JKKMMRF’S- Annai JKK Sampoorani Ammal College of Pharmacy, B. Komarapalayam Affiliated by the Tamil Nadu Dr. MGR Medical University, Chennai.
Polycystic Ovary Syndrome (PCOS) it is Endocrine Metabolic Syndrome occur in 4– 20% of women’s in Reproductive Age and defined by Hyperandrogenism, Oligomenorrhea or Amenorrhea and Polycystic ovarian morphology. PCOS is phenotypically heterogeneous multifactorial conditions in the Predisposition to gene, Insulin resistance, Hormonal imbalance, Low grade inflammation, Environmental exposure and Psychosocial stressor. It clinical manifestation ranges are Hirsutism, Acne, Obesity and Infertility to Metabolic syndrome, Type 2 diabetes, cardiovascular disease and Affective disorders. Diagnosis very Dependent on the Rotterdam criteria in two of three of the features: Ovulatory dysfunction, Hyperandrogenism or Polycystic ovarian morphology. Pathophysiology is due to androgen excess, Hyperinsulinemia and Hypothalamic pituitary ovarian axis dysregulation. Management is through lifestyle modification like diet, Exercise and Weight loss. Pharmacological treatment comprises metformin, oral contraceptives, ovulation inducers, anti-androgens and laparoscopic ovarian drilling in patients who are resistant. New developments emphasize Inositols, Vitamin D, GLP-1 receptor agonists, Microbiome modulation and Genetic biomarkers future potential for tailored medicine.
This endocrine condition is more common in women of reproductive age. It affects 5% to 15% depending on the diagnostic criteria used. PCOS is among the most common endocrine and metabolic disorders that afflict humans globally [1]. PCOS presentation is diverse hyperandrogenism, menstrual irregularities, hirsutism, acne and alopecia [2]. PCOS displays significant individual variances, but hyperandrogenism, abnormal menstruation, and multiple ovarian cysts are characteristic signs. The first to develop this complex disease are high-risk adolescents who are likely to have other complications such as obesity, type II diabetes, infertility, endometrial dysplasia cardiovascular problems and mental health issues.[3]
Since Stein and Leventhal first characterized the syndrome characteristics more than 80 years ago, its classification has been based on Rotterdam criteria with four phenotypes, raising questions over whether women who normally ovulate or do not have hyperandrogenism should be classified as having PCOS [4].
The American gynaecologist Irving F. Stein, SR, and Michael L. Leventhal called this disorder Stein Leventhal Syndrome, which is also known as multi-cystic ovaries or schlerocystic ovaries This hormonal condition impacts women between the ages of 18 and 44 [6]. It is frequently linked to metabolic abnormalities, namely insulin resistance and compensatory hyperinsulinemia, which are acknowledged as a significant contributing factor, as well as psychological issues, such as depression and other mood disorders is charge of changing the synthesis and metabolism of androgens.[7] Obese adults and Individuals who eat fast food more frequently are more likely to develop PCOS. Consequently, exercise therapy is the mainstay of PCOS treatment. The greatest strategies to attain good control would be to limit fast food consumption and use weight-loss methods in addition to calorie-restricted meals and exercise Regarding PCOS [8]
Epidemiology:
The prevalence of eating disorders in 2000 amounted to 3.5% worldwide. For 2007 through 2012, this figure stood at 4.9%. Moreover, for the 2013-2018 period, rough ground between 7.8%. Eating disorders typically reflect distortions in aspirations, thoughts and actions in relation to food, eating and body weight [9]. PCOS can seriously damage ovaries and therefore affects metabolism in general as well as fertility, The prevalence of PCOS in the world's population is estimated at between 4 and 20%. According to figures from the World Health Organization, which were released in 2012, 116 million women worldwide–or 3.4% of all women–are on earth challenges PCOS in one form and another. The prevalence of polycystic ovarian syndrome (PCOS) is 3.7% - 22.5% in India, compared to that in other developing countries [10].
Etiology:
Polycystic Ovary Syndrome is a multi- factorial hormonal, metabolic and reproductive endocrine derangement disorder. Its etiology is not known, though some of the pathogenesis factors have been proposed by recent research work.
Genetic Factors:
PCOS is genetically and familywise positive and is linked to insulin signaling, steroidogenesis and gonadotropin regulation. DNA methylation and histone modification may be epigenetic mechanisms underlying the hereditary features of PCOS [11].
Insulin Resistance and Hyper-Insulinemia:
Most women with PCOS have Insulin resistance, elevating the level of insulin. It may cause the cells in the ovaries to secrete too much androgen, leading to hirsutism and anovulation and vulnerability to type 2 diabetes and cardiovascular disease [12].
Hormonal Imbalances:
PCOS pathophysiology a further characterised by hypothalamic- pituitary- ovarian axis dysregulation with high level of luteinizing hormone (LH) compared to follicle stimulating hormone (FSH) suppressing follicular growth and anovulation. Suppressed development of the follicles can be caused by high level of anti- Mullerian hormone (AMH) [13].
Low-Grade Inflammation:
Chronic low- grade inflammation in PCOS patients is typically linked with high pro- inflammatory cytokines that worsen insulin resistance and hyperandrogenism, impairing reproductive and metabolic well-being [14].
Environmental and Lifestyle Determinants:
Diet lifestyle and exposure to environmental toxins can influence the severity of PCOS. Obesity increases insulin resistance and androgen further more severely whereas an unhealthy diet can alter gut microbiota and hence influence endocrine equilibrium [15].
Psychosocial Determinants:
PCOS is also linked with psychiatric morbidity, i.e., depression and anxiety, otherwise exacerbated by infertility, obesity and hirsutism and hence must be addressed holistically [16].
Sign And Symptoms:
Polycystic Ovary Syndrome (PCOS) is a multi-factorial etiology endocrinopathy of female disease caused primarily by secondary hormonal imbalance with elevated androgens. The presenting symptoms initially are irregular menstruation, cysts in the ovary, hirsutism, acne, and dark skin folds (acanthosis nigricans), and headache are also common. The subsequent complications of PCOS are weight gain, metabolic syndrome, insulin resistance, and risk of type 2 diabetes development. Moreover, endocrine imbalances predispose to certain cancers, e.g., endometrial cancer, and infertility, as a result of abnormal or absence of ovulation. PCOS is also linked with sleep apnea, and chronic inflammation gives rise to most systemic and metabolic complications. PCOS should be treated for overall well-being. [17].
Athophysiology:
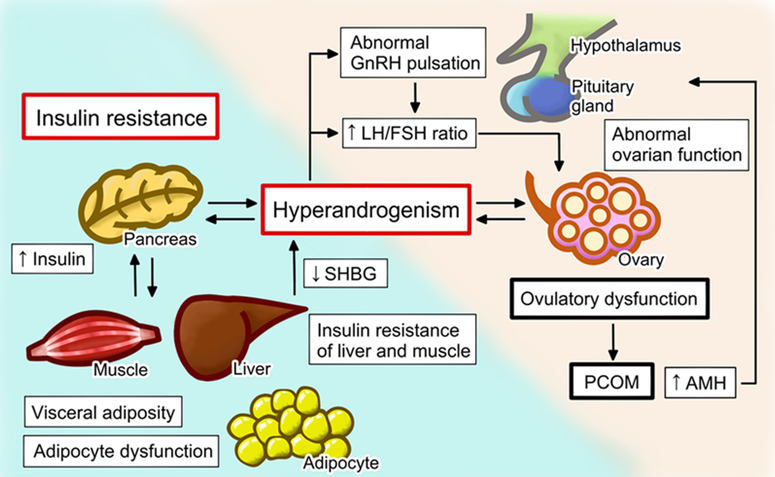
Figure.1: Pathophysiology
PCOS is an endocrine condition with multifactorial reproductive, Hormonal and Metabolic abnormalities. PCOS is defined by dysregulation of GnRH secretion leading to increased pulsatility. Low levels of progesterone may lead to a defective pattern in which the anterior pituitary overproduces LH compared to follicle-stimulating hormone.
This results in the overproduction of androgens by the cells in the ovaries. Androgens either directly or indirectly due to the peripheral conversion of androgens to dihydrotestosterone (DHT) by 5α- reductases is key factor in causation of skin features of PCOS, including Acne, Hirsutism and Androgenic alopecia [18].
Hyperandrogenism in PCOS primarily affects the pilosebaceous unit (PSU) which include the hair follicles and Sebaceous glands. Higher androgen levels stimulate the PSU. Increasing sebum production and promoting hyper keratinization. Elevated DHT levels in the PSU due to increased 5αreductase activity can worsen the effects. The hormonal environment favors acne vulgaris by causing follicular plugging and inflammation Androgen- induced follicular dynamics can lead to shortening of the hair follicle anagen phase which results in androgenic alopecia.
Hyperandrogenism in PCOS may be heightened by insulin resistance Hyperinsulinemia stimulates androgen production by exciting the ovarian theca cells and suppressing the secretion of sex hormone- binding globulin (SHBG) the liver. This increase concentration of free androgens which exert more pronounced effect on the skin Insulin resistance may lead to acanthosis nigricans a hyperpigmented velvety plaque condition seen in PCOS [19].
Diagnosis Of Polycystic Ovary Syndromes (PCOS):
The diagnosis of PCOS is largely clinical and depends upon fulfillment of some or all of the criteria. The best accepted criteria are the Rotterdam criteria which demand two or more of the following three features:
1. Clinical or biochemical hyperandrogenism: These are signs such as hirsutism, acne and alopecia or raised levels of androgens as reported by laboratory investigations.
2. Oligo-ovulation or anovulation: Irregular or missed menstrual cycles reflecting infrequent or non-ovulation.
3. Polycystic ovarian morphology (PCOM): Ultrasound scan diagnosed by the occurrence of 12 or more follicles 2–9 mm in diameter in one or more ovaries or elevated ovarian volume (>10 cm³) [20].
In teenagers, the diagnostic strategy is cautious because of pubertal physiological changes. Hyperandrogenism either clinical or biochemical and menstrual disturbance need to happen in a case of PCOS in this group [21].
Modern guidelines place a high priority on a reflective evaluation with a complete medical history, general physical examination and reflective laboratory and imaging studies. Exclusion of other conditions with a similar presentation is thyroid disease, hyperprolactinemia and non-classic congenital adrenal hyperplasia.
Metabolic Complication:
PCOS has linked in several metabolic comorbidities such as Insulin Resistance (IR), Hyperinsulinemia, Impairment of Glucose Tolerance, Type 2 Diabetes Mellitus (T2DM), Gestational Diabetes, Hypertension, Endometrial Carcinoma, Non Alcoholic Fatty Liver Disease (NAFLD), Ovarian Dysfunction, Dyslipidemias, Metabolic syndromes and cardiovascular risk enhancements [22].
Mood disorders
PCOS patients frequently have mood issues. The condition may arise as a result of numerous events, both connected and unrelated to it. The two most prevalent psychological comorbidities seen in young PCOS patients are anxiety and depression. There is also often a negative body image, psycho-sexual dysfunction, eating problems, and a lower quality of life. Since young PCOS patients are more likely to have depression at baseline and to develop depressive symptoms later on, tests such as the OGTT, fasting plasma glucose, or HbA1c should be conducted every one to three years and adjusted for other diabetic risk factors [23].
Management & Treatment:
According to the 2018 PCOS guideline, there is not enough data to conclude that any one dietary strategy has a greater positive impact on health outcomes. In accordance with general population recommendations, recommendations may adopt a range of balanced dietary strategies based on the lifestyle needs and preferences of the individual. Weight loss improves the presentation of PCOS regardless of dietary composition, according to a systematic review that compared various dietary compositions (such as low carbohydrate, low glycaemic index (GI) and glycaemic load (GL), high protein, monounsaturated fatty acid (MUFA) enriched, and fat counting diets) to best manage PCOS [24].
Aerobic workout
This is essential to cardiovascular functioning and to the increase in energy expenditure during the course of a weight-loss program. It is important to realize that an obese, unfit patient will not necessarily be able to accomplish a great deal of aerobic exercise that enhance suppleness and flexibility. Although they will not necessarily increase caloric expenditure much, they can improve morale for an exercise program, minimize risk of injury and overall enhance well-being.
Exercise for endurance
Long-term lower-intensity exercise is a suitable method for patients who are unable to handle high-intensity exercise to improve their fitness and raise their energy expenditure. Using a pedometer while walking can be a very helpful way to start increasing energy expenditure.
Training with resistance
Weight training has been overlooked as a way to improve function and body composition by increasing muscle mass and strength up until recently. Resistance training is currently thought to be a very acceptable method of influencing weight, body composition, and insulin sensitivity because of the high metabolic rate of muscle, which makes muscle mass a significant determinant of resting energy expenditure [25].
B. Pharmacological Therapy:
|
Condition |
Treatment |
Dosage |
Possible ADRS |
|
Insulin Resistance |
Metformin |
A total of 500 mg (initial dose) with increases of 500 mg within 1–2 weeks, and employing extended-release formulations may reduce side effects and improve adherence |
Nausea, flatulence, and vitamin B12 deficiency |
|
Irregular Menstrual Cycle |
Oral Contraceptives (OCPs) |
20–35 µg Low-estrogen dose OCPs (eg,Ethinylestradiol 20 µg) |
Weight gain, Venous thromboembolism, spotting and breast tenderness |
|
Hirsutism |
Cyproterone acetate (monotherapy) Ethinylestradiol (in combination) |
10 mg 20–50 µg |
Headache, breast tenderness |
|
Infertility |
Clomiphene citrate, Letrozol |
Clomiphene citrate: 50–150 mg for 5 days; Letrozole: 2.5–5 mg/day (days 3–7 of menstrual cycle) |
Nausea and mood changes Multiple pregnancies; hot flashes |
|
Hyperandrogenism |
Spironolactone, Flutamide, Finasteride |
Spironolactone: 25–100 mg Flutamide: 500 mg + OCP |
Spironolactone: fatigue, irregular cycle (at high doses), hyperkalemia Finasteride: hepatotoxicity Flutamide: hepatotoxicity |
|
Obesity |
Pioglitazone, GLP-1-agonists, Orlistat |
Pioglitazone: 15–30 mg/daily; GLP-1-agonists: Semaglutide 0.25−1 mg once weekly; Liraglutide 0.6–1.8 mg once daily, Orlistat 120 mg twice a day |
Pioglitazone: mild peripheral edema and muscle cramping; GLP-1-agonists: gastrointestinal symptoms (nausea, diarrhea, vomiting, constipation, abdominal pain, or dyspepsia); Orlistat: increased bowel movement, oily stool, oily spotting, stomach pain and some cases of liver injury [26] |
Metformin
Because it enhances ovulation, insulin sensitivity, and potentially hyperandrogenism, metformin has gained popularity as a therapy [23].
It is frequently used, either by itself or in conjunction with clomiphene-citrate, to treat infertility. Since it causes some women to ovulate more frequently, it can also raise the, frequency of endometrial shedding and could aid in the regulation of the cycle. The long-term effects of treating insulin resistance in women with normal glucose levels with metformin are unknown. Metformin reduces the progression of poor glucose tolerance to type 2 diabetes in different groups. Therefore, women with polycystic ovarian syndrome and hyperglycemia may benefit from taking metformin. Whether or not administer this medication should be decided individually. Contraception should be recommended to those who do not want to get pregnant [27].
Infertility Management:
Menstrual irregularities (such as oligomenorrhea, amenorrhea, and anovulatory cycles) can result from hormonal abnormalities in women with PCOS (such as high androgen levels), which can induce dysfunctional uterine hemorrhage and inability to conceive. The ovulatory disruption in PCOS women may result in infertility and unfavorable pregnancy outcomes. PCOS-related infertility is treated with dietary, behavioral, and exercise modifications.
Letrozole should be regarded as a first-line pharmaceutical treatment for ovulation induction in PCOS women, as should pharmaceutical therapies (oral agents like rosiglitazone, clomiphene citrate either alone or in combination, letrozole, or metformin, or injectable agents like gonadotrophins), surgical therapies (laparoscopic ovarian surgery), or in vitro fertilization (IVF) [28].
C. Non-Pharmacological/ Procedural:
HIRSUTISM:
Management in hirsute PCOS females is identical to non-PCOS hirsute females. Non-pharmacological management is removal of hair by bleaching, plucking, waxing, depilatory creams, electrolysis, thermolysis and laser.
Drug therapy involves:
First-line: Spironolactone, metformin and eflornithine topical in facial hirsutism.
Oral contraceptives: Especially low-androgenic progestins (norgestimate, desogestrel, drospirenone) with inhibition of hair growth.
Other drugs: Flutamide and finasteride are potent but to be administered during pregnancy with caution.
Combinations: Oral contraceptives and spironolactone will be effective but raise potassium. Spironolactone is more potent than finasteride, and spironolactone and rosiglitazone will be more potent than metformin. Evidence for metformin is mixed—some trials show benefit; others show little effect. Facial hair is managed with topical eflornithine cream, which is FDA-approved, and perhaps with sibutramine (an anti-obesity drug). [29]
Treatments for Hirsutism
In PCOS-afflicted women are akin to those for patients of idiopathic hirsutism, who are not PCOS victims. There are numerous nonpharmacologic treatment alternatives, such as electrolysis, waxing, bleaching, plucking, depilatory creams (whereby one dissolves the hair), thermolysis (use of heat) as well as laser therapy. Various medications have been investigated for management of hirsutism in PCOS-affected women. The medications spironolactone and contraceptive oral drugs may be combined, but with drospirenone there must be a care since the two medications can lead to the hyperkalemia. Metformin, rosiglitazone (Avandia) and acarbose (Precose) are all insulin- sensitizing drugs for the treatment of hirsutism in PCOS women. Ferriman-Gallwey scores of hirsutism have shown that rosiglitazone and spirolactone are superior to metformin. Even though flutamide (formerly Eulexin) and finasteride (Propecia) are FDA pregnancy categories X and D, respectively and work, both are off-label when prescribed for hirsutism. Spironolactone is better than finasteride according to a Cochrane review.
The drugs oral contraceptives and spironolactone can be combined together, but in the patients on drospirenone one needs to be a cautious because both of these are medications can cause hyperkalemia. Metformin, rosiglitazone (Avandia) and acarbose (Precose) are the insulin- sensitising medication used to treat hirsutism in PCOS women are metformin, rosiglitazone (Avandia) and acarbose (Precose). Ferriman-Gallwey scores for hirsutism have revealed that rosiglitazone and spirolactone are superior to metformin. According to a Cochrane review, that for treatment of hirsutism in PCOS women, metformin is as effective as oral contraceptives; however, in a recent systematic review, it was observed that metformin is ineffective. One Topical eflornithine cream has been approved by the FDA for the treatment of unwanted facial hair, particularly in PCOS patients. Sibutramine (Meridia), a prescription antiobesity medication, also decreases hirsutism.
Surgical Treatments In PCOS:
The principal surgical treatment available is laparoscopic ovarian drilling (LOD) which is intended to correct ovulation by lowering ovarian androgen production.
1. Laparoscopic Ovarian Drilling (LOD)
LOD entails the movement of a laser or electrosurgical needle through the ovarian capsule, decreasing cyst numbers and reducing androgen concentrations. Systematic review and meta-analysis in 2025 contrasted unilateral LOD (ULOD) and bilateral LOD (BLOD) in terms of improving fertility outcomes. The research outcome showed that ULOD had fewer chances of complications such as scarring of the ovaries and premature ovarian failure but had satisfactory fertility outcomes [30].
2. Ovarian Wedge Resection
Once a common operation, wedge resection of the ovary is now performed fairly infrequently due to its tendency to cause postoperative adhesions and the availability of less dangerous alternatives.
3. Bariatric Surgery
In overweight or obese women with PCOS, bariatric surgery has been demonstrated to enhance insulin sensitivity, reduce testosterone, and normalize ovulation. It is generally reserved for patients, however, in whom lifestyle modifications and pharmacologic treatments have failed [31].
4. Emerging Research
A 2023 review pointed out that surgery could be a safe and efficient method of treatment for drug-resistant PCOS, especially in women intending to conceive. The review added decreased levels of LH and AMH after surgery, reflecting an improved balance of hormones [32].
Recent Advances & Future Direction:
1. Inositols
Myo-Inositol (MI) and D-Chiro-inositol (DCI) is insulin sensitisers and have ovarian physiology effects. Meta-analyses indicate MI ± DCI enhances insulin resistance, menstrual cyclicity, and certain ovarian outcomes in PCOS women. Myo-inositol pretreatment in IVF augmented mature oocyte rates but live birth outcomes are unclear. Dosage is typically 2–4 g/day; side effects are minimal GI symptoms. Overall, inositols are safe addition therapy, but evidence is heterogenous [33].
2. Vitamin D Supplementation
Vitamin D deficiency is common in PCOS. Supplementation lowers inflammatory biomarkers (e.g., hs-CRP) can improve glucose and lipid metabolism. Modest benefits are reported by meta-analyses but inconsistent dosing regimens and heterogeneity between trials moderate the conclusion [34][35]. Correcting deficiency is acceptable, but clinical endpoints such as fertility are in doubt.
3. GLP-1 Receptor Agonists
GLP-1 RAs (liraglutide, semaglutide) lead to weight loss and enhanced insulin sensitivity, addressing specifically PCOS metabolic derangement. Clinical trials report significant weight loss and increased menstrual cyclicity and androgen, although big RCTs by fertility indications are awaited [36]. GI-associated adverse effects frequent; pregnancy is a contraindication. Possibly valuable in obese PCOS but off-label in most indications present at the moment.
4. Genetics & Molecular Biomarkers
GWAS and molecular research find several loci associated with PCOS, namely genes controlling insulin and gonadotropin pathways. Predictive ability is still moderate. Reviews invoke promise for personalized treatment through multi-omic integration (hormones, microRNAs, metabolites) but no common biomarkers yet progressed to clinical practice [37].
5. Gut Microbiome Modulation
PCOS is linked with gut dysbiosis — decreased diversity and changing taxa (e.g., ↓Akkermansia, ↑Bacteroides/Escherichia). Small RCTs and animal models indicate that probiotics, prebiotics, or synbiotics correct insulin resistance and inflammation [38]. Mechanisms are robust but microbiome-directed interventions are experimental and need larger human trials.
CONCLUSION:
PCOS is complex endocrine- metabolic disease that affects the Female Reproductive Tract, Metabolic system and Moods. Its etiology is a multifactorial, Involving genetic, Hormonal, Metabolic, Inflammatory and Environmental factors, Rendering diagnosis according to the Rotterdam criteria problematic. Successful treatment demands tailored, Multi- Disciplinary strategies with primacy of lifestyle therapy— diet, physical exercise and weight reduction and drug treatment with metformin and oral contraceptives. New treatments such as inositol therapy and genetic assessment augment personalized care. Current studies strive to optimize diagnostic precision and comprehensive treatment for improved outcomes in women with PCOS.
ACKNOWLEDGEMENT:
The authors are thankful to Department of Pharmacy Practice, JKKMMRF’s Annai JKK Sampoorani Ammal College of Pharmacy, Affiliated to Tamil Nadu Dr.M.G.R. Medical University, Chennai, Tamil Nadu, India.
REFERENCES


Archana B.*, Kiruthiga O. B., Mahalakshmi M., Arul Prakasam K. C., Polycystic Ovary Syndrome: A Comprehensive Review of Pathophysiology, Diagnosis, And Emerging Therapeutic Strategies, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 238-250 https://doi.org/10.5281/zenodo.17510878
 10.5281/zenodo.17510878
10.5281/zenodo.17510878
