP) compounds are widely utilized in agriculture, industry, and chemical warfare, making OP poisoning a major global health concern, particularly in developing regions. These compounds exert their toxic effects by irreversibly inhibiting acetylcholinesterase (AChE), resulting in excessive accumulation of acetylcholine at synapses and overstimulation of muscarinic, nicotinic, and central nervous system (CNS) receptors. The ensuing cholinergic crisis can lead to respiratory failure, convulsions, and death if not managed promptly. Diagnosis is primarily clinical, supported by biochemical assays of plasma and red blood cell cholinesterase activity. Management requires an integrated approach involving rapid decontamination, supportive care, and timely pharmacological intervention. The cornerstone of therapy includes atropine, which counters muscarinic hyperactivity; oximes such as pralidoxime and obidoxime, which reactivate inhibited AChE; and benzodiazepines for seizure control and neuroprotection. However, conventional antidotes face limitations such as poor blood–brain barrier penetration and reduced efficacy after enzyme “aging.” Recent advances have introduced bioscavenger enzymes, centrally acting oximes, and neuroprotective adjuncts like galantamine and magnesium sulfate, offering promising avenues for more effective management. This review comprehensively discusses the chemistry, toxicodynamics, clinical features, diagnostic approaches, and therapeutic strategies of OP poisoning, with an emphasis on the pharmacological mechanisms, comparative efficacy, and recent innovations in antidotal therapy. The evolving landscape of enzyme-based and combination treatments underscores the need for continued research to overcome existing therapeutic challenges and improve patient survival outcomes.
Organophosphates (OPs) are a broad class of organic compounds derived from phosphoric acid, characterized by the presence of phosphorus atoms bonded to oxygen or sulfur atoms and organic substituents. Chemically, they contain a central phosphorus atom attached to alkoxy, aryloxy, or thio groups, forming esters, amides, or thiol derivatives of phosphoric acid. These compounds act primarily as potent inhibitors of acetylcholinesterase (AChE), an enzyme responsible for hydrolyzing the neurotransmitter acetylcholine at synaptic junctions. By inhibiting AChE, OPs cause an accumulation of acetylcholine at cholinergic receptors, leading to overstimulation of muscarinic, nicotinic, and central nervous system pathways. This biochemical mechanism underlies their high toxicity in both insects and mammals. Although they are widely used for their pesticidal properties, the same mechanism of enzyme inhibition that kills pests also makes them hazardous to humans and animals when exposure occurs.
Historical Background of OP Use (Agriculture, Warfare, Insecticides)
The discovery and application of organophosphates date back to the early 20th century. Initially synthesized in the 1930s by German chemist Gerhard Schrader, organophosphates were first developed as potential insecticides due to their strong cholinesterase-inhibiting properties. However, during World War II, some derivatives such as tabun, sarin, and soman were weaponized as highly toxic nerve agents, marking one of the earliest examples of chemical warfare. Post-war, attention shifted toward their agricultural potential, and several organophosphate compounds, including parathion, malathion, and chlorpyrifos, were commercialized as pesticides. They became preferred over organochlorines due to their relatively faster biodegradation, reducing long-term environmental persistence. Nevertheless, their acute toxicity to humans, especially among agricultural workers and rural populations in developing countries, soon emerged as a major public health issue. The dual history of organophosphates—as both beneficial pesticides and deadly nerve agents—reflects their complex legacy in science, agriculture, and warfare.10-12
Epidemiology: Global and Regional Prevalence of OP Poisoning
Organophosphate poisoning represents a significant global health burden, particularly in developing countries where pesticide regulation, storage, and safe handling practices are often inadequate. According to the World Health Organization (WHO), pesticide poisoning accounts for nearly 3 million cases annually, with approximately 200,000 deaths, most of which are attributed to organophosphate exposure. The majority of these incidents occur in agricultural regions of Asia, Africa, and Latin America, where organophosphates are widely used for crop protection and pest control. India, Sri Lanka, and China report particularly high incidences, largely due to occupational exposure and intentional self-poisoning. In contrast, in developed countries, accidental or occupational exposures predominate, often due to industrial spills or contaminated food sources. Seasonal peaks in poisoning cases often coincide with agricultural spraying periods. The widespread availability of organophosphates and inadequate access to medical care contribute to the continued prevalence of morbidity and mortality associated with these compounds. Hence, organophosphate poisoning remains a critical public health issue requiring coordinated preventive, clinical, and regulatory interventions.
Relevance and Need for Reviewing Antidotal Therapy
Despite decades of research, the management of organophosphate poisoning continues to pose major therapeutic challenges. Current antidotal regimens—primarily based on atropine, oximes (such as pralidoxime), and benzodiazepines—are only partially effective and often fail to reverse severe central nervous system toxicity. Variability in response, limited efficacy of oximes in reactivating “aged” enzyme complexes, and poor penetration of antidotes across the blood-brain barrier highlight significant gaps in treatment. Furthermore, new organophosphate compounds with varying chemical structures continue to emerge, some of which display resistance to conventional therapies. Reviewing the pharmacological basis, clinical performance, and limitations of existing antidotes is essential for optimizing treatment protocols and guiding future research. Understanding the mechanisms of antidote action can also aid in the rational design of next-generation agents capable of providing broader and more effective protection against OP toxicity.
This review aims to provide a comprehensive analysis of organophosphate poisoning with a particular focus on the pharmacological antidotes currently available and under investigation. The objectives are to elucidate the chemistry and mechanism of toxicity of organophosphates, summarize their global impact on human health, and critically evaluate existing therapeutic approaches. The review also explores recent advancements in antidotal therapy, including novel oxime derivatives, enzyme-based bioscavengers, and neuroprotective agents, as well as emerging strategies for improved management. By integrating findings from experimental, clinical, and epidemiological studies, this review seeks to identify current gaps in treatment efficacy and highlight potential directions for future drug development and public health policy. Ultimately, the goal is to enhance clinical outcomes and reduce mortality associated with organophosphate poisoning through a deeper understanding of pharmacological interventions.
Chemistry and Classification of Organophosphates13-15
Chemical Structure and Classification (Based on Functional Groups)
Organophosphates (OPs) are organic esters, amides, or thiol derivatives of phosphoric acid. Their general molecular formula is represented as (RO)?P=O or (RO)?P(S)-OR’, where R and R’ denote alkyl, aryl, or alkoxy groups, and O or S represents oxygen or sulfur atoms. The phosphorus atom serves as the central reactive site, capable of forming multiple bonds with oxygen or sulfur and single bonds with organic substituents. This structural variability gives rise to a wide range of organophosphate compounds with differing degrees of lipophilicity, volatility, and stability.
From a chemical standpoint, organophosphates can be classified according to their functional groups and substitution patterns:
The P–O–C and P–S–C bonds determine the activation and metabolic conversion of these compounds. Notably, phosphorothioates and dithioates are often pro-toxicants, requiring oxidative desulfuration by hepatic cytochrome P450 enzymes to convert into active oxon forms (e.g., parathion → paraoxon), which are potent acetylcholinesterase inhibitors.
Common Organophosphate Compounds
Organophosphates encompass a diverse array of compounds used in agriculture, veterinary medicine, and warfare. Agricultural OPs are used mainly as insecticides, whereas certain highly toxic variants have been weaponized as nerve agents. The table below summarizes some of the most important and representative OPs, their chemical groups, applications, and toxicity characteristics:16-17
|
Compound |
Chemical Class / Type |
Common Use |
Mechanism of Activation |
Relative Toxicity |
|
Malathion |
Phosphorodithioate |
Agricultural insecticide, public health use |
Requires oxidative desulfuration to malaoxon |
Low to moderate (safer for mammals) |
|
Parathion |
Phosphorothioate |
Agricultural insecticide (restricted) |
Converted to paraoxon in vivo |
High |
|
Chlorpyrifos |
Phosphorothioate |
Crop protection (now banned in many regions) |
Oxidized to chlorpyrifos-oxon |
High |
|
Diazinon |
Phosphorothioate |
Household and crop insecticide |
Metabolized to diazoxon |
Moderate |
|
Dichlorvos (DDVP) |
Phosphate |
Fumigant insecticide |
Active form, no metabolic activation required |
High |
|
Sarin (GB) |
Phosphonate |
Chemical warfare nerve agent |
Direct AChE inhibition |
Extremely high (lethal at minute doses) |
|
Soman (GD) |
Phosphonate |
Warfare agent |
Very rapid “aging” of enzyme complex |
Extremely high |
|
VX |
Phosphonothioate |
Nerve agent |
Direct AChE inhibition |
Extremely high, persistent |
|
Tabun (GA) |
Phosphoramidate |
Warfare agent |
Direct inhibition |
Very high |
This diversity illustrates that organophosphates share a common pharmacodynamic mechanism (AChE inhibition) but differ widely in potency, metabolism, and environmental persistence, primarily due to variations in their chemical structure.
3.3 Physicochemical Properties Influencing Toxicity and Absorption18-22
The toxicokinetics and toxicodynamics of organophosphates are profoundly influenced by their physicochemical characteristics. Key parameters include lipophilicity, volatility, solubility, molecular weight, and stability.
Lipophilic OPs (e.g., chlorpyrifos, parathion) are readily absorbed through the skin and accumulate in adipose tissue, leading to prolonged toxicity and delayed symptoms. Their fat solubility also enhances penetration across the blood-brain barrier, resulting in central neurotoxicity.
Overview and Toxicological Implications
The chemical versatility of organophosphates accounts for their widespread use and their variable toxicological profiles. The substitution pattern around the phosphorus atom dictates not only biotransformation pathways but also the efficacy of antidotal therapy. For instance, oxime reactivators show differing effectiveness depending on whether the inhibited AChE complex involves a phosphate or phosphonate linkage. Therefore, a detailed understanding of OP chemistry is fundamental to developing effective detoxification strategies, designing new antidotes, and establishing safer alternatives in agriculture and defense.
Mechanism of Toxicity23-28
Pathophysiology: Inhibition of Acetylcholinesterase (AChE)
The primary mechanism underlying organophosphate (OP) toxicity is the irreversible inhibition of the enzyme acetylcholinesterase (AChE), which is responsible for hydrolyzing the neurotransmitter acetylcholine (ACh) into acetate and choline at cholinergic synapses. Under normal physiological conditions, AChE ensures the rapid termination of nerve impulses. However, exposure to organophosphates leads to phosphorylation of the serine hydroxyl group at the active site of AChE, forming a stable phosphorylated enzyme complex. This inactivation prevents the breakdown of ACh, causing its excessive accumulation at synaptic junctions throughout the central and peripheral nervous systems.
The inhibition is initially reversible, but with time, the phosphorylated enzyme undergoes conformational changes known as “aging”, making the inhibition irreversible and preventing reactivation by antidotes like oximes. This results in sustained cholinergic overstimulation, producing the characteristic toxic manifestations of organophosphate poisoning.
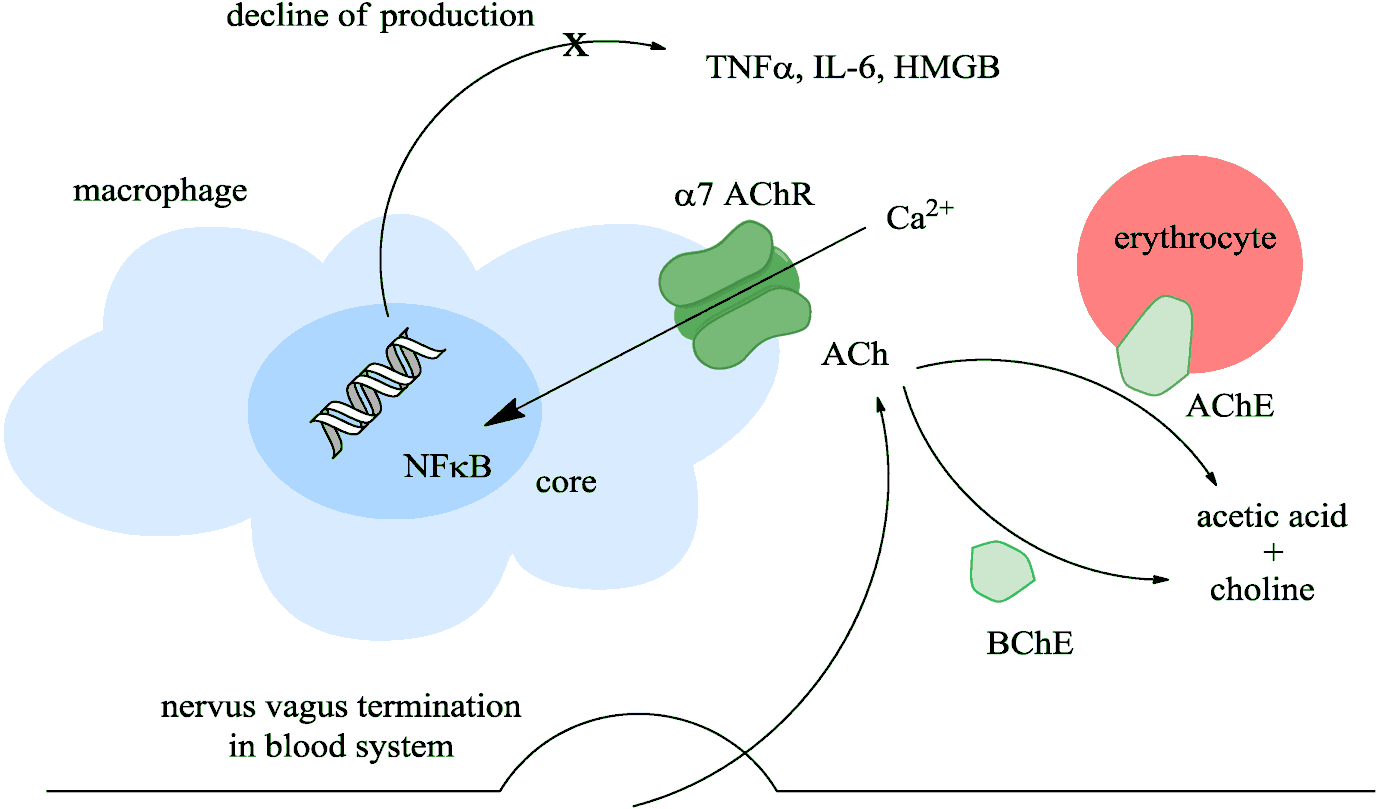
Figure 1: Mechanism of Toxicity (AChE Inhibition Pathway)
Accumulation of Acetylcholine and Overstimulation of Cholinergic Receptors
The excessive accumulation of acetylcholine at neuronal junctions leads to continuous stimulation of cholinergic receptors in the autonomic nervous system, neuromuscular junctions, and central nervous system (CNS).
The magnitude and duration of receptor overstimulation determine the severity and outcome of poisoning, ranging from mild muscarinic symptoms to life-threatening respiratory failure.
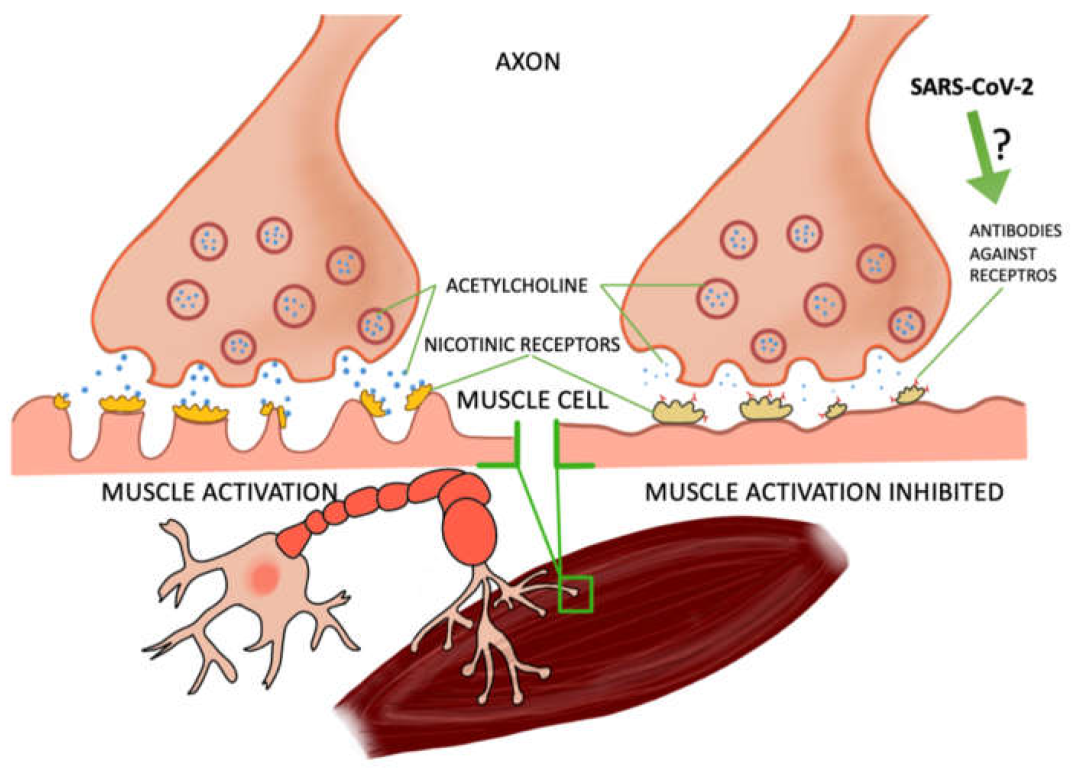
Figure 2: Cholinergic Receptor Sites (Muscarinic Nicotinic CNS)
Effects on Muscarinic, Nicotinic, and CNS Receptors
The toxic manifestations can be better understood by categorizing them based on receptor sites:
|
Receptor Type |
Anatomical Location |
Major Effects of Overstimulation |
|
Muscarinic |
Smooth muscles, glands, heart |
Miosis, blurred vision, lacrimation, salivation, bronchospasm, bronchorrhea, bradycardia, hypotension, vomiting, diarrhea, urination |
|
Nicotinic |
Skeletal muscles, autonomic ganglia |
Muscle twitching, fasciculations, weakness, paralysis, hypertension, tachycardia |
|
CNS (Central cholinergic receptors) |
Brain, medulla, and spinal cord |
Anxiety, confusion, convulsions, respiratory depression, coma |
The simultaneous activation of all these receptor systems leads to the characteristic “cholinergic crisis”, which, if untreated, can result in respiratory failure and death due to paralysis of the diaphragm and central respiratory centers.
Acute and Chronic Neurotoxic Effects
Organophosphate poisoning produces both acute and delayed (chronic) neurological consequences.
The “Aging” Process of the Phosphorylated Enzyme Complex
Once the organophosphate binds to AChE, the phosphorylated enzyme complex can undergo a spontaneous chemical change known as “aging.” During this process, one of the alkyl or alkoxy side chains is cleaved from the phosphorylated enzyme, producing a negatively charged oxygen atom, which stabilizes the phosphorus-enzyme bond and makes it resistant to nucleophilic attack by antidotes (such as oximes).
The rate of aging varies among OP compounds—rapid for nerve agents like soman (within minutes) and slower for insecticides like parathion (hours). This variability influences the therapeutic window for effective oxime treatment.
|
Compound |
Type |
Approximate Aging Time |
|
Soman (GD) |
Nerve agent |
2–6 minutes |
|
Sarin (GB) |
Nerve agent |
3–5 hours |
|
Parathion |
Insecticide |
12–20 hours |
|
Malathion |
Insecticide |
>24 hours |
|
VX |
Nerve agent |
24–48 hours |
Understanding the aging process is essential for timely administration of reactivators and successful management of organophosphate poisoning.
Clinical Manifestations of Organophosphate Poisoning29-32
Acute Symptoms
The acute cholinergic crisis presents within minutes to hours after exposure, depending on the route and dose. Symptoms can be remembered using the mnemonic “DUMBELS” (Defecation, Urination, Miosis, Bronchorrhea/Bronchospasm, Emesis, Lacrimation, Salivation).
Common clinical features include:
If untreated, death occurs due to respiratory failure, either from central depression, muscle paralysis, or excessive secretions blocking airways
Chronic Exposure Effects
Chronic or repeated low-dose exposure to OPs, common among farmers and pesticide handlers, leads to subclinical or progressive neurological impairment. Manifestations include:
These effects are thought to be due not only to AChE inhibition but also to secondary oxidative stress, mitochondrial dysfunction, and inflammation in neural tissue.
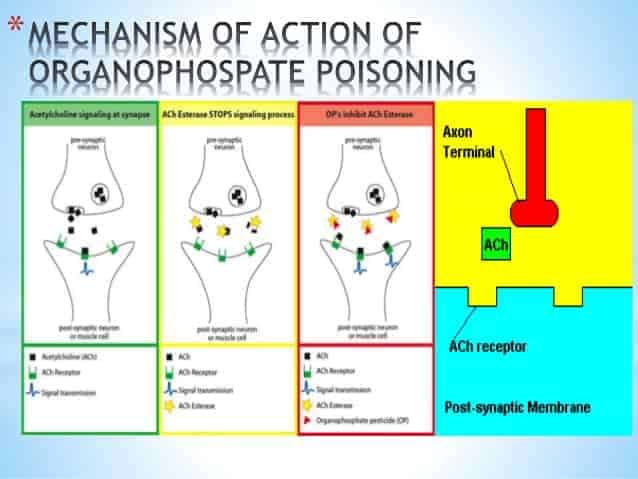
Figure 3: Organophosphate poisoning
Intermediate Syndrome (IMS) and Organophosphate-Induced Delayed Neuropathy (OPIDN)33-35
Severity Grading of OP Poisoning
The Peradeniya Organophosphorus Poisoning (POP) Scale is widely used to assess the severity of poisoning at admission, based on clinical signs such as pupil size, respiratory rate, heart rate, fasciculations, consciousness level, and seizure activity.
|
Clinical Parameter |
Score 0 |
Score 1 |
Score 2 |
|
Pupil size |
>2 mm (normal) |
Pinpoint |
- |
|
Respiratory rate |
<20/min |
20–30/min |
>30/min |
|
Heart rate |
>60 bpm |
41–60 bpm |
≤40 bpm |
|
Fasciculations |
None |
Present, localized |
Generalized |
|
Level of consciousness |
Conscious |
Impaired |
Unconscious |
|
Seizures |
Absent |
Present |
- |
This scale helps clinicians predict outcomes and determine the intensity of treatment required.
Organophosphate poisoning involves a cascade of neurotoxic events—from enzyme inhibition and acetylcholine accumulation to receptor overstimulation and progressive neuronal damage. The clinical spectrum ranges from acute cholinergic crises to delayed neuropathic syndromes, emphasizing the need for early recognition, prompt antidote administration, and supportive therapy. Understanding the mechanistic basis of these effects aids in developing more targeted pharmacological interventions and improving patient survival.
Diagnosis36-40
The diagnosis of organophosphate (OP) poisoning is primarily clinical, supported by biochemical and toxicological confirmation. Rapid and accurate identification is critical for early initiation of antidotal therapy, which can significantly improve outcomes.
The clinical diagnosis of OP poisoning is usually based on recognizing the classic cholinergic syndrome—a constellation of signs resulting from excessive acetylcholine at muscarinic, nicotinic, and central receptors. Common clinical indicators include miosis (pinpoint pupils), profuse salivation, bronchorrhea, bradycardia, muscle fasciculations, and respiratory distress. The mnemonic DUMBELS (Defecation, Urination, Miosis, Bronchorrhea/Bronchospasm, Emesis, Lacrimation, Salivation) or SLUDGE (Salivation, Lacrimation, Urination, Defecation, Gastrointestinal distress, Emesis) often aids clinicians in quick recognition. Neuromuscular weakness and central effects such as anxiety, confusion, or seizures further support the diagnosis. Clinical severity can be assessed using the Peradeniya Organophosphorus Poisoning (POP) Scale, which quantifies signs like pupil size, heart rate, fasciculations, and level of consciousness to categorize cases as mild, moderate, or severe, thereby guiding treatment intensity.
Biochemical confirmation is achieved by measuring cholinesterase activity in blood, primarily plasma (butyrylcholinesterase) and red blood cell (RBC) acetylcholinesterase levels. Plasma cholinesterase reflects recent exposure and is a sensitive but non-specific marker, while RBC AChE better represents synaptic enzyme inhibition and correlates closely with the clinical severity of poisoning. In general, plasma cholinesterase activity falls to less than 50% of normal in mild poisoning and below 10% in severe cases. Serial monitoring of enzyme activity is also useful in evaluating recovery and the effectiveness of therapy.
|
Enzyme Type |
Site of Measurement |
Function/Significance |
Interpretation in OP Poisoning |
|
Plasma (Butyrylcholinesterase, BChE) |
Serum or plasma |
Detoxification of OP compounds |
Rapidly depressed after exposure; useful for screening |
|
Erythrocyte (True AChE) |
RBC membrane |
Reflects synaptic AChE activity |
Strongly correlates with clinical severity and prognosis |
Toxicological analysis can further confirm exposure by identifying the parent OP compound or its metabolites in biological fluids such as blood, urine, or gastric contents using gas chromatography–mass spectrometry (GC-MS), high-performance liquid chromatography (HPLC), or enzyme-linked immunoassays. Metabolites such as dialkyl phosphates (DAPs) or specific oxon derivatives serve as biomarkers of OP exposure. While such analyses are vital for research and forensic investigations, clinical management typically relies on rapid bedside evaluation and cholinesterase assays due to time constraints in emergencies.
Management of Organophosphate Poisoning41-45
Effective management of OP poisoning requires a multifaceted approach, combining immediate decontamination, supportive measures, and targeted pharmacological therapy. The primary goal is to prevent further absorption, maintain vital functions, and counteract the effects of acetylcholine excess.
Decontamination is the first and most essential step in preventing ongoing exposure. Contaminated clothing should be promptly removed, and the skin thoroughly washed with soap and copious water. Eye contamination requires irrigation with saline or clean water. Gastric lavage may be considered if ingestion occurred within one hour and the airway is protected, though it is contraindicated in comatose or convulsing patients without intubation. Activated charcoal can adsorb residual poison in the gastrointestinal tract, though its use should be cautious due to potential aspiration risk. Decontamination must be carried out by trained personnel using protective gear to avoid secondary contamination.
Supportive care remains the cornerstone of treatment. Airway protection, oxygen supplementation, and mechanical ventilation are crucial in cases of respiratory compromise caused by bronchorrhea, bronchospasm, or diaphragmatic paralysis. Continuous monitoring of cardiac rhythm, pulse oximetry, and vital signs is essential. Intravenous fluids should be administered judiciously to maintain perfusion without exacerbating pulmonary edema. Seizures, if present, must be controlled promptly using benzodiazepines such as diazepam, which also offer neuroprotective benefits. Correction of electrolyte imbalance and acid-base disturbances forms part of supportive management.
Pharmacological antidotal therapy is the most specific and lifesaving intervention in OP poisoning. The standard regimen includes atropine, oximes, and benzodiazepines, often used in combination.
Atropine is a competitive antagonist of muscarinic acetylcholine receptors and remains the mainstay of therapy. It effectively reverses the life-threatening muscarinic effects such as bronchorrhea, bronchospasm, bradycardia, and hypotension. Treatment begins with 1–2 mg intravenously in adults, repeated every 5–10 minutes until full atropinization is achieved, indicated by clear lung fields (drying of secretions), heart rate above 80 beats per minute, and dilated pupils. The total dose required varies widely, often reaching hundreds of milligrams in severe cases. Continuous infusion may be necessary to maintain effect, as atropine does not influence nicotinic symptoms such as muscle weakness.
Oximes, such as pralidoxime (2-PAM), obidoxime, and HI-6, act by reactivating acetylcholinesterase before the enzyme undergoes irreversible “aging.” These compounds cleave the phosphate–enzyme bond, restoring AChE activity. The efficacy of oximes depends on the specific OP compound and the timing of administration; early use, preferably within a few hours of exposure, yields better results. Pralidoxime is typically given as an intravenous bolus of 30 mg/kg followed by infusion at 8–10 mg/kg/hour. Obidoxime, more potent in certain OPs, is used at 250 mg bolus followed by 750 mg/day infusion. The newer reactivator HI-6 demonstrates superior CNS penetration and effectiveness against nerve agents, though its availability is limited. Oximes are less effective once enzyme aging has occurred, emphasizing the importance of rapid diagnosis and intervention.
Benzodiazepines such as diazepam or midazolam serve dual roles in controlling seizures and providing neuroprotection by counteracting the excitotoxic neuronal injury induced by excessive cholinergic stimulation. Diazepam (5–10 mg IV) is administered as required to control convulsions and reduce the risk of delayed neurological sequelae. In animal and clinical studies, early benzodiazepine administration has shown to improve survival and prevent neuronal damage.
In addition to these standard antidotes, several novel or experimental agents are being explored. Human butyrylcholinesterase (BChE) acts as a bioscavenger, binding OPs before they inhibit endogenous AChE, thus offering a preventive or pre-exposure therapeutic strategy. Galantamine, a reversible AChE inhibitor with central activity, has shown potential neuroprotective effects by modulating nicotinic receptors and reducing excitotoxicity. RS194B, a new-generation oxime with enhanced BBB permeability, is under investigation for its superior CNS reactivation capacity. These advances represent promising directions toward more effective management of OP poisoning.
Several adjunctive therapies can complement standard antidotal treatment. Magnesium sulfate helps stabilize neuronal membranes, reducing ACh release and mitigating excitotoxicity. N-acetylcysteine (NAC), an antioxidant and glutathione precursor, may attenuate oxidative stress and tissue injury caused by OPs. Corticosteroids can suppress inflammatory responses and edema associated with CNS toxicity, although their clinical utility remains under debate. Together, these adjuncts may enhance recovery and minimize complications when integrated with conventional therapy.
|
Therapeutic Agent |
Mechanism of Action |
Typical Dose (Adult) |
Remarks/Advantages |
|
Atropine |
Blocks muscarinic receptors |
1–2 mg IV every 5–10 min until secretions dry; continuous infusion as needed |
Main lifesaving drug; relieves bronchorrhea, bradycardia |
|
Pralidoxime (2-PAM) |
Reactivates AChE before aging |
30 mg/kg IV bolus, then 8–10 mg/kg/hr infusion |
Effective if given early; limited CNS action |
|
Obidoxime |
AChE reactivation |
250 mg IV bolus, then 750 mg/day |
Broader spectrum than pralidoxime |
|
Diazepam |
GABA-A agonist; controls seizures |
5–10 mg IV as needed |
Provides neuroprotection |
|
Magnesium sulfate |
Stabilizes neuronal membranes, reduces ACh release |
1 g IV every 6 hours |
Adjunctive benefit; reduces mortality |
|
N-acetylcysteine |
Antioxidant, replenishes glutathione |
150 mg/kg loading, then infusion |
Reduces oxidative tissue injury |
|
Butyrylcholinesterase (BChE) |
Bioscavenger, binds OPs |
Under investigation |
Preventive/prophylactic use |
Role of Pharmacological Antidotes46-52
The treatment of organophosphate poisoning relies heavily on pharmacological antidotes, which aim to counteract the excessive accumulation of acetylcholine resulting from acetylcholinesterase (AChE) inhibition. The three main therapeutic agents—atropine, oximes, and benzodiazepines—are often used in combination to reverse muscarinic overstimulation, reactivate the inhibited enzyme, and control central nervous system (CNS) excitation. Although these antidotes have saved countless lives, limitations such as poor central penetration and reduced efficacy after “aging” of the enzyme necessitate the development of improved or adjunctive therapies, including bioscavengers and engineered enzyme-based antidotes.
The mechanism of each antidote is distinct yet complementary, targeting different aspects of OP toxicity. Atropine, a tertiary amine and competitive antagonist at muscarinic acetylcholine receptors, remains the cornerstone of therapy. It blocks the peripheral effects of acetylcholine accumulation, including bronchial secretions, bronchospasm, bradycardia, and gastrointestinal hypermotility. Its lipophilic nature allows partial penetration into the CNS, where it alleviates central respiratory depression and delirium. However, atropine has no effect on nicotinic manifestations such as muscle weakness or fasciculations, highlighting the need for adjunctive agents.
Oximes (e.g., pralidoxime, obidoxime, HI-6) play a pivotal role by directly addressing the root cause—reversible reactivation of phosphorylated AChE. These nucleophilic agents bind to the phosphorylated enzyme and remove the phosphate group, restoring normal enzymatic function and acetylcholine breakdown. The efficacy of oximes depends largely on the type of OP compound and the timing of administration. Once “aging” occurs—an irreversible chemical modification that stabilizes the enzyme–phosphate bond—oximes become ineffective. Pralidoxime (2-PAM), the most widely used oxime, is effective against many agricultural OPs but has limited penetration into the brain. Obidoxime offers broader reactivation potential and higher efficacy against dimethyl OPs. HI-6, a newer oxime, shows enhanced CNS permeability and greater activity against nerve agents such as sarin and VX, although it remains expensive and less accessible. Comparative evaluation of oximes reveals variability in reactivation kinetics and spectrum of activity, necessitating compound-specific treatment protocols.
|
Oxime |
Chemical Type |
Spectrum of Activity |
CNS Penetration |
Remarks |
|
Pralidoxime (2-PAM) |
Pyridinium aldoxime |
Effective against diethyl OPs |
Low |
Widely available; limited CNS effect |
|
Obidoxime |
Bis-pyridinium oxime |
Broader activity (dimethyl & diethyl OPs) |
Moderate |
More potent but higher toxicity risk |
|
HI-6 |
Imidazolyl oxime |
Effective against nerve agents (sarin, VX) |
Good |
Superior efficacy; limited clinical use |
|
Trimedoxime |
Bis-pyridinium oxime |
Moderate spectrum |
Poor |
Mainly experimental |
|
RS194B |
Novel oxime derivative |
Broad OP coverage |
High |
Experimental; enhanced BBB permeability |
The use of combination therapy—typically atropine + oxime + benzodiazepine—represents a synergistic approach targeting the full spectrum of OP-induced pathophysiology. Atropine relieves muscarinic effects, oximes restore enzymatic activity, and benzodiazepines mitigate CNS hyperexcitability and prevent seizures. Diazepam and midazolam, both GABAergic agonists, reduce neuronal excitotoxicity by enhancing inhibitory neurotransmission. Clinical and experimental data demonstrate that combining oximes with atropine significantly reduces mortality compared to atropine monotherapy, while the addition of benzodiazepines further prevents long-term neurological sequelae such as OP-induced delayed neuropathy (OPIDN). This multimodal therapy not only improves survival but also limits irreversible neural damage and respiratory complications, emphasizing the necessity of early and aggressive intervention.
Despite their widespread use, current antidotes possess significant limitations. The most prominent challenge is poor blood–brain barrier (BBB) penetration, particularly for quaternary ammonium oximes like pralidoxime and obidoxime, which restricts their ability to reverse central AChE inhibition. Consequently, CNS symptoms—such as seizures, confusion, and respiratory depression—may persist even after peripheral recovery. Furthermore, the aging process of phosphorylated AChE drastically reduces the therapeutic window for oxime reactivation, especially with certain dimethyl OPs where aging can occur within minutes. Variability in the structure and lipophilicity of different OP compounds also influences oxime responsiveness, rendering some cases refractory to conventional therapy. Moreover, prolonged use of high-dose atropine may lead to complications such as hyperthermia, tachyarrhythmias, and delirium, necessitating careful titration and monitoring.
To overcome these challenges, advances in antidote research have focused on developing novel compounds with improved pharmacokinetic and pharmacodynamic properties. Bioscavenger therapy, involving the administration of exogenous enzymes that bind and neutralize OPs before they reach endogenous targets, is among the most promising innovations. Human butyrylcholinesterase (HuBChE) and engineered recombinant AChE variants act as catalytic scavengers, hydrolyzing OPs into non-toxic metabolites. Such enzyme-based antidotes can serve as both prophylactic and therapeutic agents, particularly in military and occupational exposure contexts. PEGylated and mutant AChE constructs are being investigated to extend plasma half-life and enhance resistance to inhibition.53-55
Another important advance is the exploration of centrally active oximes such as RS194B and K027, which exhibit improved lipophilicity and CNS bioavailability, thus reactivating AChE within the brain. Galantamine, a reversible AChE inhibitor and nicotinic receptor modulator, has shown neuroprotective potential by attenuating excitotoxicity and oxidative stress when co-administered with standard therapy. Research into non-oxime reactivators, such as hydroxylamine-based compounds and catalytic antibodies (so-called “bioscavenger antibodies”), is ongoing, offering future alternatives with broader spectrum and faster onset.
|
Emerging Antidote Type |
Example |
Mechanism of Action |
Advantages |
Development Stage |
|
Bioscavengers (enzyme-based) |
Human butyrylcholinesterase |
Binds and hydrolyzes OPs before AChE inhibition |
Preventive use; minimal toxicity |
Preclinical/Phase I |
|
Centrally active oximes |
RS194B, K027 |
Reactivates CNS AChE; BBB-permeable |
Superior CNS protection |
Experimental |
|
Recombinant AChE variants |
PEG-AChE, mutant HuAChE |
Catalytic degradation of OPs |
Long half-life; high catalytic rate |
Preclinical |
|
Adjunct neuroprotectors |
Galantamine, memantine |
Modulate cholinergic and NMDA systems |
Reduce oxidative damage and seizures |
Clinical trials |
In conclusion, pharmacological antidotes form the backbone of OP poisoning management, with atropine, oximes, and benzodiazepines providing the best established therapeutic combination. However, their limitations—particularly inadequate CNS protection and dependence on timing—underscore the urgent need for next-generation antidotes. Ongoing advancements in bioscavenger enzyme therapy, BBB-penetrating oximes, and multifunctional neuroprotective agents represent a paradigm shift in the treatment of OP toxicity. Future strategies integrating these innovations hold the potential not only to improve survival but also to minimize long-term neurological damage, marking a significant leap toward comprehensive and effective antidotal therapy.56-58
CONCLUSION:
Organophosphate poisoning remains a critical medical emergency and a significant cause of morbidity and mortality worldwide, particularly in agricultural and low-resource settings. The core pathophysiology lies in the irreversible inhibition of acetylcholinesterase, leading to a potentially fatal cholinergic overload. Timely diagnosis, aggressive decontamination, and early administration of pharmacological antidotes are pivotal in reducing mortality.
Among available therapies, atropine, oximes, and benzodiazepines form the foundation of treatment, each addressing different facets of the toxic cascade. Despite their effectiveness, challenges persist—especially the limited central nervous system penetration of oximes, rapid “aging” of phosphorylated enzymes, and variability in OP compound responsiveness. These limitations have driven significant research toward the development of next-generation antidotes, including bioscavenger enzymes like human butyrylcholinesterase, BBB-permeable oximes, and multifunctional neuroprotective agents.
Future advancements in pharmacological and enzyme-based therapies hold the promise of more comprehensive protection, not only by reversing peripheral toxicity but also by preventing central neurodegeneration. An integrated therapeutic approach—combining early medical intervention, improved antidotes, and supportive care—remains essential to achieving better clinical outcomes and reducing the global burden of organophosphate poisoning.
REFERENCES


Nihal Tamboli*, Suyash Suryavanshi, Shrutika Patil, Abhay Potghan, Om Wangade, Diksha Auti, A Review of Organophosphate Poisoning and the Role of Pharmacological Antidotes, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 382-400 https://doi.org/10.5281/zenodo.17519373
 10.5281/zenodo.17519373
10.5281/zenodo.17519373
