Kasturi Shikshan Sanstha College of Pharmacy, Shikrapur, Shirur, Pune 412208
The COVID-19 pandemic, caused by SARS-CoV-2, represents an unprecedented global health crisis with over 700 million confirmed cases and 7 million reported deaths, with excess mortality estimates suggesting 14.9-33.5 million deaths worldwide [88,90]. The virus demonstrates remarkable evolutionary capacity, with major variants (Alpha, Beta, Gamma, Delta, and Omicron sublineages) exhibiting progressively enhanced transmissibility and immune evasion through specific spike protein mutations including N501Y, L452R, E484K, and others [93]. The pandemic has transitioned from acute emergency phase to endemic state with persistent viral circulation. Molecular characterization reveals SARS-CoV-2 as a positive-sense single-stranded RNA beta coronavirus of approximately 29.9 kb, encoding 29 viral proteins organized into two large replicase ORFs and structural genes . Pathophysiology involves complex interactions between viral virulence factors and host immune responses, with severe disease characterized by hyperinflammatory "cytokine storm" involving elevated IL-6, TNF-?, IL-1?, and IFN-?, leading to lymphopenia, vascular leakage, thrombo-inflammatory complications, and multiorgan dysfunction[65,71]. Diagnosis relies on RT-PCR as gold standard (94.7-100% sensitivity, 99-100% specificity) supplemented by rapid antigen tests (7085% sensitivity) and serological antibody detection [28,40]. Pharmaceutical interventions include antiviral agents (remdesivir, Paxlovid, molnupiravir) demonstrating 70-89?ficacy in reducing disease progression [91], immunomodulatory therapies (dexamethasone reducing mortality 20- 33%, tocilizumab reducing ICU admission, baricitinib reducing progression), and anticoagulation strategies for thrombotic complications [29,71,89]. Prevention strategies including mask wearing, social distancing, hand hygiene, ventilation improvement, and testing surveillance remain essential components of pandemic control, particularly in indoor congregate settings where airborne transmission predominates[46,52,69,72]. This review synthesizes comprehensive evidence across virology, immunology, epidemiology, clinical medicine, and pharmaceutical sciences essential for contemporary healthcare practice and pandemic preparedness.
The COVID-19 pandemic began with emergence of a novel coronavirus in Wuhan, China, in December 2019, subsequently designated SARS-CoV-2[88]. Initial cases presented with severe pneumonia of unknown etiology; rapid molecular identification confirmed a novel coronavirus distinct from previously known species [88]. The virus exhibits 82% sequence identity to SARS CoV and 90%+ identity in essential enzymes and structural proteins. The first confirmed international cases were documented in January 2020, initiating rapid global dissemination [88]. By March 2020, the WHO declared COVID-19 a pandemic due to its rapid spread across six continents affecting virtually every nation within months. The pandemic has evolved through distinct phases: (1) Initial phase (2020) with overwhelming caseloads, healthcare system strain, and rapid scientific knowledge accumulation; (2) Variant emergence phase (2021) featuring Alpha, Beta, Gamma, Delta variants alongside vaccine introduction; (3) Omicron dominance phase (20222023) with increased transmissibility, reduced severity, and breakthrough infections in vaccinated populations; (4) Endemic transition phase (2024-2025) demonstrating variant circulation similar to influenza with available therapeutics and vaccines[88,95].
Scientific and Clinical Significance
Understanding COVID-19 comprehensively requires synthesis of knowledge across virology, immunology, epidemiology, pharmacology, clinical medicine, and public health. For pharmaceutical sciences students and healthcare professionals, this comprehensive knowledge enables: designing novel antiviral agents through understanding viral replication mechanisms and identifying conserved enzymatic targets; developing effective vaccines by understanding immune responses and mechanisms of immune evasion; optimizing therapeutic drug selection and dosing in various disease stages; interpreting diagnostic test results; and appreciating pandemic preparedness importance.
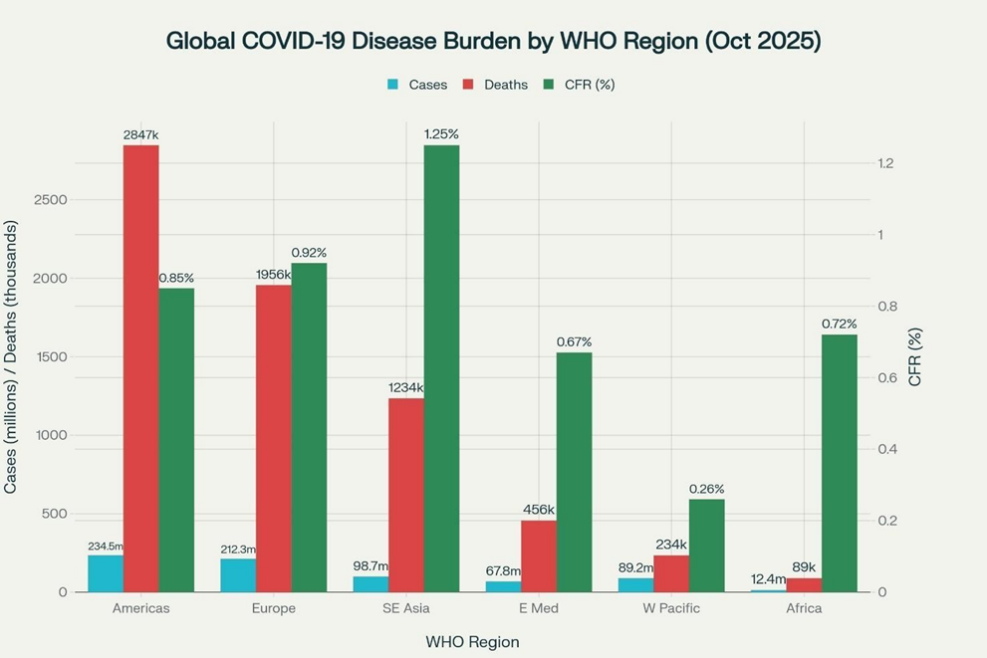
The United States reported the highest absolute case numbers (>103 million) and deaths (>858,000) as of early 2024[90]. Brazil, the second most affected nation by case count, reported 37.8 million cases and 703,324 deaths by October 2025[90]. European countries collectively reported substantial case and death burdens. Regional variations showed Europe with cumulative incidence of 14,039.95 per 100,000, Americas with highest death rate of 241.63 per 100,000[27,88]. Profound socioeconomic disparities emerged, with high-income nations achieving highest case detection but upper-middle-income countries demonstrating highest per capita death rates, reflecting diagnostic disparities, limited treatment access, and healthcare system vulnerabilities[27,92].
Molecular Virology And Genomic Structure
Viral Classification and Structural Organization
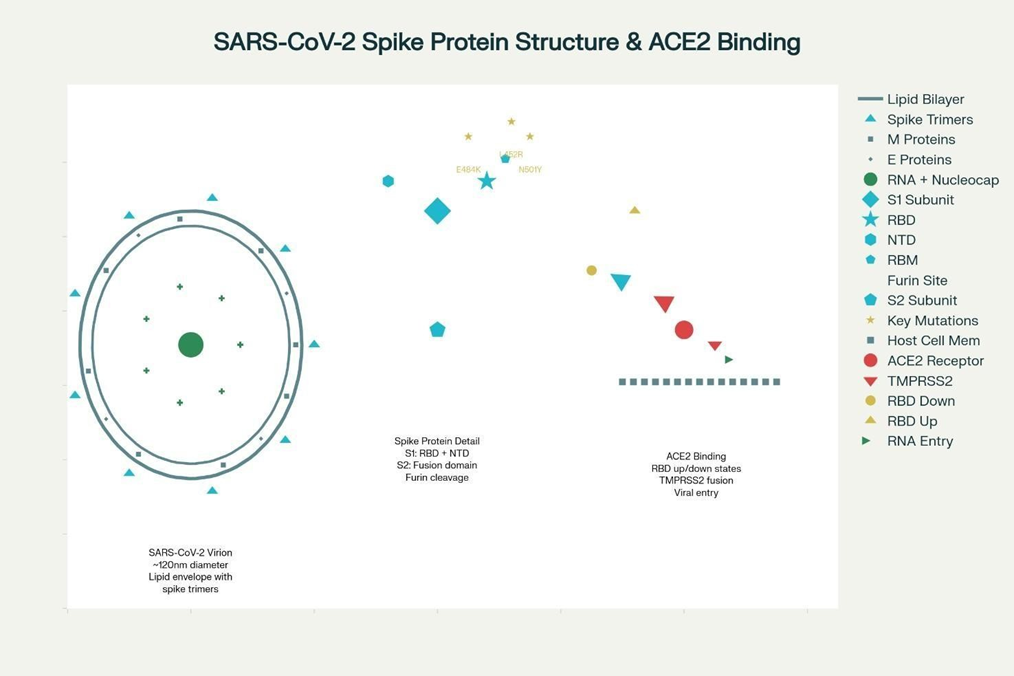
SARS-CoV-2 belongs to family Coronaviridae, subfamily Coronavirinae, genus Beta coronavirus, including important human and animal pathogens. The virus demonstrates phylogenetic relationships to SARS-CoV (82% identity) and MERSCoV, though represents distinct species. Structurally, SARS-CoV-2 presents as spherical, enveloped virion measuring 60-140 nanometers in diameter, exhibiting characteristic crown-like appearance from spike glycoproteins protruding from surface.
Each virion contains lipid bilayer envelope derived from host cell membrane with embedded viral structural proteins. The envelope contains approximately 8-12 spike protein trimers per virion with embedded membrane (M) and envelope (E) proteins. The viral interior contains RNA genome complexed with nucleocapsid proteins forming helical ribonucleoprotein structure.
GENOMIC ORGANIZATION:
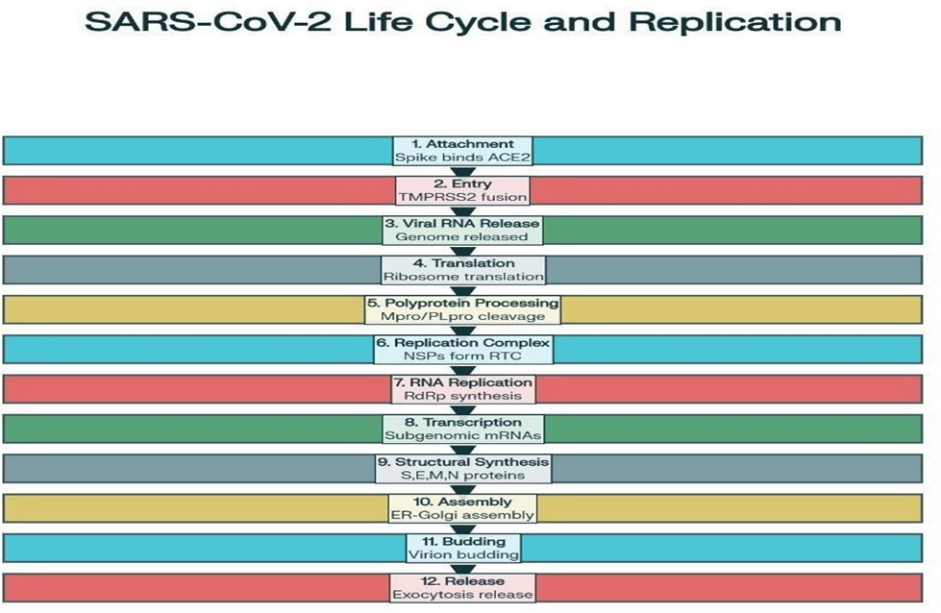
The SARS-CoV-2 genome comprises positive-sense single-stranded RNA of approximately 29,863 nucleotides, making it one of the largest known RNA viral genomes. Genome organization follows canonical coronavirus pattern: 5' UTR, replicase genes (ORFs 1a and 1b), structural protein genes (S, E, M, N), accessory protein genes, and 3' UTR. The genome encodes 13-15 open reading frames collectively encoding approximately 29 viral proteins. The two large overlapping ORFs 1a and 1b, occupying ~66% of 5' end, encode polyproteins of ~440 kDa (pp1a) and ~740 kDa (pp1ab). These polyproteins undergo post-translational processing by viral proteinases to generate 16 non-structural proteins (NSPs 1-16) essential for replication and transcription[16].
The 16 non-structural proteins generated from polyprotein processing perform diverse essential functions in viral replication [16]. Key NSPs include:
Assembly of NSPs into replication-transcription complex (RTC) enables efficient genome replication and sub genomic mRNA synthesis for structural protein production
Spike Protine Structure And Function
The spike protein exists as homotrimer, representing primary viral attachment and fusion protein[16]. Each monomer can be cleaved into S1 subunit (containing RBD and NTD) and S2 subunit (mediating membrane fusion [16]. The RBD comprises ~193 amino acids with core five-stranded β-sheet structure [16].
The receptor-binding motif (RBM) extends in cradle-like conformation from RBD core, directly contacting human ACE2 receptor[16]. The RBD adopts two conformational states: "down" (closed) state shielding receptor-binding regions, limiting antibody access; and "up" (open) state exposing RBM and facilitating ACE2 recognition[16]. Dynamic transitions between conformational states influence both viral infectivity and antibody neutralization capacity.
The spike protein contains polybasic furin cleavage site (RRAR↓S) at S1/S2 junction, absent in SARS-CoV and MERS-CoV, facilitating efficient cleavage by ubiquitous cellular furin proteases and potentially contributing to SARS-CoV-2's enhanced transmissibility.
MAJOR VARIANTS OF CONCERN AND CHARACTERISTICS
Alpha Variant
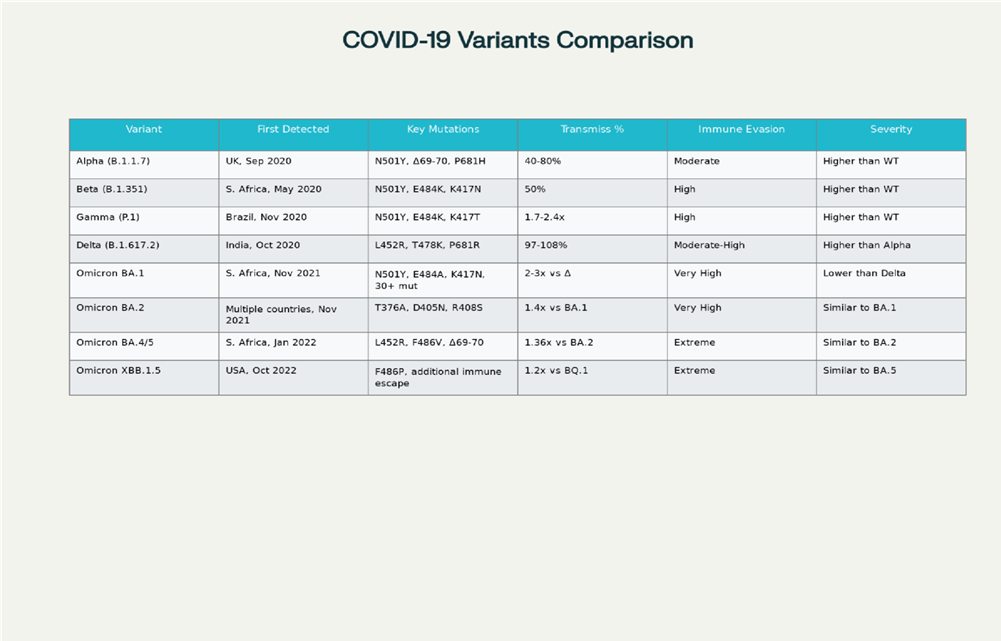
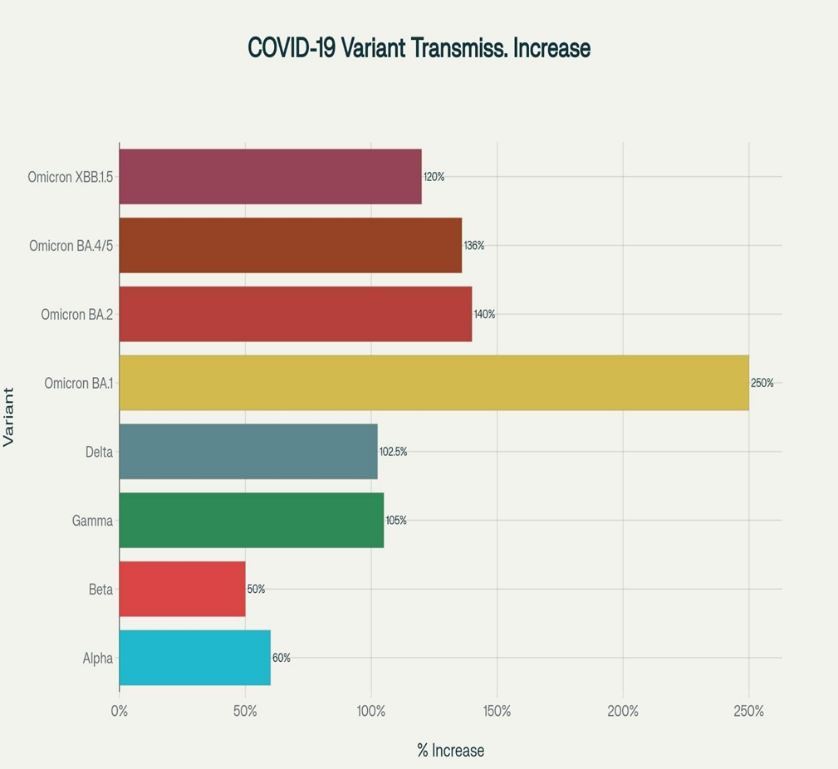
First detected in United Kingdom in October 2020, the Alpha variant represented the first substantially more transmissible variant than original Wuhan strain [88]. This variant harbored eight key spike protein mutations, most notably N501Y in RBD increasing ACE2 binding affinity, H69/V70 deletion (ΔH69/V70) in NTD, and P681H near furin cleavage site [88]. These mutations collectively conferred 40-80% increased transmissibility, with most estimates concentrating toward higher range. Alpha was associated with increased cell-to-cell fusion activity and enhanced viral protein upregulation contributing to increased infectivity. The variant spread to over 120 countries by May 2021 before being outcompeted by more transmissible Delta variant [1][8].
Beta And Gamma Variant
The Beta variant, identified in South Africa in May 2020, demonstrated significant immune evasion properties through three critical mutations: K417N, E484K, and N501Y[88]. The E484K mutation in RBD proved particularly effective at reducing antibody neutralization, earning designation as "escape mutation’’.
Combination of K417N and N501Y enhanced ACE2 binding while facilitating antibody evasion. Beta exhibited approximately 50% increased transmissibility. The variant demonstrated higher hospitalization rates and greater disease severity than Alpha and Gamma variants. By early 2021, Beta had spread to over 120 countries, though eventually outcompeted by Delta [1,8,9]
The Gamma variant emerged in Brazil between November and December 2020, harboring 17 mutations including three critical spike changes: K417T, E484K, and N501Y [1,9]. These conferred 1.7-2.4 fold increased transmissibility and higher viral loads [1]. Gamma rapidly became dominant in Brazil, responsible for 96% of cases by mid-2021 before being supplanted by Delta. The variant demonstrated substantial immune evasion capabilities, particularly against antibodies from previous infection with earlier strains [9].
Delta Variant
Delta, first detected in India in October 2020, became globally dominant by September 2021 due to exceptional transmissibility and immune evasion [1,9,8]. Key spike protein mutations included L452R and T478K in RBD and P681R near furin cleavage site. The
L452R mutation increased spike-ACE2 binding affinity and reduced neutralizing activity of many monoclonal antibodies and vaccine-induced antibodies [63]. The T478K mutation further enhanced ACE2 binding while facilitating immune escape.
Additional mutations included D614G and E484Q.
Delta exhibited 97-108% increased transmissibility compared to Alpha, with some analyses suggesting R0 of 5-7[64]. The variant demonstrated 21-fold higher relative replication rate compared to earlier variants and enhanced infectivity in human lung cells and animal models [64]. Delta showed 21% higher relative replication rate than Alpha and ~1.5-fold advantage over Gamma. The variant's enhanced replication in airway epithelial cells combined with increased resistance to neutralizing antibodies contributed to classification as most concerning pre-Omicron variant [21].
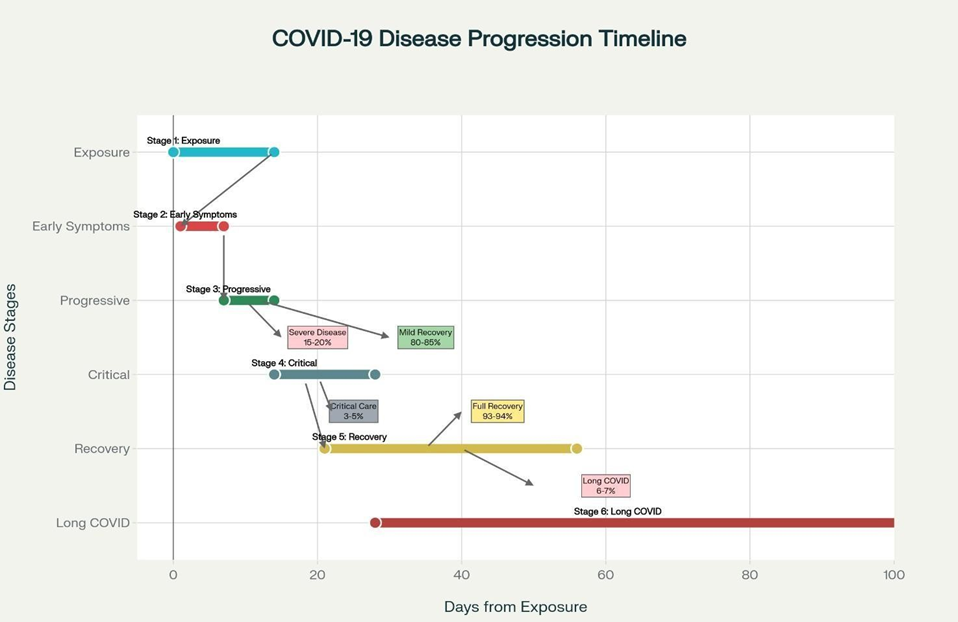
Phases of COVID-19 Disease Progression
COVID-19 pathogenesis can be conceptualized in distinct phases:
GLOBAL DISEASE BURDEN AND MORTILITY
As of October 2025, COVID-19 resulted in 700+ million confirmed cases globally with 7 million confirmed deaths [88,90]. These official figures substantially underestimate true disease burden. Excess mortality estimates comparing observed to expected baseline deaths range from 14.9 to 33.5 million deaths worldwide [88,92]. The United States reported highest absolute case numbers (>103 million) and deaths (>858,000) [90]. Brazil documented 37.8 million cases and 703,324 deaths [90]. Regional disparities were pronounced: Europe demonstrated cumulative incidence of 14,039.95 per 100,000, Americas highest death rate of 241.63 per 100,000[ 27].
Socioeconomic disparities profoundly influenced disease burden. High-income countries recorded highest case detection rates (42,742.51 per 100,000) reflecting testing capacity, while upper-middle-income countries demonstrated highest death rates (619.14 per 100,000) suggesting limited medical resources and healthcare access [27]. Low-income countries reported lowest case rates likely reflecting underreporting rather than lower disease burden [21].
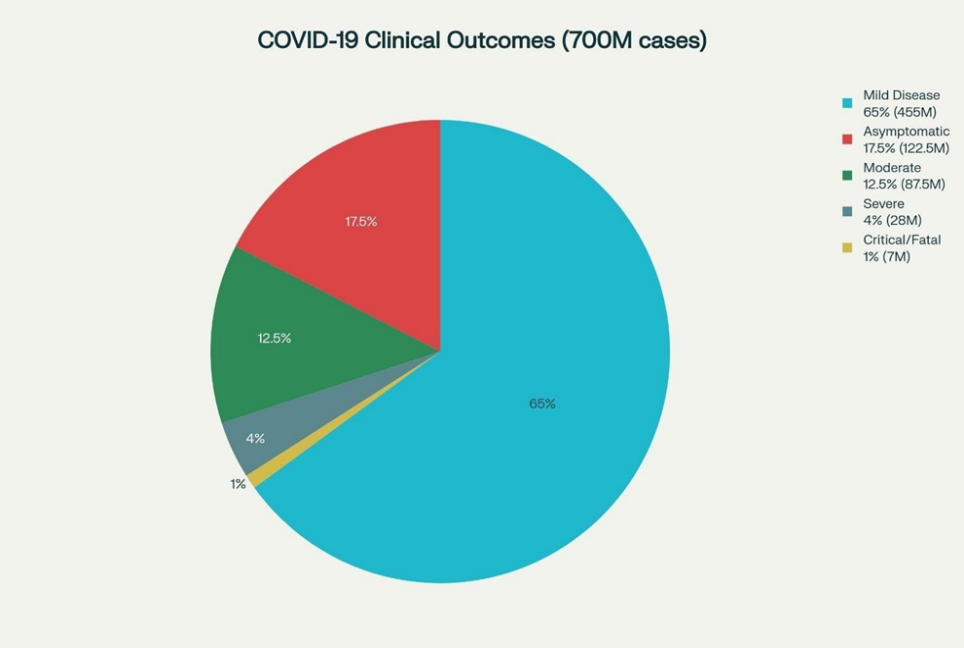
COVID-19 exhibits extraordinarily wide clinical spectrum ranging from asymptomatic infection to critical illness requiring intensive care and mechanical ventilation [18]. Incubation period typically spans 2-14 days with median 5-6 days from exposure to symptom onset [12]. Common acute phase symptoms include fever, dry cough, sore throat, fatigue, myalgia, headache, and dyspnea [18]. Additional frequently reported symptoms encompass anosmia, dysgeusia, nasal congestion, diarrhea, nausea, vomiting, and abdominal pain [48].
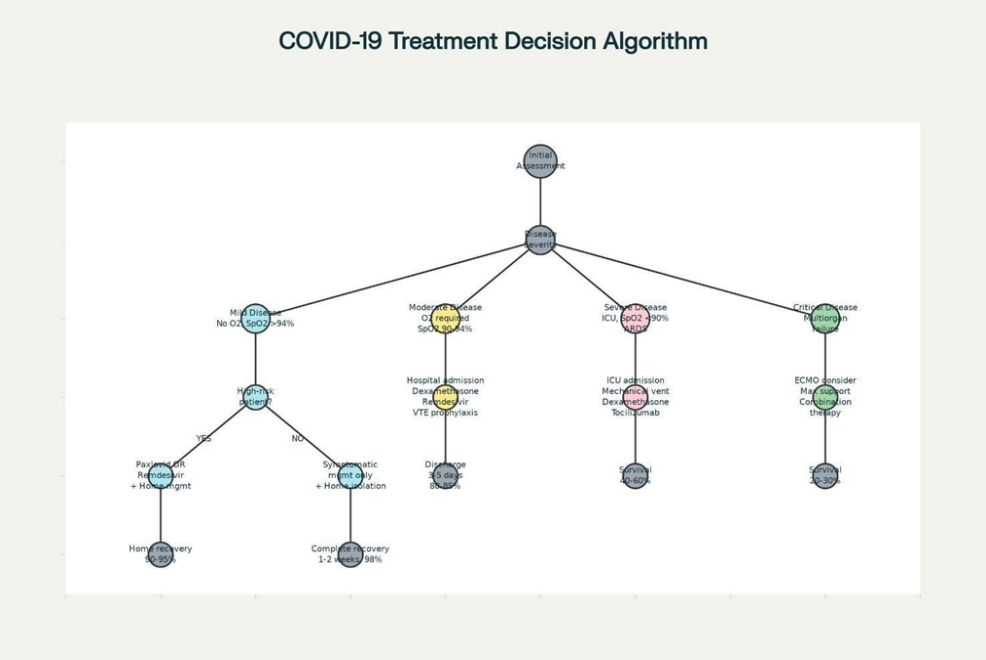
Mild cases, representing 80-85% of infections, resemble common upper respiratory infections with symptoms typically resolving within 1-2 weeks without specific interventions [18]. Moderate disease, accounting for 10-15% of cases, involves evidence of lower respiratory tract involvement with confirmed pneumonia without significant hypoxemia [18]. Severe disease, representing ~5% of infections, is characterized by severe pneumonia with hypoxemia (SpO2 <90% on room air), respiratory rate >30 breaths/minute, or lung infiltrates affecting >50% of lung fields within 24-48 hours [18]. Critical illness, occurring in 1-5% of infections, manifests as ARDS, sepsis, septic shock, multiorgan dysfunction, or other life-threatening complications requiring ICU admission [18]
DIAGNOSTIC METHODOLOGIES
Molecular Testing: RT-PCR
RT-PCR remains gold standard for COVID-19 diagnosis, offering highest sensitivity and specificity among available modalities [ 31]
Testing involves reverse transcription of viral RNA from respiratory samples (typically nasopharyngeal or oropharyngeal swabs) into cDNA, followed by specific viral gene sequence amplification using PCR technology [31].
Most commonly targeted genes include envelope (E) gene, RNA-dependent RNA polymerase (RdRp) gene, and nucleocapsid (N) gene [31]. E gene-based assay serves as first-line screening test due to high sensitivity, RdRp gene provides confirmatory testing, and N gene offers additional confirmation when needed [31].
Clinical studies documented RT-PCR sensitivity ranging from 94.7% to near 100%, with specificity of 99-100% [28,40]. RTPCR can detect viral RNA even before symptom onset, enabling early diagnosis and isolation of infected individuals [34]. However, several limitations exist: specialized equipment and trained personnel required, relatively long turnaround times (1-2 days or longer), higher cost compared to rapid tests, and false-negative possibilities from inadequate sampling, timing issues, viral mutations, or laboratory errors [31,40].
Rapid Antigen Testing
Rapid antigen tests detect specific viral proteins from respiratory specimens, typically nasal or nasopharyngeal swabs, providing results within 15-30 minutes [25,34]. Tests utilize immunochromatographic assays (lateral flow assays) similar to home pregnancy tests where sample migrates along test strip producing visible line if viral antigens present [28,31].
Advantages include rapid turnaround, lower cost than RT-PCR, minimal equipment requirements enabling decentralized testing, and ease of use allowing deployment in diverse settings [25,28]. However, antigen tests demonstrate lower sensitivity than RT- PCR, typically 70-85%, particularly in asymptomatic individuals or those with low viral loads [25,28]. Specificity generally ranges from 95-99% [25,28]. The reduced sensitivity means negative antigen test results, especially in symptomatic individuals or known exposures, may require RT-PCR confirmation [25,34].
Antigen tests perform best when viral loads are highest, typically within first 5-7 days of symptom onset or shortly before symptom development in pre symptomatic individuals [28]. Studies indicate antigen tests are approximately 100 times less sensitive than RTPCR, with limits of detection around 10,000 viral copies/mL compared to 1,000 copies/mL for PCR [40].
Serological Antibody Testing
Antibody tests detect immunoglobulins (IgM and IgG) produced in response to SARSCoV-2 infection or vaccination, typically using ELISA or CLIA methodologies with blood samples [25,34]. IgM antibodies typically appear 5-7 days after infection onset, reach peak levels at 2-3 weeks, and decline thereafter, while IgG antibodies develop 7-14 days post-infection and persist for months to years [34].
Antibody tests exhibit sensitivity ranging from 85-95% and specificity of 90-98%, though performance varies depending on testing timing relative to infection or vaccination, specific assay used, and target antigens [25,34]. Primary clinical utility lies in identifying past infection for epidemiological surveillance, determining seroprevalence in populations, screening blood donors, and assessing immune status [25,34].
Antibody tests have limited value for diagnosing acute infection, as antibodies may not be detectable during early symptomatic phase when patients typically present for care [25,34]. Antibody testing has proven valuable for large-scale epidemiological studies understanding true SARS-CoV-2 spread extent in communities and guiding public health interventions [25,34].
PHARMACEUTICAL TREATMENT MODALITIES
Antiviral Agents
Remdesivir (Veklury)
Remdesivir, a nucleotide prodrug inhibiting viral RNA-dependent RNA polymerase, became the first FDA-approved antiviral agent specifically for COVID-19 treatment.
Active metabolite, an adenosine analog, binds to viral RdRp and inhibits viral replication through premature RNA transcription termination [29]. Remdesivir is administered intravenously at 200 mg loading dose on day 1, followed by 100 mg daily, with typical treatment course of 3-5 days [29,35]. For pediatric patients weighing <40 kg, dosing is weight-based: 5 mg/kg loading dose followed by 2.5 mg / kg daily [26]. FDA and major clinical guidelines recommend remdesivir for mild-to-moderate COVID-19 in both hospitalized and non-hospitalized adults and pediatric patients at high progression risk [29,35]. For hospitalized patients requiring supplemental oxygen, guidelines recommend co-administration with dexamethasone to optimize outcomes. Clinical studies demonstrated remdesivir reduces hospitalization rates and accelerates recovery time in appropriately selected patients [29,35].
Common adverse effects include nausea, liver transaminase elevation, and prothrombin time prolongation [29]. Remdesivir is contraindicated in patients with severe renal impairment (eGFR <30 mL/min) and requires dose adjustment in patients with eGFR 3060 mL/min [29]. Concomitant use with chloroquine or hydroxychloroquine is not recommended as these agents reduce remdesivir antiviral effectiveness [29].
Nirmatrelvir-Ritonavir (Paxlovid)
Paxlovid, combining nirmatrelvir (SARS-CoV-2 main protease inhibitor) and ritonavir (CYP3A4 inhibitor boosting nirmatrelvir levels), represents the first oral antiviral granted full FDA approval for COVID-19[26][29][32][35]. Nirmatrelvir blocks viral main protease (Mpro/3CLpro) activity, essential for viral polyprotein cleavage, thereby halting viral replication [29,32].
Ritonavir, originally developed as HIV protease inhibitor, serves pharmacoenhancer role by inhibiting cytochrome P450-3A4 enzyme, slowing nirmatrelvir metabolism and allowing convenient twice-daily dosing [29,32]. FDA and current guidelines recommend Paxlovid for non-hospitalized adults and pediatric patients (≥12 years and ≥40 kg) with mild-to-moderate COVID-19 at high progression risk . Treatment must be initiated as soon as possible, within 5 days of symptom onset [32,35].
Clinical trials demonstrated Paxlovid reduces disease progression by approximately 89% [89]. Standard dosing regimen consists of nirmatrelvir 300 mg (two 150 mg tablets) co-administered with ritonavir 100 mg (one tablet) twice daily for 5 days [32]. Dose adjustment required for moderate renal impairment (eGFR 30-60 mL/min), reducing to nirmatrelvir 150 mg with ritonavir 100 mg twice daily [29,32]. Paxlovid not recommended for eGFR <30 mL/min or severe hepatic impairment [29,32].Common adverse effects include dysgeusia (metallic taste resolving after treatment), diarrhea, hypertension, and myalgia [29]. Major limitation involves numerous drug drug interactions due to ritonavir's potent CYP3A4 inhibition, potentially affecting statins, anticoagulants, anticonvulsants, immunosuppressants, and antiarrhythmics.
Molnupiravir, oral ribonucleoside analog inhibiting viral RNA polymerase through lethal mutagenesis induction, received Emergency.
VACCINATION STRATEGIES AND IMMUNOLOGY
mRNA Vaccines
Mechanism of Action: mRNA vaccines developed by Pfizer-BioNTech (BNT162b2) and Moderna (mRNA1273) represent groundbreaking messenger RNA technology applications for vaccination [44,50]. These vaccines contain nucleoside- modified mRNA encoding SARS-CoV-2 spike glycoprotein, specifically S2-P antigen consisting of full-length spike protein with transmembrane anchor and proline substitutions stabilizing protein in prefusion conformation [47].
The mRNA is encapsulated in lipid nanoparticles (LNPs) composed of ionizable cationic lipids, phospholipids, cholesterol, and polyethylene glycol-lipid conjugates, protecting fragile mRNA from degradation and facilitating host cell delivery [44,47]. Following intramuscular injection (typically deltoid muscle), LNPs fuse with cell membranes, releasing mRNA into muscle cell and antigen presenting cell cytoplasm including dendritic cells [53].
Host cell ribosomes translate mRNA to produce spike protein, which is then displayed on cell surface [53]. The immune system recognizes spike protein as foreign, triggering robust adaptive immune response including B cell activation differentiating into plasma cells producing spike-specific neutralizing antibodies (particularly targeting RBD) and CD4+ helper T cells and CD8+ cytotoxic T cell activation [47]. Importantly, mRNA never enters cell nucleus, does not integrate into host genome, and is rapidly degraded and cleared from body within days, leaving no permanent genetic changes [53].
Pathophysiological Mechanisms
Long COVID mechanisms remain incompletely understood, likely involving multiple interacting processes varying among individuals [45,54]. Proposed mechanisms include: (1) lasting organ and tissue damage from acute SARS-CoV-2 infection, particularly relevant for severe disease patients requiring ICU care, hypoxemia, or mechanical ventilation [48,54]; (2) persistent viral reservoirs with viable virus or viral RNA in various tissues including gut, lymph nodes, nervous system months postacute infection [54]; (3) immune dysregulation and chronic inflammation with persistent pro- inflammatory cytokine elevation, ongoing primed immune cell activity, and altered immune phenotypes [48,54]; (4) autoimmunity from molecular mimicry between viral and self-antigens, producing autoantibodies against various tissues [54]; (5) latent virus reactivation including Epstein-Barr, cytomegalovirus, and herpesviruses under COVID-induced immune dysregulation[48]; (6) endothelial dysfunction and microvascular damage with ongoing coagulopathy causing microthrombi in small vessels[54]; and (7) mitochondrial dysfunction from downregulated core mitochondrial genes during acute COVID [48].
CONCLUSION
The COVID-19 pandemic, caused by SARS-CoV-2, represents an unprecedented global health crisis profoundly impacting healthcare systems, economies, and societies worldwide. The pandemic has evolved through distinct phases from the initial 2020 emergence through variant-dominated 2022-2023 to the current endemic transition phase (2024-2025) with ongoing viral circulation, available therapeutics, and established vaccination programs [88,95].
Pharmacovigilance studies of COVID-19 vaccines involve systematic surveillance and monitoring of vaccine safety profiles, adverse event reporting, and potential long-term effects in vaccinated populations [41,47]. Post-marketing surveillance systems including adverse event reporting databases continuously evaluate vaccine safety while identifying rare adverse events [47]. Pharmacovigilance enables rapid signal detection for potential safety concerns, risk stratification for specific populations, characterization of adverse event frequencies and severities, and comparative safety assessment across vaccine platforms [41,47]. Major pharmacovigilance findings include identification of vaccine-induced immune thrombotic thrombocytopenia (VITT) associated with adenoviral vector vaccines and myocarditis predominantly in young males following mRNA vaccines [47].
Molecular characterization of SARS-CoV-2 reveals a positive-sense single-stranded RNA beta coronavirus encoding approximately 29 viral proteins organized into replicase and structural genes, with non-structural proteins performing critical roles in viral replication and immune evasion [16]. The spike protein, with its receptor binding domain interacting with human ACE2 receptors and its susceptibility to mutations, has emerged as the primary determinant of viral transmissibility and immune evasion [3].
The rapid evolution of SARS-CoV-2 has produced multiple variants of concern, each exhibiting distinct characteristics [93]. Alpha variant (B.1.1.7) demonstrated 4080% increased transmissibility; Beta (B.1.351) and Gamma (P.1) showed significant immune evasion properties; Delta (B.1.617.2) achieved 97-108% transmissibility with R0 estimated 5-7; Omicron variants demonstrated unprecedented immune evasion with BA.1 showing 2-3x Delta transmissibility; and Omicron sub lineages including XBB.1.5 demonstrated extreme immune escape with 41-fold resistance to bivalent vaccine sera [64,93].
Global disease burden remains enormous, with over 700 million confirmed cases and 7 million reported deaths, though excess mortality estimates suggest 14.9-33.5 million actual deaths [88,92]. Regional and socioeconomic disparities in disease burden and healthcare access remain profound, with high-income nations achieving highest case detection but upper-middle-income countries demonstrating highest per capita mortality [27,88].
Pathophysiology of COVID-19 involves complex viral-host interactions including spike-ACE2 binding-mediated entry, viral replication in respiratory and multiple organ systems, hyperinflammatory "cytokine storm" with IL-6 and TNF-α overproduction, lymphopenia with immune dysfunction, thrombo inflammatory complications, endothelial damage, and potential multiorgan failure in severe disease [65,71].
Diagnostic methodologies include RT-PCR as the gold standard (94.7-100% sensitivity, 99-100% specificity), rapid antigen tests (7085% sensitivity), serological antibody detection (85-95% sensitivity), and imaging techniques [28,40]. Each testing modality offers distinct advantages and limitations guiding clinical application selection. The COVID-19 pandemic has served as a clarion call regarding humanity's vulnerability to emerging infectious diseases and simultaneous capacity for scientific innovation and collective action confronting existential health threats. The pharmaceutical sector has played pivotal role in pandemic response through unprecedented rapid vaccine and therapeutic development, underscoring critical importance of pharmaceutical sciences in addressing global health threats. Pharmaceutical students and future healthcare professionals must understand COVID19 comprehensively across molecular virology, immune responses, diagnostic approaches, therapeutic applications, and global health implications to contribute effectively to pandemic response and future pandemic preparedness. As COVID-19 transitions from pandemic to endemic phase, sustained vigilance, adaptive strategies, and continued scientific inquiry remain essential for minimizing disease burden and protecting vulnerable populations. The lessons learned from COVID-19— regarding viral evolution, vaccine and therapeutic development timelines, public health coordination, health equity, and pandemic preparedness—will shape public health strategies for generations to come, serving as sobering reminder of collective responsibility in confronting emerging infectious disease threats to global health and human wellbeing.
REFERENCE


Kalyani Takale, Snehal Kadbhane, Dr. Vijaykumar Kale, A Comprehensive Review on Covid-19 and its Variants, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 11, 4172-4185. https://doi.org/10.5281/zenodo.17722774
 10.5281/zenodo.17722774
10.5281/zenodo.17722774
