1,3V. P. College of Pharmacy, Madhkhol, Sawantwadi, Maharashtra, India416510.
2College of pharmacy (Poly) Akluj, Solapur, Maharashtra, India 413101.
4Anandi pharmacy college kalambe, Kolhapur, Maharashtra, 416204.
5S.B. Patil College of Pharmacy, Vangali, Indapur, Pune, Maharashtra, India413106.
6DKSS’s Institute of Pharmaceutical Science & Research (for Girls), Swami-Chincholi, Pune, Maharashtra, India 413130.
7Chetana College of Pharmacy, Sardewadi, Indapur, Pune, Maharashtra, India 413130.
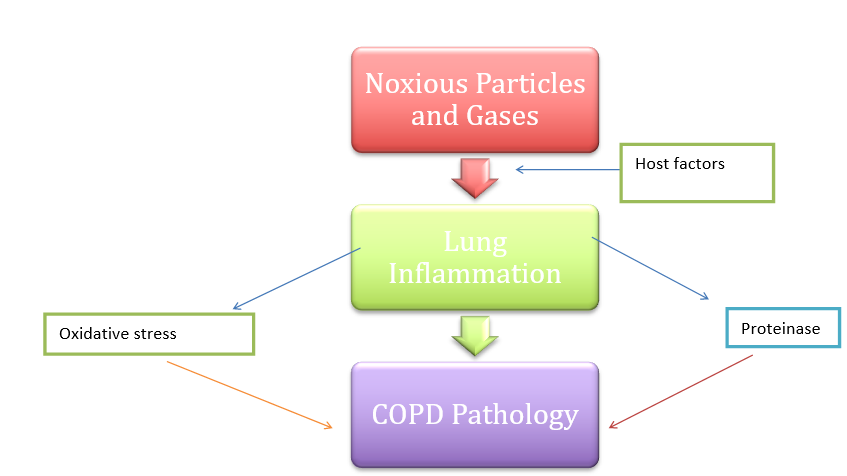
For being one of the major causes of morbidity and mortality globally and a growing health concern, our understanding of the pathophysiology of chronic obstructive pulmonary disease (COPD) has significantly expanded in recent years. The illness is brought on by interplay between environmental exposures to harmful substances, such as cigarette smoking, occupational dust, air pollution, and childhood illnesses, and personal risk factors, such as enzyme deficiencies. Emphysema, luminal blockage with mucus secretions, and permanent constriction of small airways are the main factors that may lead to airflow limitation in COPD. COPD is currently seen as a complicated, systemic disease that is marked by a persistent inflammatory process in the pulmonary tissue, which differs from bronchial asthma in pattern and is linked to extrapulmonary consequences. One of the most public health problems impacting people 40 years of age or older is COPD. By 2020, it is expected to become the third most prevalent cause of deaths worldwide, increasing from its current ranking of fourth.
The third most common cause of death in the world and an important public health issue is chronic obstructive pulmonary disease (COPD). Long-term exposure to tobacco smoking and/or inhaling harmful particles and gases from indoor, outdoor, or occupational air pollution are the main causes of chronic obstructive pulmonary disease, a generally progressive illness [1–4]. The ensuing persistent inflammation causes alveolar damage (emphysema) and airway constriction, which can be characterized by chronic bronchitis and bronchiolitis [4]. Predisposing variables, such as faulty lung development, an elevated inflammatory response to chronic irritants, or higher susceptibility to bacterial or viral infections, can raise an individual's risk of developing COPD or the rate at which the disease progresses [4, 5]. Breathing difficulties, coughing, and the generation of sputum are the main respiratory symptoms of chronic obstructive pulmonary disease (COPD), a chronic respiratory illness marked by a slow decline in lung function. As a result, COPD has a high cost caused by hospitalization absence from work, and disability. [6] Due to current data, the mortality rate from COPD is rising, and it is expected to rank as the third most common cause of death globally by 2020. [7]. In most developed and underdeveloped countries, chronic obstructive pulmonary disease (COPD) maintains to be an important cause of diseases and mortality. [8]. Poor lung development, low lung growth in early life, lung damage from cigarette smoke exposure, air pollution, infections, and airway reshaping are many the other important pathophysiological processes which contribute to this diverse syndrome. [9]
WHAT IS COPD?
COPD is an obstructive airway disease that increases in age and is unable to totally cured. It occurs by disorders of the parenchyma and airways, such as emphysema and chronic bronchitis [10]
A group of lung diseases which are called chronic obstructive pulmonary disease, or COPD, make it difficult for air to leave the lungs due to restricted airways.
Chronic = it’s a long-term condition and does not go away
Obstructive = your airways are narrowed, so it’s harder to breathe out quickly and air gets trapped in your chest
Pulmonary = it affects your lungs
Disease = it’s a medical condition [11]
HISTROY:
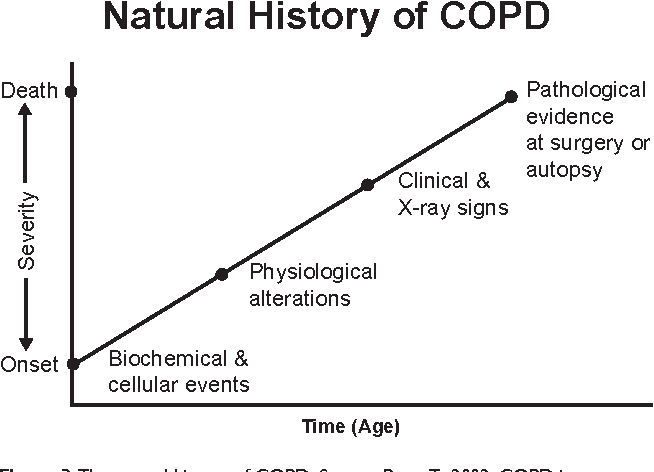
Complex biochemical and cellular processes in the small airways and surrounding alveoli are the first steps in the natural history of COPD. Elastic recoil is lost early in the process due to structural degradation [12,13]. The FVC rises as the lungs start to get bigger [13]. Simple spirometry can easily identify the early physiologic changes that come from this [14]. COPD is frequently in a moderate to advanced stage by the time clinical symptoms appear [15]. CT scans and resectional material, such as when isolated nodules are excised, can provide pathologic evidence of emphysema [16,17]. Spirometry is the most feasible method for diagnosing and tracking the functional development of COPD.
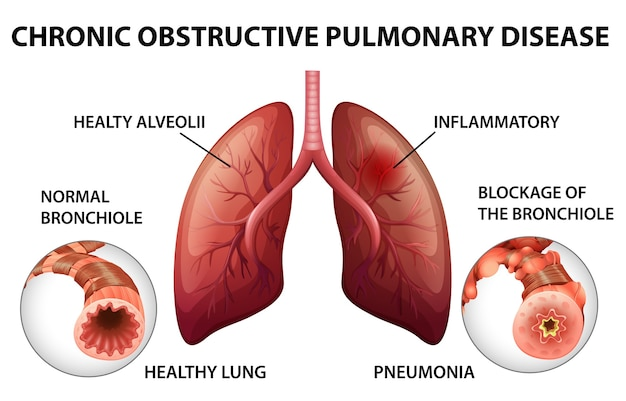
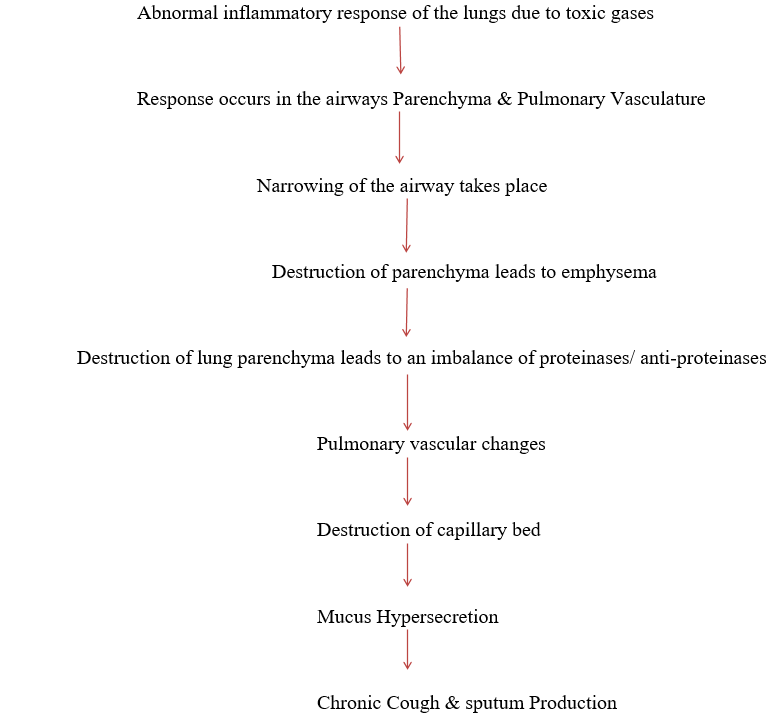
It appears the small conducting air channels and surrounding alveoli are where smoking first damages the human lungs. The lung's elastic supporting structure is diminished when alveoli are lost or injured. Because the airways are no longer bound by the radial traction forces of the surrounding alveolar attachments, there is a decrease in elastic recoil and an increase in airway resistance. The airway lumen is also decreased by remodeling and mural inflammation of the tiny airways. Therefore, bronchospasm, mucous hypersecretion, loss of elastic recoil, and airway inflammation and remodeling are all associated causes of airflow restriction in individuals with COPD. There is a complex interrelationship among these phenomena, which results in the progressive reduction in expiratory airflow as judged by the FEV1.[13,14]
TYPES: [18]
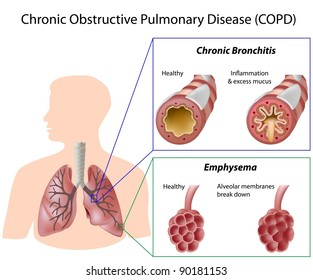
The small airways and alveoli, the outer layers of airways and air sacs, suffer damage in emphysema. This damage leads the sacs to lose their shape and its ability to deflect during the breathing cycle's expiratory phase, and holds air in the lung. The alveoli continue to swell as the outcome of this trapped air, causing an ongoing pattern of airway obstruction. The lungs get hyperinflated as a result of these modifications, which decreases gas exchange. This hinders the capacity to exhale carbon dioxide from the blood and makes it harder for people to breathe and oxygenate their blood efficiently.
Chronic Bronchitis:
The lining of the airways remains inflamed in chronic bronchitis. Swelling and the production of a lot of mucus result from this. Breathing becomes difficult due to these impacts.
Stages [19]
In addition to mild airflow restrictions, some people may also experience a persistent cough. They could cough up sputum, which is a concoction of saliva and mucus. It's possible that someone in this stage is unaware of their abnormal lung function.
In Stage 2, people frequently develop shortness of breath after training, and airflow limitation is higher. People usually seek medical assistance at this point.
In stage three, a person's airflow is greatly prohibited, which makes them also feel more breathing problems. This is accompanied by a decline in tolerance to exercise. The quality of life is diminished by the frequent periods of deteriorating symptoms.
In stage 4, people have severe airflow limitations and greatly reduced quality of life, while episodes of worsening symptoms may become life threatening.
|
Stages |
Description |
Findings (post-bronchodilator FEV1) |
|
1 |
Mild |
FEV1/FVC ratio < 70 % FEV1at least 80% of Predicted value May Have Symptoms |
|
2 |
Moderate |
FEV1/FVC ratio < 70 % FEV1 at least 50% to <80% of Predicted value May Have Chronic Symptoms |
|
3 |
Severe |
FEV1/FVC ratio < 70 % FEV1 30% to <50% of Predicted value May Have Chronic Symptoms |
|
4 |
Very severe |
FEV1/FVC ratio < 70 % FEV1 <30% of Predicted value OR FEV1 <50% of Predicted value Severe Chronic Symptoms |
Pathophysiology: [20]
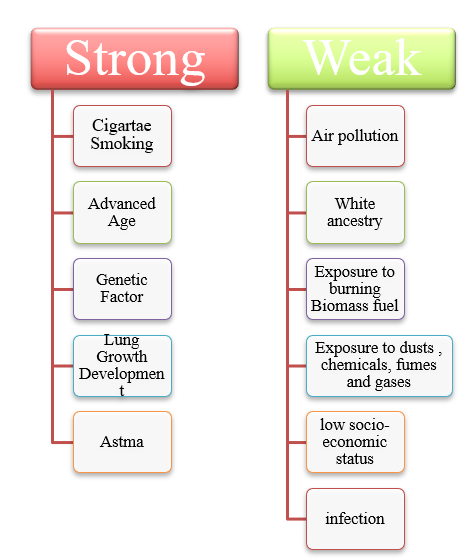
Risk Factors:[21]
Causes: [22]
Symptoms: [23,24]
Diagnosis [25]
Pulmonary function tests
Pulmonary function tests are done to find out how well your lungs are working. These tests may include:
You inhale fast and highly through a tube that is attached to a machine during this test. The device gauges the lungs' capacity to contain air as well as the rate at which air enters and exits the lungs. Spirometry determines the amount of restricted airflow and diagnoses COPD.
This test measures the amount of air the lungs hold at different times when breathing in and out.
This test shows how well the body moves oxygen and carbon dioxide between the lungs and the blood.
This easy test determines the amount of oxygen in your blood by placing a tiny device on one of your fingertips. Oxygen saturation is the proportion of oxygen in the blood. Along with an oxygen saturation test, you can also be required to walk for six minutes.
Exercise stress test.
An exercise test on a stationary bike or treadmill can be used to track lung and heart function while exercising.
Imaging
A chest X-ray may show some lung changes from COPD. An X-ray also can rule out other lung problems or heart failure.
A CT scan creates images of internal body structures by combining X-ray images from various angles. Compared to a chest X-ray, a CT scan provides far more data about abnormalities in your lungs. Chronic bronchitis and emphysema can be detected by a CT scan of your lungs. Additionally, a CT scan can assist determine whether surgery for COPD would be beneficial. Lung cancer can be detected with CT scans.
Imaging and pulmonary function tests can also be used to monitor your condition over time and assess the effectiveness of treatment.
Lab tests
This blood test measures how well your lungs are bringing oxygen into your blood and removing carbon dioxide.
Blood tests can tell if you have the genetic condition called alpha-1-antitrypsin deficiency.
Blood tests aren't used to diagnose COPD, but they may be used to find the cause of your symptoms or rule out other conditions. The GOLD was most recently updated in 2019 and was developed in 1998 to improve the diagnosis, treatment, and prevention of COPD. A post-bronchodilator FEV1 to FVC ratio of less than 0.7 is necessary for the diagnosis of COPD, which is then further divided into severity levels based on the projected FEV1 percentage.
GOLD classification of COPD on post-broncho dilator FEV1 (% predicted):
I Mild ?80%
II Moderate 50–79%
III Severe 30–49%
IV Very severe <30 [26]
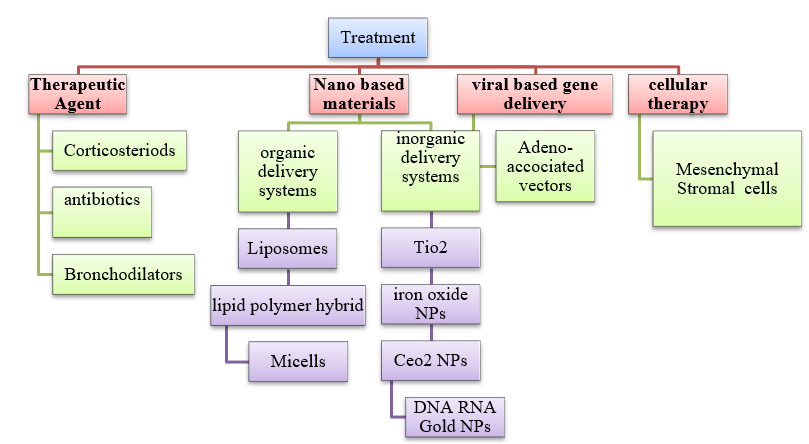
Treatment (27,28)
Oxygen therapy, a pulmonary rehabilitation program and in-home noninvasive ventilation therapy can all help treat COPD.
You could require additional oxygen if your blood oxygen level is low. Either a mask or plastic tubing with nose-fitting tips can be used to provide this additional oxygen to your lungs. An oxygen tank is connected to these. You can increase your mobility using lightweight, portable devices that you can carry with you.
Some COPD patients only utilise oxygen when they are sleeping or engaging in activities. Others constantly utilise oxygen. Oxygen therapy can prolong life and enhance quality of life. Evaluate your needs and options for oxygen therapy with your healthcare provider.
These programs typically incorporate counselling, breathing exercises, exercise training, health education, and dietary guidance. Your rehabilitation program can be customised to fit your needs by working with a range of specialists.
Following episodes of worsening symptoms, pulmonary rehabilitation may reduce the chance that you will need to return to the hospital. Additionally, pulmonary rehabilitation enhances your quality of life and enables you to engage more completely in daily activities. Discuss attending a program with your healthcare provider.
For some patients with severe COPD, this treatment may stop episodes of worsening symptoms. To find the most effective ways to apply this therapy at home, research is still being conducted. Bilevel positive airway pressure (BiPAP) and other breathing devices are supported by evidence when used in hospitals. Some persons with COPD may benefit from using BiPAP at home at night. You wear a mask over your mouth and nose that is connected to a noninvasive ventilation therapy equipment. BiPAP facilitates breathing and may reduce the risk of recurrent hospitalisation. Additionally, it reduces the amount of carbon dioxide that is exhaled into your lungs. Acute respiratory failure and the requirement for hospitalisation can result from an excess of carbon dioxide.
Even with regular treatment, there may be days or weeks when your symptoms worsen. These are referred to as exacerbations, and if treatment is delayed, they can result in lung failure.
A respiratory infection, air pollution, or other factors that exacerbate lung irritation and inflammation can all lead to exacerbations. Regardless of the reason, if you experience a cough that seems worse than normal, a change in the mucus you cough up, or difficulty breathing, you should seek medical attention immediately. You may need additional oxygen, medications like steroids, antibiotics, or both, or hospital treatment when exacerbations occur. Your healthcare provider can discuss with you how to avoid future episodes of worsening symptoms once your symptoms have improved. You might need to stop smoking, use long-acting bronchodilators, inhaled steroids, or other medications, be vaccinated against the flu every year, and stay away from air pollution whenever you can.
Surgery is an option for some people with some forms of severe emphysema that aren't helped enough by medicines alone. Surgical options include:
Small wedges of diseased lung tissue are removed from the upper lungs by the surgeon during this procedure. This makes more room in the chest, which allows the diaphragm, a muscle that aids in breathing, to function better and the healthy lung tissue that is still there to expand. This operation can help some people live longer and have a better quality of life.
This minimally invasive technique, also known as endobronchial valve surgery, is used to treat COPD patients. The lung is equipped with a tiny one-way endobronchial valve. Through the valve, air can exit the damaged lung portion, but no fresh air can enter. This gives the healthy portion of the lung more room to grow and function by causing the most damaged lobe to shrink.
If certain individuals meet certain requirements, they may be eligible for a lung transplant. A more active lifestyle and easier breathing are two benefits of lung replacement. However, there are serious dangers associated with this big procedure, including organ rejection. After receiving a lung transplant, you must take immunosuppressive medications for the rest of your life.
The destruction of the inner walls of the alveoli in the lungs results in the formation of large air gaps called bullae. As a result, one huge air sac remains rather than a collection of numerous smaller ones. Because old air is retained and new air cannot enter, these bullae can grow very large and create breathing issues. To enhance airflow, the surgeon performs a bullectomy, which involves removing the lungs' bullae.
Treatment options for persons with AAT-deficient COPD include those utilised for those with more prevalent forms of the disease. Replacing the absent AAT protein is another treatment option for certain individuals. This could stop the lungs from getting worse.
Lifestyle and home remedies
If you have COPD, you can take steps to feel better and slow the damage to your lungs:
Discuss ways to breathe more effectively throughout the day with your respiratory therapist or healthcare provider. Talk about breathing-friendly postures, energy-saving techniques like sitting down to complete work when you can, and how to unwind when you're having problems breathing.
With COPD, mucus tends to collect in air passages and can be hard to clear. Removing mucus with controlled coughing, drinking plenty of water and using a humidifier may help.
Being active could seem challenging if you have breathing difficulties. However, regular exercise and physical activity can strengthen your breathing muscles and increase your general strength and endurance. Discuss the best activities for you with your healthcare provider.
Maintaining your strength can be achieved by eating a healthy diet. Your doctor might suggest nutritional supplements if you are underweight. Losing weight can significantly improve your breathing if you are overweight, particularly when exercising.
It's important to stop smoking and stay away from areas where other people smoke. Lung damage may be exacerbated by secondhand smoke. Before you walk outside, read the daily air quality forecast because air pollution can also irritate your lungs. Determine what can cause episodes of worsening symptoms so that you can minimise your exposure to them.
Even if you're feeling well, keep to your appointment schedule. Monitoring your lung function on a regular basis is crucial. Additionally, to help avoid infections that could exacerbate your COPD, make sure you receive your yearly flu shot in the fall. Find out from your doctor when you should have the RSV, COVID-19, and pneumococcal vaccines. If your symptoms worsen or you observe signs of an infection, contact your healthcare provider. [25]
Preventions [29]
REFERENCE


Pooja A. Burungale*, Pranali A. Tate-Deshmukh, Sneha B. Powar, Pravin M. Kumbhar, Namrata S. Kathwate, Harshada S. Deshmukh, Priyanka B. Parekar, A Review Article on COPD, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 10, 696-707 https://doi.org/10.5281/zenodo.17291671
 10.5281/zenodo.17291671
10.5281/zenodo.17291671
