Dr. Subhash Technical Campus, Junagadh.
Chronic venous insufficiency or CVI, is a condition in which veins have problems moving blood back to the heart. With long-term (chronic) venous insufficiency, vein walls are weakened and valves are damaged. Chronic venous insufficiency can develop from common conditions such as Varicose Veins. It is a common condition characterized by enlarged, twisted, blue or purple bulging and painful veins, typically affecting the lower extremities of the body. It's noteworthy that even in the absence of obvious bulging veins, the term "varicose veins" is frequently used to describe superficial venous reflux. Simply put, these are known as "hidden varicose veins." A weakening of the venous valves and walls is a common cause of varicose veins. Blood might flow back and pool in veins due to damaged valves, causing them to enlarge. Weakened vein walls are longer, broader, and less elastic than normal, causing valve flaps to split, resulting in increased blood pooling and twisted veins. Usually, varicose veins worsen, causing pain, enlarged ankles, skin damage, leg ulcers, venous bleeding, and superficial venous thrombosis. A weakening of the venous valves and walls is a common cause of varicose veins. Blood might flow back and pool in veins due to damaged valves, causing them to enlarge. Weakened vein walls are longer, broader, and less elastic than normal, causing valve flaps to split, resulting in increased blood pooling and twisted veins.
The Latin term "Varix," which meaning "twisted," is where the word "varicose" originates. A "vein with a saccular development tortuous," as defined by the World Health Organization (WHO), is a varicose vein. The word "varicosity" refers generically to lengthy, twisted, pouched, thickened, friable, inelastic vessels that have similarly changed over time and are continuously losing their valvular efficiency. [7]. Varicose veins are defined as dilated, tortuous, subcutaneous veins ≥3 mm in diameter measured in the upright position with demonstrable reflux. [1-3]
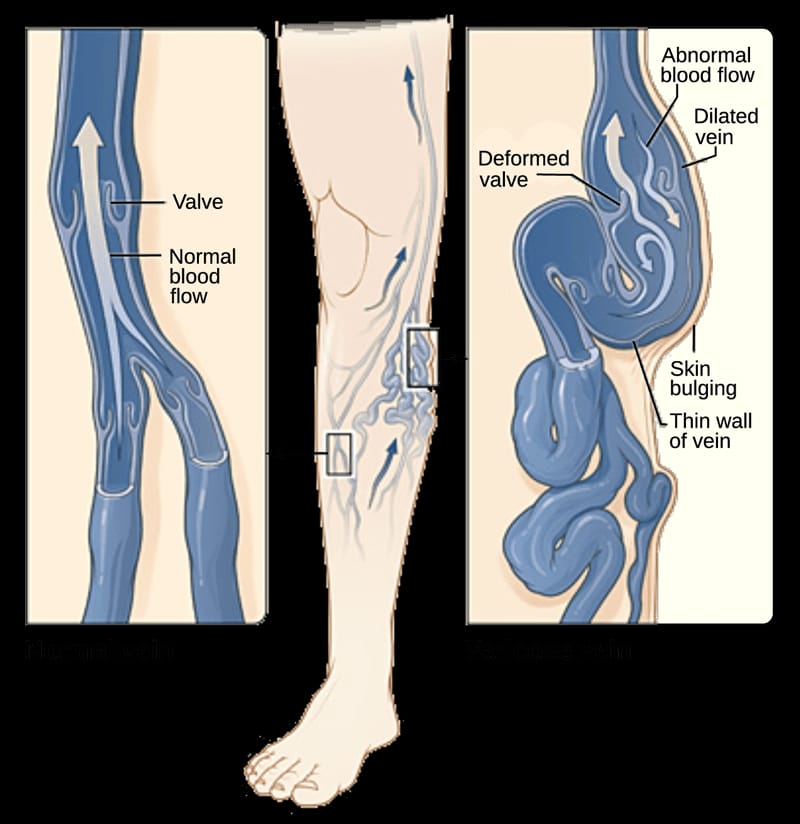
Fig 1.1 Varicose Veins forms in a lower extremity.
Anatomy
The superficial and deep venous systems carry venous blood from the lower limbs back to the right heart against gravity. Great saphenous veins (GSV), small saphenous veins (SSV), and their tributaries make up the superficial venous system. [1, 3]. The medial end of the dorsal venous arch is where the GSV begins. Veins are blood vessels located throughout the body that collect oxygen-poor blood and return it to the heart. Veins are part of the circulatory system.
ig: 1.2 Anatomical view of Varicose Vein
Pathogenesis
Varicose veins develop when the valves in the veins fail to function properly, leading to a backward flow of blood. These valves normally act like one-way doors, allowing blood to flow towards the heart and preventing it from flowing backward. [4, 5]. When these valves become weak or damaged, blood pools in the veins, causing them to swell and become visible. This pooling of blood can also put pressure on the surrounding tissues, leading to symptoms such as pain, fatigue, and swelling. [6]. The mechanism of valve failure is complex and can be influenced by factors such as age, genetics, and lifestyle. Factors like prolonged standing or sitting, pregnancy, and obesity can further increase pressure in the veins, contributing to valve dysfunction. The weakened valve system ultimately leads to the characteristic appearance of varicose veins. [4]. It is due to the various factors such as, Environmental and Patient factors, Genetic Predisposition, Local Hypoxia, Hemodynamic factors, Alteration in the extracellular matrix
Diagnosis and Evaluation
Doppler ultrasound helps with varicose veins detection and identifying severity. It is a special procedure to examine blood circulation.
Uses:
Uses:
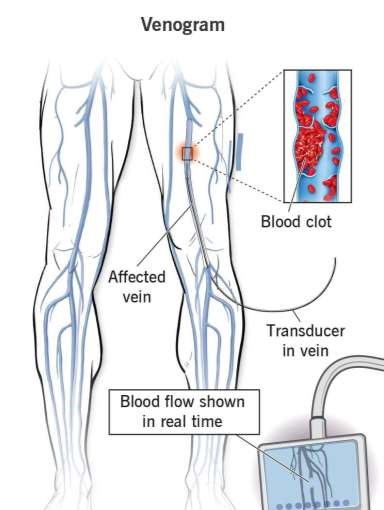
Fig. 2.1 Venogram
3. Ankle-brachial index (ABI):
This test measures blood pressure in the ankles and arms to determine the severity of arterial blockage and rule out other vascular conditions. [2, 3].
Uses:
Treatment of Varicose Vein
The conventional treatments for varicose veins involve compression therapies- employment of particular type of surgeries like cryosurgery, vein stripping, ambulatory phlebectomy. [4] The Non-surgical treatments mainly involve sclerotherapy and endothermal ablation. [5, 6].
1. Physical Therapy [6]
2. Compression Therapy [6]
Types of compression therapy device includes:
1. Surgical Therapy:
A. Vein Stripping: Vein stripping is a surgical procedure that removes or ties off a large vein in the leg to treat varicose veins and other chronic venous diseases [2, 3].The side effects are produced by this therapy that are bleeding, infections, bruishing[5, 6]. Stripping of varicose veins out surgically does not permanently remove veins, as most grow back but without valves, during the healing process, causing the same problem to reoccur. [3, 4].
B. Ambulatory Phlebectomy: In this technique by achieving laceration in the skin the superficial veins are removed. After this treatment the temporary inflammation and swelling may be observed [5].
2. Non-Surgical Treatments: The Non-surgical treatments mainly include Sclerotherapy, Ultrasound guided foam sclerotherapy and Endothermal Ablation. [3,7].
A. Sclerotherapy: By using this therapy, the spider veins or angioectasis are treated. For this treatment some sclerosing agents are used like as sodium salicylate, chromated glycerine they are administered by using small needles.
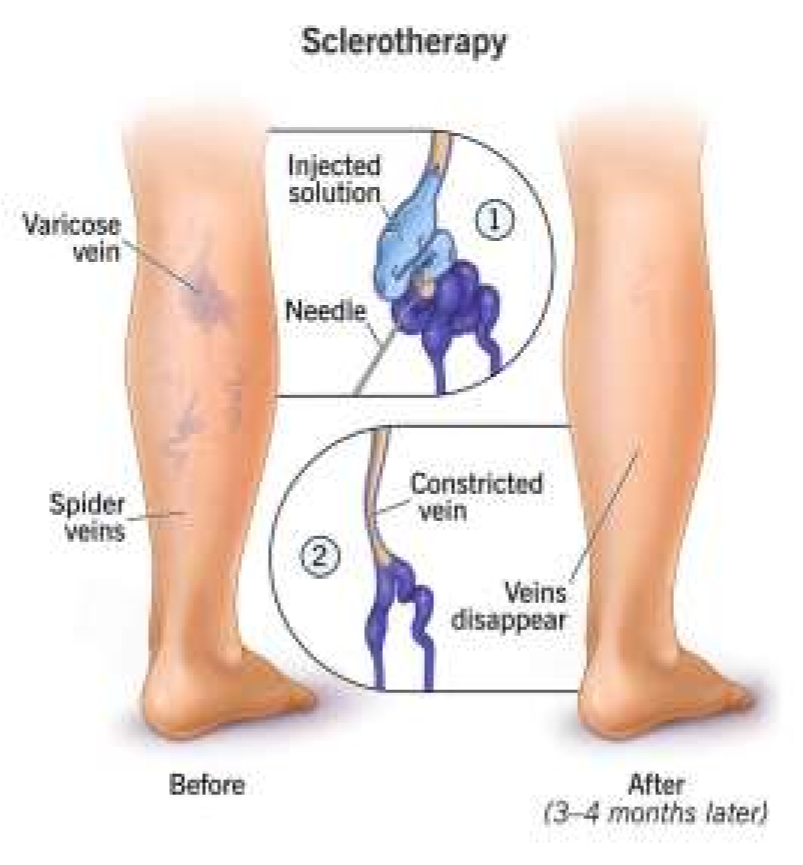
Fig.2.3 Sclerotherapy- Injecting a solution directly into varicose vein
Prevention of Varicose Vein
In most of the cases, varicose veins can be cured by early preventive measures such as,
Novel Approach of Varicose Vein
|
1. Name of Drug: Varithena 1% Approved by FDA: Originally in 2014 Active Ingredient: Polidocanol Drug Product: Polidocanol injectable (1.0%) Brand name: Asclera Class of Drug: Sclerosing agent, Vasosclerator |

|
[Table 1: Polidocanol]
|
1. |
|
White Pungent Bitter & Unpleasant |
|
2. |
BCS Class |
Class III |
|
3. |
Solubility |
Hygroscopic, Limited solubility in water & alcohol |
|
4. |
pH (solution at 3% w/v) |
4.0 - 7.5 |
|
5. |
Melting Point Range |
21 - 27°C |
|
6. |
Density at 45°C |
0.987 g/cm3 |
|
7. |
Molecular formula |
C12H25 (OCH2-CH2-), OH |
|
8. |
Route of Administration |
Intravenous Route |
|
9. |
Mean Molecular |
Approximately 600. |
Mechanism of Action
Step 1: Direct Injection into varicose veins
Step 2: Damage to the endothelial cells, leading to disruption of cell membrane integrity
Step 3: Triggers an inflammatory response à WBCs and platelets aggregation
Step 4: Fibrinogen is converted to fibrin, forming a blood clot.
Step 5: Due to replacement of fibrotic tissue à Vein wall thickening and contraction
Step 6: Fibrotic tissue contracts, causing the vein to narrow and close à Blood flow is redirected to adjacent veins.
|
2. Name Of Drug: Rivaroxaban Approved by FDA: Originally in 2011, in October 2019 it was Approved to prevent blood clots. Brand name: Xarelto Generic name: Rivaroxaban Dosage form: Tablets and Oral Suspension (10mg, 15mg) Class of Drug: Anti - Coagulate |
|
[Table 2: Rivaroxaban]
|
1. |
Physical Description
|
White to Off white |
|
|
|
Odorless Bitter |
|
2. |
Molecular weight |
435.89 g/mol |
|
3. |
Solubility |
Water: Practically insoluble, Ethanol: Soluble |
|
4. |
pH |
6.8-7.2 |
|
5. |
Melting Point Range |
220-225°C |
|
6. |
Density |
1.43 g/cm³ |
|
7. |
Molecular formula |
C19H18Cl2N4O4S |
|
8. |
Route of Administration |
Oral Route |
Mechanism of Action
Step 1: Inhibition of Factor Xa
Step 2: Prevention of Prothrombinase Complex Formation
Step 3: Reduction of Thrombin Generation
Step 4: Inhibition of Fibrin Clot Formation
Step 5: Prevention of Blood Coagulation
|
3. Name Of Drug: Apixaban Approved by: Initial U.S approval 2012 Brand name: ELIQUIS Generic name: Apixaban Dosage form: Tablets and Oral Use (2.5mg and 5 mg) Class of Drug: Anti - Coagulate
|
|
[Table 3: Apixaban]
|
1. |
Physical Description
|
Pale Yellow Film- coated Odorless Tasteless |
|
2. |
Molecular weight |
419.45 g/mol |
|
3. |
Solubility |
Slightly Soluble in water & freely soluble in methanol |
|
4. |
PH |
4.5-6.5(Slightly acidic to neutral) |
|
5. |
Melting Point Range |
165-170°C |
|
6. |
Density |
1.43 g/cm³ |
|
7. |
Molecular formula |
C25H25N5O4 |
|
8. |
Route of Administration |
Oral Route |
Mechanism of Action
Step: 1 Inhibition of Factor Xa
Step: 2 Blockage of Prothrombinase Complex
Step: 3 Decreased Thrombin Formation
Step: 4 Prevention of Platelet Activation
Step: 5 Inhibition of Coagulation Cascade
|
4. Name Of Drug: Ticagrelor Approved by FDA: Initial U.S approval 201 Brand name: Brilinta Generic name: Ticagrelor Dosage form: Tablets and Oral Suspension (90mg) Class of Drug: Anti - Platelet
|
|
[Table: 4 Ticagrelor]
|
1. |
Physical Description
|
Yellow- Pale Yellow Round & Film Coated Odorless Mild, slightly sweet or neutral taste |
|
2. |
Molecular weight |
522.65 g/mol |
|
3. |
Solubility |
Water: Practically insoluble, Ethanol: Soluble |
|
4. |
PH |
5.5- 6.5 |
|
5. |
Melting Point Range |
184-188°C |
|
6. |
Density |
1.43 g/cm³ |
|
7. |
Molecular formula |
C23H28F2N6O4S |
|
8. |
Route of Administration |
Oral Route |
Mechanism of Action
Step 1: Inhibition of P2Y12 Receptor
Step 2: Increased cAMP Levels
Step 3: Reduced Platelet Activation
Step 4: Endothelial Function Enhancement
Step 5: Prostacyclin (PGI2) Increase
Step 6: Reduced Inflammation and Oxidative Stress
|
5. Name Of Drug: Dabigatran Etexilate Approved by: Initial U.S approval 2010 Brand name: PRADAXA Generic name: Dabigatran Etexilate Dosage form: Capsule (75mg and 150mg) Class of Drug: Anti – Coagulate & Direct Thrombin Inhibitor |

|
|
1. |
Physical Description
|
Yellow |
|
|
|
Odorless Tasteless |
|
2. |
Molecular weight |
407.47 g/mol |
|
3. |
Solubility |
Soluble in water, methanol & ethanol |
|
4. |
pH |
4.6-5.6 (Slightly acidic to neutral) |
|
5. |
Melting Point Range |
180-185°C |
|
6. |
Density |
1.45 g/cm³ |
|
7. |
Molecular formula |
C25H25N2O3 |
Mechanism of Action
Step 1: Oral administration results into absorption from stomach & small intestine
Step 2 Dabigatran Etexilate is hydrolyzed to Dabigatran by esterases
Step 3: Dabigatran distributes to tissues, including the liver, kidneys, and vascular wall
Step 4: Dabigatran binds reversibly to thrombin (Factor IIa)
Step 5: Thrombin's activity is inhibited, preventing: Conversion of fibrinogen to fibrin à Activation of Factor XIII à Platelet aggregation
Step 6: Reduced thrombin activity decreases blood clot formation
CONCLUSION
Varicose veins are a prevalent and complex condition affecting millions of people worldwide. The understanding of varicose vein development and emergence of Novel approaches for varicose veins marks a significant shift in the treatment & offering improved patient outcomes. Anticoagulants and Anti-inflammatory drugs for Varicose Veins are characterized by inflammation and blood clotting. Anticoagulants and anti-inflammatory drugs target these pathways, alleviating symptoms and slowing disease progression. All drugs which we have discussed in this review have a significant in their mode of action and therapy of varicose veins. Further research is necessary to elucidate the mechanism & optimize the therapeutic action.
REFERENCES


Ishita Vekariya*, Morvi Raval, Arati Bhetariya, Dr. Chintankumar Tank, Vandana Ghul, Yash Mori, Drashti Bhalara, A Development of Varicose Vein: Today & Tomorrow, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 4, 26-34 https://doi.org/10.5281/zenodo.15117741
 10.5281/zenodo.15117741
10.5281/zenodo.15117741
