Rashtriya College of Pharmacy Hatnoor, Kannad, Chh. Sambhajinagar 431103
Pediatric epilepsy is one of the most common chronic neurological disorders in children, characterized by recurrent, unprovoked seizures resulting from abnormal electrical activity in the brain. Early and accurate diagnosis is essential to differentiate epileptic seizures from other paroxysmal events and to identify underlying etiologies such as genetic, structural, metabolic, or infection causes. A comprehensive evaluation includes detailed clinical history, neuroimaging, electroencephalography [EEG], and, when indicated, genetic testing. Treatment primarily aims to achieve complete seizure control with minimal adverse effects while optimizing the child’s neurodevelopmental outcomes and quality of life. Management involves a multidisciplinary approach integrating pharmacological therapy mainly antiepileptic drugs [AEDs] with dietary intervention such as the ketogenic diet, surgical option for drug-resistant epilepsy, and neurostimulation techniques. Additionally, psychological, educational, and social support are vital components of long-term care. Recent advances in precision medicine, novel antiseizure medications, and neuroimaging have significantly improved outcomes for many children with epilepsy. Continued research and individualized management remain key to enhancing prognosis and overall quality of life in pediatric epilepsy.
Pediatric epilepsy is one of the most common chronic neurological disorders affecting children worldwide. It estimated that around 50 million people globally live with epilepsy, and nearly 10 million of them are children under the age of 15. Every year, approximately 4 to 6 out of every 1,000 children are diagnosed with epilepsy. It is characterized by recurrent, unprovoked seizures caused by abnormal electrical activity in the developing brain. In this not only affect brain but the overall life of a child and family.
Research shows that around 80% of children with epilepsy live in low- and middle- income countries, where early diagnosis and treatment are still a challenge. India has the highest number of affected children, mainly because of its huge population and small towns. China also has close to a million children living with epilepsy, in African countries like Nigeria, Ethiopia and other Sub-Saharan regions, the situation is even more challenging. It estimated that over two million children there suffer from epilepsy, often due to infection like malaria, meningitis or birth complications, which damage the brain in early life. On other hand, developed counties such as the United States have around 470,000 children diagnosed with epilepsy, but most of them receive early treatment, regular follow-up and support systems that help them lead a better quality of life.
RISK FACTORS
Risk factor of epilepsy is higher in preterm populations due to white matter gliosis, hypoxic-ischemic brain damage, hippocampal sclerosis, decreased brain structure development, and increased infection risk in preterm populations. Eclampsia is a significant condition that can progress to epilepsy in young people via a variety of paths. In reality women may suffer hypoxia, which can increase the incidence of epilepsy and interfere with the unborn brain’s normal growth[2]. Other major factor is a positive family history are linked to genetic mutations and inherited syndromes such as Dravet syndrome. Even children whose birth weight falls within the normal range are at heightened risk for epilepsy due to intrauterine growth restriction[3].
The following are some of the risk factors that might increase the risk of epilepsy[4].
Figure 1: Epilepsy risk factors.
People with epilepsy are unable to lead normal lives because of the stigma associated with the condition. The economic burden of epilepsy is very high. The dual burden of learning disability, cognitive impairment, and subpar academic achievement is common in children with epilepsy. Perinatal insults such as metabolic derangement, and central nervous system [CNS] infections are important modifiable risk factors of epilepsy. Regretfully, there is a dearth of information from India regarding the risk factors for childhood epilepsy. There are several methodological limitations for epidemiological studies on epilepsy in developing countries[5]. Childhood epilepsy may be predisposed by perinatal causes. But the observations in epidemiological studies had been rather negative or conflicting[6]. There was no correlation found between prenatal insult and childhood epilepsy in a door-to-door survey conducted in West Bengal, however another comparable study in Kerala state supported an association between the two. The first step towards preventing epilepsy in children would be to identify such risk factors, according to a population-based survey conducted in Kerala's Northern district.
EPIDEMIOLOGY
In epidemiological research on childhood epilepsy, the exclusion of children aged<6 years, because febrile seizures are common in this age-group and would confound estimates. In studies presenting sub analyses by age-group, as expected, prevalence of epilepsy increased with age, while incidence decreased with age and the highest incidence was in the 0- to 5-year age-group[7,8].
Active prevalence of epilepsy is a measure of the proportion of patient currently suffering from active epilepsy or experiencing the consequences of epilepsy as measured by taking anticonvulsant medication[9].
TABLE 1: AGE SPECIFIC INCIDENCE RATES [ROCHESTER, MINNESOTA, 1935-1979]
|
Age group [years] |
No. patients |
Rate/ 100,000 Person-years |
Proportion |
|
Male/ female [%] |
|
Idiopathic[%] |
Partial [%] |
||||
|
<1 |
41 |
121 |
54 |
17 |
120 |
|
1-4 |
85 |
63 |
81 |
28 |
97 |
|
5-14 |
129 |
44 |
84 |
47 |
123 |
Since one need only to identify existing cases of the illness, prevalence studies are considerably easier to conduct that incidence studies. Prevalence studies have been performed across numerous populations varying by geographic area, race, and socioeconomic status. From an epidemiology standpoint, prevalence is of value chiefly as it is a reflection of cumulative incidence. Since prevalence represents the complex interaction, as a rule, is of limited value for the generation of hypotheses concerning etiology.
The estimated prevalence of epilepsy varies widely in reported studies by a factor of 20, and ranges from a low of 2/1,000 in the Marianas Islands to a high of 37/1,0000 in Nigeria[10]. Unfortunately, the variation seems more related to study methodology and to definition of epilepsy in individual studies based upon incidence cohorts, prevalence tends to increase with advancing age through early childhood, only to stabilize in the teenage and young adult years.
CLASSIFICATION
Classification of seizure type-expanded version[11]:
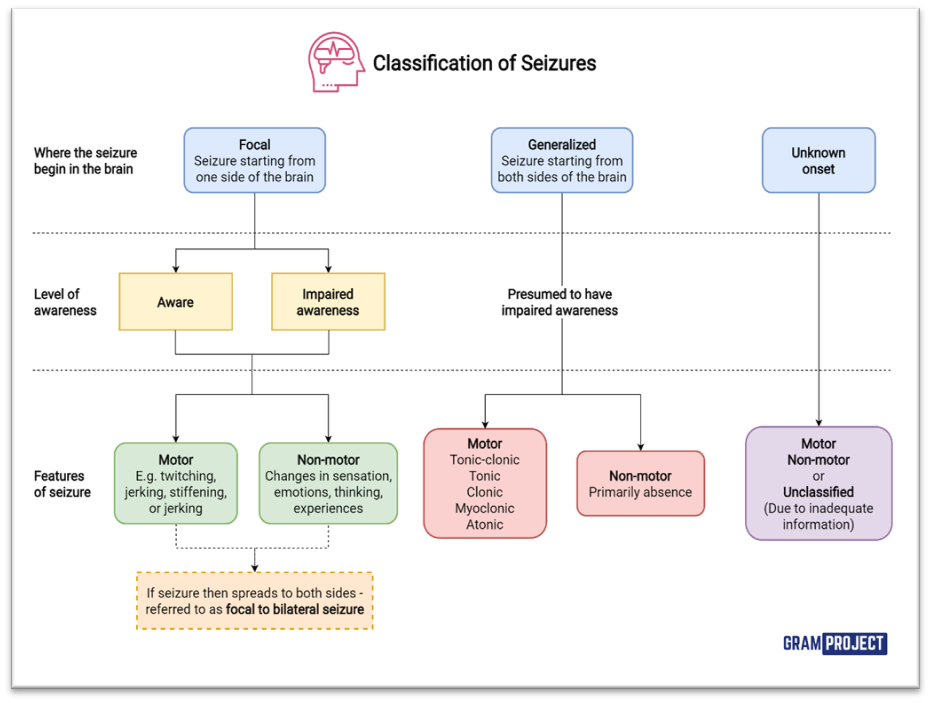
Fig 2: classification of seizures.
CLINICAL PRESENTATION
Definition:
A seizure (ictus) represents transient neurological manifestation because of abnormal, excessive neuronal discharges originating from the cerebral cortex. This discharge can result in many different neurological manifestations according to the seizure origin and spread (for example sensory, motor, somatosensory, psychic).
A convulsion refers to a seizure with motor manifestations, usually generalized tonic clonic. A “fit” is a term that should not be used as it may imply a psychogenic etiology. Epilepsy (to be attacked in Greek) is recurrent (2 or more) unprovoked seizures. Transient provoked seizures caused by fever, illness, electrolyte imbalance, toxic exposure, or head injury, are not classified as epilepsy[12].
Seizure is a paroxysmal involuntary disturbance of brain function that may manifest as:
Fig 3: Seizure symptoms.
Convulsion is generalized seizure with increased tone and tonic–clonic movements of the body.
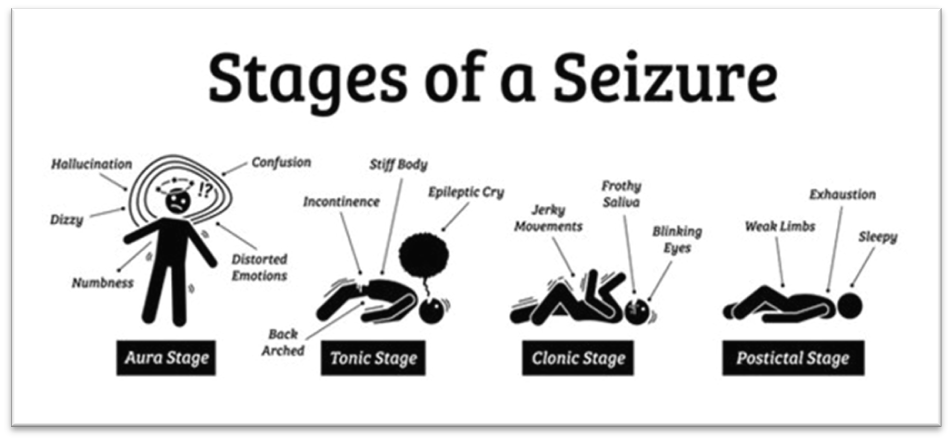
Fig 4: Stages of a seizure.
GTCS – [Generalized Tonic – Clonic Seizures]
Duration- seconds to hours.
Etiology
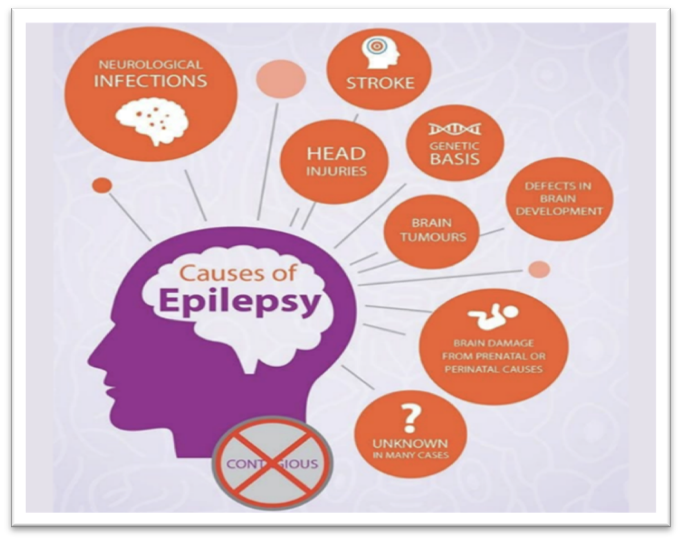
Fig 5: Causes of epilepsy.
DIAGNOSIS
The most challenging condition, which happens to be treated during an emergency, is the status epilepticus. Because of this, diagnosis and treatment section are focused on the clinical state.
Clinical presentation in status epilepticus varies. It depends on the type of seizures, stage, and previous state conditions of the pediatric patient. Diagnosis is based on the identification of continuous or recurrent seizures, and it is easy to recognize during the clinical manifestation[14].
After persisting status epilepticus, despite disappearance of motor manifestation, it is difficult to exclude non-epilepticus continuous status.
A complete instrumental evaluation can be requested in case of first clinical presentation of SE, or in case of complicated SE, comorbidity, and in infants.
Laboratory test, neurological exams, and EEG imaging methods are all necessary for epilepsy and seizures[15].
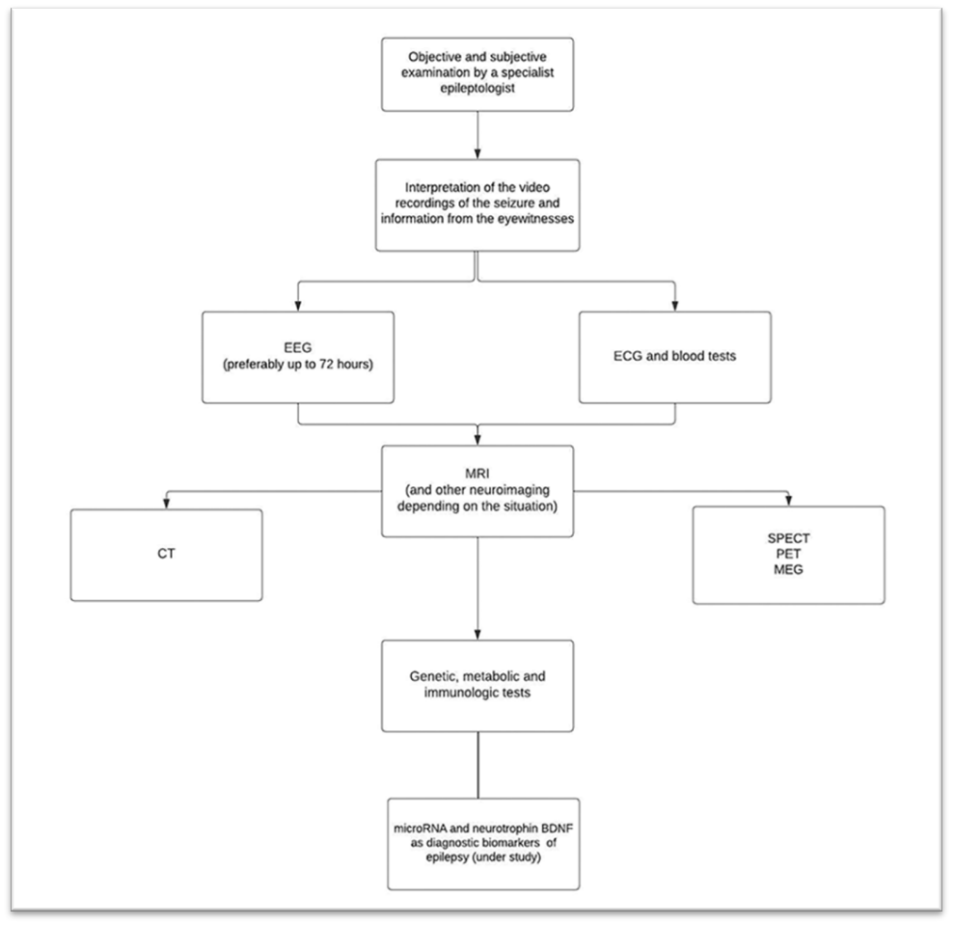
Fig 6: Diagnostic Procedure of epilepsy [16]
A healthcare provider will diagnose epilepsy in children after examination and testing that may include:
Tests help your healthcare provider understand what caused your child’s seizures and rule out conditions that cause them. An epilepsy diagnosis may take time and it usually doesn’t happen overnight[17].
TREATMENT:
Non pharmacological treatment
First Aid
Helping the patient manage the situation an epileptic seizure is known as first aid treatment. Because of the common misconception, people appear afraid when they witness someone having an epileptic seizure. Since studies have shown that patients and their families can easily control or manage epileptic seizures with the correct guidance and training, it is more important that’s ever to stay calm and help the sufferer. Since epileptic seizures are not emergencies, there is no need to call for ambulance. Consequently, the best way to help patients manage their seizures on their own and boost their confidence is through self-management training[18].
Ketogenic Diet
Throughout history, diets have been used to manage seizures. However, it was the first documented in the early 1920s, the nutritional diet was used as a therapeutic treatment for epilepsy. Dietary treatments for DRE include Low Glycemic Index Therapy (LGIT), Modified Atkins diet (MAD), and the traditional Ketogenic Diet (KD).[19] KD and MAD diets are high in fat, but LGIT focuses mostly on consuming low- glycemic foods that are low in carbohydrates. These diets compositions are explained below. A diet consisting of 90% fat, 7%protein, and 3% carbohydrates is the traditional ketogenic diet, that produces metabolic changes associated with the starvation state. A ketogenic diet, sometimes known as the keto diet, may be an option for certain kids to manage their seizures if medicine isn’t enough[20].
Diet vs MAD Ketogenic
Both RCTs compared KD with MAD. One RCT found higher rates of seizures freedom with KD than with MAD at 3 months (53% vs 25%). For seizure frequency reduction, the same RCT [21] reported an advantage of KD over MAD at both 3 months (58% vs7%) and 6 months (71%vs 28%), and the other RCT reported statistically nonsignificant results in the same direction (81% vs 54% at 3 months and 100%vs 60% at 6 moths)[22].
Neurostimulation
This treatment involves the nervous system receiving tiny electric currents via a gadget. Three forms of neurostimulation are now used to treat epilepsy they are; vagus nerve stimulation, Responsive neurostimulation, Deep brain stimulation[23].
Pharmacological Treatment
There are already more than 20 antiepileptic drugs (AEDs) on the market, and choosing the appropriate medication mostly depends on the type of seizure and the patient's age. The first-line accepted treatment is AED therapy[24], both for symptomatic myoclonic seizures and generalized tonic-clonic seizures were best administrated with sodium valproate. Primary first-line therapies for complex partial seizures were carbamazepine and oxcarbazepine, with valproate also being recommended[25]. Although using AEDs alone or in combination, approximately 20% of children with epilepsy will still have seizures[26].
The main pharmacological agents, often used first, are carbamazepine, valproic acid, oxcarbazepine and phenytoin. Other drugs used in the treatment of epilepsy are vigabatrin, lamotrigine, felbamate, gabapentin levetiracetam, ethosuximide[27,28]. The mechanisms of action of these drugs are summarized in Table 2.
Table 2. Mechanisms of action of antiepileptic drugs[29,30].
|
Drug |
Mechanism of action |
|
Phenytoin |
Inhibition of intracellular sodium currents. Reduces the influx of calcium ions into the cell. Inhibition of motor cortex and subcortical centres responsible for the tonic phase of convulsion. |
|
Carbamazepine |
Blocks potential-dependent sodium channels and secondary reduction of glutamate release and catecholamine metabolism in the central nervous system. Stabilization of the membrane of over-excite nerve fibers. |
|
Lamotrigine |
Inhibits sodium channels and blocks release of excitatory amino acids [glutamic acid]. |
|
Oxcarbazepine |
Blocks potential-dependent sodium channels. Stabilizes over-excited nerve fiber membranes. Inhibits repetitive neuronal discharges. Reduces synaptic transmission of excitatory stimuli. |
|
Topiramate |
Blocks membrane voltage-dependent sodium channels, increases gamma-aminobutyric acid activity, and shows antagonism to the receptor for glutamic acid. |
|
Gabapentin |
Inhibits voltage-gated calcium channels. |
|
Pregabalin |
Binds to an auxiliary subunit [ of the membrane voltage-shifted calcium channel in the central nervous system. |
|
Levetiracetam |
Affects protein concentrations in neurons by partially inhibiting N-type calcium currents and reducing the release of calcium ions stored inside neurons. |
|
Vigabatrin |
Selective, irreversible inhibitors of y-aminobutyric acid aminotransferase [GABA-T]. |
|
Felbamate |
Demonstrates GABA inhibitory activity and benzodiazepine receptor binding. |
|
Lacosamide |
Attenuation of low-threshold T-type calcium currents in thalamic nerve cells. |
|
Ethosuximide |
Bloking of T-type calcium channel, inhibitory effect on thalamic neurons. |
|
Eptoin |
Eptoin tablet contain the active ingredient is phenytoin, which works primarily by blocking voltage-gated sodium channels in nerve cells. This action helps to control and prevent seizures. |

Fig 6: Eptoin tablet.
Surgical treatment of epilepsy
If drug-resistant epilepsy (DRE) is diagnosed, surgery is diagnosed, surgery is an alternative to pharmacotherapy. Studies have shown the positive impact of early surgical intervention on cognitive function and thus, further intellectual development in pediatric patients[31]. Depending on the etiology of the seizures, resection, separation, or neurostimulation procedures are used.
Pediatric Epilepsy Surgeries:
Fig 7: laser interstation thermal therapy (LITT) is a minimally invasive surgical option for pediatric epilepsy where a laser is used to destroy the specific brain tissue causing seizures.
Gene Therapy:
One of the most rapidly developing methods of pharmacological therapy for treating diseases; drugs currently in the laboratory phase. Gene therapy involves placing foreign genetic material into a patient cell, resulting in one of 3 options: inhibiting production, of the gene, increasing production of the gene, or modifying the site of the gene[33].
One of the newer possible therapeutic options now is the treatment of loco-resistant epilepsy with cannabinoids (CBD), derived from the cannabis plant[34].
In 2018, CBD was approved for use by the united-states food and drug administration for treating Dravet syndrome and Lennox-Gastaut syndrome in patients aged two years and over[35].
Management Of Drug -Resistant Epilepsy
The prevalence of DRE among epilepsy patients was 30% in a recent study and the pooled incidence was 15%. Numerous research have clarified the risk factors for developing drug-resistant epilepsy. Age at onset, symptomatic epilepsy, abnormal neuroimaging findings, abnormal electroencephalography results, history of mental retardation, neuropsychiatric disorders, febrile seizures, and status epilepticus increased risk for DRE[36].
Risk Factors
DRE has already been associated with the occurrence of neuropsychiatric disorders cerebral impairment, a history of protracted febrile seizures, and particular electroencephalogram (EEG) abnormalities. DRE has been associated with the age at the epilepsy start (one year), the etiology, abnormal neuroimaging, the presence of these abnormalities, and the coexistence of these conditions[37].
Pathogenesis
Drug resistance etiology is likely diverse and complicated[38]. The hypothesized drug resistance pathways, which also include genetic and disease-related ones, may be interrelated.
The transporter hypothesis states that independent of the site of such an ASMs action increased multi drug efflux protein expression or function decreases the efficacy of ASMs in human epileptic brain tissue and DRE animal studies[39].
According to the pharmacokinetic theory, efflux transporter over expression is concentrated in decreasing the dose of ASM that is capable of permeating the BBB most likely in peripheral organs like the liver, colon, and kidneys[40].
MANAGEMENT OF EPILEPSY
Data on childhood-epilepsy management in Kenya is limited. The low rate of epilepsy diagnosis and the treatment gap are both influenced by culturally motivated health-seeking behaviours. In Kenya, the proportion of individuals with active epilepsy who lack access to appropriate medical care is known as the "treatment gap," and it is quite high. The selection of the first antiepileptic medication is affected by a combination of patient- specific and AED-Specific factors[41].
Long term AED treatment should be started after second seizure[42]. Complete seizure control without serious side effects is the goal of treatment. Complete seizure control without serious side effects is the goal of treatment. AED is based on the predominant seizer type or syndrome type with possible adverse effect and co-morbidities taken into account[42,43]. All drugs are started in low doses and increased gradually up to a maximum does till seizure control is achieved or side effects appears. Dosage needs to be adjusted to the child’s daily activity. Extended releases formulations in twice a day dosing are preferable[44].
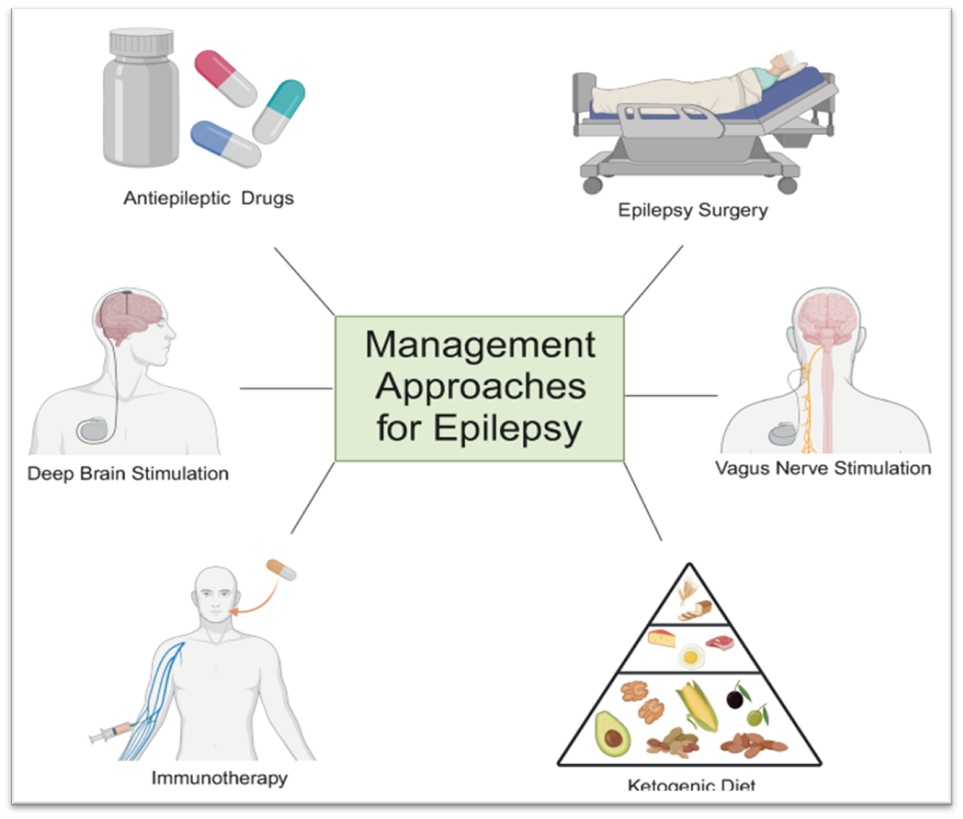
Fig 7: Management approaches for epilepsy[45].
AED choice may be influenced by seizure frequency and severity in addition to seizure type. For example, between two equally affective AEDs, a patient with daily, prolonged generalized tonic-clonic seizures may be started on the AED than can be titrated more swiftly to a therapeutic dose. Lastly, while some AED efficacy results in children parallel those in adults[46], this comparison may not apply to all pediatric epilepsy patients[47], and individualized medication selection is vital to success.
Objective self-management challenge facing adults with epilepsy include limited understanding of the condition and treatment, associated psychosocial issues, and lack of community integration. Self-management interventions improve patients medical, life role, and emotional management[48]. Epilepsy has a significant and well-researched psychosocial impact on the affected individual and their family. Interventions such as educational programs and lifestyle management education to improve self-mastery and quality of life in people with epilepsy are not necessarily integrated in standard care practices[49].
Acute and emergency management
Chronic management
FUTURE DIRECTION
The percentage of childhood-onset epilepsies that are resistant to therapy has essentially stayed constant despite significant recent advancements in our understanding of the aetiology of epilepsy and the introduction of several novel AEDs. To address this issue, there is a clear need for a more stratified approach to treatment. Traditionally, stratification has been by broad seizure type (focal or generalized), and only occasionally by epilepsy syndrome[50].
The challenges for the future will be to use this information not only for diagnosis he development of rational treatments. Gene therapy is clearly an important long-term approach, but in the meantime an understanding of epileptogenic mechanisms arising from gene mutations could provide “downstream” targets for therapy developmentIn order to screen new treatments, mouse models will be crucial. For acquired epilepsies, many potential mechanisms have also been found. Understanding which of these are necessary and sufficient to produce epilepsy should lead to intervention that will stop the development and progression of these seizure disorders[51].
Some manufactures, such as Medtronic, have newer technology that can apply electricity to the brain, but also record it, a process Dr. conner described as similar to a thermostat."It senses the situation and modifies the delivery of electricity."I think that the technology is still in its infancy, but we’re getting there,” he said. “this’s brain sensing” will help improve how effective DBS is at treating epilepsy and make it easier for physicians to program[52].
New techniques target neural networks
Thalamic responsive neurostimulation (RNS) is one of the most recent surgical techniques for treating paediatric epilepsy. This robotic-assisted procedure involves implanting a small RNS device in the thalamus-a major control center for the brain. The device continually monitors a patient’s brain waves and delivers a tiny electrical impulse to stop seizures in their tracks. The goal is to modulate a whole network of different parts of the brain that are communicating in an abnormal way to ignite a seizure[53].
Thalamic RNA offers a much-needed treatment option for children with multifocal seizures who do not respond to medication or diet therapy. Then the many patients see more that a 90% reduction in seizures[54].
CONCLUSION
Seizure in children are a serious medical issue that has to be diagnosed and treated quickly. Finding the underlying cause of the seizures requires an understanding of the several etiologies, which range from neurological problems to metabolic issues. Children’s risk of seizures is further influenced by risk variables such age, genetic predisposition, and prior neurological history. Treatment choices depend on an accurate diagnosis, which frequently requires imaging, laboratory testing, and clinical examination. The main goal of treatment to manage seizures and stop them from happening again by using medicine, changing one’s lifestyle, and occasionally having surgery.
REFERENCES



Sangram Nagargoje, Vaishnavi Rodge, Pratiksha Pawar, A Review by Paediatric Epilepsy: A Comprehensive Overview of Diagnosis, Treatment and Management, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 349-364. https://doi.org/10.5281/zenodo.17793261
 10.5281/zenodo.17793261
10.5281/zenodo.17793261
