Pravara Rural Education Society’s College of Pharmacy (For Women), Chincholi, Nashik, 422102, (Maharashtra), India.
Any detectable molecular predictor of cancer risk, cancer occurrence, or patient prognosis is referred to as a molecular cancer biomarker. Proteomic markers, transcriptional changes, epigenetic signatures, and germline or somatic genetic variants are a few examples.These markers rely on biomolecules, such proteins and nucleic acids, that can be found in tissue samples taken by tumor biopsy or, in a simpler and non-invasive manner, in stool, urine, buccal swabs, saliva, blood (or serum or plasma), etc. Over the past few decades, there has been a significant advancement in detection technologies, including approaches for studying circulating tumor DNA/RNA or exosomes, nanotechnology, and next generation sequencing. Biomarkers have a variety of clinical applications.they may aid in improving clinical practice decisionmaking. Furthe rmore, since recently developed targeted medicines only work in people with particular cancer genetic mutations and biomarkers are the tools used to identify these patient subsets.precision oncology is required. To solve the scientific obstacle of creating novel biomarkers with higher sensitivity, specificity, and positive predictive value, however, advancements in the field of cancer biomarkers are required.(1).
Due to the lack of access to proper diagnostic methods and treatments, more than 8.2 million people lose their lives to Cancer every year. Through cancer screening, prognostics assessment and monitoring the researchers
investigating strategies For the identification and treatment of cancers. Nevertheless, there are currently no recognized diagnostic techniques that do not negatively impact patients well- being while detecting cancer. For instance, radiography is widely used to diagnose cancer, but a patient receiving too much ionizing radiation may be at risk for health problems . However, it is believed that on-radiation modalities, like magnetic resonance imaging (MRI) and ultrasound scans, are ineffective in detecting minimal residual disease . Additionally, because of tumor heterogeneity, the "solid biopsy" method of detection is invasive and unable to precisely track dynamic changes in tumors . Therefore, in the age of precision medicine (PM), the need to develop accurate and non-invasive techniques for early cancer diagnosis is becoming more and more pressing. (2) .A biomarker is any sign that abnormal or normal biological processes, diseases, or illnesses are present. These markers can be discovered in bodily fluids, such as blood or tissues.When customized for the oncology domain, a cancer biomarker precisely detects cancerous traits, ideally with a high level of precision and dependability, known as its sensitivity and specificity. There is more to using cancer biomarkers than just figuring out what kind of cancer a patient has. Tumor markers can, in fact, offer important information about the probable course of the illness, including the likelihood of recurrence and the anticipated results of treatment, once a diagnosis has been made. Cancer biomarkers are essential for describing a
disease’s prognosis without regard to treatment (prognostic biomarkers) or for forecasting a cancer’s response to a particular treatment, which aids in anticipating treatment results (predictive biomarkers). The presence of proteins belonging to many functional groups, including enzymes, hormones, antigens, and receptors, is the primary basis for the classification of the many cancer biomarkers that have been discovered. Unique genetic signatures result from changes in cancer-related genes, such as single gene-level mutations, amplifications, and translocations, or from the development of genetic profiles using microarrays. These modifications aid in the discovery and classification of cancer biomarkers, which advances our knowledge of and ability to treat the illness. No matter what kind of cancer biom”rker’they are, the best ones have simple, repeatable, dependable, and economical detection techniques that are associated with measurable improvements in patient outcomes. Taking intoaccount both the developments in testing methods and a deeper understanding of tumor biology, this review will examine the present uses and potential future developments of cancer biomarkers. How these advancements support the efficient use of biomarkers in cancer diagnosis, prognosis, and treatment planning will be discussed.(3) Because more people are adopting lifestyle choices linked to cancer, cancer is the second leading cause of mortality in emerging nations and the leading cause of death in economically developed nations . Cancer-related morbidity and mortality are rising as the global population ages and developing nations continue to modernize. The most frequent causes of cancer-related mortality each year are lung, liver, colorectal, stomach, and breast cancer. A combination of genetic variables and environmental agents (physical, chemical, and biological carcinogens) leads to the complicated disease known as cancer, which is caused by genetic mutations or aberrations that allow normal cells to convert into tumor cells.Furthermore, abnormal gene combinations that result in mutations, overexpression, or deletions might give birth to malignancies. Gene mutations or changes result in a disdain for cell cycle checkpoints during carcinogenesis, which allows a normal cell to expand out of control. Therefore, cancer cells possess two heritable characteristics: (A).they invade and colonize areas that are typically designated for other cells. (B). they and their offspring procreate despite the normal constraints on cell division. A comprehensive understanding of the mechanism of cancer growth is still necessary, despite the fact that various scientific fields have demonstrated throughout the years to be able to answer the mystery surrounding the onset of cancer.
Several biomarkers have responded well in recent years and have been successfully used to predict the course of cancer. The creation of new and reliable biomarkers has been aided by developments in genomics, high technology testing, and molecular procedures .Similarly, these developments give us a fresh perspective on the many approaches to cancer treatment. The molecular markers for cancer diagnosis and prognosis will be the main topic of this paper. Due to the lack of access to proper diagnostic methods and treatments, more than 8.2 million people lose their lives to cancer every year . Through cancer screening, prognostic assessment, and monitoring, researchers have been investigating strategies for the identification and treatment of cancers. Nevertheless, currently no recognizeddiagnostic techniques that do not negatively impact patient’s’ physical well-being while detecting cancer.(4)
WHAT IS BIOMARKERS
"According to NCI, a biomarker is "a biological molecules" present in blood and other body tissues .Cancer is included in this Usually, biomarkers distinguish a patient with the illness from one who does not. Post-translational modifications, transcriptional changes, and germline or somatic mutations are some of the possible causes of the changes. The range of biomarkers is enormous and includes, among other things, proteins (such an enzyme or receptor), nucleic acids (like a microRNA or other non-coding RNA), antibodies, and peptides. Gene expression, proteomic, and metabolomics signatures are examples of changes that can be grouped together to form a biomarker. When biomarkers are found in the bloodstream (whole blood, serum, or plasma) or in excretions or secretions (stool, urine, sputum, or nipple discharge), they can be readily evaluated non-invasively and serially. Alternatively, biomarkers can be obtained from tissue and need to be evaluated by biopsy or specialized imaging. Genetic biomarkers can be somatic, such as mutations in DNA extracted from tumor tissue, or inherited, such as sequence differences in gerlie liDNA recovered from whole blood, sputum, or buccal cells.(5)
STEPS DEVELOPMENT IN BIOMARKERS
There are several methods for identifying potential biomarkers. Finding potential Generally speaking, the word “biomarker” in medicine refers to a protein that is detected in the bloodstream and whose quantity reflects both a pharmacological reaction to the applied therapy and a normal or pathological response of the organism. Looking at it more broadly, a biomarker is any indicator that serves as a gauge of how severe an illness or other physiological biomarkers based on the biology of the tumor and its surroundings or the pharmacological agent's metabolism has been the conventional method. Biomarker identification is now commonly carried out using a "discovery" approach, employing methods like high-throughput sequencing, gene expression arrays, and mass spectroscopy to swiftly identify individual or groups of biomarkers that vary between cohorts, as a result of the explosion of new knowledge about tumors and the introduction of new technology. Due to the large volume of data produced by these methods, special attention must be given to the study design and data processing to reduce the possibility of finding relationships that turn out to be false positives Condition is in the body.
ANALYTICAL VALIDATION
It is crucial to concentrate on both pre-analytic and analytic aspects of the test in order to identify the biomarker while developing a new prospective biomarker. Pre-analytic validity is the way the sample that will be analyzed using the innovative assay is handled (Moore et al., 2011) .The duration and storage circumstances between sample collection and processing, the type and duration of fixation, or lack thereof, and the storage conditions are only a few of the many sample-related parameters that Because they could have an impact on the outcomes and the reproducibility of the potential biomarker, these preanalytic issues should be taken into account. Analytical validity refers to the technical evaluation of the biomarker assay, which needs to adhere to specific criteria. Assessing the assay's robustness, specificity, and sensitivity is essential. Both within and between laboratories, the results' correctness and reproducibility must be ensured. For instance, problems can arise when labs use an antibody in an experiment whose quality varies from lot to lot.
To create uniformity for sample handling, sample testing, assay interpretation, and result reporting across laboratories, proficiency testing programs are currently being developed for specific key biomarkers, such as estrogen receptor and Her2 assessment in breast cancer (Hammond et al., 2010, Wolff et al., 2007). The College of American Pathologists or other certifying bodies may grant accreditation to laboratories that successfully complete the programs.
CLINICAL VALIDAIONS
Following the development of a technically sound assay, the biomarker needs to be examined to ascertain its clinical, or “biologic,” validity. The ability of the biomarker to consistently separate the entire population of interest into two groups for example, those who are more or less likely to have an event is known as clinical validity. Clinical validity does not meanthat clinical care should be guided by the biomarker. As in any science, validity must be confirmed by reproducing anobservation of apparent clinical validity in a totally different collection of samples. Numerous methods for validation, or replication, have been put forth. Overfitting, however, might provide the impression that a test has exceptional discriminatory capacity, which cannot be replicated when independently validated, if the samples in the test and validate groups are not independent. While some researchers contend that an entirely independent researcher should conduct the independent validation, others think that the original researchers should conduct of the initial validation study using the original methodology but with a different sample cohort is seen in the (Ransohoff, 2007)
CLINICAL UTILISATION
An assay must demonstrate clinical value with extremely high levels of evidence before it may be used to guide patient care (Simon et al., 2009). Prognostic biomarkers are frequently measured by clinicians for their patients. However, unclear instructions on how to use the data for patient care might cause misunderstandings and, worse, poor treatment choices. To guarantee that new biomarkers introduced into clinical practice will appropriately direct by the patient BIOMARKERS OF CANCER
By seeing cancer as a disease process, biomarkers are demonstrated here. Another name for a tumor marker is a “cancer biomarker.” It is a trait that may be measured and assessed objectively as a sign of pathogenic processes, normal biologic processes, or pharmacologic reactions to a therapeutic intervention. Either the tumor or the body’s reaction to cancer produces this trait or biomarker (6).In order to guide decision-making and ensure the effectiveness of innovative anticancer treatments, cancer biomarkers have become essential in cancer research and drug development. One Two primary categories of biomarkers exist:
1)Biomarkers for diseases.
2)Biomarker associated with drugs
Disease-related biomarkers help with staging cancer, predicting disease outcomes, identifying cancer patients in the general population, and risk stratification. On the other hand, biomarkers linked to drugs offer important insights into survival and prognosis after clinical intervention.These predictive variables aid in determining which patients are most likely to benefit fromparticular therapies as well as evaluating the efficacy and any adverse effects of those treatments. Only a few number of biomarkers have been successfully translated into routine clinical use, despite some advancements in biomarker development. An ideal biomarker should be inexpensive, noninvasive, or minimally invasive, and simply and consistently assessed with good analytical specificit and sensitivity. However, issues like small sample sizes, mismatched case and control specimens, and mistakes in sample collection, handling, storage, preparation, and analysis make it difficult to translate biomarkers from the lab to clinical practice. In the age of targeted therapy, when personalized medicine seeks to forecast a patient’s reaction to medical treatment and customize therapies based on unique biological data, the identification of biomarkers is important. The cancer mortality rate decreased by 1.5% between 2019 and 2020, which helped to prevent and estimated 3.8 million deaths from cancer and resulted in a 33% decrease in overall cancer deaths. The fall in death annually between 2016 and 2020, is primarily attributable to improvements in cancer treatment. The therapy of cancer has been transformed by recent developments and trends in cancer biomarkers. (7)
CLASSIFICATIONOF BIOMARKERS OF CANCER:

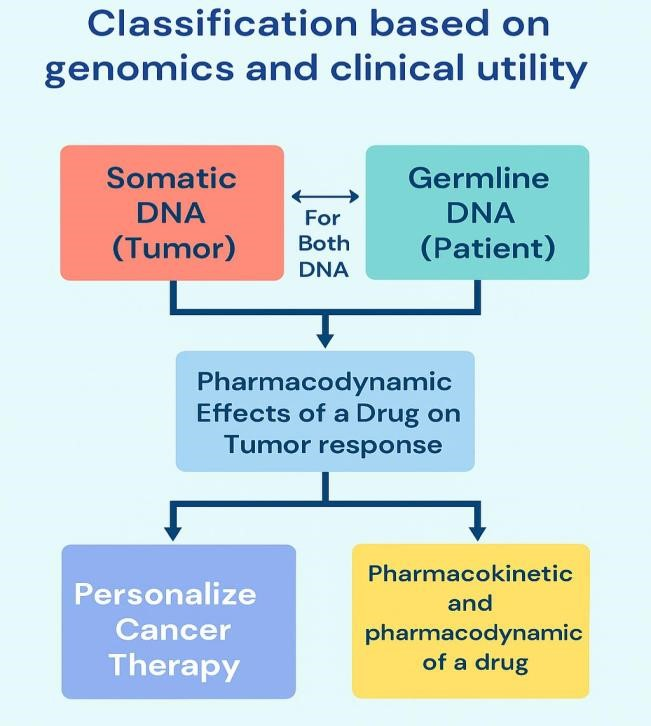
There are two types of cancer biomarkers: prognostic and predictive. Insights into illness outcomes are provided by prognostic biomarkers, whilst treatment responses can be assessed by predictive biomarkers fig.1 Additionally, biomarkers can be classified as germline or somatic based on the genetic makeup of the patient. Moreover, a more intricate framework is available for classifying the i pathogenicit of biomarkes.
DETECTION
There are two methods for detecting biomarkers: quantitative and qualitative. The quantity of the marker associated with the disease or disease stage is determined by the quantitative biomarker. Only thqualitative biomarker connects the marker to the illness state. Assessing the validity of any biomarker is complicated process that requires meeting three main requirements. A)Content validity indicates how well a biomarker captures the biological process under study.B)Construct validity, which deals with other pertinent features of the illness or characteristic.C)Criterion validity, which is often assessed by sensitivity or specificity, the predictive power, demonstrates the degree to which the biomarker correlates with the particular disease The identification and assessment of biomarkers should constantly take the disease’s heterogeneity into account, since the full and intricate understanding of many diseases is still being worked out. The “Early Detection Research Early Detection Research Network” of the National Cancer Institute (NCI) detailed the systematic development and evaluation of biomarkers in five phases in 2002. These phases are as follows:
Phase I: It is the pre-clinical exploratory phase, during which promising directions are identified.
Phase II: It is the validation phase, during which the clinical assay for biomarker validation is established
Phase III: It is the retrospective longitudinal phase, during which study subjects’ specimens are assessed prior to the onset of the disease.
Phase IV: It is the prospective screening study phase, which assesses the biomarker’sensitivity and specificity in a prospective study.
Phase V: Cancer control phase to assess the new diagnostic test’s overall hazards and benefits for the screened population
CANCER SCREENING
Traditionally, patients with a limited number of cancers have been monitored for recurrent disease using cancer-related protein markers, such as lactate dehydrogenase (LDH) for malignant melanoma, carcinoembryonic antigen (CEA) for colorectal adenocarcinoma, AFP for hepatocellular carcinoma, and CA-125 for ovarian cancer. While cancer-related protein indicators are very sensitive and specific to cancer activities in germ-cell tumors, most cancer-related proteins, such as LDH, are only used as screening tools for cancer recurrence with insufficient specificity.(9)Finding cancer at a clinically localized stage and conducting a test are only a small part of the screening process. An asymptomatic person undergoes a screening test to detect the possibility of cancer and to determine whether additional testing, such as a biopsy and staging, is required. In order to be beneficial, screening must identify the disease early and result in an effective therapy; additionally, early use of the effective treatment must provide better results than treatment at the commencement of symptoms. Additionally, the advantages must exceed the disadvantages. An apparent confined malignancy does not necessarily benefit from early identification. The literature contains numerous examples of screening tests and therapies that resulted in earlier disease detection and longer longevity as evaluated from the date of diagnosis, but no change in mortality or net harm was experienced (10)
CANCER BIOMARKERS UNDER THE EVALUATION OF CLINICAL TRIALS
Several predictive biomarkers, primarily derived from a single gene or protein, are presently undergoing phase II or III study in conjunction with the treatment drugs that accompany them . The trend toward developing minimally invasive cancer diagnostics and the growing significance of predictive biomarkers are both evident from this snapshot. Less common malignancies are also benefiting from the quick advancements in the field, since biomarkers that have been proven to be effective in one type of cancer are being found and confirmed to be effective in other cancers (such as BRAF mutations or HER2 overexpression) that arise from certain common oncogenic pathways. In a large prospective trial that is currently enrolling over 6,600 participants in nine countries, the 70-gene breast cancer signature is being evaluated for its recurrence-predictive capabilityincomparison to clinicopathological assessment (MINDACT study). According to preliminary findings, the 70gene signature provided information to standard assessment.(11).
Incorporating biomarkers into clinical trials presents significant obstacles. This is why they are typically incorporated into oncology clinical trials as exploratory outcomes (McShane et al., 2009). The successful treatment of advanced tumors is significantly impacted by individual patient heterogeneity, both within metastatic lesions and across original and metastasis sites (Kummar et al., 2015). While tumor heterogeneity and changes over time are expected to contribute to the evolution of treatment resistance, they are not adequately addressed since patient biopsies frequently target a single piece of tissue at a single time point rather than at many ones longitudinally (Kummar et al., 2015).Additionally, biomarkers may indicate molecular abnormalities that are either passenger or driving events (Kummar et al., 2015). In order to target various abnormalities, other concerns include the percentage of cells, the technique for acquiring a tumor sample, and the order in which multicombinatorial drugs and their dosage levels should be employed (Kummar et al., 2015). In spite of this, biomarkers can be utilized to create more uniform groups by leveraging the genetic composition of the tumor to guide the treatment choices of specific patients (Mandrekar and Sargent, 2009) Prognostic, predictive, surrogate, screening or diagnostic, pharmacodynamic efficacy and resistance, and integral and integrated biomarkers are some of the classifications of biomarkers that have been made in the literature With a brief summary of the others, we primarily concentrate on prognostic and predictive indicators for the purposes of this article. When employed as an early indicator of treatment efficacy, a surrogate marker—such as HIV load—is a biomarker that regulatory bodies have approved as a replacement for a clinical objective and may be cost-effective (Mandrekar et al., 2013). PSA levels in prostate cancer are one example of a condition that is monitored using screening or diagnostic indicators.
Response and treatment resistance are measured using pharmacodynamic efficacy and resistance biomarkers, respectively (Hong and Simon, 2013). Lastly, while integrated biomarkers are not utilized to determine patient therapy, they do determine patient incorporation and/or guide clinical trial protocols (Mankoff et al., 2015). Prognostic indicators, such as a BRCA1/2 mutation, which can also predict the use of PARP inhibitors,(12) .
PRESENT AND FUTURE OF CANCER BIOMARKERS
There seems to be little progress in the study of cancer biomarkers. In the past two decades, very few, if any, novel cancer biomarkers have been brought into clinical use. This is due to the fact that the majority of recently identified cancer biomarkers are less sensitive and specific than the traditional cancer biomarkers already in use. Finding novel and enhanced cancer biomarkers was not possible with the groundbreaking technologies of proteomics, genomics, and other omics. In contrast, the rapid expansion of whole genome and exome sequencing in recent years has made it possible to obtain, for the first time, nearly comprehensive mutational landscapes of numerous cancer types in thousands of samples examined. We now know that cancer is the only disease where many of these mutations occur. Therefore, the mutant proteins that these genes express might be the longsought, extremely specific cancer molecules that we might hope to employ as cancer biomarkers. Here, I hypothesize that contemporary mass spectrometry might possess the sensitivity and specificity required to identify mutant proteins in a range of biological fluids for the purposes of illness monitoring, diagnosis, and prognosis.(13).
The simultaneous examination of thousands of biological molecules Is made possible by the development of potent proteomic and genomic technologies combined with sophisticated bioinformatic tools. The development of novel tumor signatures through these methods opens the door to personalized cancer treatment since they are sensitive and specific enough for early cancer detection, disease progression tracking, and appropriate treatment selection.(14).
In order to identify biomarkers indicative of the cancer phenotype and potential therapeutic targets, cancer research has spent decades examining the molecular characteristics that distinguish cancer cells from their healthy counterparts. As a result, numerous molecular characteristics of cancer that are involved in signal transmission.
(1) cell senescence.
(2) other characteristics of cancer cells .
(3) have been identified. The metabolome is seen to be the most representative of the phenotype, even if the genome, transcriptome, proteome, and transcriptome are all functional levels of a biological system.
(4) Investigating the metabolome of cancer may be the most effective method of identifying phenotypic alterations in relation to biological function, particularly in cases where minute variations in metabolite concentrations may be easily managed
These factors make metabolomics, along with many other areas of life science, one of the field in cancer research that is growing the fastest. Specific biomarkers that may be utilized in screening for prognostic and diagnostic purposes are anticipated to be identified for a variety of malignancies. It should be possible to consistently identify a trustworthy biomarker in samples, and sample collection should be done with the least amount of patient or subject invasion possible. In the quest for possible.biomarkers that characterize a special cancer and whose directional change is noticeably greater than all other endogenous metabolites that make up the frequently complicated sample for analysis , the use of metabolomics in cancer is growing yearly (15)
EXAMPLES OF CANCER BIOMARKERS IN DESCOVERY, RESEARCH OF ONCOLOGY
Cancer has been the subject of numerous omics-based research projects. Biomarker-based patient stratification is ideal because of the disease’s heterogeneity and the difficult relapse episodes. 3, 25, 38, and 39 Selected publications that highlight the advancements in biomarker identification and the ways in which different omics technologies can speed up this process by molecularly characterizing cancer cells and their byproducts are discussed in the sections that follow.
SOLID TUMOR:
There have also been reports of solid tumor monitoring and identification using noninvasive biomarkers. To detect pancreatic, ovarian, colorectal, bladder, melanoma, gastroesophageal, breast, hepatocellular, and head and neck cancers, for instance, Bettegowda et al. measured circulating tumor DNA (ctDNA). 53 These authors found that 75% of the patients (640) had ctDNA in 5 ml of plasma, and that the concentration of ctDNA was inversely related to survival rates. Furthermore, compared to 55% of patients without metastases, 82% of patients with metastatic disease had ctDNA identified. To find alterations in each patient, NGS was utilized for whole genome or exome sequencing of samples taken from solid tumors.The suggested approach enabled the detection of known clinically relevant K-Ras mutations in patients with metastatic colorectal cancer with a sensitivity of 87.2% (the test was positive for 87.2% of patients) and a specificity of 99.2% (the test was negative for 99.2% of healthy volunteers used as a control group) in tests without prior solid tumor genetic profiling, even though the initial genetic profiling of the tumor was required to track ctDNA.(16).
TRETMENT ON BIOMARKERS OF CANCER
One of the biggest global public health concerns is cancer, a complicated and multidimensional collection of disorders . With a predicted 19.3 million new cases and 10 million cancer-related deaths in 2020 alone, cancer continues to be a major source of morbidity and mortality globally . Breast, lung, colorectal, and prostate cancers are among the most prevalent cancers, however the prevalence of other cancer types varies greatly (4). In particular, lung cancer caused the greatest number of cancer fatalities (18%), and breast cancer accounted for 11.7% of new cases.(17).
BREAST CANCER:
Globally, breast cancer is the primary cause of cancer-related deaths among women. Over 625,000 deaths and approximately 2.1 million new cases were reported in 2018. As a result, the pharmaceutical business and public research face significant challenges in the treatment of breast cancer [57]. Additionally, one of the main issues is the frequent occurrence of therapeutic resistance in this cancer. Breast cancer recurrence, the primary cause of fatalities from breast cancer, can be used to describe this resistance. In order to achieve synergistic effects in killing tumor cells, drug combinations have been evaluated extensively in the treatment of breast cancer .The first example is the molar ratio of 1:20 between doxorubicin (DOX) and glycyrrhetinic acid. When used against MCF-7 breast cancer cell lines, this combination increased intracellular DOX accumulation and improved cytotoxicity and apoptosis [58]. The combination of verapamil (VERA) and paclitaxel(PTX) on adriamycinresistant breast cancer cells (MCF-7/ADR) is another. When both drugs were used together, the IC50 values were much lower than when PTX was used alone because VERA increased PTX’s sensitivity and effectiveness against these resistant cancer cells. Overall, cell cycle arrest and apoptosis seemed to be the mechanisms underlying the suppression of cell proliferation.
COLORECTAL CANCER:
More than 1.85 million cases and 850,000 deaths from colorectal cancer (CRC) occur each year, making it the third most frequent cancer in the world. Twenty percent of cases are classified as metastatic, and twenty-five percent of initially localized cancers eventually proceed to a metastatic stage, making it a prevalent metastatic malignancy. A major problem is that 40% of cases in the US relapse after receiving initial therapy for localized malignancies. In this situation, a combination of pharmaceutical drugs may be effective in preventing relapse and resistance mechanisms.
A combination of oxaliplatin and trifluridine/tipiracil (FTD/TPI) was shown by Limagne et al. to be effective against the microsatellite-stable colorectal cancer cell line CT26. As in vitro trials gave way to in vivo ones, the significance of this combination became clear. In fact, it seems that oxaliplatin is necessary for the induction of immunogenic cell death (ICD) in cell culture [61]. In a different study, Guo et al. demonstrated that GW4064, an agonist of the farnesoid X receptor (FXR), increases the chemosensitivity of colorectal cancer cells to oxaliplatin by stopping the growth of tumor cells in vivo and causing pyroptosis and apoptosis in vitro.
PROSTATE CANCER:
With about 1.4 million new cases and almost 375,000 deaths in 2020, prostate cancer was the second most prevalent disease diagnosed globally and the fifth greatest cause of death for males [63]. Metastatic castration-resistant prostate cancer is one of the several resistance phenomena that are seen. Androgen deprivation therapy is usually used as the first therapeutic strategy to stop the growth of tumor cells. The effectiveness of this first line of treatment is, however, compromised by observed resistance phenomena. One possible strategy to address this resistance is the use of medication combinations. Fizazi et al.’s study, which examined the use of prednisone and abiraterone acetate in conjunction with androgen deprivation therapy, provided evidence of this. For men with castration-sensitive prostate cancer that has spread, this combination greatly improved overall survival and radiographic progression-free survival. (18).
CLINICAL APPLICATION OF CANCER BIOMARKERS:
Cancer biomarkers have a wide range of therapeutic uses, and precision medicine is their ultimate objective in order to maximize cancer prevention, screening, and treatment methods. Risk assessment, screening and early detection, precise diagnosis, patient prognosis, therapy response prediction, and cancer surveillance and response monitoring are some of these uses. The National Comprehensive Cancer Network Compendium ,the FDA's Table of Pharmacogenomics Biomarkers in Drug Labelling (therapeutic area = oncology) , and the National Cancer Institute's Tumor Marker List , all contain updated lists of biomarkers currently being used in cancer patients. Additionally, a knowledge library called OncoMX was created lately to investigate cancer biomarkers in light of relevant data
These biomarkers are intended to identify cancer in patients who are otherwise healthy and have not displayed any symptoms of illness. In actuality, they are implying the existence of cancer, which requires a different medical diagnosis. Their usage is primarily justified by the fact that the survival rate rises and the likelihood of complications or morbidities falls when cancer is discovered early and asymptomatic. The use of these biomarkers, however, can occasionally result in overdiagnosis, or the identification of a malignancy that would never exhibit any symptoms. In addition to being highly specific— that is, having a very low falsepositive rate—a good screening biomarker assay should ideally be noninvasive and reasonably priced. Among the issues brought on by overdiagnosis and the false-positive rate are more intrusive medical treatments, psychological discomfort in patients, and excessive, needless healthcare system expenses. Numerous blood-based screening biomarkers, such as alpha-fetoprotein for liver cancer, PSA for prostate cancer, CA199 for pancreatic cancer, and CA125 for ovarian cancer, have been or are being utilized in clinical practice. Some of these indicators, such blood PSA screening for prostate cancer, do not, however, meet the high specificity and sensitivity standards. Additionally, we are unable to differentiate between people with benign prostatic hyperplasia and those with malignant prostate cancer using this biomarker. As a result, only men who specifically indicate interest in screening would benefit from the existing PSA-based prostate cancer screening program, which is not desired in a clinical environment. A newly created biomarker panel that combines the filamin-A gene, age, and prostate volume is one of the new tests being evaluated. It performs better than PSA alone, particularly in men with benign hyperplasia. Curiously, promising liquid biopsies for multi-cancer early detection tests are currently being developed to supplement singlecancer screening tests, and they appear to work better.
Diagnostic biomarkers are used to determine a cancer subtype or to confirm the existence of cancer. These biomarkers are helpful because an accurate diagnosis can result in the best possible treatment and, consequently, the highest odds of survival. Whereas some screening biomarkers are also used as diagnostic biomarkers, the latter are only utilized on patients who exhibit symptoms, whereas screening biomarkers are used on people who do not exhibit any symptoms. Diagnostic biomarkers must be used in conjunction with other diagnostic techniques, such as imaging or biopsies, to provide a definitive diagnosis, even though they can aid in the detection of cancer or the subtyping of patients.
After a tumor has been identified, a prognostic biomarker tells us about the likely progression, recurrence, and overall survival of the patient, independent of the treatment. These biomarkers can occasionally indicate the tumor load, which can subsequently be used to determine the cancer's stage (e.g., the tumor–node–metastasis classification). Protein biomarkers like CEA for colorectal cancer, CA19-9 for pancreatic cancer, and CA125 for ovarian cancer are a few examples of commonly used prognostic biomarkers. Other tests based on gene expression profiles for breast cancer include MammaPrint and Prosigna. Additional instances would include the genetic changes linked to patient outcomes that provide a precise risk-stratification of individuals with acute leukemia. Clinicians may find the data gathered from these biomarkers helpful in deciding whether to administer aggressive or protracted therapy. However, as this is better in a clinical situation, several of the prognostic indicators that are currently accessible have also been developed to predict the benefits of chemotherapy.
CONCLUSION
Even while biomarkers are very appealing as screening tests, their relevance for early cancer detection is limited by their low sensitivity and specificity as well as the low incidence of cancer in asymptomatic people. The systematic use of a test to find people who have not sought medical attention because of signs of a particular condition and are at high enough risk to benefit from additional research or direct preventative action is known as screening (1). For screening to be useful, the disease must be identified sooner and treated effectively, and the earlier application of effective treatment must have better results than treatment available when symptoms first appear.(2) The goal of screening is to identify disease or a predisease condition in asymptomatic patients, which is different from diagnosis. There are currently very few screening tests that have been proven to lower cancer mortality. These include the Papanicalaou (PAP) test for cervical cancer screening, fecal occult blood testing (FOBT) for colorectal cancer (CRC) screening, and mammography for breast cancer screening, particularly in women over 50. There are a number of benefits to using biomarkers as cancer screening tests as opposed to techniques like radiography, cytology, and endoscopy (4). Among these benefits are:
1) Blood and urine are biological fluids that may be acquired with little discomfort to screening patients and can be used to detect biomarkers. High rates of compliance should follow from this.
2) automated tests are available for many biomarkers, enabling the processing of a large number of samples in a comparatively short amount of time.
3) Biomarker tests yield objective endpoints and quantitative outcomes.
4)Biomarker assays are reasonably priced.(19).
REFERENCES


Pratiksha Suryawanshi*, Neha Kadam, A Comprehensive Review on the Clinical Significance of Cancer Biomarkers, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 1887-1900 https://doi.org/10.5281/zenodo.17591038
 10.5281/zenodo.17591038
10.5281/zenodo.17591038
