Anuradha College of Pharmacy, Chikhli, Buldhana, Maharashtra 443001
Convulsions, or seizures, are defined as sudden, involuntary, and violent muscle contractions resulting from various underlying conditions, most notably seizures themselves, but also including high fevers, head injuries, infections, and exposure to certain toxins. Although convulsions and seizures are often conflated, they are not interchangeable; seizures pertain to abnormal electrical activity in the brain and can present in several forms, including absence seizures, which are characterized by a brief lapse in awareness without muscle contractions. A convulsion is marked by uncontrollable muscle contractions and spasms, leading to abrupt and jerky movements, and may affect specific body areas or the entire body, with durations ranging from seconds to minutes. Tonic-clonic seizures are primarily responsible for convulsions, while numerous seizure types do not result in this physical manifestation, further underscoring the distinction. It is crucial to implement early, evidence-based treatment strategies to prevent mortality and complications associated with prolonged status epilepticus (SE). Benzodiazepines are recognized as the most effective first-line therapy for SE, though they are frequently under-dosed. Alternatives for second-line treatment include levetiracetam, fosphenytoin, or valproic acid, all demonstrating equivalent efficacy in managing established SE. In scenarios where patients develop refractory or super-refractory SE, inducing an anaesthetic coma may be necessary, although there exists a lack of high-quality evidence to guide the selection of anaesthetic agents, the depth and duration of the coma, EEG treatment targets, and strategies for weaning off anaesthesia. Recent investigations suggest that ketamine may effectively terminate status epilepticus, although definitive proof from prospective comparative studies remains absent. Understanding the aetiology of SE is essential as it is a significant predictor of patient outcomes and should inform therapeutic approaches. If an immunological etiology is suspected, prompt empiric treatment with immunomodulatory drugs is recommended.
Convulsions or Seizures are defined as sudden, involuntary, and violent muscle contractions that can arise due to various underlying conditions, most commonly seizures, but also high fevers, head injuries, infections, and exposure to certain toxins (1, 2). It is important to note that while convulsions are often associated with seizures, the two are not synonymous; seizures refer to abnormal electrical activity in the brain, which can manifest in forms other than convulsions, such as absence seizures where a person may not exhibit any muscle contractions but instead becomes momentarily unresponsive. A convulsion is characterized by uncontrollable muscle contractions and spasms, resulting in abrupt and jerky movements (3, 4). This phenomenon is caused by disruptions in normal nerve cell activity in the brain and can engage specific body parts or the entire body, with durations varying from seconds to several minutes. Seizures that commonly result in convulsions include tonic-clonic (formerly known as grand mal) seizures, while it is crucial to understand that not all seizure types cause convulsions. For instance, absence seizures lead to a brief lapse in awareness without physical shaking (5-7). The common causes of convulsions encompass:
In terms of medical intervention, it is imperative to seek immediate help if A convulsion is the individual's first occurrence. The convulsion persists beyond five minutes. Injury occurs during the convulsion. The individual has pre-existing heart conditions or is known to be pregnant. There is no return to normal consciousness post-event. Given the complexities surrounding convulsions and seizures, medical consultations are vital for accurate diagnosis and treatment planning, potentially requiring the expertise of neurologists or specialists in infectious diseases (8-10).
2. TYPES OF CONVULSIONS OR SEIZURES
Seizures are broadly classified based on where they begin in the brain and the person's level of awareness during the event. Convulsions, which are physical jerking movements, are a type of motor symptom most notably associated with tonic-clonic seizures (Figure 1). The main classifications are focal onset and generalized onset seizures, with a third category for unknown onset (11-14).
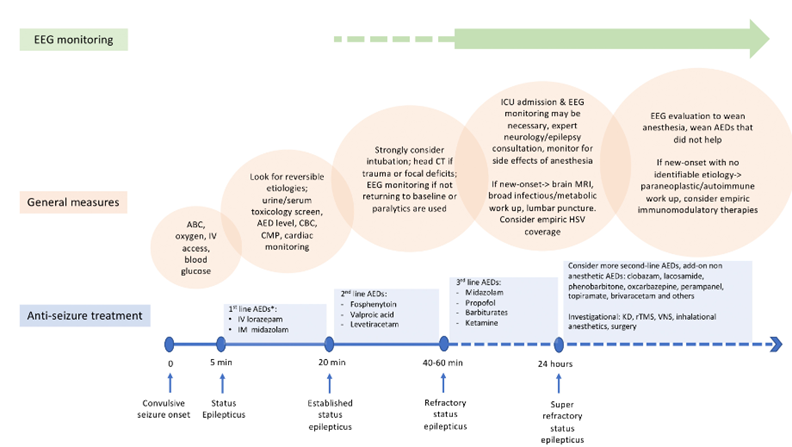
Figure 1: Types of Convulsions or Seizures
2.1 Focal Onset Seizures
2.2 Generalized Onset Seizures
These seizures involve electrical activity that begins on both sides of the brain at the same time and typically cause a loss of consciousness (15, 16).
2.3 Unknown Onset Seizures
Sometimes, due to lack of witnesses or inadequate information, the start of the seizure cannot be determined. These are classified as unknown onset seizures until more information is available. If a seizure lasts longer than 5 minutes or a person does not fully recover between seizures, it is a medical emergency known as status epilepticus, and emergency services should be called immediately (17-19).
3. MANAGEMENT OF CONVULSIONS OR SEIZURES
In the management of patients with prolonged clinically apparent or convulsive seizures, families of the affected individuals and emergency medical services play a critical initial role. It is vital to document the onset time of seizures when known, as this information assists in guiding subsequent treatment stages. The initial five minutes of seizure activity, referred to as the 'stabilisation phase,' necessitate the application of an ABC approach—addressing airway, breathing, and circulation—while also ensuring environmental safety to mitigate the risk of injury. In cases of convulsions, it is important to consider the possibility of psychogenic non-epileptic seizures. A simultaneous assessment for conditions that might trigger or prolong seizures is crucial. This includes the initiation of monitoring oxygen saturation and cardiac function, given that hypoxia and cardiac complications frequently occur during such medical emergencies. Laboratory tests such as blood glucose levels, toxicological screening, and serum levels of antiepileptic drugs (AEDs) are essential for identifying easily reversible causes of status epilepticus and should be obtained while establishing intravenous access. Special attention should be given to patients with suspected alcohol use, who should receive intravenous thiamine to prevent complications. Additionally, it is common for subtherapeutic AED levels to result from non-compliance or interactions among medications, which can be triggers for seizures in individuals with epilepsy (18, 20).
3.1 First Line Therapy
Seizures that persist for over 5 minutes or recur without recovery intervals are classified as early status epilepticus, necessitating immediate first-line treatment. Clinical trials support the efficacy of pre-hospital benzodiazepine administration, with the specific drug choice influenced by factors such as availability in the field and the presence of intravenous (IV) access. First-line treatment options include IV lorazepam (0.1 mg/kg, maximum 4 mg), IV diazepam (0.15–2 mg/kg, maximum 10 mg), intramuscular or buccal midazolam (10 mg, reduced to 5 mg for older patients or those weighing less than 40 kg), and rectal diazepam (10 mg, reduced to 5 mg for similar populations). In some European regions, IV clonazepam (0.015 mg/kg, maximum 1 mg) is also employed. If seizures persist for 5 minutes after the initial dose of benzodiazepines, a second dose should be administered. While IV benzodiazepines generally provide a rapid onset of action, alternative routes (like intranasal midazolam and lorazepam) can achieve similar cessation times when accounting for speed of administration. Key considerations in treatment include drug availability, appropriate dosing, and administration timing, as under-dosing is a common issue. Studies indicate that administering adequate doses of benzodiazepines may reduce the need for tracheal intubation. Once seizure activity exceeds 5 minutes post maximum/last benzodiazepine dose without intervals of recovery—which occurs in approximately 40% of convulsive status epilepticus cases—preparation for second-line therapy is crucial, marking the transition to established status epilepticus. For other types, including non-convulsive status epilepticus, early benzodiazepine treatment is recommended, although evidence from large randomized controlled trials is still limited. The management of non-convulsive status epilepticus demands early neurology or epilepsy expert consultation, EEG confirmation of the diagnosis, and tailored treatment approaches that consider causes, individual responses, and expected outcomes, especially in cases of acute brain injury (21-23).
3.2 Second Line Therapy
Until recently, there was a noticeable gap in high-quality evidence regarding the selection of antiepileptic drugs (AEDs) for the second-line treatment of established status epilepticus. Current therapeutic options include intravenous (i.v.) fosphenytoin, administered at a dosage of 20 mg/kg (with a maximum limit of 1500 mg), valproate at 40 mg/kg (maximum 3000 mg), and levetiracetam at 60 mg/kg (maximum 4500 mg). A multicenter, double-blind randomized trial conducted by Kapur et al. examined the efficacy of i.v. levetiracetam, fosphenytoin, and valproate in a cohort of 384 patients, both adults and children over the age of 2 years, who presented with convulsive status epilepticus resistant to benzodiazepines in emergency settings. The trial's primary outcome, which focused on the absence of clinically apparent seizures and enhanced responsiveness at 60 minutes post-infusion, revealed no significant differences among the three treatment options. Seizure termination was achieved in approximately 50% of patients within each treatment group, and no notable variations were identified in secondary outcomes or safety profiles across the three AEDs. An alternative second-line treatment option is i.v. phenobarbital, administered at a dose of 15-20 mg/kg, provided it has not been previously administered. Although phenobarbital is recognized for its effectiveness, its use is often constrained due to the associated risks of sedation, respiratory depression, and hypotension. Additionally, intravenous lacosamide (at a dose of 400 mg) has been increasingly utilized for established and refractory status epilepticus, with potential efficacy comparable to conventional antiepileptic drugs; however, this efficacy has yet to be conclusively demonstrated (24-26).
CONCLUSION
Implementing early, evidence-based treatment modalities is critical to preventing mortality and complications associated with prolonged status epilepticus (SE). Benzodiazepines remain the most effective first-line therapy, though they are often under-dosed. For second-line therapy, options include levetiracetam, fosphenytoin, or valproic acid, all of which have shown equivalent efficacy in managing established SE. In cases where patients progress to refractory and super-refractory SE, a trial of anaesthetic coma may be necessary; however, there is limited quality evidence regarding the choice of anaesthetic agents, the depth and duration of therapeutic coma, EEG treatment targets, and weaning strategies. Recent studies indicate that ketamine can be effective in aborting status epilepticus, though there is a lack of prospective comparative studies to confirm these findings. The aetiology of SE serves as a crucial predictor of patient outcomes and should guide therapeutic options. If an immunological cause is suspected, early empiric treatment with immunomodulatory drugs is advisable. In super-refractory SE cases, several additional treatment options can be considered, including repetitive transcranial magnetic stimulation (rTMS), vagal nerve stimulation (VNS), and resective surgery. Nonetheless, these treatments should be reserved for super-refractory instances, as careful consideration is warranted due to their limited evidence and potential risks of harm.
CONFLICT OF INTEREST
None
REFERENCES

Akanksha Borade, Dr. K. R. Biyani, Dr. R. A. Ingle, Dr. P. N. Folane, A Comprehensive Review on Clinical Perspectives on Convulsions and their Management, Int. J. of Pharm. Sci., 2025, Vol 3, Issue 12, 3601-3607. https://doi.org/10.5281/zenodo.18047787
 10.5281/zenodo.18047787
10.5281/zenodo.18047787
